
Abstract
Objective
To assess the cost-effectiveness of strategies to increase cervical cancer screening uptake at first invitation (STRATEGIC trial).
Methods
We performed an economic analysis alongside the STRATEGIC trial, comparing each of seven novel interventions for improving cervical screening uptake with control general practices in Greater Manchester and Grampian (United Kingdom). A template was developed to measure the intervention costs. Trial estimates of screening uptake were combined with data from the literature to estimate healthcare costs of each intervention. The added lifetime costs and quality adjusted life years (QALYs) of attending cervical screening were estimated by a systematic literature review, with relevant results pooled and weighted by study quality. Trial results and estimated lifetime costs and benefits of screening were then combined in a decision analytic model, giving an incremental cost per QALY gained for each intervention. Uncertainty was addressed in probabilistic and univariate sensitivity analyses.
Results
Intervention costs per screening round per woman attending varied from about £1.20 (2014 UK) for the nurse navigator intervention to £62 for the unrequested HPV self-sampler kit. The meta-analysis revealed a lifetime discounted benefit from screening of 0.043 QALYs per woman attending, at an additional lifetime discounted cost of £234. The incremental cost per QALY gained in all interventions was below £13,000. Probabilistic sensitivity analyses suggested that only unrequested self-sampling and timed appointments have a high probability of being cost-effective.
Conclusions
Unrequested self-sampling and timed appointments are likely to be cost-effective interventions. Further research is required on the duration of effects and on implementing combinations of interventions.
The United Kingdom (UK) has a lower than average incidence rate of cervical cancer among all European countries. 1 This is partly attributable to the National Health Service Cervical Screening Programme, which was established in 1988 throughout the country. 2 Coverage of the screening programme fell between 2003 and 2013 in England and Scotland,3,4 most notably at initial cervical screening among young women, who already had lower coverage rates than older women. Similar trends have been reported in other developed countries. 5 This decline in coverage among young women is already reflected in the rising incidence of cervical cancer amongst this cohort. 6 Another concern is the great variation in coverage rates across local authorities, which implies unequal distribution of the screening programme benefits at national level, potentially disadvantaging socially deprived and ethnic minority groups.
The Strategies to Increase Cervical Screening Uptake at First Invitation (STRATEGIC) trial was designed to investigate whether a range of novel interventions, when embedded within routine cervical screening practice, improve young women’s receptivity to and uptake of cervical screening. 7 As part of the trial, this study aimed to assess the cost-effectiveness of these interventions in terms of lifetime costs and quality adjusted life years (QALYs). Such information can support the redesign of cervical cancer screening services in the UK to reduce the future health and economic impact of cervical cancer.
Methods
An economic analysis was designed to be conducted alongside the STRATEGIC trial, a pragmatic, multicentre, cluster randomized controlled trial. The study included all women registered in general practices from three Greater Manchester (England) Primary Care Trusts and Grampian (Scotland), who were about to receive their initial cervical cancer screening invitation (aged 25 in Manchester and 20 in Grampian). The trial offered seven novel interventions in two consecutive phases, to increase screening attendance in those women. In phase 1, the trial offered a pre-invitation leaflet (pre-leaflet) six weeks prior to their first invitation that aimed to prepare young women to engage more fully, as well as an online booking system that enabled women to book their initial screening test at a date of their convenience (online booking). In phase two, the trial offered the following five interventions: a letter sent to the women offering them the opportunity to request a human papilloma virus (HPV) self-sampling kit (RSS), an unrequested HPV self-sampling kit (USS) sent directly to their home, a nurse navigator (NN) available to offer help and advice in attending a cervical screening test, a letter with a timed appointment for a cytology test with the option to be rearranged at a more convenient time if needed, and a letter offering women the choice of either having access to an NN or an RSS. A detailed description of how the interventions was operationalized is presented in Supplemental file 1.
In phase 1, 276 general practices (20,879 women) were randomized to the pre-leaflet group or a control group (i.e. women were not offered a pre-leaflet). Practices in Manchester Primary Care Trusts only were also randomized to the online booking group or a control group (i.e. online booking was not offered) and balanced for the pre-leaflet intervention. In phase 2, whilst also balanced for phase 1 interventions, 267 practices were randomized to one of the five phase 2 interventions (i.e. RSS, USS, NN, timed appointment, choice) or a control group (i.e. none of the phase 2 interventions was offered). The interventions in phase 2 were provided only to women who had not undergone screening by six months following their initial invitation and remained located in the same Primary Care Trust. The Consolidated Standards of Reporting Trials diagram for the STRATEGIC trial is presented in Figure 1. Further details of the study design and the provided interventions are provided in the trial protocol
8
and the accompanying paper.
9
CONSORT diagram for the STRATEGIC trial.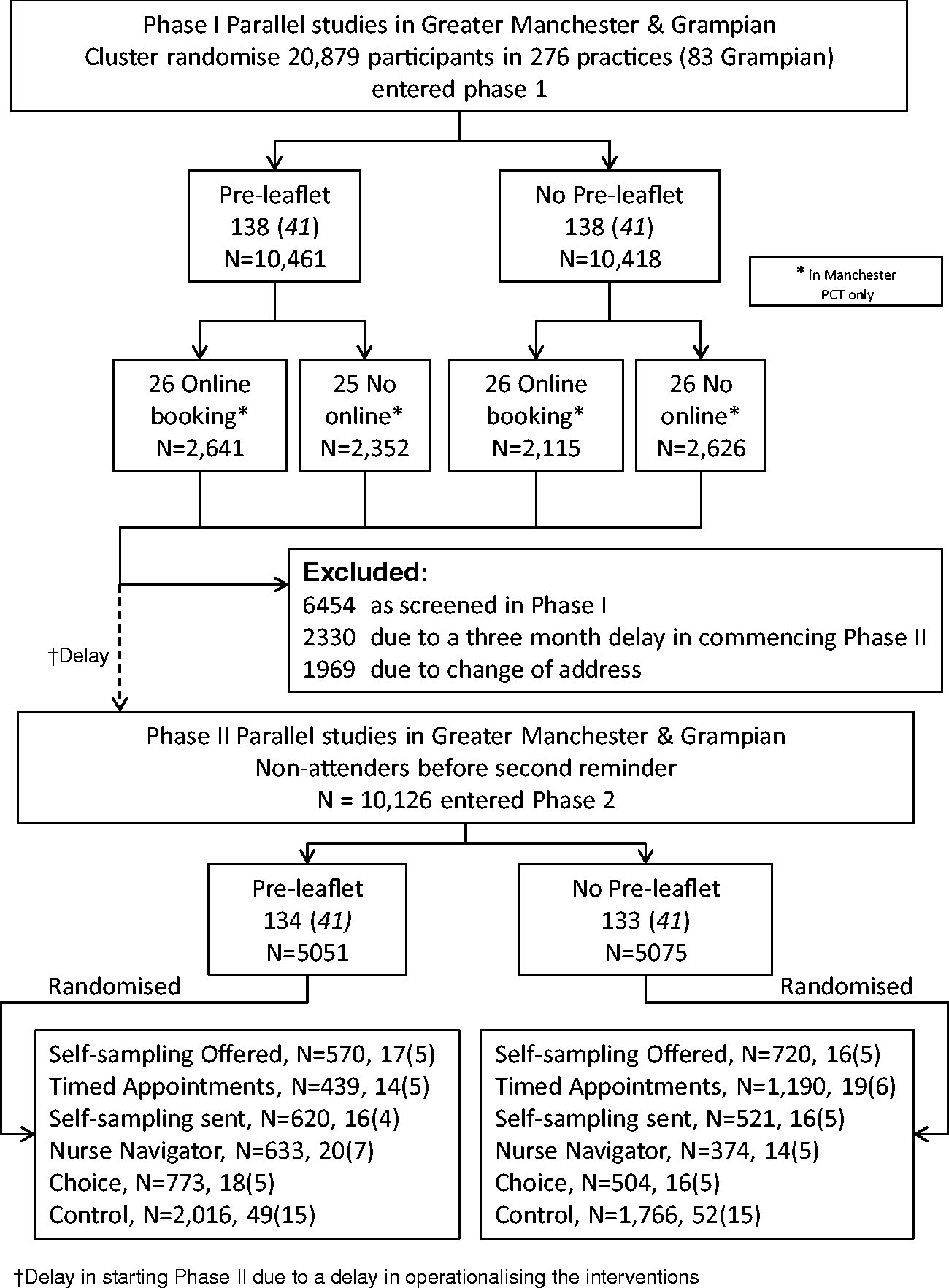
This economic analysis was designed alongside the STRATEGIC trial and aimed to provide reliable estimates of cost and cost-effectiveness, while adhering to the general approach of the trial, which maximized the use of routine data sources and minimized direct contact with participating women. The design and reporting follow the methodological guidelines issued by the National Institute of Health and Care Excellence (NICE) for economic evaluations 10 and the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) statement. 11
All resources required to develop and implement each intervention were identified and recorded by two trial research team members, and intervention providers cross-checked these to ensure completeness and accuracy. The list included labour time, printing and distribution of information materials, laboratory kits, rent for meeting rooms, training of professionals, information and communications and programming. Labour time costs were based on total employer cost (including salary, superannuation, and national insurance) corresponding to the salary grade of the staff involved in an activity, and included 20% overhead costs to cover premises and utilities. A detailed list of the items for each intervention, and associated costs, is presented in Supplemental file 2. Data on cytology tests and HPV self-sampling tests were collected from the screening agencies in Greater Manchester and Grampian. The number of colposcopies was estimated using information from the National Screening Programme about the colposcopy referral rate for the relevant age group, the attendance rate, and the proportions of outpatient diagnostic procedures, outpatient diagnostic procedures with biopsy and therapeutic colposcopies. Based on this information, we estimated the total number of HPV tests, cytology tests and colposcopies for each intervention and control group. Unit costs of HPV tests and cytology tests were obtained from previous studies,12,13 and included staff time in screening centres and laboratories, equipment and consumables. Unit costs of different types of colposcopy procedures were obtained from the NHS reference costs 2013–2014. All unit costs were inflated to 2014 prices using the Hospital and Community Health Services inflation index.
The within-trial outcome measure for all interventions was completion of a cervical cancer test at the age of initial screening, measured at three and six months post-invitation for phase 1 interventions (i.e. pre-leaflet and online booking) and at 12 and 18 months post-invitation for phase 2 interventions. The primary endpoint for phase 1 interventions was uptake of screening at three months, and for phase 2 interventions at 12 months post-invitation.
Information about the incremental lifetime costs and benefits (quality adjusted survival) of attending cervical cancer screening was obtained through a systematic literature review (see Supplemental file 3). We searched for all economic evaluations of cervical cancer screening strategies which included no screening as a comparator and reported lifetime costs and outcomes in the form of life years and/or QALYs, and followed the recommendations of the Centre for Reviews and Dissemination 14 and Cochrane Central Register of Controlled Trials 15 in searching MEDLINE, MEDLINE In-Process, EMBASE, EconLit, and NHS Economic Evaluation Database (NHS EED). Letters, editorials, animal studies, studies published before 1995 and non-English language studies were excluded. Titles and abstracts of retrieved studies were scanned for relevance and full text accessed if the paper was judged to meet the inclusion criteria. Full texts were then assessed for eligibility against the PICOS criteria. The process was documented in MS Excel, and reasons for inclusion and exclusion were detailed to facilitate updates of the review. The websites of agencies including NICE, MRC, and national cancer screening programmes were also scanned for relevant reports. A template was developed and used to extract the information from the studies most relevant to the STRATEGIC trial. In this process, the next more costly strategies to no screening, as well as strategies that had similar population (i.e. age groups), interval of screening, and discount rates (i.e. 3.5%) to UK were preferred. Where results from cancer screening in several countries were reported, we selected the UK-based estimates. The review was performed in May 2015. The quality of identified studies was assessed by two assessors using checklists of good practice for modelling and reporting,11,16 with mean assessment score assigned in cases of disagreement.
Costs were inflated from each study’s price reference year to 2014 using consumer price inflation rates for each study’s country of origin, as reported by OECD, 17 and converted to UK Sterling using average exchange rates for the year 2014 (see Supplemental file 3). 18 Life-years and QALYs retrieved from the included studies were adjusted to make them comparable and relevant to the UK context, by applying the ratio of discounted life expectancy between the screening and control cohorts in the selected studies to the discounted life expectancy at the mean age of women in the trial. Mean EQ5D utility weights from women in the UK general population at each year of the discounted life expectancy were then applied to calculate discounted QALYs. These modelling studies included screening coverage at different age groups to allow for different non-attendance patterns over a woman’s life, and these patterns are therefore included in our pooled lifetime estimates for outcomes and costs.
A meta-analysis was then performed, using a random effects model to pool the estimated lifetime discounted costs and outcomes reported in the identified studies, assuming real differences in treatment effects because of heterogeneity in screening strategies, population, and other factors. 19 Study quality scores were used to weight each study’s contributed information to the pooled estimate (i.e. a study with high quality score contributed more to the pooled estimate than a lower quality study).
A decision model was constructed in Excel to calculate the lifetime costs and outcomes of each intervention. In the baseline analysis, we treated all interventions as independent. The accompanying paper reports no significant interaction between the phase 1 interventions, or between the phase 1 and phase 2 interventions. Consequently, each of the seven interventions was compared with the respective control group. However, some of the phase 2 interventions could be considered mutually exclusive, and so we also report an analysis comparing them against each other. The basic approach of the model was to combine the within-trial cost and effectiveness results for each intervention and control group with the estimated lifetime discounted outcomes and costs of screening attendance, derived from the results of the meta-analysis. The probabilities of attendance in each intervention and control group were informed by the trial results. Intervention costs were obtained from the trial and lifetime QALYs and lifetime costs from the meta-analysis. Incremental cost-effectiveness ratios (ICERs) were expressed as incremental costs per woman attending a screening test, and incremental costs per QALY gained.
Probabilistic sensitivity analysis was performed to address uncertainty in the ICERs by performing 5000 draws of all cost and effect parameters using pre-specified distributions, recording incremental costs and incremental QALYs from each draw, and plotting the results on cost-effectiveness planes and acceptability curves. The latter display the probability that each intervention is cost-effective, as the ceiling ratio for the maximum acceptable incremental cost-effectiveness ratio varies from £0 to £75,000 per QALY gained. Distributions for within-trial costs, outcomes and attendance rates were derived from reported means and standard errors. Distributions for lifetime screening costs and QALYs were estimated from means and standard errors from the meta-analysis. The intervention costs per attendee, unit costs and probabilities of having an HPV test, cytology test and colposcopy were also included in the probabilistic sensitivity analysis.
Seven univariate sensitivity analyses were also performed. One examined the impact of using secondary endpoints (six months instead of three for phase 1, 18 months instead of 12 in phase 2) of the trial on the results of the economic evaluation (Supplemental file 4). In a second sensitivity analysis, study quality scores based on Phillips et al. 16 to weight the pooled estimates in the meta-analysis were replaced with study quality scores based on the CHEERS statement. In a third sensitivity analysis, only the lifetime costs and lifetime QALYs reported in the most recent UK study were used in the meta-analysis. The fourth, fifth and sixth sensitivity analyses explored the effect of changing the baseline assumption that the intervention is a one-time behavioural “nudge”, i.e. that a non-attender is a never attender and that once the intervention achieves screening adherence, the woman becomes an always attender. These analyses assessed the impact on the results if the interventions had to be provided 3, 6 or 12 times, respectively, in a woman’s lifetime to obtain lifetime participation in cervical screening. The seventh sensitivity analysis assessed the impact on the results of the economic evaluation of treating phase 2 interventions as mutually exclusive.
Finally, a scenario analysis was performed to explore the adoption of these interventions for a population of 365,087 women in phase 1 interventions, which is approximately the total number of women annually invited for cervical screening for the first time in England, Scotland, and Wales. A similar scenario analysis was performed for phase 2 interventions applied to a population of 255,561 women, assuming that only 30% of women were screened during phase 1. In these analyses, intervention costs were categorized into fixed one-off costs, semi-fixed scalable costs which are incurred in steps as scale increases and variable costs. In this analysis, it was assumed that large-scale purchasing of materials and equipment would allow a cost discount – set at 20% – to be obtained. Therefore, only the components of total cost that are not variable will affect the cost per woman and the ICERs.
Results
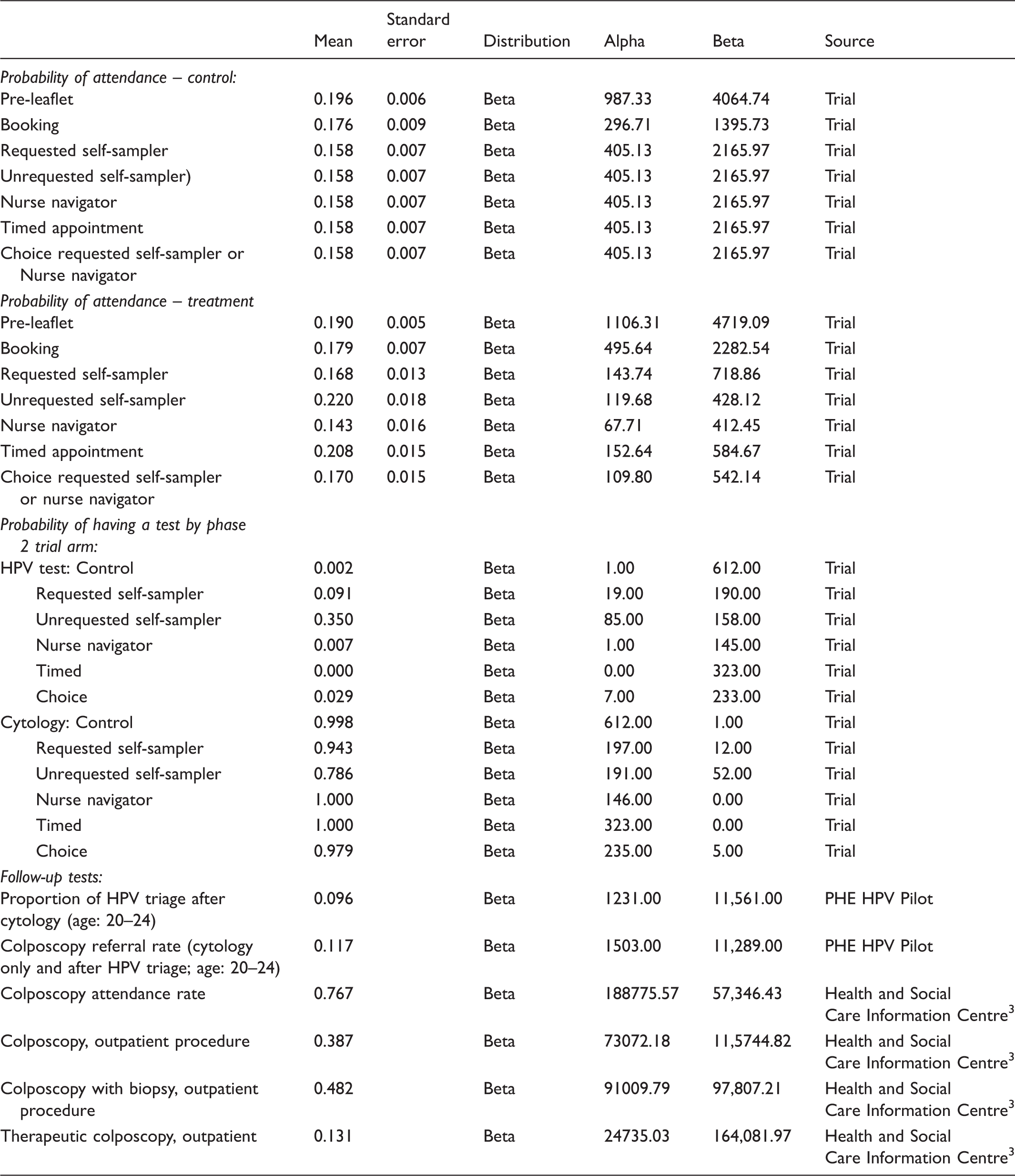
Probability of attendance (at three months follow-up for phase 1, 12 months for phase 2), and probability of being tested, by arm and intervention: mean (se), distribution and source.
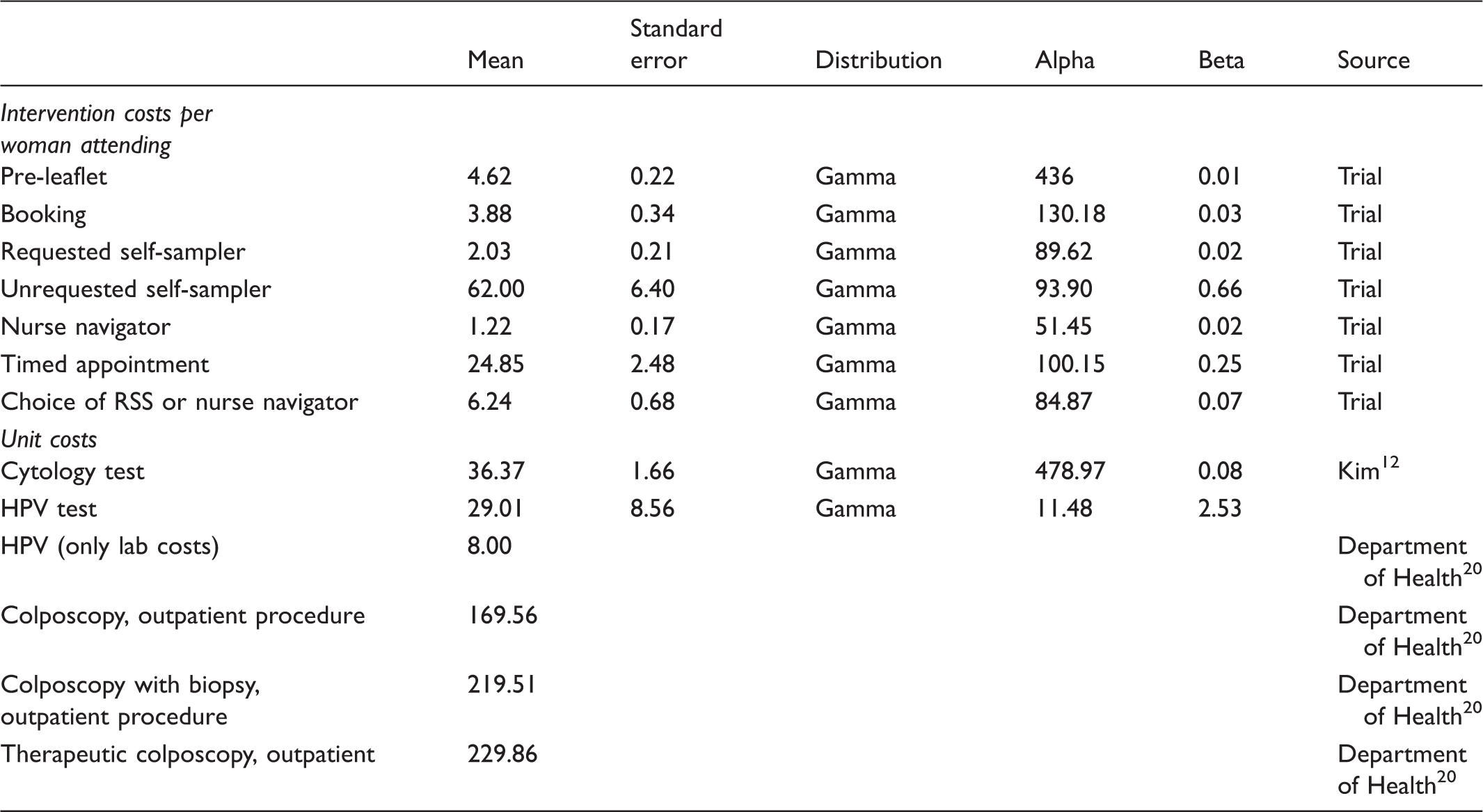
Costs of each intervention for one screening cycle (at three months follow-up for phase 1, 12 months for phase 2), and unit costs for tests and procedures: mean (se), distribution and source (£s 2014).
Pooled estimates from meta-analysis of lifetime discounted costs and outcomes for screened and unscreened populations.

QALY: quality adjusted life year.
Cost-effectiveness of each intervention compared with control, assuming each intervention is offered only at initial screening round.
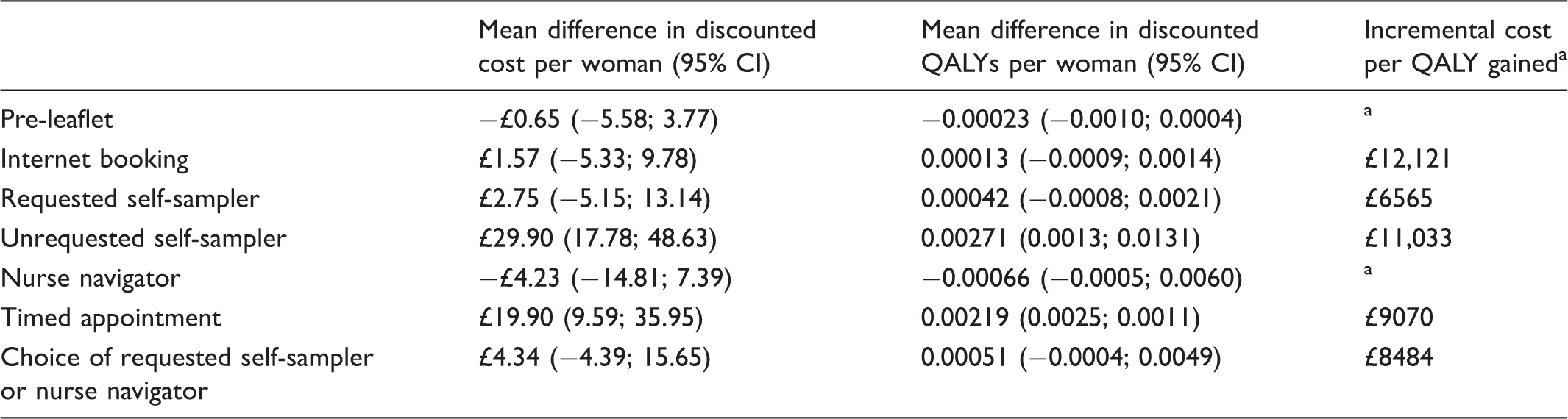
QALY: quality adjusted life year.
Difference in costs divided by difference in outcomes.
Lower costs and lower outcomes.
The results from the probabilistic sensitivity analysis are presented in Figure 2, in the form of cost-effectiveness acceptability curves, which display the probability of each intervention being cost-effective at different willingness-to-pay values for one QALY. The probabilities do not add up to 1 because the interventions are treated as independent. The pre-leaflet intervention is characterized by high uncertainty surrounding costs and effectiveness; hence, the probability of this intervention being cost-effective is very low. A similar pattern is displayed by the NN intervention. Internet booking similarly has no clear evidence of effectiveness, and so the probability that this intervention is cost-effective at conventional ceiling ratios (i.e. NICE uses a range between £20,000 and £30,000 as an explicit threshold) of willingness-to-pay for one QALY never rises above 60%. RSS has a slightly higher probability of being cost-effective, but this rises no higher than 73% at any level of willingness to pay; a similar pattern is displayed by the Choice intervention, which includes RSS. For timed appointments, the probability that the intervention is cost-effective at a ceiling ratio of £20,000 per QALY gained is 90% rising to 95% at a ceiling ratio of £30,000. USS, the most expensive intervention, has 85% and 94% probability of being cost-effective at £20,000 and £30,000 ceiling ratio per QALY, respectively. Both interventions are clearly more effective than control, and both are also almost certain to cost more than control. This is illustrated clearly in the cost-effectiveness planes for each intervention, reported in Supplemental file 6, in which 5000 cost–effect pairs are derived with all parameters varying.
Cost-effectiveness acceptability curves for each intervention (baseline analysis: interventions offered over 1 cycle; outcomes assessed at three months for phase 1 interventions and 12 months for phase 2).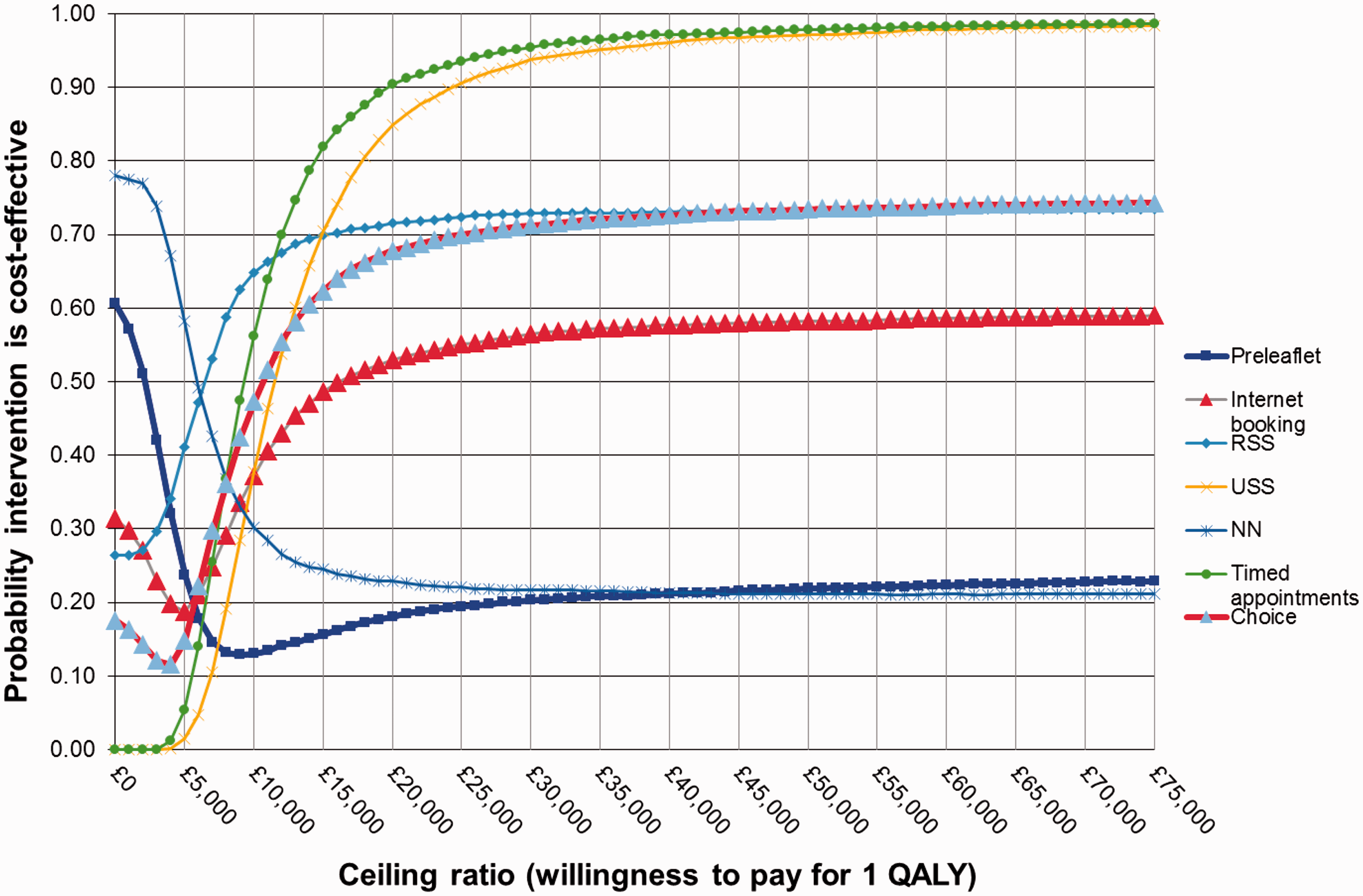
Cost-effectiveness results from the univariate sensitivity and scenario analysis.

NA: not applicable; ED: subject to extended dominance; QALY: quality adjusted life year.
Note: each STRATEGIC intervention is compared with control in all Panels except Panel G, where they are compared with the next most effective STRATEGIC intervention.
Lower costs and lower outcomes.
USS compared with timed appointment.
Timed appointment is compared with RSS after deleting extendedly dominated option (Choice).
Higher costs lower outcomes.
Panel B of Table 5 reports the results for each intervention when the studies used to derive estimates of lifetime benefits and costs of screening are given quality weights using the CHEERS study criteria. This change makes each intervention slightly more cost-effective. Panel C shows the results when using only the most recent UK study for estimates of the lifetime costs and outcomes of screening; lifetime costs and outcomes are both lower than in the pooled meta-analysis results, but particularly outcomes, with the result that the cost-effectiveness ratios all increase compared with the baseline analysis while uncertainty increases. Panels D, E and F and Supplementary Figures 6.5, 6.6, and 6.7 show the results when assuming that the interventions are provided for three, six and 12 rounds, respectively, over a woman’s lifetime, compared with a single round in the baseline analysis. As expected, the ICERs increase substantially and the corresponding probability that any of the interventions are cost-effective at a £20,000 ceiling ratio decreases markedly. Panel G reports cost-effectiveness results if the phase 2 interventions were to be treated as mutually exclusive, ranked in ascending order of effectiveness and compared with the next best intervention. The two phase 1 interventions – pre-leaflet and internet booking – are omitted from this comparison. The choice intervention is shown as being extended dominated. Results for the RSS intervention are unchanged, control being the next best alternative; timed appointments have an ICER of £9660 compared with RSS, and USS has an ICER of £19,380 when compared with timed appointments. These results are also shown graphically in Supplementary Figure 7.1.
Panel H in Table 5 reports the results of the scenario analysis in which it is assumed that the relevant population is all women eligible for cervical screening in England (365,087 in 2014). Effectiveness is unchanged in this analysis, but the per person costs of each intervention are lower due to economies of scale in the fixed costs of these interventions, which could be spread over a much larger population. We have also assumed that some variable costs, such as printing and postage, could be reduced via bulk contracts if these interventions were scaled up to the national level, and have assumed a reduction of 20%. As a result, the cost-effectiveness of all interventions improves.
Discussion
In this study, we have estimated the within-trial costs and lifetime cost-effectiveness of each of the interventions considered in the STRATEGIC trial, in comparison with the relevant control group as in the trial design, and also in comparison with each other in a sensitivity analysis.
Using information collected in the trial, we found that the costs of each intervention varied widely, from £1.22 per woman attending for the NN to £62 for USS per woman attending. These costs could be lower if the interventions were rolled out nationally and realized economies of scale, but the reductions were not dramatic.
The effectiveness of the interventions in our study is informed by the observed impact in the trial of the interventions on screening attendance. It was clear from the attendance probabilities of different interventions that the USS intervention had the largest statistically significant effect, followed by the timed-appointment intervention. The trial provided less guidance on how the different interventions examined in phase 1 and phase 2 of the evaluation might be offered in routine practice, and in particular, whether they can be considered mutually exclusive, or might be combined in various ways. Statistical tests suggested no interaction between the two phase 1 interventions, or between the phase 1 and the phase 2 interventions, but it is not clear whether phase 2 interventions could be offered simultaneously, or whether, for example, timed appointments could be offered to all, and USS to those who did not attend. The full range of such implementation scenarios goes beyond the remit of this study and would require further attention. However, whether the interventions are independent or mutually exclusive affects the economic evaluation directly, and given the ambiguities, we have provided results under both assumptions, which show that the ICERs remain below the £20,000 threshold.
Neither does the STRATEGIC trial provide clear guidance on the duration of the effects observed for some interventions. In our baseline analysis, we simulate a continuing effect from the initial intervention. However, in sensitivity analyses, we vary this assumption between a single round and offering the intervention for all 12 rounds of the current screening programme, making the intervention less cost-effective. Studies with longer follow-up could provide valuable evidence on this question.
Previous economic evaluations of interventions aimed at increasing (mainly breast) cancer screening uptake are relatively few and have methodological limitations such as short time-horizons.21–23 A recent economic evaluation of strategies to increase uptake of cervical cancer screening in Spain had a 3.5-year time-horizon, and reported ICERs in terms of costs per 1% increase in screening coverage. 24 To translate participation in the screening programme into the lifetime cost-effectiveness perspective that decision makers require, we extracted and pooled information on the lifetime costs and benefits of participating in cervical cancer screening from a systematic literature review and meta-analysis of lifetime models of cervical cancer screening. Our baseline analysis uses the pooled results across all eligible studies, but we also report an analysis using only the most recent UK-based modelling study, which results in poorer cost-effectiveness estimates combined with more uncertainty. Further work would be helpful in understanding the sources of heterogeneity between such models. Existing models also typically simulate lifetime participation or non-participation in screening, and further research is required to explore changes in participation rates over the life-cycle and their effects.
The STRATEGIC study found that two of the interventions examined – USS and timed appointments – were associated with small but statistically significant increases in screening uptake. 7 In this analysis, which also takes the intervention costs and possible long-term costs and benefits into account, we find that both interventions offer a reasonable probability of being cost-effective at conventional UK thresholds. The results of our analysis can also be used to estimate the cost reductions (such as lower kit prices) that would be required to increase the likelihood of USS being cost-effective at a £20,000 ceiling ratio, if its effectiveness made it an attractive option to decision makers or to women in the target age-groups.
The economic analysis has not replicated the sub-group analyses performed in the main trial results, comparing vaccinated and unvaccinated women and comparing Grampian and Greater Manchester, because it is unclear how any cost-effectiveness differences arising from these comparisons could be interpreted or used by decision makers. However, it is likely that vaccination will have an increasing impact on the future operation and cost-effectiveness of the cervical cancer screening programme.
Conclusion
Using new evidence from this large cluster randomized controlled trial, we conclude that USS and timed appointments offer a reasonable probability of being cost-effective at conventional UK thresholds. Further research is required on the duration of effects and on implementing combinations of interventions.
Footnotes
Acknowledgments
The authors thank Zeinab Abbas for her valuable assistance, and Carly Moseley from the STRATEGIC trial team for her support in conducting this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by NIHR (NIHR-HTA Ref 09/164/01) as part of the STRATEGIC trial (Trial Registration: ISRCTN 52303479).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.