
Abstract
Background:
Cervical cancer is considered the third leading cause of death among women worldwide, and human papillomavirus was identified as a major causative agent for developing cervical cancer.
Objectives:
This study aimed to assess the knowledge and attitudes towards cervical cancer prevention among women in Khartoum state, Sudan.
Design:
A community-based cross-sectional study implemented in Khartoum state, Sudan, from 1 August 2020 to 1 September 2020.
Methods:
We conducted a descriptive cross-sectional community-based study using an electronic questionnaire for data collection. Descriptive statistics, frequency, mean, and percentage were computed.
Results:
The study included 716 female participants with a mean age of 27.6 + 8.7 years. 580 (81.0%) and 229 (32.0%) had heard about cervical cancer and Pap test, respectively. cervical cancer was assumed related to alcohol consumption 109 (15.2%), giving birth to many children 51 (7.1%), ageing 118 (16.5%), and having many sexual partners 335 (46.8%). In addition, 300 (41.9%) attributed cervical cancer to having human papillomavirus infection, 256 (35.6%) to the prolonged use of contraceptives, and 162 (22.6%) to smoking. Knowledge about the best time to be vaccinated against human papillomavirus, 110 (15.4%) stated it is better after marriage. Regression models to predict the effectors on participants’ knowledge and attitudes showed a low standard deviation of the estimates with higher values of the adjusted R2 [R: 0.041, 0.017, and 0.006; std: 1.527, 0.417, and 0.426]. This indicates the combined influence of occupation, educational level, family income, and marital status on the participant’s knowledge and attitude levels.
Conclusion:
This study revealed that the participant’s knowledge and attitudes levels are mainly driven by their occupation, educational level, family income, and marital status altogether. This underscores the need for a countrywide community engagement campaign through health education and raising awareness sessions, and massive social media to sensitize the community and healthcare providers about the risk of cervical cancer and the available prevention and control measures.
Introduction
Cervical cancer (CC) is one of the most common cancers affecting the female genital tract worldwide, with about 80% of the cases reported from developing countries.1–3 In Sudan, CC has been reported as the second most common female cancer between 1954 and 1961. 4 In addition, previous studies have demonstrated that CC represents over 8% of all types of cancer among females during 2000–2006. 5 More than 8000 cases are reported annually in Sudan, usually presented at the late stages of the disease.6,7 In 2020, according to the International Agency for Research on Cancer (Globocan) data, there were 1227 new cases of CC cases that represent 7.4% of the number of all new cancer cases among females. And ranks the fifth type of cancer in incident rate with 828 (4.9%) deaths. 8 However, Sudan National cancer registry is inactive, and the only data source available is Khartoum Cancer Registry. 8 Therefore, records of cancer cases that existed are mainly obtained from hospitals and fragmented research reports,9–12 making planning and implementing preventive and healthcare services towards CC challenging to achieve.
Furthermore, in Sudan, to the best of our knowledge, a few hospitals initiated a Papanicolaou smear (Pap smear) and/or visual inspection with acetic acid (VIA) testing for CC diagnosis. 13 Nevertheless, Pap smear or VIA test is mainly requested by gynaecologists when cervical malignancies are suspected. However, most of them failed due to the scarcity of well-trained cytologists and cytopathologists.14,15 Also, religious beliefs and behavioural aspects of conducting the diagnosis make it difficult to rely on it in cases of screening of ordinary checkups. 16 CC screening is not currently available through the public health system in Sudan. Women can be screened at some hospitals but must pay out of pocket for the screening. One study found as few as one in 10 women have been screened for CC, 17 and a second study found slightly higher rates but still low screening rates, 36.8%. 16
CC can be induced by different etiological factors. The human papillomavirus (HPV) is one of the most important aetiological agents that lead to CC development.11,16,18 Over 99% of all CC cases are associated with HPV infection. 19 Fortunately, regular screening can prevent CC by detecting preinvasive diseases or cervical intraepithelial lesions (CIN).19–21 Such screening programmes have successfully led to the detection of precancer CIN and cancer in an early stage using the Pap smear or VIA test.6,20,22 Adopting Pap smear as a screening tool for the early detection of CC in population-based screening programmes has successfully reduced the incidence of late CC by 85% in several developed countries over the past decades.10,23
CC can be prevented by either preventing infection with HPV or detecting and treating CIN before progression into invasive cancer.24,25 While CC is a highly preventable disease in western countries, it is one of the leading causes of death among African women due to the absence of a population-based screening, early detection, and poor case management of the disease. 26 Multiple factors contribute to the suboptimal CC screening in low-income countries, such as the fragile health systems, inadequate national screening systems, and lack of awareness among the population at risk, healthcare providers and policymakers, as well as limited access to healthcare services and lack of public awareness.16,24,27 A study conducted in Sudan has demonstrated that lack of awareness, poverty, and limited health insurance resulted in deficient access to healthcare services leading to late diagnosis of CC. 21 Another study in the Congo reported that low levels of knowledge, lack of good health practices, and poor attitudes towards CC were associated with high prevalence and mortality rates. 24 Previous research has shown that raising awareness about CC risk factors, and symptoms were associated with a significant increase in the numbers of patients diagnosed in earlier stages I and II. 28
There is severely limited data on women’s awareness of CC in Sudan. Therefore, this study was designed to assess Sudanese women’s knowledge and attitudes regarding CC and their beliefs about the disease risk factors and preventive measures. Furthermore, investigates the link between socioeconomic status, education level, and other factors to women’s knowledge and attitudes towards CC and explores the obstacles of early screening and other preventive measures, including the HPV vaccine.
Methods
Study design and site
This is a community-based cross-sectional study implemented in Khartoum state, Sudan, from 1 August 2020 to 1 September 2020, to assess women’s knowledge and attitudes towards CC prevention. Khartoum state is the capital of Sudan, with a wide ethnical diversity that represents the country. 29
The study questionnaire design, validation, and methods of distribution
We have adopted a well-established questionnaire 28 to be delivered via an electronic survey (Google Form) and printed format. For validation of the questionnaire, the questionnaire was circulated among five experts; each of them independently rated each question on the questionnaire as satisfactory or unsatisfactory on a validation form. Questions that had been validated as unsatisfactory were improved and reassessed until all questions were rated as satisfactory, and we optimized them so they could be answered within less than 15 min.
English and Arabic versions of the questionnaire were developed. Both were pre-tested among a small group of women to validate and modify the questionnaire to ensure that the interviewees and data collectors understood the questions without losing their power to capture accurate information. Then, the final approved questionnaire was shared with different Sudanese groups, with the females majority in the community and on social media. The questionnaire included 28 questions covering demographic and socioeconomic characteristics, knowledge of CC, its risk factors, the screening methods, including Pap smear, preventive measures towards HPV, and the vaccination programmes. The demographic data include age, education level, occupation, family monthly income, and marital status. Regarding reproductive-health data, we asked about the number of children, presence or absence of a family history of CC, history of sexually transmitted diseases, methods used for family planning, number of sexual partners, smoking, and alcohol consumption. Furthermore, questions regarding the knowledge about CC included hearing about CC and the associated risk factors. The questionnaire consisted of 16 closed-ended questions (Yes, No, and I do not know) and 12 questions with multiple-choice and options for individual open-answers. A form of the questionnaire is available as a Supplemental File 1. Considering the social preference for social media in Sudan, the online form questionnaire study was shared through Facebook® and WhatsApp®. To avoid personal identification, we followed institutional guidelines and regulations, including data anonymization and individual data coding. The online form of the questionnaire is available at (https://docs.google.com/forms/d/e/1FAIpQLSfb-bt7vOYKWDW912Ybh4T9qIj7emA2UevJjZcuPoadSfJU0w/viewform). A pre-questionnaire statement was included as an informed consent prior to participation in the survey.
Sample size determination and study population
Sample size determination was restricted by the survey duration of 30 days between 1 August and 1 September 2020. The identification of the target population for the survey was based on the population at risk featured as females over 17 years old, regardless of any other differentiating features. Participating in the survey was limited to residents of Khartoum state only to reduce the selection bias due to the limited access to the Internet in the other states and lack of funding for the data collector to travel there in person. Inadequately filled questionnaires were excluded from the analysis. A flow chart describing the study flow is illustrated in Figure 1.

Flow chart showing the detail of the flow of the study.
Statistical analysis
The study data were amalgamated to be exploitable in an Excel sheet using Microsoft Office software 2016. A verification step based on the respondent age groups was included to ensure the sample’s representativeness compared to the source population. The mean, standard deviations, and frequency of each variable among the respondent were calculated. The Chi-square test was used to analyse data and test the significance level. The t-test was used to analyse continuous variables; a p-value < 0.05 was considered statistically significant. Also, multiple linear regression models were tested to predict the effectors on participants’ knowledge and attitude. All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS version 20).
Results
The demographic and socioeconomic characteristics of participants
In total, 716 females from Khartoum state participated in this study. Their age ranged from 18 to 74 years old, with an average of 27.6 years (Std 8.7 years). Among the participants, 35.1% were students, while 22.1% were unemployed. The remaining occupations were 10.6% medical doctors, 6.0% laboratory technologists, 5.7% teachers, and 5.4% managers. The remaining 15.1% consisted of other disciplines that were insignificantly frequent.
Regarding the family history of CC, 31 (4.3%) reported a family history of CC, 523 (75.0%) confirmed no family history, and 148 (20.7%) did not know about their family history (Table 1).
Demographic characteristics, behavioural, and historical background of the study population.
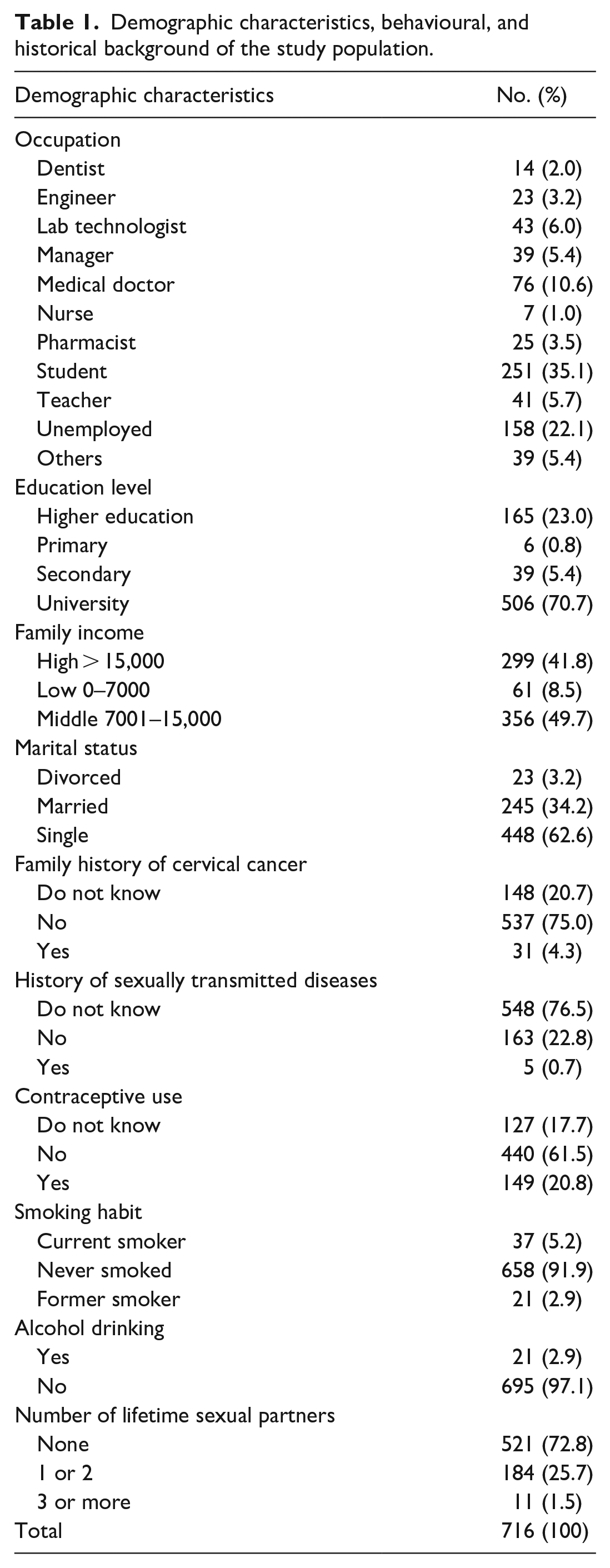
Five hundred forty-eight (76.5%) did not know whether they were previously infected or not. While those who confirmed no previous or current infection were 163 (22.8%), and only 5 (0.7%) participants indicated current or previous infection with sexually transmitted diseases (STDs).
Respondents who reported avoiding contraceptives were 440 (61.5%), while 149 (20.8%) stated they were using contraceptives for family planning. Alarmingly, 127 (17.7%) did not know what contraceptives were or their use. 658 (91.9%) were non-smokers, with current and former smokers 37 (5.2%) and 21 (2.9%), respectively. Only 21 (2.9%) reported drinking alcohol occasionally, while 695 (97.1%) did not drink alcohol.
The number of lifetime sexual partners mainly was within one or two partners; 184 (25.7%), while those with more than two partners were only 11 (1.5%). 521 (72.8%) participants had no sexual partners (Table 1). The distribution of demographic characteristics, behavioural and history background of the study population related to HPV and cervical cancer is shown in Supplemental Table S1.
Knowledge on CC and HPV among the participants
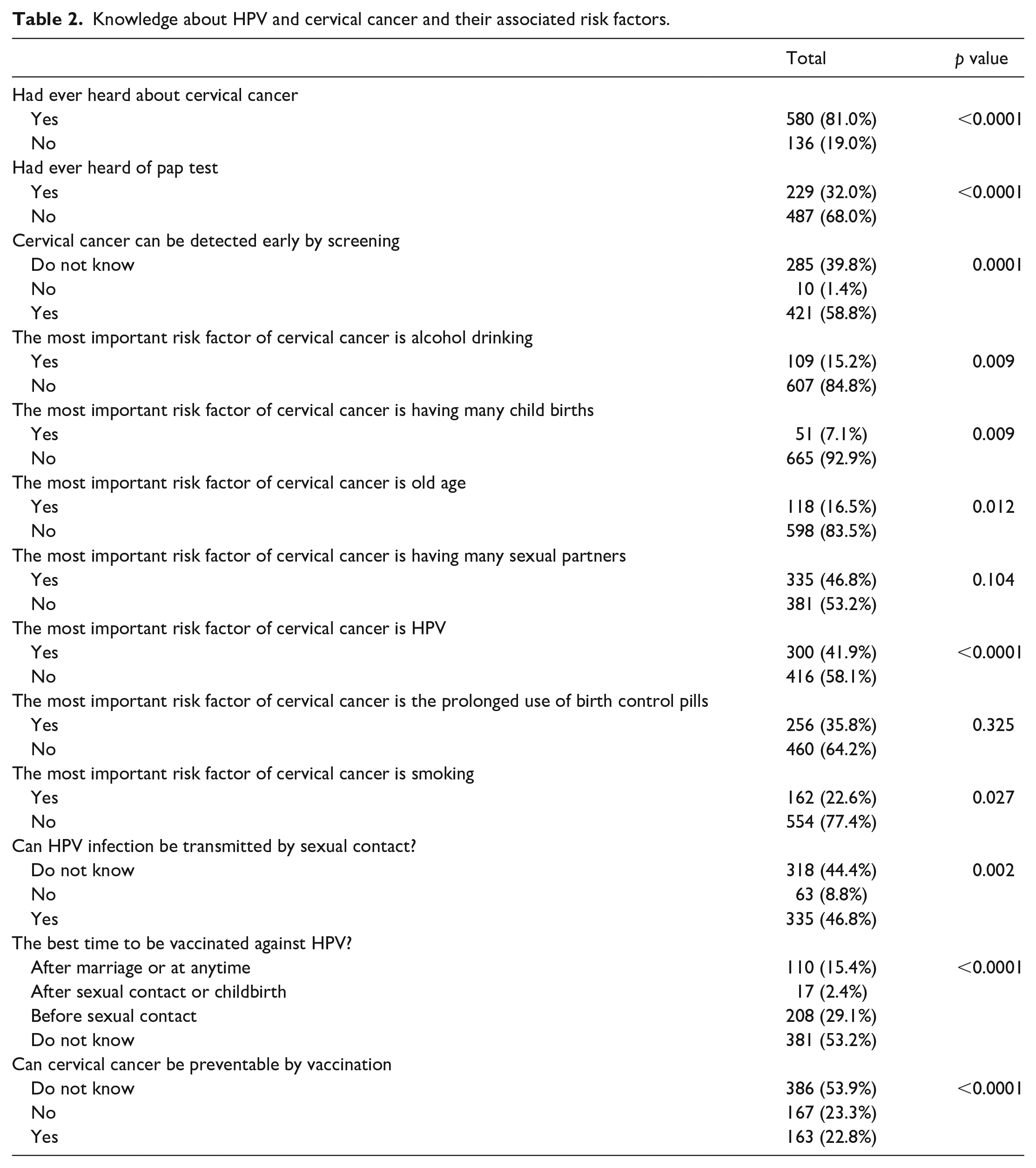
There were 580 (81.0%) participants who have heard about CC, and the remaining 136 (19.0%) reported no knowledge about it. However, 229 (32.0%) have heard about the Pap test. The knowledge about the early detection of CC by screening was known among 421 (58.8%). When we investigated the knowledge about risk factors for CC perceived by the participants, 109 (15.2%) assumed it to be related to alcohol drinking. In comparison, 51 (7.1%) attributed having CC to giving birth to many children, 118 (16.5%) to age, 335 (46.8%) to having many sexual partners, 300 (41.9%) to having HPV infection, 256 (35.6%) to the prolonged use of birth control pills, and 162 (22.6%) related to smoking.
The knowledge concerning the transmission of HPV through sexual contact was stated by 335 (46.8%) respondents. In contrast, 318 (44.4%) did not know about it. Regarding the best time to be vaccinated against HPV, 381 (53.2%) did not know; 110 (15.4%) reported the best time for vaccination is to be after marriage, 17 (2.4%) after first sexual contact or childbirth, and 208 (29.1%) considered the best time for vaccination is before the first sexual contact (Table 2). When we examined the knowledge of the participants about whether CC is preventable via vaccination, 163 (22.8%) answered yes, while 167 (23.3%) answered no, and 386 (53.9%) did not know about the prevention measures. Accordingly, the overall knowledge about HPV, CC, and their associated risk factors was significantly related to the participant’s age group; specifically, the age group between 20 and 30 years had the highest knowledge score among all other age groups (p-value < 0.001) (Table 3). In addition, the knowledge about CC and HPV was positively associated with the highest education levels; in university and post-university groups (p-value < 0.001) (Supplemental Table S2).
Knowledge about HPV and cervical cancer and their associated risk factors.
Correlation of the educational levels with the respondent sociodemographics and attitudes related to HPV and cervical cancer.

Attitudes of the participants towards CC and HPV
We asked the participants about their decision if they were offered free screening for CC. While 521 (72.8%) agreed to be screened, 112 (15.6%) did not respond, and 83 (11.6%) refused to be screened; 256 (35.8%) intend to be screened for CC within the next 3 years (Table 4). Respondents’ attitudes towards CC screening varied significantly among the different age groups. The willingness to participate in screening was highest among the age group of 21–30 years old (p-value < 0.001). Acceptance and willingness for screening were also highest among females with university and post-university-level education 109 (96%) (Supplemental Table S3).
Correlation of the educational levels with the respondent attitudes related to HPV and cervical cancer.

Nevertheless, 112 (15.6%) of study participants have expressed that their reason for refusing the CC screening was their psychological fear of finding out that they have cancer already. 29 (4.1%) were HPV vaccinated compared to 687 (95.9%) unvaccinated. The percentage of vaccine recipients was insignificantly associated with the age group (p-value 0.74). 473 (66.1%) reported willingness to receive a free HPV vaccine. The frequency slightly decreased to 52.9% (379/716) when asked whether they would be vaccinated even if they had to pay for it. Regarding the reason for vaccine refusal, 83 (11.6%) responded that they do not trust the vaccine safety, 75 (10.5%) considered there is no need to have the vaccine as they are not sexually active, 43 (6.0%) were due to the cost of vaccine might be very high (Supplemental Table S4).
The regression model to predict the effectors on participants’ knowledge and attitudes revealed that the influence resulted from the combination of occupation, educational level, family income, and marital status altogether than by each affecter separately, adjusted R square; [R 2 : 0.041, 0.017, and 0.006; Std: 1.527, 0.417, and 0.426] (Table 5).
Regression models to predict the sociodemographic effectors on participants’ knowledge and attitudes.

Discussion
The conventional Pap smear is one of the tools recommended for CC screening or initial diagnosis. In low- and middle-income countries (LMICs) such as Sudan, where no CC national surveillance programme is implemented, Pap smear use is mainly restricted for CC diagnosis. Therefore, the knowledge and attitudes of women in Khartoum state were assessed to evaluate the suitability and demand generation for implementing a CC surveillance programme with consideration to its preventable measures, mainly HPV vaccination. On April 2022, based on the Strategic Advisory Group of Experts on Immunization (SAGE) evaluation, the World Health Organization (WHO) declared that a single dose of HPV vaccine offers protection from CC. 30 The current WHO 31 strategy is to vaccinate at least 90% of females aged 15 or younger by 2030. Recently, the availability of the HPV vaccine and the massive development of screening programmes decreased the rate of CC-related mortality significantly in many countries. 27 Access to health centres providing CC screening and HPV vaccination is considered a main strategic intervention for preventing CC. According to the WHO guidelines for HPV vaccination, HPV DNA detection in a screen and treat and HPV DNA detection in a screen, triage, and treat approaches starting at the age of 30 years periodic screening every 5 to 10 years as main strategies for CC prevention among the general population of women. However, in Sudan, HPV vaccination is not included in the national vaccination schedule, leaving the community at risk of HPV infection and increased risk of developing CC. Moreover, the application of these health measures depends on the level of awareness among the general population, healthcare providers, and policymakers about the early detection of cancer and the available prevention measures. 21
In this study, more than half of the participants were unaware that CC is a preventable disease, with 68% had not heard about the Pap test. This indicates poor awareness regarding CC prevention and its screening programmes. These findings agree with several studies conducted in developing countries like Ghana, Ethiopia, and Iraq, where 3.3%, 28.79%, and 21.4% of those surveyed had heard about the Pap test, respectively.28,32,33 This highlights the need for extensive advocacy, public health promotion, and education about CC screening tools, especially the Pap test, by implementing educational content through campaigns, social media, or embedded within the academic curriculum of either primary or secondary schools. This method has been assessed and evaluated previously in Sudan to help malaria control by implementing how and when to use insecticide-treated bed nets and malaria treatment through health campaigns and school children’s education. 34 And to respect and protect religious beliefs and at the same time be able to reach global health coverage, prevention of CC in a community such as Sudan, deployment of HPV vaccination will provide prevention and reduce CC incidence due to HPV even if most of the community avoid CC screening.
According to Ferlay et al., 35 about 80% of CC death worldwide occurs in LMICs, where the level of awareness can be considered the main factor for reducing CC-related death. Despite the poor knowledge about the Pap test, CC early detection knowledge is relatively high (58.8%); it might be attributed to insufficient knowledge or behavioural beliefs and self-embarrassments. In facilities where a Pap test is performed, young girls over 18 years or at reproductive age avoid screening for CC as it leads to loss of virginity. Therefore, performing the test when required is only applicable to married women. this underscores the reporting of CC mostly among old-married or divorced women, such as reported previously by Demirtas and Acikgoz. 36 This underscores the inadequate application of the Pap test among primary health facilities, urging for more interventional strategies to increase motivation towards screening and promote regular cervical screening to increase public awareness about the Pap test and stimulate early detection of CC.
In this study, less than half of the participants reported having many sexual partners as a significant risk factor, and less (41.9%) cited HPV as the critical risk factor. These results align with a study conducted by Touch and Oh, 37 who demonstrated that having multiple sexual partners and HPV, were selected as the most risk factor for CC when assessing the knowledge of Cambodian females regarding CC. In addition, this is in line with the findings reported in South Africa and Iraq, in which 48.5% and 36.9% of the participants selected HPV as a causal factor.33,38 Interestingly, this is per scientific data indicating the direct relationship between sexual behaviour and CC as an eventual result of HPV transmission.39,40 According to a systematic review of 39 studies conducted in 11 countries, the overall understanding of the public regarding HPV and CC risk is poor. 41 However, several studies support that HPV is related to several other squamous epithelial carcinomas in Sudan,11,42,43 emphasizing that the gap between HPV aetiology in our study population and HPV awareness is still significant.
The age group of 20 to 30 years and those with university and post-university levels were associated with good knowledge. Respondents’ attitudes towards CC screening were also significantly better among this age group. However, respondents’ attitudes were insignificantly associated with education level. This finding is inconsistent with a Chinese study reporting that education level is the only significant factor related to positive attitudes. 44 Nevertheless, that study and ours agree that knowledge alone is insufficient for positive attitudes, and education is essential in improving awareness among the population.
According to vaccine status and attitudes, only 29 (4.1%) of the study participants had been vaccinated for HPV. This reflects a lower percentage of vaccinated women compared to international vaccine programmes targeting high coverage in developing countries which exceeds 85% in most of these countries. 45 However, 473 (66.1%) of the participants were motivated and ready to be vaccinated, while for those not vaccinated and not willing to get vaccinated, the most common reasons for refusal included lack of trust in vaccines and vaccine efficiency, indicating that knowledge about vaccine efficiency and safety at the national health facilities should be considered a barrier to HPV vaccine implementation in our population. Several studies have reported similar results indicating that dissemination of vaccine knowledge at a level that can be widely understood is a determining factor for vaccine implementation success.46–48
The limitations of this current study may include; the research participants were self-identified, and their enrolment in the study may be influenced by the restriction of their own awareness about the CC. Furthermore, this study is considered a cross-sectional study; hence, it cannot differentiate between the cause and effect across the variables.
Conclusion
Sudanese women have a low level of awareness of CC screening programmes; few attended CC diagnosis, but the willingness of participants to get the HPV vaccination was high. Therefore, by increasing the access to CC screening and advocate for HPV vaccination when available will substantially increase women’s awareness about CC and the benefits of early screening. This study recommends promoting health education for healthcare staff and women of reproductive age about the benefit of early CC screening to detect CIN and malignancy early and further introduces HPV vaccination campaigns in every healthcare facility to help reduce the morbidity and mortality of CC through the elimination of HPV.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231166286 – Supplemental material for Knowledge and attitudes towards cervical cancer prevention among women in Khartoum state, Sudan
Supplemental material, sj-docx-1-whe-10.1177_17455057231166286 for Knowledge and attitudes towards cervical cancer prevention among women in Khartoum state, Sudan by Emmanuel Edwar Siddig, Ayman Ahmed, Eiman Siddig Ahmed, Mona Ali Mohammed, Ezzan Kunna, Sarah M El-Sadig, Yousif Ali, Rana Alamin Hassan, Eman Taha Ali and Nouh Saad Mohamed in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057231166286 – Supplemental material for Knowledge and attitudes towards cervical cancer prevention among women in Khartoum state, Sudan
Supplemental material, sj-docx-2-whe-10.1177_17455057231166286 for Knowledge and attitudes towards cervical cancer prevention among women in Khartoum state, Sudan by Emmanuel Edwar Siddig, Ayman Ahmed, Eiman Siddig Ahmed, Mona Ali Mohammed, Ezzan Kunna, Sarah M El-Sadig, Yousif Ali, Rana Alamin Hassan, Eman Taha Ali and Nouh Saad Mohamed in Women’s Health
Supplemental Material
sj-docx-3-whe-10.1177_17455057231166286 – Supplemental material for Knowledge and attitudes towards cervical cancer prevention among women in Khartoum state, Sudan
Supplemental material, sj-docx-3-whe-10.1177_17455057231166286 for Knowledge and attitudes towards cervical cancer prevention among women in Khartoum state, Sudan by Emmanuel Edwar Siddig, Ayman Ahmed, Eiman Siddig Ahmed, Mona Ali Mohammed, Ezzan Kunna, Sarah M El-Sadig, Yousif Ali, Rana Alamin Hassan, Eman Taha Ali and Nouh Saad Mohamed in Women’s Health
Supplemental Material
sj-docx-4-whe-10.1177_17455057231166286 – Supplemental material for Knowledge and attitudes towards cervical cancer prevention among women in Khartoum state, Sudan
Supplemental material, sj-docx-4-whe-10.1177_17455057231166286 for Knowledge and attitudes towards cervical cancer prevention among women in Khartoum state, Sudan by Emmanuel Edwar Siddig, Ayman Ahmed, Eiman Siddig Ahmed, Mona Ali Mohammed, Ezzan Kunna, Sarah M El-Sadig, Yousif Ali, Rana Alamin Hassan, Eman Taha Ali and Nouh Saad Mohamed in Women’s Health
Supplemental Material
sj-docx-5-whe-10.1177_17455057231166286 – Supplemental material for Knowledge and attitudes towards cervical cancer prevention among women in Khartoum state, Sudan
Supplemental material, sj-docx-5-whe-10.1177_17455057231166286 for Knowledge and attitudes towards cervical cancer prevention among women in Khartoum state, Sudan by Emmanuel Edwar Siddig, Ayman Ahmed, Eiman Siddig Ahmed, Mona Ali Mohammed, Ezzan Kunna, Sarah M El-Sadig, Yousif Ali, Rana Alamin Hassan, Eman Taha Ali and Nouh Saad Mohamed in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.