
Abstract
Background:
Obstetric fistula (OF) is a severe and debilitating complication of childbirth that primarily affects women in developing countries, particularly the Democratic Republic of the Congo. It results in chronic urinary and/or fecal incontinence, often accompanied by social isolation, stigma, and psychological distress, thereby having a profound negative impact on the quality of life of affected women.
Objectives:
This study aims to evaluate the level of awareness and knowledge regarding OF among Congolese women of reproductive age in the North Kivu Province.
Design:
This is a community-based, cross-sectional study.
Methods:
A two-stage cluster random sampling method was employed to select a sample of 500 women aged 15–49 years. Data were collected using a pretested, semi-structured questionnaire administered through face-to-face interviews. The questionnaire gathered information on sociodemographic characteristics, reproductive history, and knowledge of OF. Data were analyzed using descriptive statistics and binary logistic regression to identify factors associated with a good OF knowledge.
Results:
The mean age of respondents was 33.7 ± 10.4 years. Among the 467 surveyed, 22.7% demonstrated good OF knowledge. Urban residence (adjusted odds ratio, aOR = 2.8, 95% CI [1.6–4.6]; p < 0.0001), being single (aOR = 2.6, 95% CI [1.3–4.6]; p = 0.0078), lack of professional occupation (aOR = 1.7, 95% CI [1.0–2.7]; p = 0.0407), use of family planning services (aOR = 1.9, 95% CI [1.2–3.2]; p = 0.0111), and personally knowing someone who had suffered from OF (aOR = 9.6, 95% CI [2.0–46.9]; p = 0.0052) were independently associated with good OF knowledge.
Conclusion:
The study revealed that a substantial proportion of women in North Kivu province have limited knowledge about OF. Strengthening awareness and education efforts, particularly in rural settings, is essential to promote early recognition of symptoms and timely care-seeking behavior. Targeted health education programs and community-based interventions are crucial to improving understanding and reducing the burden of this preventable condition. Moreover, identifying the determinants of good OF knowledge can inform the design of more effective prevention and intervention strategies at the elimination of this condition.
Plain Language Summary
Background:
Obstetric fistula (OF) is a serious childbirth-related injury. It typically occurs when a woman experiences a prolonged or obstructed labor without timely medical intervention. This condition is most common in low-income countries, especially in the Democratic Republic of the Congo (DRC). Women affected by OF experience constant and uncontrollable leakage of urine, feces, or both. This can severely impact their quality of life, leading to stigma, isolation, and other health problems.
Objective:
The goal of this study was to find out how much Congolese women aged 15 to 49 in the North Kivu Province know about OF.
Design:
This was a cross-sectional study conducted at the community level.
Methods:
Data were collected through face-to-face interviews using a well-prepared and pretested questionnaire. The questionnaire included questions on participants’ background, reproductive history, and knowledge of OF. The information was analyzed using descriptive statistics and multiple logistic regression to find out which factors were linked to good knowledge of OF.
Results:
The mean age of the women who participated was 33.7 ± 10.4 years. Out of the 467 women, 22.7% had good knowledge about OF. Women were more likely to have good knowledge if they lived in urban areas, were single, had no professional occupation, had used family planning services, or personally knew someone affected by OF.
Conclusion:
The study found that many women in North Kivu Province do not know enough about OF. Increasing awareness and education, especially in rural areas, through targeted health programs and community outreach, could help women recognize the symptoms early and seek appropriate medical care.
Introduction
Obstetric fistula (OF) is a devastating complication of childbirth, characterized by an abnormal communication between the genital tract and either the urinary or digestive tract, and is particularly prevalent in sub-Saharan Africa and Southeast Asia.1,2 These injuries most commonly occur during prolonged or obstructed labor, often when the fetus’s head becomes impacted in the maternal pelvis, leading to ischemia and subsequent tissue necrosis due to sustained pressure and impaired blood flow.3,4 The consequences of OF include persistent urinary and/or fecal incontinence, severe social stigma, and a reluctance to seek treatment, frequently due to limited awareness of available medical options. 5 This condition significantly affects the physical, psychological, and social well-being of affected women.6,7 Studies from Tanzania and Uganda 8 have shown that over 50% of women with OF delay seeking medical care for more than a year, thereby extending and reducing the chances to successful surgical repair.
In many cultural contexts, OF remains poorly understood, and erroneous beliefs persist. It is sometimes perceived as result of divine punishment, harmful traditional practices, curses, malevolent spirits, bad luck, or perceived immoral behavior by women.1,9,10 Such misconceptions fuel the stigmatization of women living with OF and contribute to barriers to timely healthcare access.4,11 In this context, the knowledge and perception of OF among women of reproductive age play a critical role in its prevention, early recognition, and timely access to appropriate care. A limited understanding of the condition may result in delayed healthcare-seeking, heightened social exclusion, and increased psychological distress among those affected. 12
Prevention of OF involves delaying the onset of pregnancy, eliminating harmful traditional practices, and ensuring timely access to skilled obstetric care. 13 A range of contributing factors has been identified, including the absence of trained birth attendants, poor maternal health-seeking behaviors, weak referral and transportation systems, and socioeconomic determinants such as poverty and low levels of education.2,4,14,15
In the Democratic Republic of the Congo (DRC), the incidence of OF remains among the highest globally. According to the 2007 Demographic and Health Survey, 16 an estimated 1–10 cases per 1000 live births occur, translating to approximately 42,000 untreated cases nationwide. Despite this alarming prevalence, the knowledge and perceptions of Congolese women of reproductive age regarding fistula remain poorly studied and insufficiently documented.
Evidence from other low-resource settings highlights diverse levels of awareness. For instance, in Ethiopia, a study by Tsega et al. 17 found that 36.4% of women surveyed demonstrated good knowledge of OF, with this knowledge being significantly associated with residence, level of education, and attendance at antenatal care and pregnancy forums. Similarly, in Burkina Faso, Banke-Thomas et al. 5 reported that rural women were significantly less likely to possess adequate preventive knowledge compared to their urban counterparts (OR = 0.35, 95% CI [0.16–0.79]).
This study aims to assess the level of knowledge about OF and its associated factors among Congolese women of reproductive age living in North Kivu Province, DRC. By addressing this gap, the study seeks to generate context-specific evidence that can inform the design of effective awareness campaigns, targeted interventions, and public health strategies to both prevent and manage this devastating condition.
Materials and methods
Setting, design, period, and study population
A cross-sectional, community-based survey consistent with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist 18 was conducted in North Kivu Province, located in the eastern region of the DRC, from April 1 to July 31, 2023. North Kivu is one of the 26 in the DRC, with an estimated population of 8,985,711 inhabitants. 19 The province comprises 31 health zones and 154 health facilities.
A two-stage cluster random sampling was carried out, with a minimum sample size of 422, calculated according to the following formula: n = z2 p(1 − p)/d2, with a 95% confidence interval (95% CI; z = 1.96), a prevalence (p) of 50% (due to the absence of data on the prevalence of good knowledge among women in the DRC), a margin of error (d) of 5% and a nonresponse rate of 10%. Although the initial sample size was calculated without incorporating a design effect due to lack of prior data on intra-cluster correlation, we increased the final sample size from 467 to 500 participants to partly account for clustering bias inherent in the two-stage cluster sampling design. In the first stage, we randomly selected two urban centers (Goma and Beni) and four rural villages (Mabalako, Lubero, Masisi, and Mweso) from the list of health zones in North Kivu province. Within each selected site, streets (in urban areas) and paths (in rural areas) were selected using systematic random sampling. Households were then selected randomly. In the second stage, one eligible woman of childbearing age (15–49 years) per household, who had resided in the area for at least 1 year, was randomly chosen to participate. Participants were required to understand and speak Swahili (the local language) well and to give written consent for the study to be included. They were included in the study regardless of their parity. Participants aged less than 18 had one of their parents to give consent on their behalf. Those who were seriously ill or unable to respond were excluded. Trained health professionals approached each selected woman at home, explained the study’s objectives and benefits, obtained her informed consent, and conducted face-to-face interviews using a pre-tested, semi-structured questionnaire.
Conduct of the survey
The study was conducted between April to July 2023. A semi-structured questionnaire, developed based on an extensive literature review and refined with input from subject-matter experts, was pretested with 20 women of reproductive age to assess clarity, cultural relevance, and linguistic appropriateness.
The data collection instrument was a semi-structured questionnaire consisting primarily of closed-ended questions. To ensure clarity and accuracy of responses—particularly given the varying literacy levels among participants—the questionnaire was administered through individual face-to-face interviews. These were conducted by experienced doctors and nurses who had been actively involved in OF care campaigns for several years. Prior to data collection, they received a focused briefing session on the study protocol and standardized administration procedures to ensure uniformity and accuracy. Prior to each interview, the study objectives and potential benefits were clearly explained, and informed written consent was obtained from each participant. The volunteer participants then responded to the questionnaire, which collected information on their sociodemographic background, reproductive history, and knowledge of OF.
The questionnaire consisted of three structured sections. The first section collected sociodemographic characteristics, including age, level of education, marital status, religion, occupation, and place of residence. The second section focused on obstetrical history, covering parity, place and mode of the most recent delivery, use of family planning, and whether participants had received any information or advice about OF. The third section assessed participants’ knowledge through five questions, addressing: (1) types of fistula, (2) signs and symptoms, (3) causes and risk factors, (4) prevention methods, and (5) management options. Each correct answer was received 1 point, and incorrect or “don’t know” responses were scored 0. A total score below 3 points was classified as poor knowledge, while a score of 3 or above indicated good knowledge of OF.
Statistical analysis
Data were entered into Microsoft Excel (Microsoft Corporation) and analyzed using STATA version 16 (StataCorp LLC). Descriptive statistics were used to calculate frequencies, proportions, means, and standard deviations. To assess the relationship between explanatory variables and the level of knowledge about OF, binary logistic regression was performed. Initially, bivariate analysis was conducted using the chi-squared test. Variables with a p-value <0.05 in bivariate analysis were included in the multiple logistic regression model to adjust for potential confounding factors. Adjusted odds ratios (aORs) with 95% CI were calculated. A p-values <0.05 was considered statistically significant.
Ethical considerations
This study was conducted in accordance the principles of the Declaration Helsinki on ethical standards in medical research. Ethical approval was obtained from the Medical Ethics Committee of the University of Goma (Approval number: UNIGOM/CEM/011/2022). All data were collected anonymously, and each participant provided informed written consent before participation, without receiving any compensation or incentive. For participants who were unable to read or write, the study details and consent form were explained orally in the local language, and consent was recorded via thumbprints as confirmation of agreement.
Results
Of 500 women of reproductive age initially targeted, 467 participated, yielding a response rate of 93.4%. The mean age of respondents was 33.7 ± 10.4 years, approximatively 20% aged between 30 and 34 years. Among the participants, 50.7% resided in rural areas, 70.2% were married, 57.4% were employed, and 39.4% identified as Catholic. Regarding educational attainment, 31.9% had no formal education, 40.0% had completed primary education, 13.9% attained secondary education, and 14.2% had pursued higher or university-level education (Table 1).
Sociodemographic background of the 467 participants in North Kivu Province.

Among the 467 participants, 40.5% were multiparous, while 50.3% grand multiparous. The most recent childbirth had occurred at home for 12.6% of women (59/467), with nearly half of them (28/59) citing lack of transportation or financial resources as the primary reason. Use of family planning services was reported by 33.8% of the participants. Only 22.7% (106/467) had ever received information about OF, with 55.7% (59/106) receiving it from health professionals, and 91.5% (97/106) outside of the context of pregnancy. Just over half (52.9%) of the women had attended a health education session on pregnancy and its complications, while only 1.7% reported personally knowing someone affected by OF (Table 2).
Obstetrical profile of 467 participants in North Kivu province.
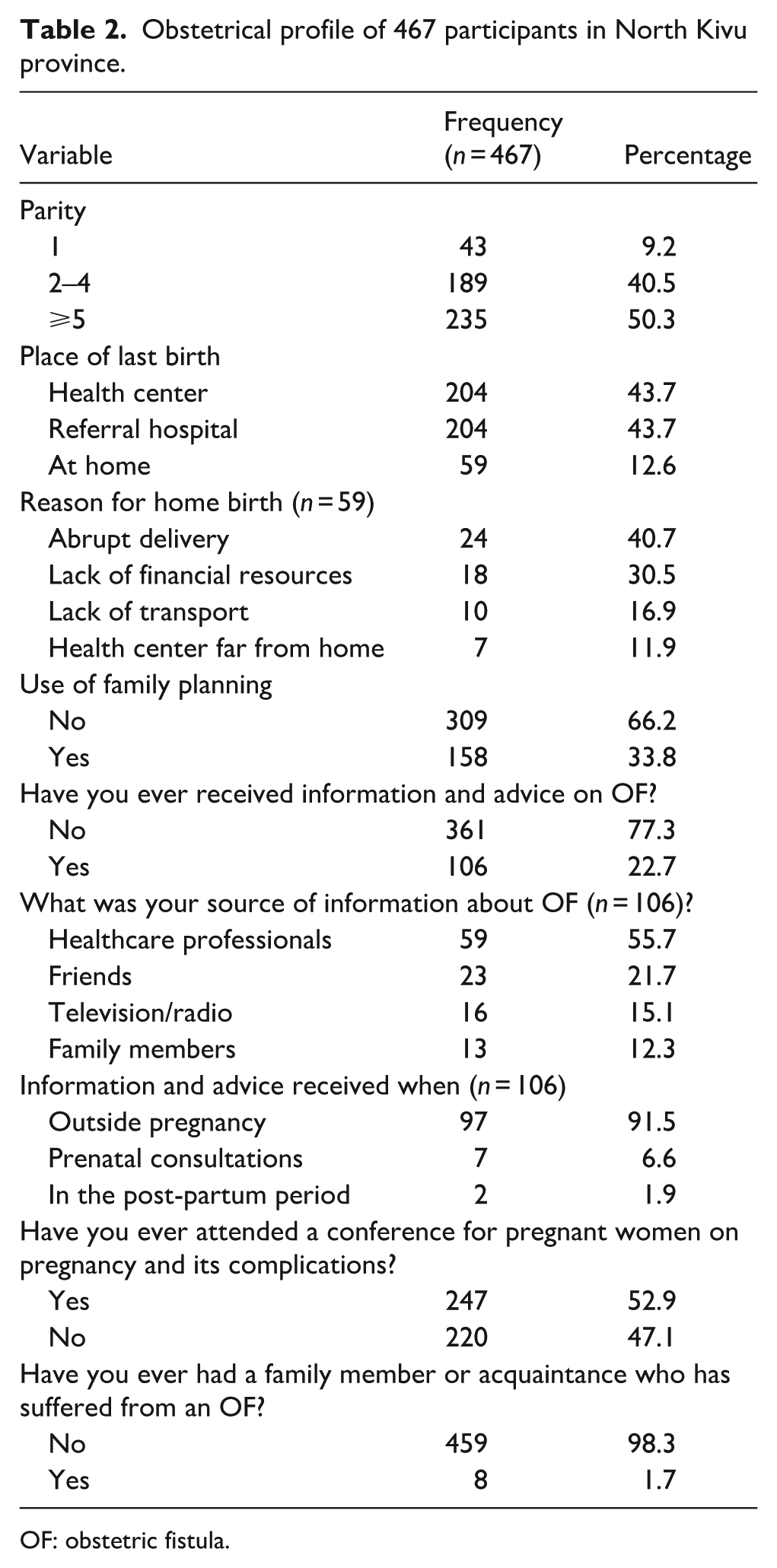
OF: obstetric fistula.
Among the 467 respondents, 106 women of childbearing age (22.7%, 95% CI: 19.1%–26.7%) demonstrated good knowledge of OF. Knowledge was assessed using five questions covering types, signs/symptoms, causes/risk factors, prevention methods, and management options. Each correct answer was scored 1 point, and incorrect answers 0 points. A total score of 3 points or more was classified as good knowledge, while a score below 3 indicated insufficient knowledge. Regarding knowledge of fistula types, 16.3% of participants recognized urogenital fistula, and 4.7% identified digestive fistula. The most frequently mentioned symptoms were urinary incontinence (12.6%), fecal incontinence (5.8%), and persistent urine odor (5.1%). Cited risk factors included obstructed labor (7.1%), prolonged labor (5.1%), lack of quality obstetric care (4.5%), and home delivery (4.3%). Regarding prevention, the most reported measures were receiving skilled care at birth (9.9%), seeking skilled obstetric care promptly (8.1%), abandoning harmful traditional obstetric practices (2.4%), and delaying the first pregnancy (1.9%). In terms of management, 22.7% of women knew that OF was treatable, and among those informed (106 women), 76.4% (81/106) could identify a health facility capable of managing fistula cases (Table 3).
Knowledge of obstetric fistula among the 467 participants in North Kivu Province.

OF: obstetric fistula.
Bivariate analysis revealed that place of residence, marital status, employment status, having a relative who had suffered from OF, and use of family planning services were all significantly associated with good OF knowledge (p < 0.05; Table 4).
Bivariate analyses of factors associated with good knowledge of obstetric fistula among 467 respondents in North Kivu Province.
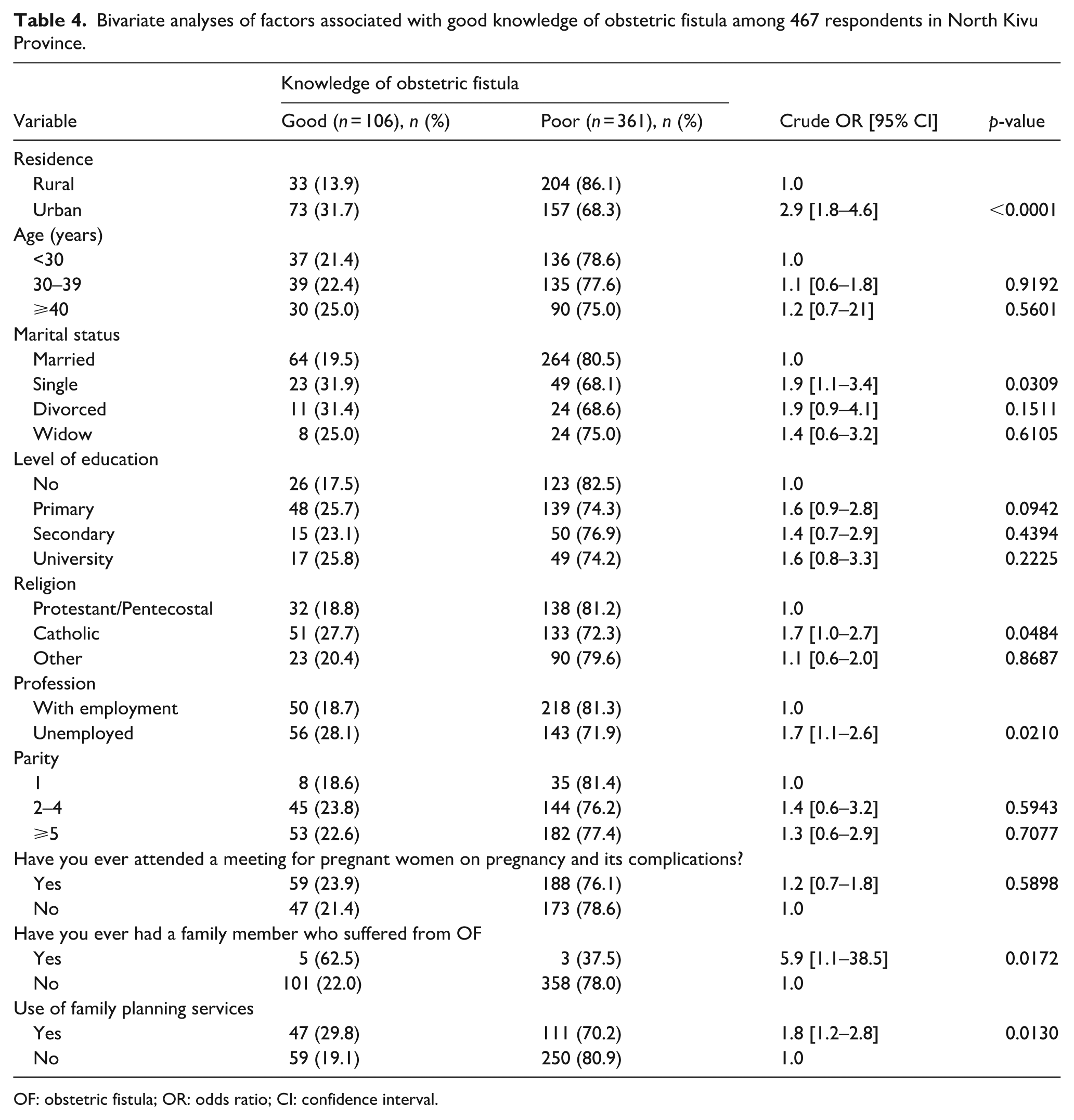
OF: obstetric fistula; OR: odds ratio; CI: confidence interval.
The multivariate logistic regression analysis confirmed that these five variables were independent predictors of good OF knowledge. Women living in urban areas were more than twice as likely to have good OF knowledge compared to those in rural areas (aOR = 2.4, 95% CI [1.5–3.9]; p < 0.0001). Single women had high odds of good OF knowledge than married women (aOR = 1.9, 95% CI [1.1–3.4]; p = 0.034). Similarly, unemployed women were significantly more likely to be informed than their employed counterparts (aOR = 1.7, 95% CI [1.1–2.7]; p = 0.027). The use of family planning services also associated with good OF knowledge (aOR = 1.9, 95% CI [1.2–3.2]; p = 0.007). Finally, participants who personally knew someone affected by OF were substantially more likely to have good OF knowledge, with odds 8.3 times higher than those who did not (aOR = 8.3, 95% CI [1.8–37.8]; p = 0.006; Figure 1).

Predictors of good knowledge of obstetric fistula among 467 participants in the North Kivu Province.
Discussion
This study assessed the level of knowledge about OF and its associated factors among women of reproductive age in North Kivu Province, DRC. Overall, only 22.7% of participants demonstrated good OF knowledge, a proportion that is higher than the 12.8% reported in Gambia, 20 but lower than figures observed in Ghana (29%), 14 Ethiopia (ranging from 36.4 to 53%),17,21–23 and Nigeria (57.8%). 24 These inter-country variations may attributed to differences in sample sizes, educational levels, and the sociodemographic characteristics of the populations studied. Additionally, some countries have integrated OF management and prevention into primary healthcare systems, which may contribute to greater public awareness and understanding of the condition.
Findings of this study revealed a significant disparity in OF knowledge between urban and rural women, with urban residents being more than twice as likely to have good OF knowledge (aOR = 2.4, 95% CI [1.5–3.9]). This result is consistent with the study by Tsega et al. 17 in north-west Ethiopia, where urban residents had good OF knowledge (aOR = 3.19, 95% CI [1.33–7.66]). Similarly, Banke-Thomas et al. 5 in Burkina Faso reported that rural women were nearly three times less informed than urban counterparts. These findings underscore the persistent geographical disparities in access to health information. Women living in urban areas are often benefit from better access to reproductive health services, more frequent exposure to media campaigns, and closer proximity to health facilities, which collectively enhance awareness and understanding of OF. Conversely, women in rural settings may face limited access to health education, fewer trained health providers, and cultural or logistical barriers to care. Therefore, targeted public health interventions are essential to bridge this urban–rural gap. Policymakers should prioritize community-based education campaigns, integration of OF education into antenatal and postnatal services, and capacity building of rural health workers to disseminate accurate and culturally adapted information on OF.
The study found that single women were 1.9 times more likely to be knowledgeable about OF than those who were married or divorced (aOR = 1.9, 95% CI [1.1–3.4]; p = 0.034). This finding suggests that single women may have greater exposure to health information or may perceive and engage with health topics differently than women in marital relationships. They may also have more autonomy or time to access reproductive health education. However, these results contrast with those of Tweneboah et al., 20 who reported that single women were 46% less likely to be informed about OF than married women (aOR = 0.54, 95% CI [0.47–0.62]). This discrepancy underscores the importance to contextual and cultural factors in shaping access to health information. It highlights the need to tailor awareness campaigns based on marital status, taking into account how social roles, relationship dynamics, and sources of information may differ between single and married women.
Findings of this study also showed a significant association between women’s occupational status and their knowledge of OF. Women who were unemployed were 1.7 times more likely to have good OF knowledge than those who were employed (aOR = 1.7, 95% CI [1.1–2.7]). One possible explanation is that unemployed women have more time and flexibility to seek out health information or participate in health education activities. In contrast, work-related demands may limit employed women’s opportunities to engage with such resources. Interestingly, these findings do not align with those of Azanu et al., 14 who found that employed women were nearly five times to have heard about OF compared to those who were unemployed or housewives. The authors of that study suggested that employed women may face few financial barriers, increasing their access to antenatal care services, where health education about OF is often provided. 14 These contrasting results emphasize the complexity of socioeconomic and contextual determinants of health knowledge. They suggest that occupational status alone does not fully explain disparities in OF awareness and should be interpreted in conjunction with other factors such as health system engagement, media exposure, and community-level education efforts.
This study demonstrated a significant association between the use of family planning services and women’s knowledge of OF. Women who had used family planning were more likely to be well informed about OF than those who had not. This relationship suggests that family planning consultations may serve as valuable platforms for reproductive health education, including awareness on the risk factors and consequences of OF. Regular engagement with these services likely facilitates exposure to health information through interactions with trained providers. These findings are in line with previous studies, which have shown that women receiving antenatal care are more likely to have good OF knowledge.14,17,22,25 Antenatal and family planning services often include counseling sessions, where health professionals can discuss maternal complications, thereby improving awareness. However, it is essential to interpret this association with caution, as it does not necessarily imply a direct causal relationship. Other confounding factors, such as educational level, socioeconomic status, and general access to healthcare, may influence both the use of family planning and the level of knowledge about OF.14,17
Furthermore, the study identified that having a close contact—such as a family member or friend— who had experienced OF was one of the strongest predictors of good OF knowledge. Participants who reported such personal exposure were 8.3 times more likely to be well informed about the condition (aOR = 8.3, 95% CI [1.8–37.8]). This finding underscores the critical role of lived experiences in shaping understanding. Firsthand accounts may increase awareness of the clinical manifestations, causes, prevention strategies, and treatment options for OF, and may also promote empathy and reduce stigma within communities. These results highlight the importance of leveraging both formal healthcare encounters and informal social networks to disseminate accurate information about OF. Integrating peer-led education or testimonies from survivors into health campaigns may further strengthen community awareness and improve early care-seeking behavior.
This study is strengthened by its community-based design, inclusion of both urban and rural participants, use of probability sampling, and a scientifically validated sample size determination method, enhancing its validity and generalizability. It is also the first study in North Kivu to assess knowledge of OF among women of reproductive age—a high-risk group. However, several limitations should be noted.
The study has some limitations. The cross-sectional design prevents establishing causal relationships, allowing only associations. Self-reported data may be subject to recall or social desirability bias, particularly for sensitive topics such as family planning or fistula. The study was limited to selected health zones, which may affect the generalizability of findings. Stigma surrounding OF may have led to underreporting, and the knowledge assessment, based on only five questions, may not fully reflect participants’ understanding. Despite these limitations, the study offers valuable evidence to guide targeted awareness and prevention strategies of OF.
Conclusion
This study revealed that, in North Kivu Province, the overall level of knowledge about OF among women of reproductive age remains alarmingly low, with fewer than one in four women demonstrating adequate understanding of the condition. Multivariate analyses identified several factors significantly associated with better OF knowledge, including being single, unemployed, urban residence, prior use of family planning, and knowing someone personally affected by OF. These findings underscore the urgent need for targeted and context-specific interventions aimed at improving awareness and knowledge of OF. Educational strategies should be tailored to the socio-cultural context of the region and designed to reach vulnerable populations, particularly rural women who are often most at risk. Efforts should prioritize the development of community-based health education programs, incorporating tools such as awareness campaigns, interactive group discussions, and collaboration with local leaders, health workers, and survivor advocates to promote early recognition and appropriate care-seeking behaviors. Moreover, improving access to reproductive health services—including antenatal care and family planning—and addressing harmful traditional practices, such as female genital mutilation, are essential components of a comprehensive strategy to prevent OF and mitigate its consequences. Ultimately, bridging the knowledge gap is not only a matter of health education but also of health equity and human rights. Strengthening public awareness and facilitating access to care are key to reducing the burden of OF and restoring dignity to the affected women.
Footnotes
Acknowledgements
The authors are thankful to all the members of the communities who participated in this study. Also, the authors would like to thank all the individuals and corporate bodies who provided the means that help to tackle obstetric fistulas in the DRC.
Ethical considerations
This study was carried out under consideration of the Helsinki Declaration of Medical Research Ethics. The study was authorized by the Medical Ethics Committee of the University of Goma (Approval number: UNIGOM/CEM/011/2022).
Consent to participate
All data were collected anonymously. Each participant gave informed written consent prior to the interviews, without any form of compensation or inducement. Written consent was obtained using a form validated by the medical ethics committee. For those who could not read or write, the details of the study and the consent form were explained verbally in the language best understood, and their thumbprints were collected as confirmation of their agreement. Participants aged less than 18 had one of their parents to give consent on their behalf.
Consent for publication
Not applicable.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.