
Abstract
Background:
Obstetric fistula, a preventable consequence of prolonged obstructed labor, inflicts profound physical, psychological, and social suffering, leaving many women described as “living dead.” In Ethiopia, where the burden remains high, little is known about women lived experiences and coping strategies beyond clinical outcomes. This review was conducted to synthesize qualitative evidence, illuminate these challenges, and inform holistic interventions.
Objectives:
To synthesize available evidence on the lived experiences and coping mechanisms of women with obstetric fistula in Ethiopia.
Design:
This study employed a qualitative meta-synthesis approach.
Data sources and methods:
This review was conducted in accordance with the Joanna Briggs Institute systematic review and meta-synthesis methodological guidance and reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. ATLAS.ti software, Version 25, Lumivero was used for analysis. A comprehensive literature search was performed across multiple databases up to May 25, 2025, including both published and unpublished studies examining the lived experiences of women with obstetric fistula. All eligible studies were critically appraised using the Critical Appraisal Skills Program to ensure methodological rigor. Data were systematically extracted and analyzed using thematic synthesis, and the results are presented through tables, narrative summaries, and illustrative diagrams, providing a coherent and evidence-based synthesis of women’s experiences and coping mechanisms.
Results:
Eight studies met the inclusion criteria, encompassing the diverse experiences of women with obstetric fistula in Ethiopia. Four major themes were developed: physical challenges such as pain, foot drop, odor, and urinary incontinence; psychological challenges including hopelessness, grief, and suicidal ideation; socioeconomic challenges like stigma, isolation, divorce, loneliness, social disintegration, and economic difficulties; and coping mechanisms such as self-isolation and wearing multiple layers of clothing.
Conclusion:
Women with obstetric fistula face intersecting physical, psychological, and socioeconomic burdens that erode dignity and social participation. Coping strategies such as self-isolation and layering clothes, while adaptive, often reinforce stigma and exclusion. These findings highlight the need for comprehensive interventions that go beyond surgical repair to include psychosocial support, stigma reduction, and economic reintegration programs.
Registration:
Registered with PROSPERO 2025 CRD420251064015.
Plain language summary
In Ethiopia, thousands of women live with a hidden injury -an obstetric fistula - that silently devastates their bodies, mind, and social lives. Caused by prolonged, obstructed labor without timely medical care, this condition leads to uncontrollable leakage of urine or feces. But the suffering doesn’t stop there. These women are often abandoned by their families, divorced by their husbands, and excluded from their communities. Many describe themselves as “living dead,” trapped in shame, isolation, and despair. Some wear layers of clothing to hide the wetness and odor. Others retreat from society altogether, avoiding markets, churches, and even their own relatives. This study brings together voices from across Ethiopia eight qualitative studies that reveal the raw, unfiltered experiences of women with obstetric fistula. The findings are clear: Physically, they endure pain, sores, foot drop, and constant wetness. Psychologically, they face hopelessness, grief, and suicidal thoughts. Socially, they suffer stigma, loneliness, and economic hardship. To cope, they isolate themselves and use improvised methods to manage their condition. But these strategies, while understandable, often deepen the problem delaying care and reinforcing exclusion. This review calls for urgent change. Healing must go beyond surgery. Women need mental health support, economic empowerment, and community reintegration. Obstetric fistula is not just a medical issue it’s a matter of dignity, justice, and equity.
Introduction
Obstetric fistula is an abnormal tear that forms between the vagina and the rectum and/or bladder, typically resulting from prolonged and obstructed labor. 1 It is regarded as one of the most severe maternal health complications. The continuous leakage of urine, feces, or both often leads to women with fistula being abandoned and socially excluded. 2 The profound physical and psychological distress caused by the condition significantly diminishes their quality of life, to the extent that they are often referred to as “living dead.” 3
Obstetric fistula is a preventable cause of maternal morbidity which affect between 50,000 and 100,000 women worldwide each year. 4 In regions such as sub-Saharan Africa and Southeast Asia, where access to adequate and timely obstetric care is limited, it is estimated that over 2,000,000 young women live with untreated obstetric fistula. 5 Although obstetric fistula is most prevalent in sub-Saharan Africa and Southeast Asia, cases have also been documented in Latin America, albeit less commonly. 5 In addition, incidence of obstetric fistula has been estimated to be about 124 cases per 100,000 deliveries in sub-Saharan Africa. 4
Ethiopia faces a particularly high burden of obstetric fistula due to its persistently high fertility rate and limited access to skilled maternal care, with more than half of births (52%) occurring without professional assistance. Compounding this, nearly 80% of the population resides in rural areas where poverty, malnutrition, and geographic isolation intersect to heighten women’s vulnerability. 6 These structural inequalities not only increase the risk of obstructed labor but also hinder timely access to life-saving interventions, thereby sustaining one of the highest global burdens of obstetric fistula. For instance, from 2010 to 2013, on average, about 2000 women with fistula had surgery every year in Ethiopia. 7
The continuous and uncontrollable leakage of urine and/or feces often results in severe stigmatization for women living with fistula. 8 As a result, these women experience ongoing distress and anxiety about their future. 2 The impact of obstetric fistula is devastating not only for the affected women but also for their families.9,10 Beyond the physical health challenges, the social repercussions are profound women with fistula are frequently ostracized by their communities, abandoned by their spouses, divorced, and often remain helpless.11,12 In many cases, community members blame these women for their condition, perceiving it as a punishment for sin, a venereal disease, or a curse. 12 Consequently, women with fistula are often excluded from religious ceremonies and social events, as they are viewed as unhygienic and impure. 3
Despite growing recognition of the devastating physical, social, and psychological impacts of obstetric fistula, there remains a significant gap in understanding the lived experiences and coping mechanisms of affected women from a comprehensive, evidence-based perspective. In this context, lived experiences refer to the personal, subjective realities of women navigating obstetric fistula, including the emotional, social, and relational challenges of the condition. 13 Coping mechanisms refer to the strategies, behaviors, and resources women employ to manage, adapt to, or mitigate the challenges imposed by obstetric fistula.13,14
Most existing reviews have focused narrowly on clinical outcomes or isolated social consequences. While some reviews have examined general knowledge or the overall burden of obstetric fistula, they seldom provide an integrated synthesis of how women actively navigate these multifaceted challenges over time.15 –17 This lack of comprehensive evidence hinders the development of interventions that address not only the medical but also the psychosocial needs of women living with fistula.
Therefore, this review aims to qualitatively synthesize available evidence on the lived experiences and coping mechanisms of women with obstetric fistula, systematically combining qualitative findings across diverse settings, identifying diverse experience and generating robust, culturally sensitive insights. By doing so, it seeks to inform holistic care strategies that improve both health outcomes and overall quality of life, filling a critical gap left by prior reviews that focus solely on disease burden or general knowledge.
Review questions
What are the psychological, physical, and socioeconomic experiences of women living with obstetric fistula in Ethiopia?
What coping mechanisms do women with obstetric fistula in Ethiopia employ to manage their condition and its associated challenges?
Methods
Protocol and registration
A rigorous systematic review of qualitative studies was conducted following the Joanna Briggs Institute systematic review and meta-synthesis methodological guidance. 18 This review adhered to a pre-registered protocol in the PROSPERO database (Registration Number PROSPERO 2025 CRD420251064015), ensuring transparency and methodological integrity. The reporting of findings aligns fully with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (see Supplemental Table 1), 19 providing a structured and comprehensive synthesis of evidence on the lived experiences and coping mechanisms of women with obstetric fistula.
Search strategy
We conducted a comprehensive search for both published and unpublished studies examining the lived experiences of women with obstetric fistula in Ethiopia. No restrictions were placed on the publication date in order to capture the full breadth of qualitative evidence ever produced on this issue. This inclusive approach was essential to ensure that earlier studies, which may reflect historical contexts and long-term trends, were not overlooked, while also incorporating more recent evidence that reflects current health system dynamics and social realities. A step-by-step search strategy was utilized in this review. Primarily, electronic databases related to health systems research, including PubMed, Scopus, ScienceDirect, and google scholar, were searched. Unpublished works were also sought from Google Scholar and university repositories for dissertations and theses. Additionally, hand-searching reference lists and citation tracking of included studies were performed to identify further relevant studies. The search was conducted independently by two authors (YA and DB) using three main categories of keywords related to the review question, Medical Subject Headings (MeSH), and employing Boolean operators “OR” and “AND.”
The main keywords used for the article search included for instance on PubMed: (“obstetric fistula” OR “vesicovaginal fistula” OR “rectovaginal fistula” OR “female genital fistula”) AND (“lived experience” OR “personal experience” OR “patient perspective” OR “women’s perspective” OR “narrative” OR “phenomenology” OR “qualitative research” OR “qualitative stud” OR “interview” OR “focus group*” OR “thematic analysis” OR “grounded theory”) AND (“patient” OR “woman” OR “women” OR “survivor” OR “victim”) AND “Ethiopia.” The initial database searches were conducted from April 10, 2025, to May 10, 2025, and updated on May 25, 2025. To develop review question PerSPecTIF Question formulation framework for qualitative evidence syntheses was used (Table 1). 20
PerSPecTIF question formulation.

Eligibility criteria
The eligibility of studies for inclusion in this systematic review was carefully determined based on predefined inclusion and exclusion criteria (Table 2). The study selection process was guided by the PICo framework, highlighting the main elements of the research question: the Population (patient with obstetrics fistula, their family members), the phenomenon of Interest (lived experience), and the Context (Ethiopia).
Inclusion and exclusion criteria.

Study selection
Search results were imported into Rayyan, Rayyaan System Inc, where duplicate records were identified and removed. Two authors independently screened and abstracted the records using Rayyan, Rayyan System Inc. 21 The first stage involved screening titles and abstracts to identify relevant studies and exclude those that did not meet the review question and eligibility criteria. This stage was carried out by two authors (YA and DB), with each article independently reviewed by two of them. In cases of disagreement, the issue was carefully discussed to reach consensus with third person among the review team (RD). Each abstract was thoroughly evaluated to decide whether the full article should be assessed in the second stage. The same authors conducted the full-text screening, including detailed evaluation against the inclusion and exclusion criteria. Studies that all authors agreed upon were included, while any discrepancies were resolved through discussion. Subsequently, the selected full-text articles were extracted for data collection and underwent quality assessment. The study selection process was documented using a PRISMA 2020 flow diagram, which clearly illustrated the number of studies screened, excluded, and included, along with reasons for exclusion at the full-text stage (Figure 1). The database was searched for every article published on lived experience of women with obstetric fistula in Ethiopia till May 20, 2025, and continued to update until we sent it for publication. The data were extracted from April 1 to 20 and later analyzed from May 1 to 20 and the report generation till May 20, 2025.

Flow diagram of included studies.
Quality appraisal
All studies that met the criteria during the full-text review underwent a quality assessment using the Critical Appraisal Skills Program checklist specifically designed for qualitative research. 22 This tool includes 10 questions that examine various aspects such as the clarity of research objectives, appropriateness of methodology and design, recruitment procedures, data collection and analysis methods, reflexivity, ethical issues, results, and overall contribution of the study. Each item is scored as: Yes (1.0 point), Partial Yes (0.5 points), or No (0 points). Based on their total scores, studies were classified into three quality levels: high quality (9.0–10.0), moderate quality (7.5–8.5), and low quality (7.0 or below). The assessment was independently performed by two reviewers (YA and DB), and any differences in scoring were resolved through discussion. Notably, the purpose of this appraisal was to highlight possible limitations within the research rather than to exclude studies from the review (Supplemental Table 2).
Data extraction
Two authors (YA and DB) independently extracted data from eligible studies using a tailored data extraction form. The system was set up so that data from each included study were extracted by two authors. Authors then reviewed and verified the accuracy of the extracted data by comparing the side-by-side outputs from the two authors. The extraction form collected information such as the first author, publication year, region where the study was conducted, study objectives, focus areas, study design, setting, study period, data sources or perspectives, sample size, sampling methods, data collection techniques, data analysis methods, and results pertinent to the review question (lived experience). Sample of data extraction table is shown in supplemental file (see Supplemental Table 3).
Data synthesis
We performed a qualitative evidence synthesis following the thematic synthesis method outlined by Thomas and Harden. 23 Thematic synthesis is a variation of thematic analysis, commonly used for analyzing primary qualitative data. It involves becoming thoroughly familiar with the data, coding findings from primary studies, developing themes, and using these themes to generate deeper insights and hypotheses. 23 To develop our initial coding framework, we selected four high qualities13,24 –26 studies from the included pool, chosen for their rigorous methodologies, clear results relevant to our synthesis questions from diverse perspectives, and precise use of terminology. We then applied line-by-line “free” coding to facilitate the translation of concepts across studies and to expand our codebook as we reviewed additional studies and themes. Themes and sub-themes were generated by incorporating direct participant quotes and summaries provided by the original study authors in their findings. Codes labels or categories used to group similar data segments were organized into clusters or overlapping themes. These overlapping themes, representing shared ideas across multiple codes, were merged into broader themes, which were then further categorized and synthesized. Ultimately, the identified themes related to lived experience and coping mechanisms were organized according to the biopsychosocial model, classifying them into physical, psychological, and social (Figure 2). The synthesis was conducted by two authors (YA and DB), who also selected illustrative participant quotations to support the thematic structure. All data handling and coding were performed using ATLAS.ti, Version 25, Lumivero. The result was presented in tables, text, and diagram as proper.

Biopsychosocial model description of challenges in the lived experience of women with obstetric fistula and their coping mechanisms in Ethiopia.
Results
Study selection
A total of 798 records were retrieved from database searches and additional sources, yielding 476 unique records after duplicates were removed. Following title and abstract screening, 19 articles remained for full-text review, of which 8 studies met the eligibility criteria. The screening and selection process is presented in the PRISMA flow diagram (Figure 1). The included studies represent diverse settings across Ethiopia, offering a comprehensive view of the lived experiences of women with obstetric fistula.
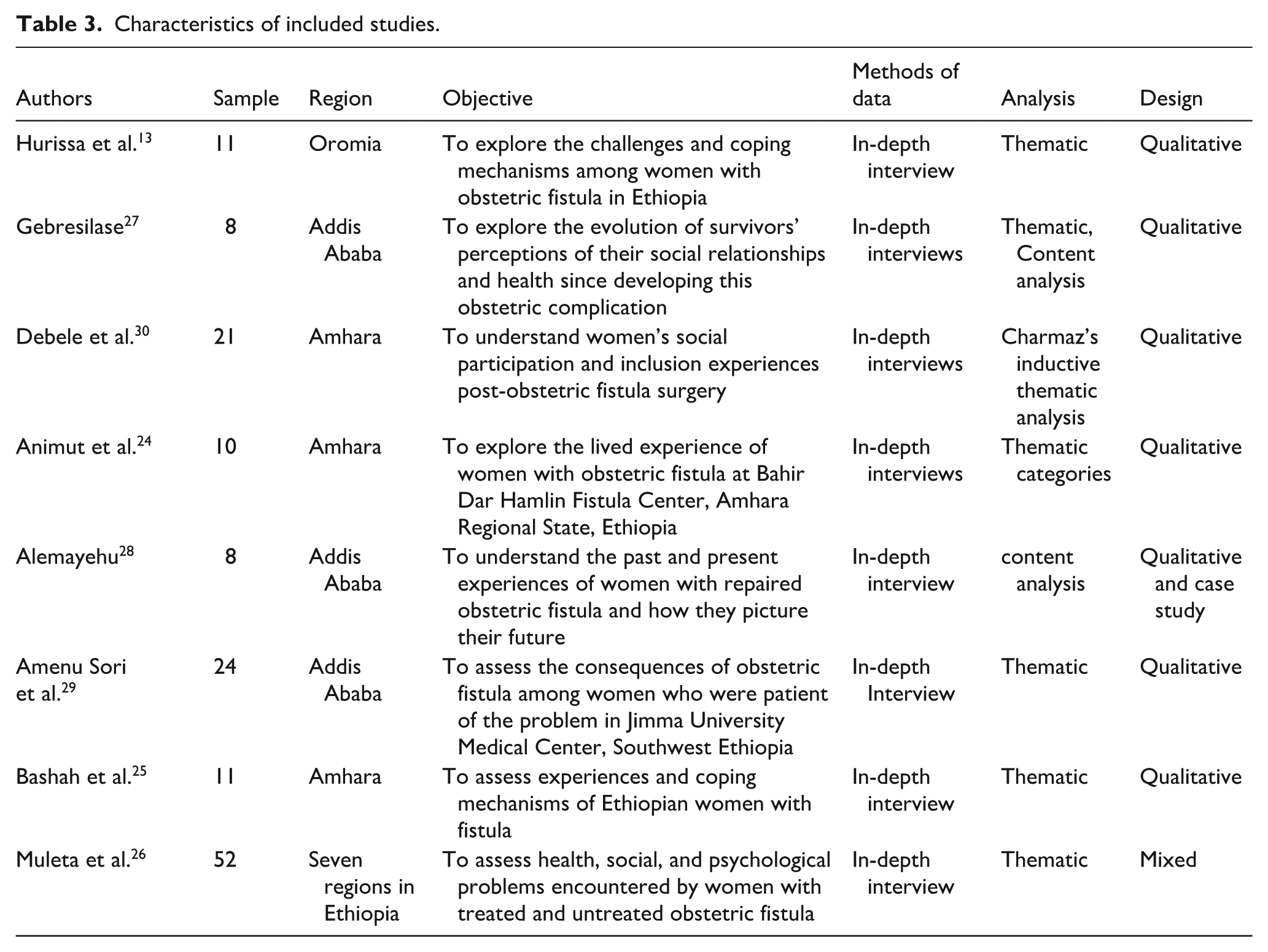
The foundational work by Muleta et al. 26 employed a mixed-methods design both qualitative and quantitative to explore the health and social challenges faced by women with fistula across seven regions of Ethiopia. This was the only mixed-methods study included in this review. Hurissa et al. 13 conducted a qualitative study at five fistula centers: Jimma University Medical Center, Asella Hospital, Harar, Mettu, and the Addis Ababa Hamlin Fistula Center. Bashah et al. 16 carried out their study at Gondar Specialized Referral Hospital Fistula Center, while Gebrselassie 27 conducted research in Addis Ababa. Two included studies were unpublished: Alemayehu 28 is available in a university repository, and another by Amenu Sori et al. 29 was retrieved from a preprint server; both were included despite not being peer-reviewed. Animut et al. 24 conducted their study in northern Ethiopia at the Hamlin Fistula Center in Bahir Dar, while Debele et al. 30 carried out research at both the Hamlin Fistula Center in Bahir Dar and Gondar Specialized Hospital in the Amhara Region. Details of the included studies are summarized in Table 3.
Characteristics of included studies.
Meta-synthesis of challenges and coping mechanisms of women with obstetric fistula in Ethiopia
During the synthesis of evidence from the qualitative studies included in this review, 4 main themes and 14 sub-themes were identified (see Table 4). Illustrative quotes, along with the detailed themes and sub-themes, are provided in Supplemental Table 3.
Summary of themes and subthemes of meta-synthesis.

Challenges in the lived experience of women with obstetric fistula
Physical challenges
Incontinence
Four studies13,24,25,29 consistently identified urinary incontinence as one of the most distressing sequelae of obstetric fistula. Initially, some women interpreted the leakage as a temporary or self-limiting problem; however, symptoms typically worsened over time.
25
In some communities, the condition was misattributed to cultural explanations such as “sunstroke (cultural conception which encompass various interpretations of illness related to heat exposure).”
31
Women described the continuous flow of urine as severely disrupting their sleep and daily functioning:
“I am passing urine continuously day and night. I can’t get good sleep. My sleeping ‘Agoza’ (local sleeping place made of animal skin) is always wet. Sometimes, I prefer to lie on the bare ground rather than on the ‘Agoza’. I would prefer to live a healthy life for five years than die having lived with this problem for 20 years”
24
Genital pain and sores
Persistent wetness from leakage often resulted in painful genital sores, burning sensations, and itching.13,24,25,28,29 These physical complications contributed to social withdrawal, as women sought to conceal their suffering and avoid public scrutiny. One participant described:
“. . .When I wash clothes, I experience a burning sensation in my vagina. It burns me like a flame in my vagina and inner thighs. . .” (Woman with fistula, 30 years).
13
Odor
The constant leakage of urine or feces led to an unpleasant odor, which participants described as socially devastating.13,28,29 This odor functioned as a visible marker of illness, provoking gossip, ridicule, and rejection within communities. The resulting embarrassment compelled women to withdraw from social life, reinforcing their isolation and psychological distress:
“Everybody covers their nose and mouth and starts to talk about me when they look at me. At that time, my mind is disturbed very much, I feel bad, lonely most of the time, and preferred to die. I couldn’t buy and sell due to fear of people’s facial expressions. I didn’t see any women like me before, who have the same problem. I always talk to myself about why I am the only woman who suffers from this problem. Why? . . .” (Divorced woman with fistula, 35 years).
13
Foot drops
Nerve damage, compounded by genital sores and prolonged immobility, was reported to cause complications such as foot drop, numbness, and leg deformities.13,27 –29 These conditions severely restricted mobility and independence, limiting women’s ability to perform daily tasks or generate income.
Psychological challenges
Suicidal ideation
Several studies24,26,29 documented suicidal thoughts among women living with fistula, often linked to feelings of incurability, neglect, and social abandonment. Divorce and return to natal families heightened dependency and despair. Some women reported attempted suicide, sometimes prevented by relatives:
“I was thinking that I shouldn’t be alive as inferior of human being. I had to take some toxin drugs and die. (Her eyes filled with tears). After a while, I became improved to some extent; at least I could walk, eat and drink by myself following the treatment.” “Even I cannot sit close to my mother and father. I tried to kill myself for several times. (Crying. . .) Once a day, my father stopped me while I tried to take rat killer (toxic substance).”
24
Hopelessness
The perceived incurability of fistula, coupled with marital breakdown and reliance on others, fostered deep hopelessness.24,28,29 Women frequently expressed pessimism about the possibility of remarriage, childbearing, or recovery even after multiple surgeries. This sense of lost future intensified their emotional suffering:
“Even a wild animal does not deserve this. Let God not give this to a wild animal.”
Grief due to child loss
Three studies16,24,28 highlighted compounded grief from perinatal loss associated with obstructed labor. Women not only endured fistula but also mourned the death of their infants, describing this as a “double burden.” In some accounts, fistula was attributed to delayed or instrumental delivery.16,24
Socioeconomic challenges
Divorce
Divorce emerged as a recurrent theme across studies.13,24,26,28,29 Initially, some husbands separated sleeping arrangements in anticipation of recovery; however, prolonged illness often led to abandonment. Despite women’s attempts to maintain their marital role, most were eventually divorced and replaced by “healthy” wives:
“. . .My husband used to love me very much; he usually says, ‘I can’t live without you;’ I do the same. But, after I faced this problem, he ignored me saying, ‘you are not healthy and no more important to me;’ and he has married and now living with another healthy woman; but I remained with my problem, and he never asked me at least. I am left alone with nothing; I don’t even have a single hen. Thanks to my father that I am alive till today. . .. . .” A 36 years old mother, who faced fistula during her first birth at the age of 16, and lived with the fistula for the last 20 years.
29
Loneliness and social disintegration
Women frequently withdrew from social life due to odor, shame, and family restrictions.13,24
–27 They avoided markets, religious services, and community gatherings, citing fear of stigma and self-perceived impurity. This isolation extended to health care access, as women reported difficulty using public transport. One woman explained:
“I preferred to be alone. I cannot sleep with my husband; I cannot pray in church; I cannot sit with people at the coffee ceremony. So why do I live” 40-year-old woman with obstetric fistula explained her experiences
24
Social stigma
Social rejection due to odor was pervasive, often manifesting in ridicule, avoidance, or derogatory remarks.13,24,27 This social rejection contributes to profound emotional distress, as many women reports feeling inferior, sinful, and shamefully different from those around them. These experiences reinforced feelings of inferiority, guilt, and hopelessness, further undermining attempts at reintegration.
Economic challenges
The inability to work or generate income emerged as a major challeng.13,24,25,29,30 Women were often abandoned by husbands and unable to support themselves, both pre- and post-surgery. Routine tasks such as trading or farming became impossible, leaving many dependents on family or low-paying, menial labor:
“Before the problem I was selling ‘tella’ [local alcoholic drink], also continued after my illness but when my condition became recognized. . ..no one was coming to my house. . .. Now I stopped it. When (husband) left me. . .. I went to my mother’s home to live with. . ..” “I was roasting maize/barley for a woman who prepares “tella” for sell every week. She will give me on the day I complete the work, I will use that for soap, underwear and sometimes for salt and coffee (Age 26–30 years, separated, lived with condition for 2 years and 11 months).
25
Coping mechanisms
Self-isolation
Six studies13,24 –27,29 described self-isolation as a common coping mechanism. To avoid ridicule and stigma, many women deliberately withdrew from community life, with some retreating to remote areas. While protective in the short term, this strategy reinforced marginalization and hindered access to treatment. 31
Wearing multiple layers clothes
In Ethiopia, women with obstetric fistula often manage continuous urine leakage by layering multiple garments, which function as improvised absorbents.13,25,29 These clothes are changed frequently when resources allow, while dark or neutral outer coverings help mask wetness and reduce visible stigma. Such strategies reveal both the physical burden of the condition and the social resilience required to preserve dignity in the face of profound marginalization.
“I wore ugly ‘dirty’ clothes that does not expose the sign of urine and mystify my condition” (Age 26–30 years, divorced, lived with condition for 3 years).
25
Interpretive integration
Across all domains, the findings reflect a profound entanglement of physical suffering, psychological distress, and socioeconomic marginalization. Physical symptoms such as incontinence, odor, and pain not only impaired daily functioning but also acted as triggers for social stigma, marital breakdown, and economic exclusion. These in turn deepened feelings of hopelessness, grief, and suicidal ideation. Coping mechanisms, though adaptive in intent, often reinforced cycles of isolation and concealment. Collectively, the evidence supports a biopsychosocial model of fistula, wherein the disorder extends far beyond biomedical pathology to encompass layered social, cultural, and psychological consequences. This model illustrates the psychological, social, and physical phenomena associated with the experience of the disease (Figure 2). 32
Discussion
Summary of the findings
Obstetric fistula is a severe childbirth injury that leads to significant and persistent physical challenges for affected women. This review synthesized qualitative evidence on the lived experiences of women with fistula in Ethiopia, encompassing both their personal challenges and coping strategies from their own perspectives. This synthesis identified the physical, social, economic, and psychological burdens women with obstetric fistula bear and their coping strategies, which are particularly important in Ethiopia due to the country’s high prevalence of obstetric fistula, limited access to specialized healthcare, and sociocultural barriers that exacerbate stigma and isolation.
Physical challenges
The most common physical problems include continuous incontinence, pain, foot drop, and strong body odor, all of which severely impact daily life and well-being. This is in line with other studies showing that nearly all women with obstetric fistula experience continuous leakage of urine and/or feces, often described as both stress and urgency incontinence. Findings from the Ghana Women’s Hospital indicate that pain, foot drop, urinary incontinence, and strong body odor are frequent physical challenges faced by women with fistula. 33 A previous review from sub-Saharan Africa also indicated that physical challenges of obstetric fistula commonly include incontinence, pain, foot drop, and unpleasant body odor. 16 Similarly, evidence from Uganda shows that many women continue to suffer from residual incontinence even after successful fistula repair, underscoring the need for robust follow-up care after procedure. 34
The smell of urine and the leakage itself were deeply stigmatizing and discrediting for women, causing feelings of shame, low self-esteem, anxiety, and embarrassment, as well as leading to humiliation. The way others perceived them became highly significant, creating a basis for internalizing these negative and demeaning views. 35 While women with obstetric fistula have a critical need for sanitary materials to maintain personal hygiene and stay clean, the economic burden of acquiring these materials poses a significant challenge (as also described below under economic challenges). Even when they manage to obtain sanitary products, the frequent washing and maintenance required can be exhausting and discouraging, leading some women to give up on proper hygiene practices altogether. 2
These physical challenges are particularly important because they directly influence social participation, mental health, and economic productivity. Mechanistically, inadequate education and low health literacy may limit women’s ability to understand hygiene instructions, navigate healthcare systems, and adopt effective coping strategies. Additionally, persistent physical symptoms reinforce stigma and social exclusion, which in turn exacerbate psychological distress and reduce motivation to seek care. Understanding these interlinked pathways is crucial for designing holistic interventions that address both medical and sociopsychological needs.
Psychological challenges
Hopelessness and suicidal ideation emerged as prominent themes in this review, arising from multiple interrelated factors. Following the onset of obstetric fistula, many women experience abandonment, social marginalization, and the loss of marital relationships, intensifying emotional suffering and perceived social failure. A substantial number believe they will never remarry or have children, further exacerbating feelings of grief, loss, and despair. Suicidal thoughts among women with obstetric fistula have been documented in systematic reviews from Nigeria 36 and study from Kenya. 37 Beyond the physical debilitation caused by the condition, reactions from individuals with limited or inaccurate knowledge about fistula often magnify psychological distress. 10 The interplay of disease characteristics, social rejection, and negative judgment from both the wider community and, at times, close relatives can profoundly affect mental health, frequently leading to hopelessness, existential crises, and a diminished sense of purpose. Women who experience stillbirth while developing fistula endure compounded trauma, resulting in profound grief and emotional suffering; globally, 90.1% of pregnancies complicated by fistula result in stillbirth, primarily due to obstructed or prolonged labor. 15 In this review, however, many women attributed fistula development to instrumental delivery rather than to obstructed labor, likely reflecting inadequate counseling or poor communication from healthcare providers regarding the necessity and rationale of such interventions.
Addressing these psychological consequences requires a holistic approach: healthcare providers must actively identify early signs of distress and suicidal ideation and integrate mental health referrals into treatment plans. Furthermore, education of families and communities is essential to reduce stigma, foster support, and enhance the social reintegration of affected women. 38 Systematically, these psychological challenges are compounded by limited health literacy, social isolation, and internalization of stigma, which together can perpetuate cycles of emotional distress, avoidance of care, and social withdrawal. Recognizing and addressing these interlinked pathways is critical to improving both mental health outcomes and overall quality of life for women living with obstetric fistula.
Social challenges
This systematic review and meta-synthesis found that women lived with obstetric fistula faced socioeconomic challenges including stigma, isolation, divorce, loneliness and social disintegration, and economic challenges. This is congruent with the literature robustly demonstrates that women living with obstetric fistula experience profound social challenges—universal and severe stigma; enacted (from others) and felt (internalized) stigma arise from incontinence and odor, often leading to ostracism and loss of social status regardless of geographic context for instance. Finding from Malawi shows that significant number of women with fistula experienced divorce, loneliness. and social disintegration. 39 Finding from Uganda also indicates that women with fistula face profound social challenges, including stigma, isolation, including divorce. Their marital and sexual lives often lose joy and fulfillment. 40 Other studies also indicates that women with obstetric fistula self-isolate or are abandoned by community/family, reporting deep loneliness and reduced social participation in different context including Uganda34,40,41 and Sudan. 42 In addition, high rates of separation/divorce are commonplace and closely tied to the onset of fistula and subsequent “impurity” or loss of dignity and social status.2,42 –44 As the stigma surrounding the fistula often leads to marital breakdown and loss of spousal support, it underscores the importance of targeted interventions within marital and family counseling to address misconceptions, improve communication, and support couples in coping with the challenges posed by the fistula.
Another important theme was impaired economic activity: Incontinence limits women’s ability to farm, trade, or perform household roles, with many families forced into asset depletion. This common experience of women with fistula in different context in Africa like Tanzania, 2 and in Uganda. 44 Additionally, study highlights that even the lack of money for transportation acts as a barrier to seeking healthcare, despite their awareness of available treatment options. 31 This may be because of a couple of reasons. First, the physical limitations caused by incontinence can hinder women’s participation in labor-intensive tasks like farming or trading, as they may struggle with mobility and face embarrassment or fear of stigma in public settings. Second, the healthcare costs associated with managing fistula and health-related issues can drain family resources, forcing families to sell assets or deplete savings to cover medical expenses.
Coping mechanisms
In this review, emerged coping mechanisms were self-isolation wearing multiple clothes to hide their situation. Women with fistula across diverse African contexts use a combination of emotional (e.g., self-isolation) and practical (e.g., homemade pads, layered clothing) coping strategies to manage the persistent challenges of incontinence in the same way with current review findings. For instance, finding from Malawian women, 42 Kenya, 45 Nigeria, 10 and Sudan. 46 Despite their efforts, many experience loneliness, either through self-isolation or exclusion by family and community members, leading to a significant loss of marital and sexual rights. 47 Concealment strategies to hide the condition from community, kin, or spouses, sometimes leading to further psychosocial challenges and hinder them from seeking healthcare. 48 Such coping mechanisms comes from stigma, and stigma not only drives emotional distress but also affect practical behaviors (e.g., layering multiple clothes to mask odor).2,47 The coping mechanisms adopted by women with fistula, such as self-isolation and concealment through layered clothing, reflect the deep-rooted stigma surrounding the condition, which not only causes emotional distress but also drives behaviors that can further isolate women and delay their access to healthcare. These findings imply that interventions must go beyond medical treatment to address the social stigma and psychosocial barriers that hinder women from seeking timely care and support. 17 Community education and awareness campaigns are crucial to reduce misconceptions and discrimination, while psychosocial support services should be integrated into fistula care programs to help women cope healthily without resorting to harmful isolation or concealment. 48 Additionally, involving families and spouses in counseling could help rebuild social ties and protect women’s marital and sexual rights, ultimately improving their overall quality of life.
Strengths and limitations
This review offers several notable strengths. It is the first Ethiopia‑focused qualitative meta‑synthesis on obstetric fistula, systematically integrating women lived experiences with their coping strategies. By emphasizing survivor-centered perspectives and framing findings within a biopsychosocial model, it underscores that obstetric fistula is not merely a surgical issue but a multidimensional public health and social justice challenge. Nonetheless, its primary limitation is the geographical focus on Ethiopia. While providing rich national context, the findings may not fully capture experiences in other sub-Saharan African countries, highlighting the need for future multi-country reviews to assess the transferability and broader applicability of these insights.
Implications of the study
Obstetric fistula disproportionately affects marginalized women, arising from childbirth complications that often result in child loss, marital dissolution, and social isolation. Beyond physical suffering, women experience profound emotional distress, including grief, hopelessness, and suicidal ideation, compounded by societal stigma and economic hardship. Coping strategies such as self-isolation, while understandable, can further restrict access to medical care and social support. These findings highlight the need for a comprehensive, multi-dimensional approach addressing the physical, social, economic, and psychological challenges of affected women. Eradicating this preventable condition requires coordinated policy interventions, resource allocation, and a commitment to both prevention and holistic care.
Public health implications for policy and practice
Obstetric fistula is not merely a surgical problem but a complex public health and social justice issue. Women living with fistula experience lives constrained by incontinence, pain, stigma, and economic marginalization, challenges that cannot be fully addressed through clinical repair alone. Effective policy and practice, therefore, must adopt a woman-centered, biopsychosocial approach. Prevention is paramount and requires strengthening maternal health systems to ensure timely access to emergency obstetric care, skilled birth attendants, and robust referral networks, particularly in rural areas. Such measures not only reduce the incidence of fistula but also lower maternal and neonatal mortality. Treatment and rehabilitation must extend beyond surgical closure to encompass psychosocial counseling, peer support, and livelihood programs that facilitate social reintegration, restore dignity, and rebuild confidence. Addressing stigma is equally critical: public awareness campaigns and engagement with community and religious leaders can challenge misconceptions, reduce blame, and create a supportive environment that encourages reintegration. Finally, economic empowerment initiatives such as microfinance programs, vocational training, and social protection schemes are essential to secure financial independence and sustainable social inclusion, preventing women from remaining trapped in cycles of marginalization even after successful surgical repair. Taken together, these strategies underscore that combating obstetric fistula requires integrated interventions addressing medical, psychological, social, and economic dimensions, with women lived experiences at the center of policy and practice.
Conclusion
This systematic review and meta-synthesis comprehensively examined the deeply concerning lived experiences of women affected by obstetric fistula. The findings revealed a confluence of multifaceted challenges, encompassing physical morbidity, profound psychological distress, and significant socioeconomic hardship. A common coping mechanism employed by these women is wearing multiple layers of clothing, often accompanied by self-isolation from others.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251411072 – Supplemental material for The lived experiences and coping mechanisms of women with obstetric fistula in Ethiopia: A systematic review and meta-synthesis of qualitative evidence
Supplemental material, sj-docx-1-whe-10.1177_17455057251411072 for The lived experiences and coping mechanisms of women with obstetric fistula in Ethiopia: A systematic review and meta-synthesis of qualitative evidence by Yonas Abebe, Diriba Bekele and Robera Demissie in Women's Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057251411072 – Supplemental material for The lived experiences and coping mechanisms of women with obstetric fistula in Ethiopia: A systematic review and meta-synthesis of qualitative evidence
Supplemental material, sj-docx-2-whe-10.1177_17455057251411072 for The lived experiences and coping mechanisms of women with obstetric fistula in Ethiopia: A systematic review and meta-synthesis of qualitative evidence by Yonas Abebe, Diriba Bekele and Robera Demissie in Women's Health
Supplemental Material
sj-docx-3-whe-10.1177_17455057251411072 – Supplemental material for The lived experiences and coping mechanisms of women with obstetric fistula in Ethiopia: A systematic review and meta-synthesis of qualitative evidence
Supplemental material, sj-docx-3-whe-10.1177_17455057251411072 for The lived experiences and coping mechanisms of women with obstetric fistula in Ethiopia: A systematic review and meta-synthesis of qualitative evidence by Yonas Abebe, Diriba Bekele and Robera Demissie in Women's Health
Footnotes
Acknowledgements
None.
Ethics considerations
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data used in this work can be provided upon reasonable request by contacting the corresponding authors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.