
Abstract
Background:
Warning signs of pregnancy are not reliably predictable. But, knowing these early warning signs is very important for pregnant women to eliminate serious complications and start treatment immediately. The higher level of maternal mortality can be reduced by providing quality maternity service and empowering women with good knowledge of the danger signs of pregnancy and promoting appropriate health-seeking behavior. Therefore, this study aimed to assess the knowledge of pregnancy danger signs and health-seeking behavior among reproductive age women in southwest Ethiopia.
Method:
A cross-sectional study was carried out with 526 randomly selected women from 1 to 30 January 2019. The data were collected through face-to-face interviews and analyzed using Statistical Package for the Social Sciences version 21. Both bivariate and multivariable logistic regression analyses were conducted to determine factors associated with the outcome variable. The level of significance was declared at a p-value < 0.05.
Results:
The proportion of mothers who had good knowledge of pregnancy danger signs were 43.2%. The majority (65%) of those surveyed mentioned vaginal bleeding as a pregnancy danger sign. The factors associated with good knowledge of pregnancy danger signs were husbands with secondary education and above (adjusted odds ratio = 2.52, 95% confidence interval (1.08–5.91) monthly income ⩾ 1000 Ethiopian Birr (adjusted odds ratio = 2.64, 95% confidence interval (1.48–4.71) being multigravida (adjusted odds ratio = 2.14, 95% confidence interval (1.17–3.94) and last delivery at the health facility (adjusted odds ratio = 6.84, 95% confidence interval (4.02–11.63) The proportion of mothers who experienced pregnancy danger signs and had good health-seeking behavior was 72.7%.
Conclusion:
The knowledge of pregnancy danger signs among reproductive age women was low in the study area. This indicates the large proportions of women who do not know the danger signs are likely to delay in deciding to seek care when they face the problem. Therefore, empowering women, improving the quality of health information about danger signs during antenatal care follow-up, and promoting institutional delivery are the recommended interventions.
Keywords
Background
Pregnancy is a normal process that causes a range of physiological and psychological changes in pregnant women. However, a normal pregnancy may be accompanied by certain problems and complications that endanger the life of the mother and fetus.1–4 Nearly 15% of all pregnant women develop a specific obstetric complication. 5
According to the 2015 World Health Organization (WHO) 6 report, approximately 10.7 million mothers died from 1990 to 2015 as a result of obstetric complications. Almost all of these deaths (99% of maternal deaths worldwide) occurred in developing countries, with 66% of these deaths occurring in sub-Saharan African countries, including Ethiopia. 7 The progress of reducing maternal mortality ratio (MMR) is notable; however, the annual rate of decline was less than half of what was needed to achieve the fifth Millennium Development Goal (MDG5). The 34% decline of MMR for the period 1990–2008 translates into an average annual decline of just 2.3%. This was far from the annual decline of 5.5% required to achieve MDG5. 8
Maternal deaths have both direct and indirect causes. Worldwide, nearly 85% of maternal deaths are due to direct obstetric danger signs. 5 Pregnancy danger signs (PDSs) are warning obstetric signs that women experience during pregnancy. 9 Danger signs of pregnancy are not reliably predictable; 10 however, knowing these early warning signs by pregnant women is very important to eliminate serious complications and start treatment immediately.1,9 The direct cause of maternal mortality was easily avoidable if the mother and family recognized signs and sought immediate care. 11
Women’s ability to identify signs of danger during pregnancy and seek health care plays a key role in preventing and reducing maternal morbidity and mortality. Poor knowledge of obstetric signs of danger during pregnancy contributes to delays in the search for or to receive qualified care,12,13 which results in maternal deaths.9,14 The three phases of delay in accessing obstetric care have been identified: delay in deciding to seek care; delay in reaching a healthcare facility; and delay in receiving appropriate treatment after reaching the health facility. 15 Knowledge of the danger signs of pregnancy is a critical first step in accepting appropriate and timely referrals to obstetric care.16,17 It assists in decision-making for seeking health care in case of complications, 14 which is very important toward the achievement of sustainable development goal 3 (SDG 3); reducing the global MMR to less than 70 per 100,000 live births by 2030. 18 The health-seeking behavior of pregnant women relies heavily on their knowledge of the danger signs of pregnancy.1,19 Anderson 20 revealed that the presence of predisposing (socio-demographic characteristics), enabling (facilitates individuals to use services such as availability of resources such as income, access to free services, availability and access to the service), need (physical conditions illness or disease conditions that motivate service use), and external factors influence the utilization of health services. The availability, affordability, and cultural acceptability of health services were the factors that greatly affect the utilization. 21 Kebede et al. 22 revealed that poor risk awareness, inadequate infrastructure and transport, poor quality of care, and lack of financial independence hinder easy access to obstetric care.
Women’s knowledge of pregnancy-related danger signs is influenced by multiple factors, including maternal age, occupation, education, marital status, husband’s education and occupation, monthly income, residence, family size, gravidity, parity, antenatal care (ANC) visit and number of ANC, place of delivery, attendants of the previous delivery, time is taken to reach health facility on foot, health education, and source of information.2,9,13,17,23–34
High maternal mortality rates can be reduced through the provision of quality maternity care and empower women to know the danger signs of pregnancy and promote appropriate health-seeking behavior;17,30 however, no studies revealed the knowledge profile of PDSs and health-seeking behavior among reproductive age women in the study area. Unlike other obstetric danger signs, the danger signs of pregnancy are not the actual obstetric complications but are symptoms that could be easily recognized by non-clinical personnel. 31 That is why this study only assesses the knowledge of obstetric danger signs during pregnancy. Therefore, this study aimed to assess the knowledge of PDSs and health-seeking behavior among reproductive age women in Mizan-Aman town, southwest Ethiopia.
Methods
Study design, area, and period
A community-based cross-sectional study was conducted in the town of Mizan-Aman in the Bench-Sheko zone of southwest Ethiopia from 1 to 30 January 2019. Mizan-Aman town is the administrative center of the Bench-Sheko zone and has two sub-cities (namely Mizan & Aman) and five kebeles (smallest administrative unit in Ethiopia), three kebeles (namely Adisketema, Hibret, and Ediget) are under Mizan sub-city and two kebeles (Kometa and Shasheka) are under Aman sub-city.
Populations
The source population was all women in the reproductive age group (15–49 years old) who gave birth within the past 12 months before the date of data collection and who had been living at least for 6 months in Mizan-Aman town. The study population was randomly selected women of the reproductive age group. All mothers of the reproductive age group who had a delivery in the past 12 months, regardless of the place and outcome of delivery, were included in this study. Mentally ill and health workers were excluded.
Sample size determination
The required sample size for this study was calculated by using a single population proportion formula using the assumption of 95% confidence level, 5% precision of the estimate, and proportion of mothers with good knowledge of obstetric danger signs during pregnancy 30.4%, which was taken from the previous study done at Aleta Wondo district, Ethiopia, 33 1.5 design effect and 10% of non-response rate compensation. The final computed sample size was 537.
Sampling procedure
Stratification was done into urban (n = 3) and semi-urban (n = 2) kebeles. Then, in each stratum, one-third of kebeles (one urban and one semi-urban) kebeles were selected by a simple random sampling method. Then census was done in the selected two kebeles to identify mothers who gave birth in the last year before the data collection. Based on census results, the total households were found to be 556 households in urban kebele and 541 households in semi-urban kebele. The total calculated sample size (n = 537) was proportionally allocated (271 and 266 mothers from urban and semi-urban kebeles, respectively) for each kebele based on the number of eligible mothers (based on census) present in the area. Then the total households in each kebele, which were 556 households in urban kebele and 541 households in semi-urban kebele were divided by the respective sample sizes allocated to get the sampling intervals (k). As a result, the sampling intervals for urban and semi-urban kebeles was nearly 2. The random start was selected randomly, and finally, every two households from a random start were studied until the required sample size was obtained.
Study variables and measurements
The dependent variable was knowledge of PDSs. The independent variables were sociodemographic factors (maternal age, women’s occupation, women’s education, husband’s education, and income), obstetric factors (gravidity, parity, and experience of danger signs), and health service–related factors (place of the previous delivery, ANC follow-up, advised on danger sign during ANC and women’s satisfaction by health provider approach and advice).
Danger signs are conditions that increase the chances of a pregnant woman and/ or her unborn child dying or in poor health. The key PDSs commonly manifested are severe vaginal bleeding, swollen hand or face, blurred vision, persistent frontal or occipital headache, altered consciousness, abnormal body movement (convulsions), severe abdominal/epigastric pain, profuse vaginal discharge, absence or reduction of fetal movement, and persistent and severe vomiting, especially after 12 weeks’ gestational age. 35
Spontaneous knowledge refers to the respondent’s naming of a PDS without being asked about that sign by name. 17 Good knowledge of PDSs refers to those participants who mentioned at least three PDSs spontaneously, if not poor knowledge. 23 Experience of PDS(s) refers to any sign of PDS(s) reported by women, which occurs during pregnancy.
Practice (health-seeking behavior) refers to the action taking of participants to seek care for PDSs. 36 Good practice refers to those participants who require immediate medical care when they experience PDSs. 36 Poor practice refers to those participants who seek care from a traditional birth attendant and an elderly woman, and who have stayed home when they experience PDSs. 36
Data collection tools and techniques
Data were collected through face-to-face interviews using a structured questionnaire adapted from a safe motherhood questionnaire developed by the Maternal and Neonatal Health Program of JHPIEGO (Johns Hopkins Program for International Education in Gynecology and Obstetrics), an affiliate of John Hopkins University. 36 A pretest was done on 5% of the total sample size in Tepi town and a necessary amendment was made (the amendments made were the flow of questionnaire, avoiding questions that do not make sense to participants or ambiguous questions or problems with the questionnaire that might lead to biased answers). Two diploma midwives and four health extension workers (HEWs) who speak the local language fluently participated in the data collection. Two BSc health officers supervised the data collection process. Two days of training were given to data collectors and supervisors on the objective and method of data collection and addressed the presence of unclear questions on the questionnaire.
Plan for data analysis
The data were verified for completeness and consistency, then coded and entered into Epi-data manager software and analyzed using Statistical Package for the Social Sciences (SPSS) version 21. Descriptive statistical analysis was used to present the socio-demographic, obstetric, and health service–related characteristics and the knowledge of PDSs. The results are presented in tables and numerical summary measures such as mean and standard deviation (SD). Binary logistic regression was used to determine the association of each explanatory variable with knowledge of PDSs. Explanatory variables associated with the outcome variable at a p-value of less than or equal to 0.25 in the bivariate logistic regression model were included in the multivariable logistic regression model to control the potential confounders. Multi-collinearity between the model-independent variables was checked, and the variance inflation factor (VIF) was considered acceptable (less than 2). The Hosmer–Lemeshow goodness-of-fit test indicated (p = 0.679) that the model was good enough to fit the data well.
Results
Socio-demographic characteristics
Of the 537 recruited mothers, 526 responded to the interview, resulting in a response rate of 98%. The mean age of respondents was 28.8 (±5.5 SD) years ranging from 19 to 45 years. Close to half (50.8%) of the respondents belonged to the Bench ethnic group. Two hundred seventy-nine (53%) of the respondents have completed secondary or higher education. Over two-third, (68.8%) of those interviewed earned a monthly income of ⩾ 1000 Ethiopian Birrs (Table 1).
A socio-demographic characteristics of reproductive age women in southwest Ethiopia.

ETB: Ethiopian Birr.
Includes Oromo, Tigre, and Selti, ethnic groups.
Obstetric and health service–related characteristics
Of the 526 respondents, more than two-thirds (71.7%) and more than three-fourths (86.7%) of the respondents were multigravida and ANC-attended for their last pregnancy, respectively. Of the 456 respondents who attended ANC services, 55 (12%) of the respondents had four or more ANC visits (Table 2).
Obstetric and health service–related characteristics of reproductive age women in southwest Ethiopia.
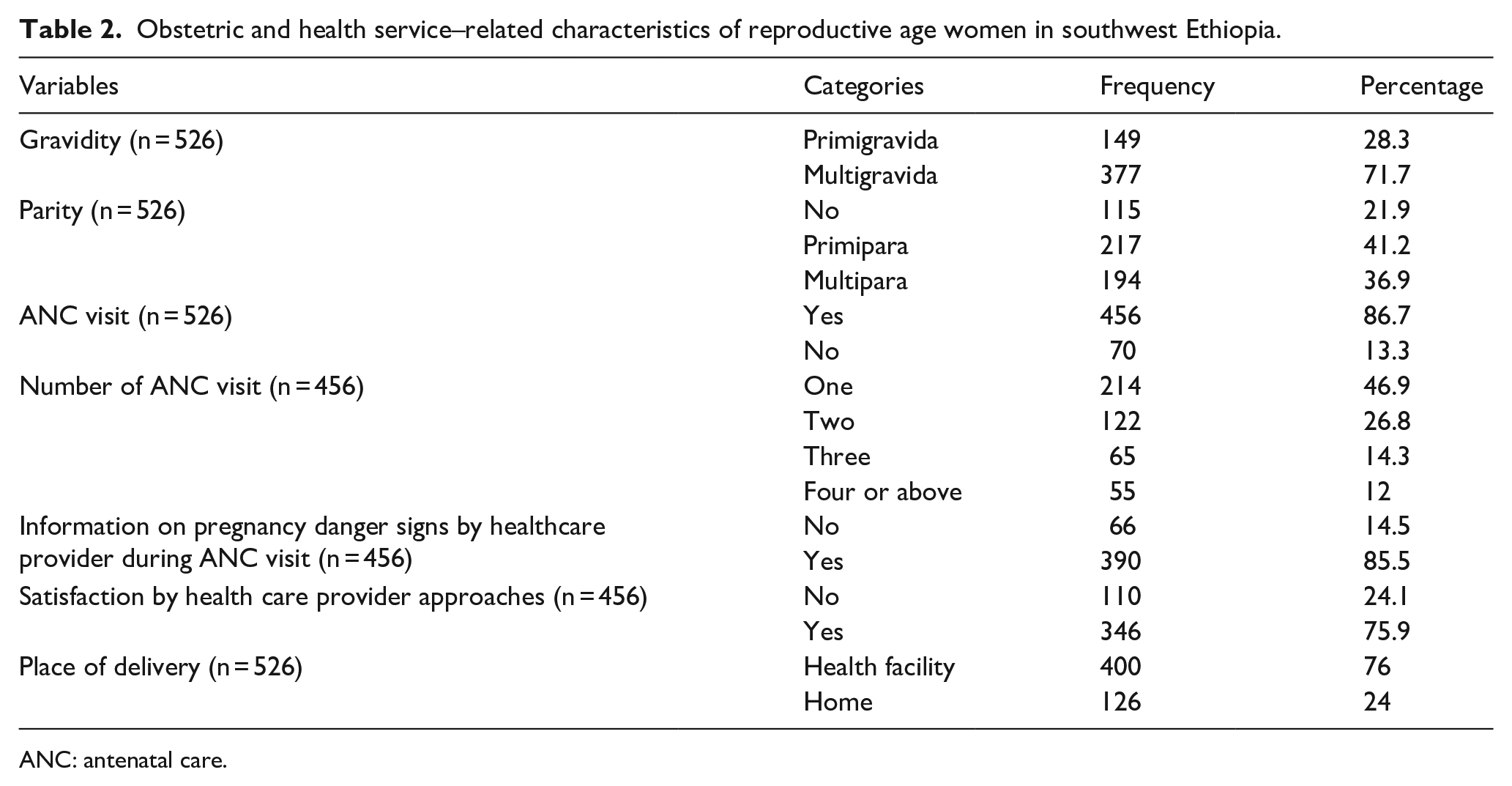
ANC: antenatal care.
Knowledge regarding PDSs
Of the 526 respondents interviewed, the proportion of good knowledge about obstetric danger signs during pregnancy was 43.2% (227). The majority (65%) of those interviewed cited vaginal bleeding as a PDS (Table 3).
Knowledge regarding pregnancy danger signs among reproductive age women in southwest Ethiopia.

Health-seeking behavior of women toward PDSs
Of the 526 interviewees, 77 (14.6%) had a history of PDSs. Vaginal bleeding was the most frequently reported PDS (46.5%) followed by swelling of the hand and/or face (39%), and persistent headache (14.5%). Of the 77 participants, majority (72.7%) had a good practice (sought treatment health in institutions). Of the 21 mothers who did not seek medical treatment, 15 (71%) and 5 (23%) perceived it as harmless and a lack of money, respectively.
Factors associated with women’s good knowledge of PDSs
After adjusting mother’s education, husband’s education, monthly income, and place of delivery as confounding factors, husband secondary and above education (adjusted odds ratio (AOR) = 2.52, 95% confidence interval (95% CI) (1.08–5.91) monthly income ⩾ 1000 ETB (AOR = 2.64, 95% CI (1.48–4.71) being multigravida (AOR = 2.14, 95% CI (1.17–3.94) and delivery at a health facility (AOR = 6.84, 95% CI (4.02–11.63) were significantly associated with good knowledge of PDSs (Table 4).
Factors associated with women’s knowledge of pregnancy danger signs in southwest Ethiopia.

PDS: pregnancy danger sign; CI: confidence interval; COR: crude odds ratio; AOR: adjusted odds ratio; ETB: Ethiopian Birr.
p < 0.25; **p < 0.05.
Discussion
Studies revealed that knowledge of the danger signs of pregnancy complications is the essential first step in accepting appropriate and timely referral to obstetric care.16,17 The health-seeking behavior of pregnant women relies heavily on their knowledge of the danger signs of pregnancy.1,19 Based on the above fact, we aimed to assess the factors associated with knowledge of PDSs and health-seeking behavior among reproductive age women in Mizan-Aman town, southwest Ethiopia. The proportion of mothers with good knowledge about PDSs was 43.2%, 95% CI (39%–47.4%).
This finding was in line with some studies conducted in Ethiopia.17,23 It was lower than some studies conducted in Ethiopia,26,30,31 Uganda, 37 Madagascar, 28 and India.38,39 But it was higher than some studies conducted in Ethiopia,2,32–34,40 Tanzania, 13 and Kenya. 10 The variation observed compared to other studies could be due to the differences in sample size, the operational definition used (most studies used two, some used three and others used four, and so on criteria to say knowledgeable about PDSs), and methodology in general. Besides, the socioeconomic, cultural, and educational profiles of the study population may create a significant variation.
Respondents who had well-educated husbands were more aware of the signs of danger during pregnancy. Respondents with husbands having secondary and above education were 2.5 times more likely to have a good knowledge of PDSs than respondents with husbands unable to read and write. This finding was in line with studies conducted in Ethiopia.26,27 This could be due to the high tendency of educated husbands to be aware of their wives.
Respondents who had a monthly income of ⩾ 1000 ETB were 2.6 times more likely to have a good knowledge of PDSs than their counterparts. An increased monthly income was significantly associated with a good knowledge of PDSs. This finding was supported by studies conducted in Ethiopia.9,27 This could be because of the better income associated with a better purchasing power of television and radio, since getting information from mass media is an important contributing factor for developing good knowledge.29,31,41
Respondents who were multigravida had two times more probability to have a good knowledge of PDSs than primigravida. Being multigravida was significantly associated with good knowledge of PDSs. This finding was consistent with studies conducted in Ethiopia.30,34 This could be because the mother with multiple pregnancies may have repeated exposure to education regarding PDSs during each ANC visit.
Respondents who delivered at a health facility were 6.8 times more likely to have a good knowledge of PDSs than those who delivered at home. Being delivered at a health facility was strongly associated with good knowledge of PDSs. This finding was supported by studies conducted in Ethiopia.17,27,31
The proportion of mothers who experience PDSs and had good health-seeking behavior was 72.7%, 95% CI (62.7%–82.7%). This finding was lower than 86.3% in Debre Berhan, Ethiopia. 29 But it was higher than 56% in Tanzania 13 and 57.4% in Harar town, eastern Ethiopia. 42 The variation observed could be due to the differences in socioeconomic, educational, and cultural factors across different studies.
Conclusion
The knowledge of PDSs among reproductive age women was low in the study area. This indicates the large proportions of women who do not know are likely to delay in deciding to seek care when they faced the problem. Therefore, empowering women, improving the quality of health information about danger signs during ANC follow-up, and promoting institutional delivery are the recommended interventions.
Limitations
First, this study only assessed the obstetric danger signs during pregnancy; the other obstetric danger signs, which may happen during childbirth and postpartum time were not included. Second, because of the small sample size observed, we did not do regression analysis for identifying factors associated with women’s health-seeking behavior.
Footnotes
Acknowledgements
The authors acknowledge the study participants for their valuable participation and the Mizan-Aman town administration for their full collaboration and support by providing important data during the study. We would like to acknowledge data collectors and supervisors for their valuable contributions during data collection.
Author contributions
T.Y. was involved in the conception, design, and acquisition of data, analysis, and interpretation of the results. M.T. was involved in the design, acquisition of data, and analysis of the results. T.Y. drafted the manuscript, and all the authors approved it for publication.
Availability of data and material
The datasets used and/or analyzed during this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
Ethical approval was obtained before starting data collection from Mizan-Tepi University Institutional Review Board (MTU-IRB) on 20 December 2018 with the reference number MTUIRB/068/2018. All study participants were informed about the purpose of the study, their right to deny participation, anonymity, confidentiality of the information. Written informed consent was also obtained before participation in the study.