
Abstract
Introduction:
Anaemia is a global public health concern. Anaemia in women of reproductive age has negative outcomes on their health and reproduction.
Objective:
This study assessed the knowledge, prevalence and associated factors of anaemia among non-pregnant and non-lactating women of reproductive age in Northern Ghana.
Design:
This is a cross-sectional study.
Method:
A systematic random sampling was used to select 317 participants from the Tamale Metropolis. A semi-structured questionnaire was used to collect data on the sociodemographic, knowledge level of anaemia and iron foods. Haemoglobin levels were determined using URIT-12. Haemoglobin status was classified according to the World Health Organization standards. Descriptive statistics and chi-square were used in the statistical analysis.
Results:
The mean age (SD) of participants was 26.4 ± 6.9. A large proportion (68.8%) of the women had knowledge about anaemia, and the source of information was mainly health professionals (56.4%). More than half of the participants knew of the symptoms (80%), causes (83.9%), prevention measures (81.2%), consequences of anaemia (64.2%) and iron-rich food sources (76%). A greater share of the participants, however, had no knowledge of both iron-enhancing foods (53.7%) and iron-inhibiting foods (51.8%). The prevalence of anaemia was high generally (63.1%) and was highest among females at the tertiary institutions (43%) and who were single (60.5%). A significant association existed between income status and haemoglobin status (χ2 = 6.3, p = 0.044).
Conclusion:
The majority of participants knew about anaemia; however, they had limited knowledge of iron-enhancing and inhibiting foods. The prevalence of anaemia was high among women of reproductive age. Integrating economic empowerment and nutrition education with the inclusion of iron-enhancing and iron-inhibiting foods could help to reduce the high prevalence of anaemia among women of reproductive age.
Introduction
Anaemia is simply defined as low haemoglobin (Hb) levels or Hb levels less than 120 g/L.1,2 There are different types of nutritional anaemia such as megaloblastic and pernicious. The most prevalent type, across the lifecycle, is iron deficiency anaemia.2 –5 The global all-age prevalence of anaemia is 22.8%. 6 Anaemia, one of the main public health issues, mainly affects females in the reproductive age and children. In pregnant women, the global prevalence is 36.8%. 7 The prevalence of anaemia in pregnant women, non-pregnant women (15–49 years) and children (under 5 years) in the lower-middle income countries (LMIC) is found to be above 45.2%, 39.5% and 56.5%, respectively.8,9 The prevalence of anaemia in LMIC was the highest in sub-Saharan Africa, Middle Eastern, Central America and South Western Asia.6,10 In Ghana, the prevalence of anaemia among female adolescents is 50.3%, 11 35.6% in children (less than 5 years) and 21.7% in non-pregnant women. 12
Anaemia is caused by nutritional and non-nutritional factors, with the nutritional factor being the commonest.13,14 The development of anaemia culminates from a low production of red blood, rapid destruction of red blood cell, blood loss or a combination of all these factors. 2 These factors could have their roots from physiological, pathological, environmental and genetic malfunctioning. 15 The risk factors of anaemia vary from age, gender and socioeconomic status. 16 A systematic review indicated that menstruation, parasitic infection, low educational status and food intake practices were the leading contributors of iron deficiency anaemia among adolescents in developing countries. 17
A multifaceted approach is required to manage and prevent anaemia due to its multiple causes. 17 In poor-resource settings, the short- to medium- and long-term interventions implemented to control anaemia include daily and intermittent iron supplementation, home fortification with micronutrient powders, fortification of staple foods and condiments, and activities to improve food security and dietary diversity.17,18 In Ghana, malaria control and antihelminth administration are popular strategies to manage and prevent anaemia. 19
The knowledge level of anaemia and iron foods among adolescents11,20,21 and pregnant women22 –24 has been investigated by several researchers. The studies indicated varied outcomes: while some showed low knowledge levels,20,22 others showed a high knowledge level.21,23 There appears to be very few studies or even none to have been carried out solely among non-pregnant and non-lactating mothers in the reproductive age, focusing on knowledge of anaemia and iron foods.
Identifying and addressing the risk factors of anaemia among non-pregnant women of reproductive age (WRA) is considered as prime nutritional preconception care to reduce maternal, neonatal and infant mortality associated with anaemia. 25 The prevalence of anaemia consistently increased across the pregnancy duration in women in Bolgatanga. 26 Awareness about the prevalence of anaemia in non-pregnant women has the potential to influence the urgency and array of interventions to alleviate it. Tackling anaemia among non-pregnant and non-lactating women would help to prevent and reduce the rate of anaemia in pregnancy and lactation. Thus the aim of the study was to assess the knowledge, prevalence and associated factors of anaemia among WRA in the Tamale Metropolis of Ghana.
Materials and methods
Study area, design and participants
This analytical cross-sectional study was conducted in Tamale Metropolis in the Northern region of Ghana. Tamale as the capital, is located in the middle of the Northern Region at latitude 9.403423 and longitude −0.842416. Tamale shares borders with Sagnarigu district to the West and North, Mion district to the East, East Gonja to the South and Central Gonja to the South-West. The Metropolis is approximately 180 m above sea level and it has one rainfall season annually. It has a total female population of 189,693. The majority of the people are Dagombas, with a few being Akans, Gonjas, Mamprusis, Dagaabas and Ewes. The population largely engages in sales and services, with a few also into craft work, agriculture, forestry and fishery work. 27
The Cochran’s formula was used to calculate the sample size with a drop-out rate of 10%, hence 317 participants were obtained as the total sample. A systematic random sampling was used in the selection of the participants. Participants recruited were WRA (15–49 years old) who were non-pregnant and non-lactating. Women of fertile age diagnosed or with a history of cancer in any form, those who were pregnant (indicated by a pregnancy test done at the hospital), and who took any form of vitamin or mineral supplements were all excluded.
The article was prepared according to the STROBE Guidelines.
Data collection
Duration
The data collection lasted for 3 months between the period of May 2023 and July 2023.
Questionnaire
The sociodemographic, knowledge of iron deficiency anaemia and iron foods of participants were assessed using pretested semi-structured questionnaires. These questionnaires have been validated by the Food and Agriculture Organization. 28
Knowledge of iron deficiency anaemia and iron foods
Assessment of the awareness, general signs, causes, prevention and management anaemia, consequences of anaemia, iron-rich foods, iron-enhancing foods and iron-inhibiting foods questionnaire was adapted from the Food and Agriculture Organization document titled ‘Guidelines for assessing nutrition related knowledge, attitude and practices’. 28 The overall knowledge score was 7; participants with scores of ⩾4 and above were classified as high knowledge and those with scores of ⩽3 were classified as low knowledge level.
Determination of Hb levels
The Hb level was determined using URIT-12 (Aliroad Medical, B-7-3-3, Hi-Tech Medical Device Park, No. 818, Gaoxin Avenue, East Lake Hi-Tech Development Zone, Wuhan, Hubei, CN). The participant’s middle finger was massaged from the knuckle to the tip to stimulate blood flow. The site for pricking was cleaned with alcohol and wiped dry with a gauze pad. The underside of the finger was incised or pricked with a lancet and light pressure was applied to obtain the blood. A drop of blood was applied to the test strip by touching the hanging blood drop to the test spot. It was ensured that the blood was large enough to fill the test spot. The test results were displayed in less than 30 s. Anaemia is defined according to the World Health Organization for non-pregnant women as no anaemia (⩾12 g/dL), mild anaemia (11–11.9 g/dL), moderate anaemia (8–10.9 g/dL) and severe anaemia (<8.0 g/dL). 1
Statistical analysis
The statistical package for social sciences (SPSS version 25) was used for data analysis and cleaning. The continuous data were tested for normality with the aid of Kolmogorov–Smirnov and Shapiro–Wilk tests. The normally distributed data were analysed with the parametric method. Descriptive statistics was used in the presentation of the sociodemographic, knowledge level of anaemia and Hb status. Chi-square tested the association between the sociodemographic awareness of anaemia and Hb status. Independent sample t-test was used to assess the mean Hb levels between anaemic and non-anaemic participants. Data were presented in mean, standard deviation, frequency and percentage. All p-values considered significant were <0.05.
Results
The results on the sociodemographic characteristics are indicated in Table 1. The average age for the participants was 26.4 ± 6.9, with the majority (60.9%) being single. With reference to their educational level, a greater proportion (82%) of the females had some form of formal education, though the females at the tertiary level were the majority (47.3 %) for the formal educational group. The largest group of participants were students (38.5%), followed by traders (31.5%). Less than 5% of the females were in the high-income status bracket, with over 86% falling within the lower income bracket.
Sociodemographic characteristics.

Others (banker, farmer, security officer and housewife); low (⩽Ghc900); moderate (Ghc1000–Ghc1900); high (⩾Ghc2000), single (never married/divorced/widowed).
The knowledge level of anaemia and iron foods of the participants are summarized in Table 2. More than half (68.8%) of the women in their reproductive age indicated they had knowledge about anaemia, and their source of information was largely from health professionals (56.4%) and media (17.8 %) or school (17%). About 80% of the female respondents knew of the symptoms of anaemia, with 64.2% knowing of the consequences that come with anaemia. A greater number of the respondents (83.9%) knew of the causes of anaemia, as well as ways to prevent or manage anaemia (81.2%). About 76% of females had knowledge of iron-rich food sources, while more than half (53.7%) had no knowledge of iron-enhancing foods. The greater share of the participants (51.8%) had no knowledge of iron-inhibiting foods.
Knowledge of anaemia and iron foods.
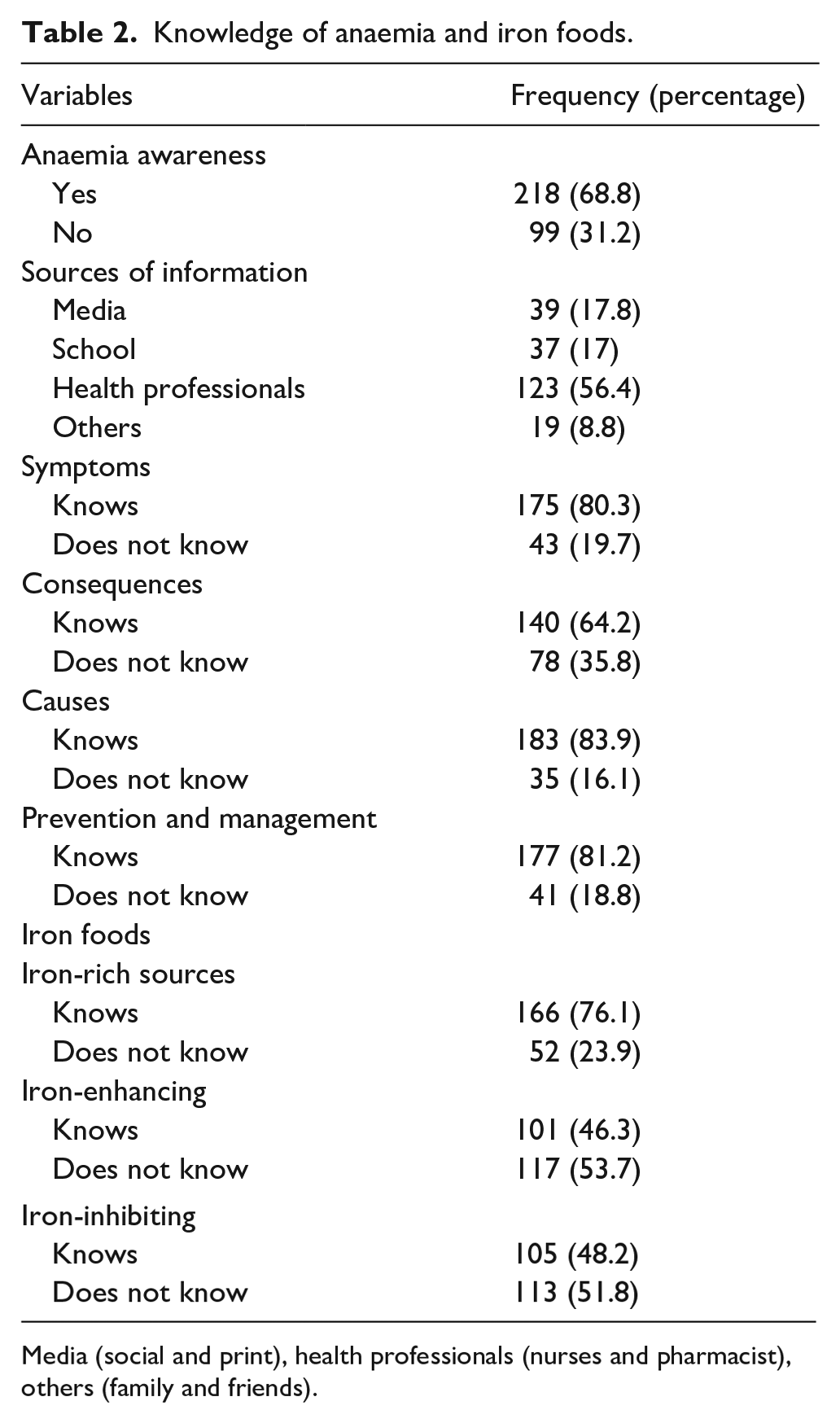
Media (social and print), health professionals (nurses and pharmacist), others (family and friends).
The mean Hb level was 11 ± 2.1, with the majority of participants (63.1%) having low Hb levels (9.9 ± 1.8) (Table 3). In terms of classification, only a smaller percentage of the respondents (12%) were severely anaemic, with 54% and 34% presenting with moderate and mild anaemia, respectively (Figure 1).

Classification of anaemia among the participants.
Haemoglobin levels and status.

Independent sample t-test. Mean (M), standard deviation (SD), p < 0.05.
There was a significant association between income status and Hb level (χ2 = 6.3, p = 0.044). Marital status, educational level and knowledge of anaemia had no associations with Hb levels (Table 4).
Association between sociodemographic characteristics, awareness of anaemia and haemoglobin status.

Chi-square (χ2), data presented as frequency (N) and percentage (%), p < 0.05.
Discussion
The aim of the study was to assess the knowledge, prevalence and factors associated with anaemia among WRA in Tamale Metropolis. The outcome revealed that WRA were highly aware of anaemia, causes, consequences, prevention and management. The prevalence of anaemia was high among the study participants. The high prevalence of anaemia was significantly associated with low-income status.
Generally, the findings showed that participants had a good knowledge of anaemia, its causes, consequences, prevention and management and rich food sources largely from health professionals, media or school. This observation is contradicted by that of Sheriff et al. 29 and Oyelese et al., 30 who stated that more than half of the WRA had no knowledge of anaemia. The differences might have resulted from the fact that the majority of the participants in this study had some form of tertiary education, and were living in an urban community with access to information, compared with the rural setting in the study of Sheriff et al. 29 The source of information by respondents in this study was also contrasted by Oyelese et al., 30 who reported that a greater share of the WRA were informed by their social circle (friends, family, neighbours). The findings of this study might indicate that the agencies responsible for educating the public on anaemia are doing well in terms of information dissemination. The high knowledge level on iron-rich foods in this study could have resulted from the source of information, which happened to be largely from health workers and schools, thus they might have been informed about the sources of iron-rich foods. The limited knowledge of iron-inhibiting and iron-absorption foods is a gap that needs to be addressed. These foods can therefore be incorporated into public education materials for dissemination, as knowledge of these foods is also vital in combating anaemia.
The prevalence of anaemia was higher in this study than other studies in Ghana, 12 Sri Lanka 29 and Rwadan, 31 though the knowledge level of anaemia and iron- rich food sources was higher among the participants in this study. These differences might have resulted from the financial capacity of the females that could have limited their ability to purchase the foods as many are within the low and moderate income status. In addition, participants may have been engaging in iron-inhibiting foods and also reduced consumption of iron-enhancing foods, as the results showed that the majority had low knowledge of iron-enhancing and iron-inhibiting foods. Knowledge of iron-enhancing and iron-inhibition foods influences their consumption.21,22,32 Studies have shown that low economic status is associated with anaemia.17,29,33 In terms of classification, only a smaller percentage of the respondents were severely anaemic, with more than three-fourth presenting with mild to moderate anaemia. The pattern was similar to that of Sheriff et al. 29 This might have resulted from the knowledge and intake of the iron-rich food sources, when the income levels allowed it, and might account for the greater percentage of mild to moderate, compared with severe anaemia.
Anaemia was more prevalent among the married women than those who were single, a finding consistent with that of Sheriff et al. 29 and AlFaris et al., 34 studies from Sri Lanka and Saudi Arabia, respectively. This might be because the majority of the participants were students whose eating habits could easily be influenced into making poor food choices, 35 irrespective of their good knowledge levels in iron-rich foods. Again, it may be that the married women were largely found in the low and moderate income brackets, hence affecting their purchasing power.
Anaemia was highest among the pre-tertiary participants. This finding is consistent with studies36,37 which indicated that anaemia is more prevalent in non-pregnant women with a lower educational level in China. The findings are, however, contrary to Amoaning et al., 38 which showed that the prevalence of anaemia is high among tertiary students in Ghana. The observation in this study might have resulted from the poor knowledge of iron-inhibiting and enhancing foods. The pre-tertiary group, mostly people in late adolescence, are also known to have poor food choices which culminate in anaemia,20,39 and this might have accounted for this observation. The findings further showed that participants with a higher education level had low prevalence of anaemia, and this may be attributed to the fact that they could read and understand issues related to anaemia and iron foods. Moreover, those participants may be gainfully employed and earning a good enough income to buy a variety of foods and to eat from diverse sources of food.
In this study, anaemia was highest among WRA with a lower income. This finding is similar to other studies conducted in Rwanda 31 and China. 37 Although people might have knowledge, the lower level of economic freedom will limit what an individual can purchase. The income status of an individual is known to have an effect on the purchasing power, irrespective of educational knowledge. This is because iron-rich foods, which mostly happen to be animal-sourced foods are expensive, and the majority of the participants (tertiary and pre-tertiary) might have to depend on parents/relatives as they might not be fully engaged in an occupation that can increase their income levels. This observation might have resulted from not putting into use the knowledge on the iron-rich food sources or the frequent intake of iron-inhibiting and enhancing foods, due to inadequate knowledge.
The outcome of the current study revealed that income status was significantly associated with anaemia. This finding is in agreement with Ali et al., 40 which showed that poor economic status is an instigator of anaemia among women in Pakistan. Education has been shown to be associated to anaemia among pregnant women in Pakistan, 41 which was contrary to the findings of this study. The differences could have resulted from the higher educational levels of our study participants.
Practical applications
To address the high prevalence of anaemia and inadequate awareness of iron foods among WRA, we call for a multi-sectoral and comprehensive strategy. This comprises nutrition/health education (anaemia: causes, signs, and symptoms, prevention and management, repercussions; iron foods: iron-rich, iron-enhancing, and iron-inhibiting foods, as well as hygiene), deworming, improved healthcare access and economic empowerment. We recommend that governments, organizations and future researchers prioritize several key dimensions to improve women’s education, healthcare access and access to credit for farming (iron-rich foods such as poultry and livestock, iron-boosting foods such as fruits and vegetables) or agribusiness among WRA. We propose using qualitative and quantitative methodologies to address the intake of iron-rich and iron-enhancing foods as barriers to the timely prevention and management of iron deficiency anaemia in WRA, as well as identify the factors that contribute to excessive iron-inhibiting food consumption. Furthermore, we suggest looking into the relationship between anaemia and hygiene in WRA. Finally, we propose intervention studies that include nutrition education, hygiene practices, cooking demonstration or food fair, deworming and economic empowerment of women, such as including women in animal or iron food farming to boost consumption and sales and make extra cash in low-income settings.
Strengths and limitations
This study provides insight into the knowledge level of iron deficiency anaemia and iron foods, and prevalence of anaemia and its precipitating factors among non-pregnant and non-lactating WRA. As a limitation to this study, the outcomes could not be generalized due to the exclusion of pregnant and lactating WRA. Due to the adoption of a cross-sectional approach, a causal relationship could not be established between variables.
Conclusion
Knowledge about anaemia was high, however, it was limited in terms of iron foods. There was a high prevalence of anaemia among WRA. Income status was significantly associated with anaemia. Nutrition education about the relevance of iron-enhancing and iron-inhibiting foods, sources of iron food and appropriate dietary practices of iron foods should be promoted by health professionals in health facilities, durbars and the media. Academic institutions are encouraged to introduce nutrition education as part of the curriculum in all aspects of the academic ladder aimed at awareness creation of anaemia and iron foods. Organizations with interest in WRA should also focus on empowering them economically to increase their purchase of a wide variety of foods, including iron-rich and iron-enhancing foods.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241263826 – Supplemental material for Knowledge, prevalence and factors associated with anaemia among women of reproductive age in Tamale Metropolis, Ghana: A cross-sectional study
Supplemental material, sj-docx-1-whe-10.1177_17455057241263826 for Knowledge, prevalence and factors associated with anaemia among women of reproductive age in Tamale Metropolis, Ghana: A cross-sectional study by Michael Akenteng Wiafe, Georgina Benewaa Yeboah, Emmanuel Gyamerah, Happy Dubique Konlaa, Ikimah Ibrahim and Anita Benewaa in Women's Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057241263826 – Supplemental material for Knowledge, prevalence and factors associated with anaemia among women of reproductive age in Tamale Metropolis, Ghana: A cross-sectional study
Supplemental material, sj-docx-2-whe-10.1177_17455057241263826 for Knowledge, prevalence and factors associated with anaemia among women of reproductive age in Tamale Metropolis, Ghana: A cross-sectional study by Michael Akenteng Wiafe, Georgina Benewaa Yeboah, Emmanuel Gyamerah, Happy Dubique Konlaa, Ikimah Ibrahim and Anita Benewaa in Women's Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.