
Abstract
Background:
Obesity is associated with decreased physical performance, especially in older individuals. Some studies have examined the impact of exercise on obesity outcomes as part of a palliative care program.
Objective:
This parallel-group randomized controlled trial investigated the effects of water-based aerobic exercise training and vitamin D3 supplementation on body mass index (BMI) and physical performance in postmenopausal women who were overweight or obese and had insufficient or deficient levels of serum vitamin D.
Design:
This was an experimental study.
Methods:
Forty women were randomly assigned to one of four groups: Water-based training + vitamin D (WTD), water-based training (WT), vitamin D (D), and control. The training program (aerobic-based exercise) and vitamin D3 supplementation were conducted for 8 weeks, three times a week. Measurements were taken before and after the intervention.
Results:
The WTD group showed significant improvement in BMI, handgrip strength, and gait speed compared to all other groups (p > 0.05), and significant enhancements in right and left leg static balance and gait speed compared to the D and control groups (p < 0.05). The WT group demonstrated improvements in handgrip strength compared to the control group and enhancements in right and left leg static balance and gait speed compared to the D and control groups (p < 0.05). Vitamin D3 supplementation improved handgrip strength compared to the control group (p < 0.05).
Conclusion:
Water-based training with or without vitamin D3 supplementation significantly improved physical fitness indices, with combination showing the most pronounced effects. Vitamin D3 supplementation alone did not have a significant impact on most physical fitness measures.
Introduction
With the global aging population, the number of postmenopausal women experiencing functional decline is rising rapidly. Recent data indicate that more women aged >60 years report limitations in daily activities due to physical impairments, compared to men in the same age group. 1 Physical performance is an important indicator of aging and is influenced by various factors including menopause. Surgical or natural menopause is associated with significant declines in physical performance, primarily due to the loss of estrogen which plays a critical role in maintaining muscle mass, strength, and metabolic function.2,3
Obesity further exacerbates these challenges, as it is biologically linked to decreased physical performance, especially in older individuals. 4 Estrogen deficiency during post-menopause contributes to obesity, negatively influencing muscle mass and bone density 5 and increasing cardiac limitations 6 which can result in poor physical performance. Several longitudinal studies have shown that postmenopausal women experience a rapid decline in grip strength 7 and gait speed. 8 Grip strength measures muscle strength in older adults, and low handgrip strength is associated with poor health status, higher chronic comorbidities, functional deficiencies, and all-cause mortality. 9 Gait speed is determined by the interaction of sensory perception, muscle strength, and sensory-motor, and declines with aging in older women. 10 Reductions in gait speed are related to sarcopenia and frailty, as well as disability and mortality. 11 Balance is a key component of performance for older people in their daily activities, and its impairment is related to the risk of falling and related morbidity and mortality. It has been reported that balance deteriorates in postmenopausal women. 12
Therefore, improving muscle mass, strength, and cardiovascular system can be a target for improving physical functioning. Given the critical role of vitamin D in muscle function and bone health, its potential impact on improving muscle mass, strength, and cardiovascular outcomes has been widely investigated. Many studies have indicated a negative association between serum vitamin D and obesity in the elderly. 13 While vitamin D supplementation has been proposed to improve muscle strength 14 and handgrip performance, 15 its efficacy appears to depend on duration and baseline status. Long-term supplementation (⩾6 months) has shown mixed results; however, emerging evidence suggests that measurable improvements in physical performance and vitamin D status can occur within 8–12 weeks, particularly when combined with structured physical activity.16 –18 Some trials report no significant improvements in muscle strength or gait speed despite normalized serum vitamin D levels following 6 months of vitamin D supplementation. 19
Importantly, combining vitamin D with exercise may amplify its effects. This synergy likely arises from vitamin D’s role in modulating pathways like AKT/mTOR signaling and oxidative stress reduction 20 which are also activated by exercise. 21 For instance, short-term interventions (8–12 weeks) involving aquatic training and moderate-dose vitamin D supplementation have demonstrated improvements in muscle function and physical performance in older populations.22,23 However, some trials report no significant improvements in muscle strength or gait speed despite normalized serum vitamin D levels following 6 months of supplementation. 24 These discrepancies may be attributed to differences in study design, dosage regimens, baseline vitamin D status, and the type and intensity of physical activity.
Water-based exercise is a combination of resistance and aerobic exercise performed in water, offering unique benefits such as reduced joint strain and improved postural control. 25 Previous findings have shown that water-based or resistance exercise lasting 12 weeks–9 months can influence strength, balance, and cardiorespiratory fitness in older adults differently.26 –28 Given that long-term adherence to structured exercise programs can be challenging, identifying effective short-duration interventions is crucial for clinical applicability and participant compliance. Regarding vitamin D supplementation, moderate doses (400–1000 IU/day) have been shown to effectively raise serum 25(OH)D levels without the risks associated with high-dose regimens. 29 Although higher doses (>1000 IU/day) have been tested in some trials, recent evidence indicates limited additional benefit on physical performance outcomes in older adults. 30 Moreover, excessive vitamin D intake carries the risk of hypercalcemia and toxicity, particularly in sedentary populations with low baseline requirements. 31
Water-based exercise is usually performed in indoor swimming pools, which may contribute to vitamin D deficiency. 32 However, no study has been found to explore the effects of indoor water-based training and vitamin D3 supplementation on physical function. Given the correlation between vitamin D and physical fitness indices,14 –16 this study aimed to investigate the effects of an 8-week water-based aerobic training program combined with moderate-dose vitamin D3 supplementation on body mass index (BMI) and physical performance indices—such as grip strength, gait speed, and static and dynamic balance—in overweight or obese postmenopausal women with insufficient or deficient serum vitamin D levels.
Materials and methods
Study design and participants
This study was a parallel-group, double-blind (assessors and statisticians), randomized controlled trial conducted in Shiraz, Iran, from January to March 2023. The intervention period lasted 8 weeks, with assessments performed before (pre-intervention) and after (post-intervention) the program. The inclusion criteria were: natural menopause, at least 10 years following the last menstruation, no vitamin D supplementation during the 5 months before the test, serum vitamin D insufficiency (20–30 ng/ml), age range of 60–70 years, being overweight (BMI: 25–29.9) or obese (BMI >30), insufficient (20–30 ng/ml) or deficient(<20 ng/ml) serum concentrations of 25(OH)D, not suffering from metabolic and hormonal diseases affecting the variables, no cardiovascular or physical diseases preventing sports activities, and not sports participation for at least 5 months. Exclusion criteria were previous hysterectomy, not following the exercise program or vitamin D supplementation, and any changes in daily physical activity and nutrition reported weekly.
A total of 95 women were initially assessed for eligibility, of which 51 were excluded due to not meeting inclusion criteria (n = 15), declining participation (n = 30), or other unspecified reasons (n = 10). Of the 44 randomized participants, 12 were assigned to the water-based training plus vitamin D group, 11 to the water-based training group, and 11 to the vitamin D group. During follow-up, a total of four participants were excluded from analysis: three due to lack of regular participation in exercise sessions or vitamin D consumption, and one due to discontinuation of the intervention (because of catching a cold). Thus, 40 participants completed the study and were included in the final analysis, with 10 in each treatment group. This study adhered to the CONSORT 2010 guidelines for reporting parallel-group randomized trials. A CONSORT flow diagram is provided as Supplemental Material.
A priori sample size calculation was conducted using G*Power software version 3.1.9.7. 33 Based on previous studies evaluating the effects of combined exercise and vitamin D supplementation on physical fitness indices (e.g., BMI, handgrip strength, gait speed), 34 an effect size of f = 0.071 was selected as a conservative estimate to detect significant differences among the four intervention groups (alpha = 0.05, power = 0.80). This resulted in a minimum required sample size of 10 participants per group. Although this sample size is relatively small, it was based on practical constraints such as participant availability and resource limitations. In addition to the a priori sample size calculation, a post hoc power analysis was conducted using the observed effect sizes (partial η²) from the analysis of covariance (ANCOVA) results to assess the achieved statistical power. For example, for handgrip strength (partial η² = 0.95), the corresponding effect size (f = 0.44) yielded a post hoc power of over 95%. Similarly, high power levels (>90%) were observed for other key outcomes including BMI (partial η² = 0.848, f = 0.39, power >90%), gait speed (partial η² = 0.978, f = 0.69, power >99%), and dynamic balance (partial η² = 0.955, f = 0.45, power >95%). These findings indicate that despite the relatively small sample size (n = 10 per group), the study had sufficient statistical power to detect significant differences among the four intervention groups.
The ethical recommendations of the Declaration of Helsinki (1975, revised in 1983) were followed in this study. Participants signed a written informed consent form and the study proposal and procedures were approved by the Ethics Committee at Shiraz University of Medical Sciences, School of Medicine (No: IR.SUMS.REC.1400.466).
Procedures
Before the study, blood samples were collected to evaluate serum 25(OH)D levels. Participants were randomized using a computer-generated randomization sequence (block size of 4) stratified by BMI. Allocation concealment was maintained using sealed, opaque envelopes generated by an independent researcher not involved in assessments or data analysis. Due to the higher likelihood of a decrease in the number of subjects in the intervention groups, the number of subjects was considered as follows: (1) water-based training + vitamin D3 intake (WTD; n = 12), (2) water-based training without vitamin D3 intake with placebo intake only (WT; n = 12), (3) vitamin D3 intake group (D; n = 11), and (4) control group (CON; n = 10). Regarding exclusion criteria, final analysis was performed on four groups of equal number (n = 10). Assessors and statisticians were blinded to group assignments. Participants in the vitamin D and placebo groups could not distinguish between supplements due to identical packaging.
To comply with ethical principles, after the treatment period, water-based exercise facilities were provided for the non-exercise groups, and vitamin D3 supplements were provided for the non-vitamin D group. In addition, the nutritional habits of participants were recorded at the beginning and end of the intervention, and they were recommended not to use any supplements other than vitamin D in related groups. Participants were asked to maintain their habitual dietary patterns and report any lifestyle changes (diet or physical activity) throughout the study period. Blood samples were taken before and after the intervention to measure serum vitamin D levels. The health of all groups was monitored by a physician every 15 days.
Measurements
The participants performed functional tests (walking speed, static balance of both legs, dynamic balance and handgrip strength) before and after the intervention program. One week prior to the tests, they were familiarized with the procedures.
Forty-eight hours before and after the training sessions, all tests were conducted with suitable walking shoes and clothes. The BMI of participants was estimated using the formula: weight (kg)/height (m)2. Weight and height were measured using a stadiometer scale (Anea scale, made in Iran) while the participants were minimally clothed and barefoot.
To perform the gait speed (10-m walking) test, participants stood still then walked 10 m at their usual pace. The time of walking was recorded using a stopwatch. If the walking speed was faster or slower than the usual walking speed, the participant was asked to perform the test again. Walking time was measured as the 100th of a second. The walking speed was estimated by dividing the distance of 10 m by the walking time (m/s). 35 The good validity and reliability of the test were approved for older people. 35
To assess static balance, participants performed a valid and reliable one-leg standing balance test alternately on the right and left legs. They were asked to stand barefoot and then stand on one leg, bend the contralateral knee backward 90°, and maintain a vertical thigh position parallel to the supporting leg. Tests were performed alternately on the right and left legs, and they were allowed a 10-s rest between trials. If they stood on one leg for 30 s (recorded with a stopwatch), this was recorded as one-leg standing balance time for that particular leg. If 30 s was not reached, allow up to three attempts until 30 s are reached; otherwise, the maximum time of three attempts was recorded. The total standing one-leg duration was calculated as the sum of time of the one-leg standing of the right and left legs. 36 The validity and reliability of the one-leg standing balance test have been approved by a previous study. 37
Dynamic balance was measured by timing participants as they stood up from a chair, walked 2.44 m, turned around, walked back to the chair, and sat down on the chair again. The time required to complete the test was recorded. The tests validity has been previously established. 38
Handgrip strength was measured using a digital hand dynamometer 39 to the nearest 0.1 kg. Participants stood upright with feet hip-width apart, and elbows extended. They then performed the maximum grip strength test with a dynamometer three times with each hand. The participants held the dynamometer at their maximum strength for about 3 s. After at least 30 s of rest, the next measurement was performed. The maximum value among the six measurements by both hands was considered the handgrip strength. 39 The validity of the hand rip test has been approved as good. 40
Training program
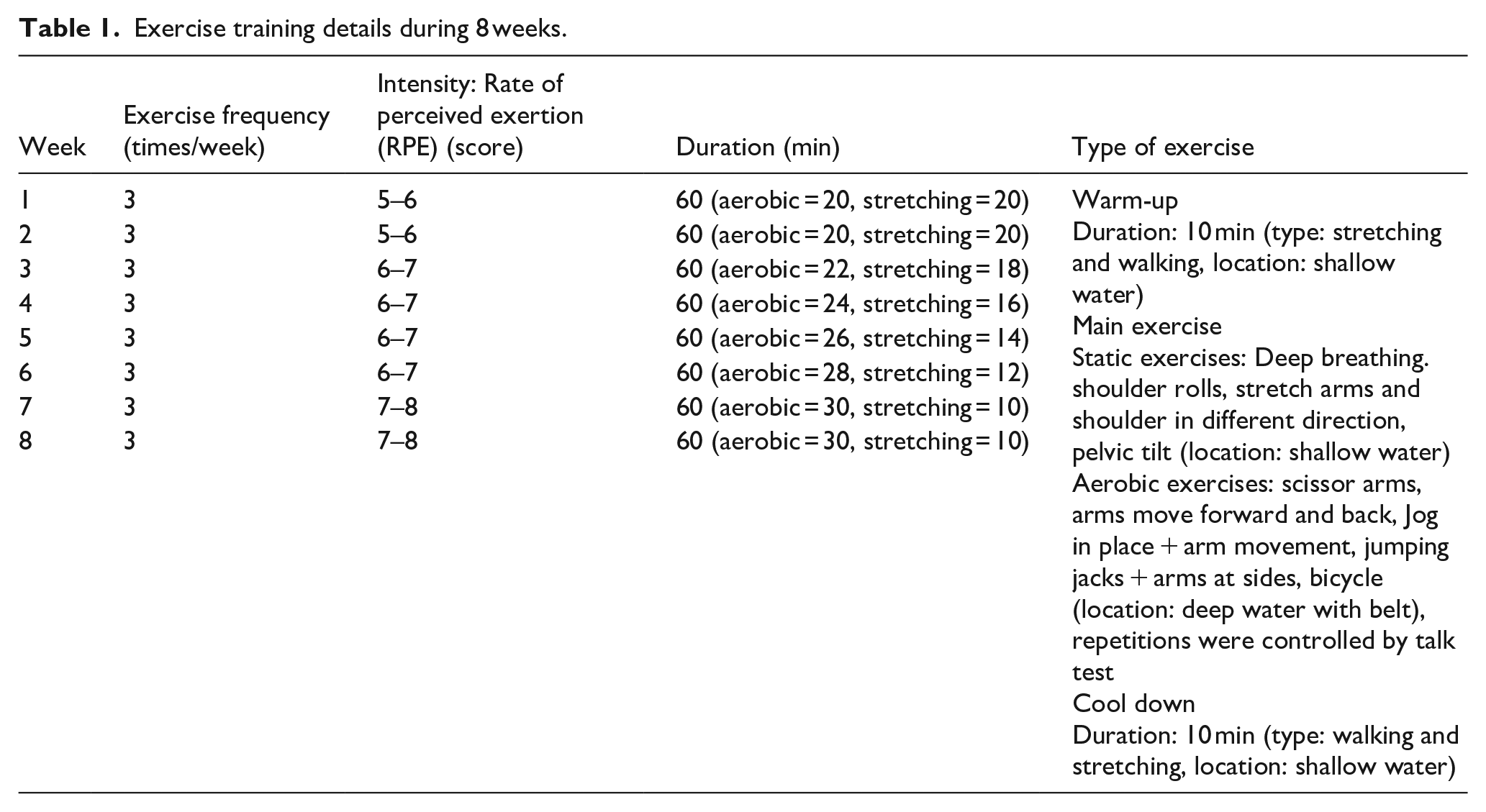
Both training groups (AT and WTD) participated in water-based aerobic exercises for 8 weeks, with three sessions per week and lasting 60 min each session. The other groups did not engage in any exercise training. At the beginning of each session, warm-up exercises were performed for 10 min. The exercises included stretching and flexibility movements and low-intensity walking in water. The main exercise training program included aerobic water exercises. During the first and second weeks, the participants performed 20 min of aerobic exercises, including fast walking and aerobic rhythmic water exercises intended to increase cardiovascular endurance, balance, and muscle strength, especially for the lower limbs.
Over the following 6 weeks, the duration of aerobic exercise gradually increased reaching 40 min in the seventh and eighth weeks, by extending the walking distance and repetitions of rhythmic movements. During the recovery phase, the participants walked slowly in water for 10 min and performed light stretching movements while floating.
Training intensity was measured based on the Borg scale (1–10). During the first and second weeks of training, the intensity was about at a five to six level until it was increased to seven to eight during the seventh and eighth weeks. Due to the feasibility of the talk test and its correlation with the Borg scale,41,42 we used a talk test to control for intensity and rate of perceived exertion. The details of exercise training are listed in Table 1.
Exercise training details during 8 weeks.
Vitamin D3 supplementation
Participants were selected based on their serum vitamin D levels. A blood level of at least 30 ng/ml was considered sufficient, 20–30 ng/ml as insufficient, less than 20 ng/ml as deficient, and less than 7 ng/ml as severely deficient. 43 Participants were chosen from those with insufficient (20–30 ng/ml) or lower-level sufficient vitamin D (30–35 ng/ml). According to available documents 44 and physician recommendations, a moderate oral dose of 400 IU/day of vitamin D3 was prescribed for 2 months to the vitamin D patients with insufficient vitamin D and 1000 IU/day for patients with deficient vitamin D.
Statistical analysis
Statistical analyses were conducted using IBM SPSS Statistics version 23 (IBM Corp., Armonk, NY, USA). Descriptive statistics were presented as mean ± standard deviation (SD). Normality was assessed using the Shapiro–Wilk test. To ensure the appropriateness of ANCOVA, we tested the assumption of homogeneity of regression slopes by examining the interaction term between group and baseline scores. Non-significant interactions indicated that this assumption was satisfied. Multicollinearity among baseline covariates and outcome variables was assessed using variance inflation factor, with all values below 5, indicating acceptable independence among predictors.
Regarding the meeting of assumptions, the statistical test of ANCOVA was used for overall between-group comparisons, and in the case of significant findings, the Tukey’s honestly significant difference test was employed for post hoc pairwise comparisons, which appropriately adjusts for multiple comparisons by controlling the experiment-wise error rate across all pairwise contrasts. Partial η² was extracted from ANCOVA for use in power analysis. For all significant comparisons, partial η² was calculated to estimate effect sizes when comparing repeated measures of pre- and post-interventions in each group.
Results
The study included 40 postmenopausal women (mean age: 65.3 ± 3.4 years) with obesity or overweight (BMI range: 44.9–46.8 kg/m²) and insufficient/deficient serum 25(OH)D levels (20–30 ng/ml). All participants were naturally postmenopausal (⩾10 years since last menstruation) and reported no structured physical activity for ⩾5 months prior to the study (Table 2). No significant differences were observed between groups at baseline for age, BMI, or serum vitamin D levels (p > 0.05, Table 3). The mean age of participants was 65.1 ± 3.21 years in the WTD group, 65.2 ± 3.48 years in the WT group, 66.00 ± 3.56 years in the D group, and 65.4 ± 3.28 years in the control group indicated no significant difference between groups (F = 0.377, p = 0.770). All participants were sedentary and had either insufficient (serum vitamin D: 20–30 ng/ml) or deficient (<20 ng/ml) vitamin D levels at baseline. The demographic characteristics of participants are presented in Table 2.
Demographic characteristics of participants.

Values are mean ± SD. BMI: body mass index; SD: standard deviation.
Comparison of walking speed, left and right foot balance in study groups by ANCOVA test.
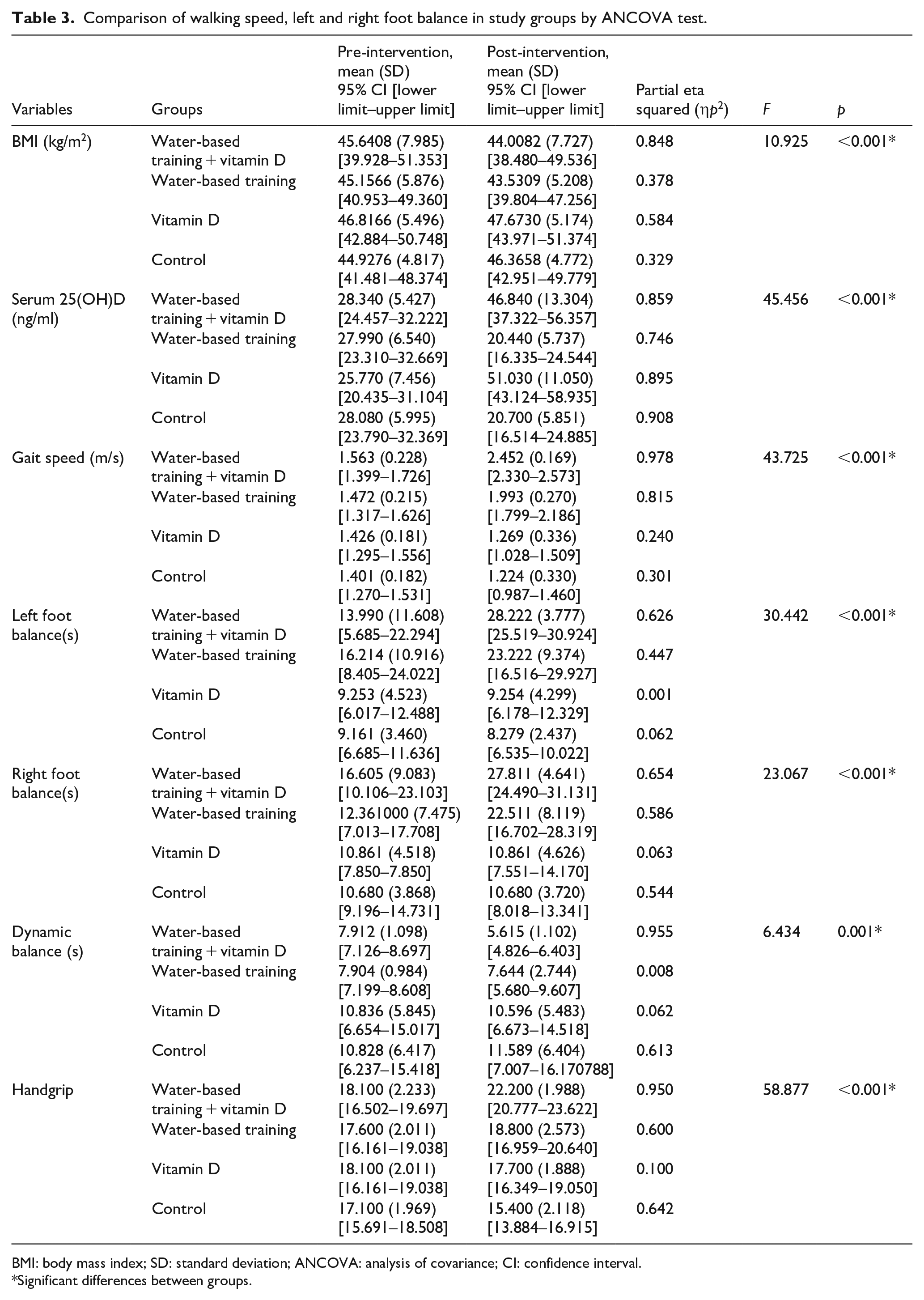
BMI: body mass index; SD: standard deviation; ANCOVA: analysis of covariance; CI: confidence interval.
Significant differences between groups.
According to the findings in Table 3, there was statistically significant difference in post-intervention BMI (F = 10.925, p < 0.001), gait speed (F = 43.726, p < 0.001), left foot balance (F = 30.442, p < 0.001), right foot balance (F = 23.067, p < 0.001), dynamic balance (F = 6.434, p = 0.001), and handgrip (F = 58.877, p < 0.001) considering pre-intervention as a covariate.
Additionally, as shown in Table 2, partial findings of the study indicated that post-intervention serum 25(OH)D was significantly different between groups (F = 45.456, p < 0.001). Paired group comparisons showed that increase in the serum 25(OH)D level in the groups of vitamin D3 supplementation, including WTD (η p ² = 0.859) and D (η p ² = 0.895) was higher than the CON and WT (p < 0.001). There was no significant difference between other paired groups (p > 0.05).
Both the WTD and WT groups experienced significant reductions in BMI. The combined WTD group showed the largest effect size, with partial η p ² = 0.848. Post-intervention BMI in the WTD group was 44.0 kg/m² (95% confidence interval (CI): 38.5–49.5), significantly lower than pre-intervention levels and significantly lower than the D group (47.7 kg/m² [44.0–51.4], p = 0.005) and the control group (46.4 kg/m² [43.0–49.8], p = 0.001). The WT group also showed a reduction (43.5 kg/m² [39.8–47.3]), with similar significance compared to D and control groups (Tables 3 and 4 and Figure 1).
Paired group comparison of variables.

BMI: body mass index.
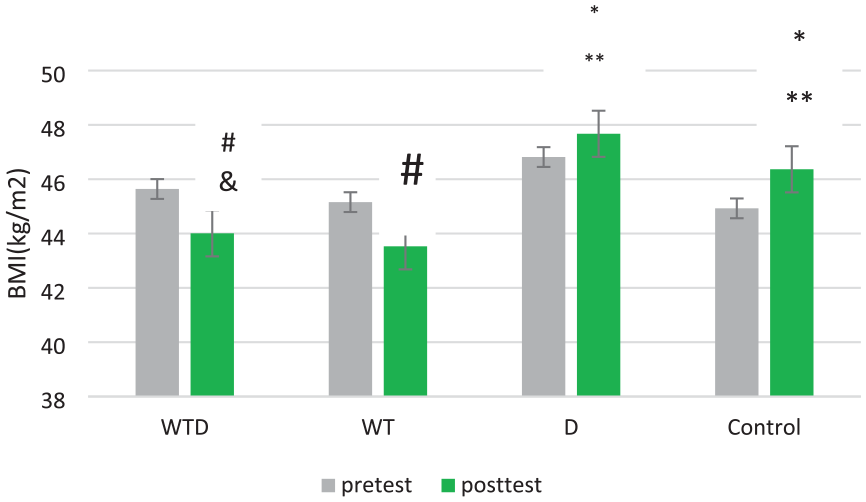
Comparison of post-intervention of BMI (kg/m2) among the four study groups. Bars represent mean values with error bars indicating 95% confidence intervals.
The most substantial improvement in gait speed was observed in the WTD group (η p ² = 0.978), followed by the WT group (η p ² = 0.815) both indicating very large effect sizes. Post-intervention gait speed in the WTD group was 2.45 m/s (95% CI: 2.33–2.57), significantly higher than in the WT group (1.99 m/s [1.80–2.19], p < 0.001), the D group (1.27 m/s [1.03–1.51], p < 0.001), and the control group (1.22 m/s [0.99–1.46], p < 0.001). The WT group also showed improvement over both the D and control groups, although the effect sizes were smaller. There was no significant difference between the D and control groups (p = 0.808; Tables 3 and 4 and Figure 2).

Comparison of post-intervention gait speed (m/s) among the four study groups. Bars represent mean values with error bars indicating 95% confidence intervals.
Both left and right foot balance improved significantly in the WTD group, with partial η p ² values of 0.626 and 0.654, respectively, representing moderate to large effects. In contrast, the D group showed minimal changes in balance performance (η p ² < 0.01). For static balance, left-foot balance increased in the WTD group (28.2 s [25.5–30.9]) compared to the WT (23.2 s [16.5–29.9], p < 0.05), D (9.3 s [6.2–12.3], p < 0.001), and control (8.3 s [6.5–10.0], p < 0.001). Similar improvements were observed in right-foot balance in the WTD group (27.8 s [24.5–31.1]; Tables 3 and 4 and Figure 3).
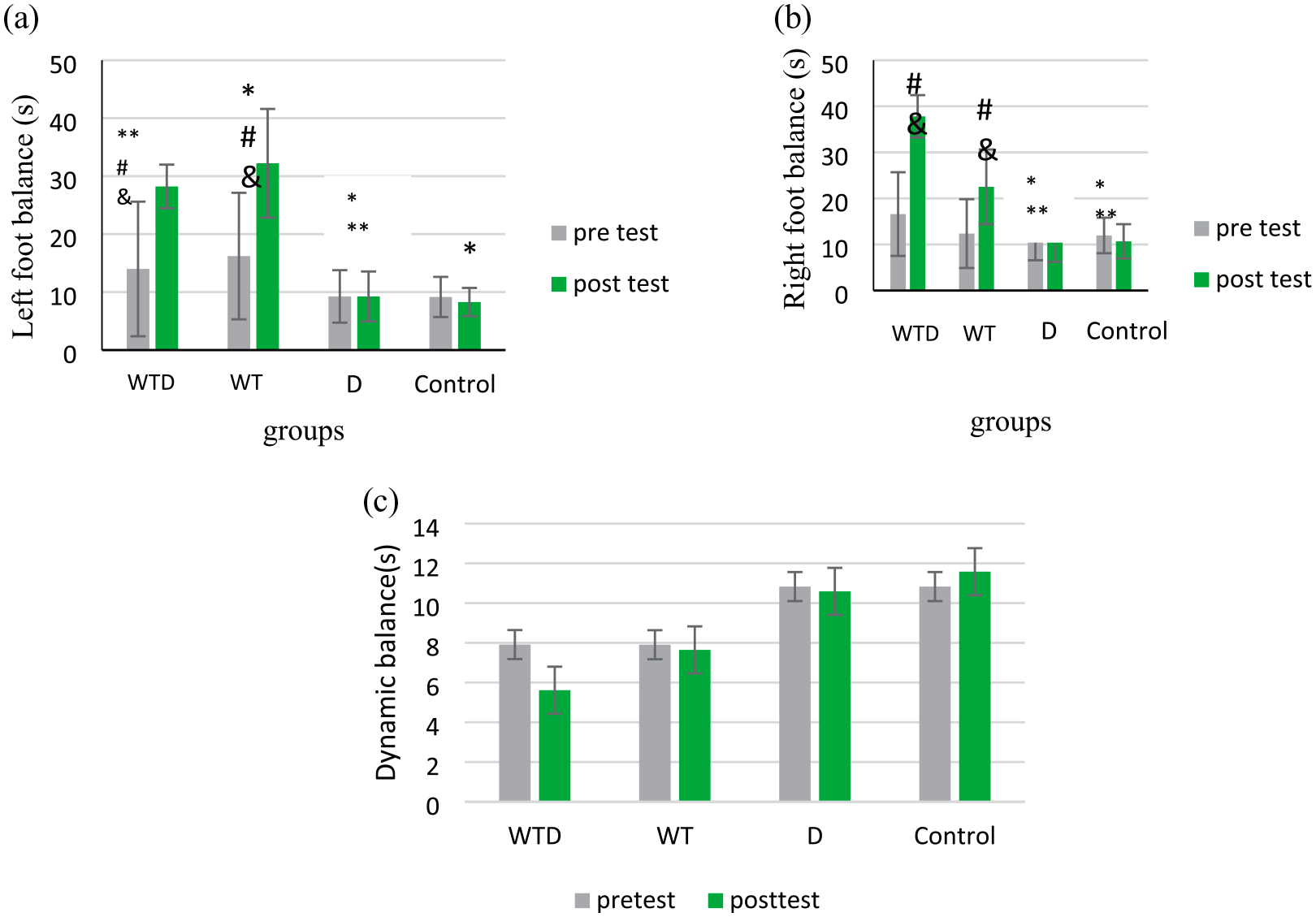
Comparison of post-intervention of left (a) and right (b) foot and dynamic balance (c) balance(s) among the four study groups. Bars represent mean values with error bars indicating 95% confidence intervals.
The combined intervention group demonstrated a marked reduction in dynamic balance time, with a large effect size (η p ² = 0.955). Dynamic balance improved significantly in the WTD group (5.6 s [4.8–6.4]) compared to the D group (10.6 s [6.7–14.5], p = 0.034) and the control group (11.6 s [7.0–16.2], p = 0.001). No significant differences were observed among the other group comparisons (Tables 3 and 4 and Figure 3).
The greatest increase in handgrip strength was found in the water-based training + vitamin D group (η p ² = 0.95), indicating a very large effect of the intervention. The water-based training group also showed a moderate effect (η p ² = 0.6), whereas the vitamin D-only group had a negligible effect (η p ² = 0.1). Post-intervention handgrip strength was significantly higher in the WTD group (22.2 kg [20.8–23.6]) compared to the WT group (18.8 kg [16.9–20.6], p < 0.001), the D group (17.7 kg [16.3–19.1], p < 0.001), and the control group (15.4 kg [13.9–16.9], p < 0.001). The WT group showed greater handgrip strength than the control group (p < 0.001), and the D group also showed improvement over the control group (p = 0.001). However, no significant difference was found between the WT and D groups (p = 0.112; Tables 3 and 4 and Figure 4).

Comparison of post-intervention handgrip (kg) among the four study groups. Bars represent mean values with error bars indicating 95% confidence intervals.
A part of this study was previously published and indicated that the serum 25(OH)D level in the WTD was higher than WT and CON, and in the D was more than the CON and WT. 24
Discussion
This study investigated the effect of water-based exercise and vitamin D3 supplementation on physical fitness indices in overweight and obese postmenopausal women with insufficient or deficient vitamin D levels. The results indicate that both interventions—water-based training alone and in combination with vitamin D3—improved physical fitness measures such as BMI, gait speed, balance, and handgrip strength, with the combined intervention showing the most pronounced benefits. Vitamin D3 supplementation alone had limited effects, primarily improving handgrip strength but not significantly affecting other variables.
Considering gait speed, the findings of the present study indicated that WTD and WT increased gait speed, whereas vitamin D3 supplementation was not significantly effective on gait speed. In other words, water-based exercise increased gait speed and vitamin D3 supplementation enhanced the effect of exercise. Consistent with our findings, resistance and balance exercises were effective on gait speed in patients with acute coronary syndrome. 45 Water-based exercise for 8 weeks in older women has increased lower limb muscle strength and improved gait speed compared to the control group, which was similar to the results of our study. 46 Water-based exercises are performed with the resistance of water and performing exercises in water require balance, both of which may contribute to increasing gait speed. Decreased bone function and muscle weakness in the lower limbs due to the aging process lead to changes in walking patterns in older individuals. Decreasing gait speed is the most obvious change in walking patterns, and is strongly correlated with decreased balance and the risk of falling. 47 Therefore, there is a need for sufficient muscle power and strength during walking. Endurance or strength training can help increase the strength of the muscles in the lower limbs and improve the balance system in older individuals. According to a review study, water-based exercise, especially for older individuals, results in better physical performance in terms of improving walking patterns than exercise on land. Another reason for gait speed enhancement can be justified by the fact that a major part of progress in the initial sessions of exercise training is the result of neural adaptations that are related to learning, coordination of movements, and the brain’s ability to use more motor units. In later stages of training, however, improvements in gait speed are more strongly influenced by muscle hypertrophy and increased bone and muscle strength. 48
Considering the enhancing effect of vitamin D3 supplementation, consistent with our findings, taking vitamin D along with resistance training has shown an increasing effect on skeletal muscles in older people; therefore, it has a significant effect on functional factors, including improving gait speed. 28 There is a close relationship between vitamin D intake and bone health, muscle, and bone function. 49 A review study found that walking speed was slower in older adults with hypovitaminosis D. 16 In confirmation of our findings, a study indicated that in older adults with low serum 25-hydroxyvitamin D level and high risk of falling, high-dose vitamin D supplementation, ⩾1000 IU/day, did not improve measures of physical function compared to 200 IU/day. 50 Although the consumption of vitamin D3 in this research increased serum vitamin D, firstly, this increase in serum 25(OHD) was higher in the combined interventions as WTD group compared to the D group, and secondly, perhaps this increase was not effective on muscle function and gait speed. Due to approved correlation between speed and BMI, 51 the effect of WTD and WT on reducing BMI in these two groups can be another effective factor on gat seed. Also, it is possible that the effect of water-based training was more prominent than vitamin D on gait speed.
Regarding balance, our data indicate that water-based training significantly improves static balance compared to control conditions, while dynamic balance showed less pronounced changes. Vitamin D3 supplementation did not show any positive effect on static or dynamic balance. Sadeghi et al. demonstrated that water-based exercise could effectively enhance balance. 52 Two systematic reviews also supported the positive impact of water-based exercise on balance suggesting it as an alternative to land-based exercise for improving dynamic balance.53,54 Probably water-based exercise can enhance balance in older individuals by providing resistance to physical movements, as movements walking in water require balance which may act as an improving factor for balance.
Our study also found a positive effect of combining vitamin D with water-based training. Vitamin D3 supplementation alone had limited effects on physical fitness indices. Although it significantly improved handgrip strength compared to the control group, no significant differences were observed when comparing the D group to the WT group or the combined WTD group. These findings suggest that vitamin D3 supplementation alone may offer modest benefits in improving muscle strength, particularly in individuals with insufficient or deficient levels, but its greatest impact is seen when combined with water-based aerobic training. Renerts et al. indicated that combining sports activity with vitamin D3 supplementation can increase bone mass and improve functional factors including balance. 55 Another study found that vitamin D supplementation, especially in severely deficient patients, could improve balance. 56 Participants in the present study were selected from patients with insufficient and lower level of sufficient serum 25(OH)D level. Thus, vitamin D3 supplementation might not be so effective on physical function, although it increases their serum vitamin D. Another reason for the lack of a significant effect of vitamin D on balance may be the amount of supplementation, which needs future clarification.
The decline of neuromuscular, musculoskeletal, and sensory systems with age can lead to difficulties in maintaining balance. Most likely, the reason for this phenomenon deterioration in proprioception 57 and muscle weakness 58 in older women. Therefore, improving the endurance and muscle strength of the lower limbs of older women may enhance the efficiency of the motor nervous system and strengthen the muscles and joints receptors. 59 Water-based exercise which combines resistance and endurance improved balance in our study. Additionally, considering the relationship between BMI and balance, 60 reducing BMI in the WTD and WT groups can be another effective factor in improving balance.
Handgrip strength improved most significantly in the group receiving both water-based training and vitamin D supplementation, followed by the exercise-only group, whereas vitamin D3 supplementation did not have a significant effect. A recent meta-analysis study has shown the positive impact of water-based exercise on muscle strength. 61 This type of training may have led to an increase in muscle mass, as a study found that training for more than 120 min/week was associated with improvements in body composition and muscle mass. 62 Similarly to our findings, no significant effect of vitamin D supplementation on handgrip strength has been found in older trauma patients. 15 In a study involving women with low 25(OH)D levels who consumed supplemental vitamin D or placebo, there was no benefit of 2800 IU/day of 25(OH)D versus placebo for grip strength and knee flexion strength. 63 A recent meta-analysis study also found a small but insignificant improvement in grip strength following vitamin D intake. 64 The dosage of vitamin D may not be the reason for its lack of a significant effect on handgrip strength or other physical functions, as a study found that high-dose vitamin D supplementation (⩾1000 IU/day) did not improve physical functioning indices compared to a lower dose (200 IU/day) in older individuals with low serum 25-hydroxyvitamin D levels. 50
The mechanisms by which vitamin D and exercise may affect skeletal muscle, and consequently muscle strength, likely involve increased expression of myogenic regulatory factors (such as MYOD, MYOG, MYC2, skeletal muscle fast troponin I and T, MYH1, IGF1 IGF2, FGF1 and FGF12, BMP4, MMP9, and FST), increased protein synthesis signaling via AKT, mTOR, and GSK3B; increased GLUT4 and GLUT1 translocation, improvement in interleukin-6 myokine release and inhibition of interleukin-6 protein which reduces oxidative stress.65,66 The consumption of vitamin D alone may not be effective on some physical fitness indices, but when combined with water-based exercise it has a synergistic effect.
Finally, BMI was reduced in both exercise groups, regardless of vitamin D supplementation, indicating that caloric expenditure and metabolic adaptations from regular aerobic activity are primary drivers of weight loss in this population. However, vitamin D3 alone did not show any significant effect on BMI. The reduction in BMI due to exercise may be attributed to a negative energy balance resulting from increased energy expenditure. Since participants did not report any significant changes in their diet, it is possible that their energy intake remained unchanged. Additionally, long-term exercise training can increase resting metabolic rate by promoting lean muscle mass. 67
Regarding vitamin D supplementation, while some studies have shown a positive effect on weight reduction in older adults, 13 the relationship between vitamin D and obesity is still unclear due to various limitations and factors. 68 In this study, swimming was conducted in an indoor pool, to control for the effect of sun exposure on serum vitamin D levels. Preliminary findings also suggested an increase in serum vitamin D levels in vitamin D3 supplementation groups, especially those receiving combined interventions. Therefore, the study highlights the more prominent effect of exercise training compared to vitamin D3 supplementation on BMI. Nevertheless, further research is recommended for clarification.
Strengths and limitations
Although this study was the first to evaluate the impact of water-based training with and without vitamin D3 supplementation on physical fitness indices in obese or overweight women with insufficient serum vitamin D levels at risk of impaired physical fitness, it had some imitations. One limitation of the present study was the inclusion of only women aged 60–70 years with natural menopause and no major comorbidities. This limits the generalizability of the findings to broader postmenopausal populations, particularly those with surgical menopause or younger or older age groups. Another limitation of the present study was the combination of participants with vitamin D insufficiency (20–30 ng/ml) and deficiency (<20 ng/ml) into a single cohort. Also, the study included the relatively small sample size. Although, post hoc power analysis confirmed sufficient statistical power (>90%) for detecting medium-to-large effect sizes, due to the relatively small sample size (n = 10 per group), further stratification into subgroups based on baseline vitamin D levels was not feasible. This approach may have masked potential differential effects of vitamin D supplementation in individuals with varying degrees of deficiency. Future studies with larger sample sizes are recommended to explore these subgroup differences more thoroughly. Another limitation of this study was the lack of detailed monitoring and quantification of participants’ dietary intake and caloric expenditure outside the intervention sessions. While participants were instructed to maintain their usual eating and physical activity habits and were asked to report any major lifestyle changes, no formal dietary tracking (e.g., food diaries, 24-h recalls) or caloric expenditure assessments were conducted. This lack of dietary control may represent a potential confounding factor, particularly for outcomes such as BMI and muscle strength, which can be influenced by nutritional status. Future studies should consider incorporating more rigorous dietary monitoring to better isolate the effects of the interventions.
Conclusions
In summary, water-based aerobic training emerges as a key intervention for improving multiple domains of physical fitness in postmenopausal women, with vitamin D supplementation offering additional benefits primarily in combination with exercise. Future research should explore longer-term interventions and varying dosages of vitamin D to better understand its role in enhancing physical performance alongside structured exercise programs.
Supplemental Material
sj-doc-1-whe-10.1177_17455057251361255 – Supplemental material for Vitamin D3 supplementation enhances the effect of aerobic water-based training on physical fitness indices in obese and overweight menopausal women: A randomized controlled trial
Supplemental material, sj-doc-1-whe-10.1177_17455057251361255 for Vitamin D3 supplementation enhances the effect of aerobic water-based training on physical fitness indices in obese and overweight menopausal women: A randomized controlled trial by Foroozandeh Zaravar, Golamhossein Tamaddon, Mohammadamin Safari, Leila Zaravar and Maryam Koushkie Jahromi in Women’s Health
Footnotes
Acknowledgements
We thank all participants of this study for their commitment and regular participation in this study program.
Ethical considerations
The study proposal and procedures were approved by the Ethics Committee at Shiraz University of Medical Sciences, School of Medicine (No: IR.SUMS.REC.1400.466).
Consent to participate
Participants signed a written informed consent form.
Consent for publication
Not applicable.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research did not receive any external specific funding agencies.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data related to this manuscript is available and will be provided upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.