
Abstract
Background
Vitamin D is a key nutrient in bone health and the vitamin D status of individuals with regular exposure to solar or artificial ultraviolet B (UVB) radiation is generally superior to those with limited exposure.
Objective
By means of a cross-sectional, observational design, explore the association of serum 25-hydroxy vitamin D (25(OH)D) concentrations and biochemical markers of bone turnover across a spectrum of vitamin D status by comparing women who regularly use tanning beds with women of minimal UVB exposure.
Methods
A total of 69 healthy women, ages 25–82 y, were recruited. Serum concentrations of 25(OH)D, intact parathyroid hormone (iPTH), leptin, bone-specific alkaline phosphatase (BAP), osteocalcin (OC), and C-terminal telopeptides of Type I collagen (CTx) were measured.
Results
There were no significant differences in age, height, weight, BMI and dietary intakes between groups. Serum 25(OH)D concentrations were significantly higher in tanners (n = 20) compared with non-tanners (n = 49) (p < 0.0001). Serum iPTH concentrations were lower in tanners than in non-tanners (p < 0.0001) and were negatively correlated with serum 25(OH)D concentrations (r = –4571, p < 0.0001). Of the bone turnover markers, only serum OC concentrations were lower in tanners compared with non-tanners (p = 0.0002). After adjusting for age and menopausal status, osteocalcin was negatively correlated (r = –0.0178; p = 0.04) with 25(OH)D and positively correlated with iPTH (r = 0.035; p = 0.05).
Conclusions
Our results show healthy women with regular UVB exposure via tanning beds have significantly greater vitamin D status and lower serum osteocalcin concentrations than those without and that there is a significant inverse relationship between serum serum 25(OH)D and osteocalcin concentrations which appears to be PTH-dependent.
Introduction
Vitamin D is classically known for its biological function in maintaining calcium homeostasis through its actions on the intestine and bone. 1,25-dihydroxyvitamin D (1,25(OH)2D), the active metabolite of vitamin D, increases intestinal calcium absorption and serum calcium concentration via the induction of both genomic and non-genomic mechanisms of calcium transport across the enterocyte. 1 In the bone, 1,25(OH)2D enhances the mobilization of calcium and phosphorus from stores during times of calcium deprivation by inducing stem cell monocytes to become mature osteoclasts, thus stimulating bone breakdown and the subsequent release of minerals into circulation. 2 A lack of vitamin D leads to secondary hyperparathyroidism which too accelerates bone breakdown. 1
There is also evidence for a direct anabolic effect of 1,25(OH)2D on bone. In animal models, both acute and chronic vitamin D treatment resulted in increased bone formation and an increase in the number of osteoblasts and osteoblast precursor cells.3,4 In vitro studies using osteoblast-like cells have demonstrated the effects of 1,25(OH)2D on mRNA, protein expression and enzyme activities; including effects on the regulation of collagen type I (major bone matrix protein), osteocalcin (most abundant noncollageneous bone matrix protein) and alkaline phosphatase activity (indicator of bone formation). 5
Although there is clear evidence that adequate vitamin D status has a positive effect on bone mineral density (BMD) in humans,6–8 results from studies exploring the relationship between vitamin D status and measures specific to bone formation in humans are more ambiguous. Presumably this is because the mineral homeostasis effects of vitamin D are intertwined with any direct role the vitamin has on bone metabolism. 5 Moreover, the majority of published reports exploring vitamin D status and biochemical markers of bone formation are limited to postmenopausal women and populations with compromised vitamin D status.9–13
Circulating concentrations of 25-hydroxyvitamin D (25(OH)D), the standard measurement of vitamin D status, are typically higher in individuals with increased exposure to ultraviolet B (UVB) radiation due to the cutaneous production of vitamin D from its precursor, 7-dehydrocholesterol.14–16 One investigation recently demonstrated that healthy individuals routinely exposed to artificial UVB light via tanning beds have significantly greater serum 25(OH)D concentrations and hip BMD z scores than those who do not. 17 While serum parathyroid hormone concentrations were assessed and found to be significantly lower in tanners, no other biochemical markers of bone turnover were reported.
Bone biochemical markers offer a dynamic assessment of the skeleton. They can be used to assess the balance between bone formation and resorption and can measure changes over short periods of time. 18 Additionally, bone markers can be used to predict response to therapy. In several controlled trials, baseline and/or changes in biochemical markers have been shown to be better predictors of antifracture efficacy than BMD measures.19–22
In the current study, our objective was to explore the association of serum 25(OH)D concentrations and biochemical markers of bone turnover across a spectrum of vitamin D status. Towards this end, we compared the vitamin D status and serum bone marker concentrations of healthy tanning and nontanning women. We included women from the age of skeletal maturity (~25 years) through older adulthood.
Subjects and Methods
Subject recruitment and testing procedures
The study described herein is part of a larger project to explore the relationship between vitamin D status and markers of general health in women. 23 All procedures involving human subjects received approval from the University of Missouri Health Sciences Institutional Review Board.
A total of 69 female subjects, ages 25–82 years, were recruited from the Columbia, Missouri, with advertisements posted via University of Missouri campus email and to local tanning salons and gyms/health clubs as previously described to be included in the study, participants had to be Caucasian females who were at least 25 years of age. Additionally, to qualify as a “Tanner,” women had to regularly use a broad spectrum (UVA and UVB) tanning bed at least once per week for a minimum of 4 months. “Non-Tanners” needed to have minimal daily sunlight exposure, as assessed by a screening questionnaire, and no tanning bed use. Exclusion criteria included exclusive use of high-pressure tanning beds, use of tobacco, use of vitamin D supplements other than regular multivitamins (≥400 IU); current or previous medical condition or medication affecting vitamin D status, bone health, or immune function; current use of hormone replacement therapy; use of ultraviolet radiation as medical therapy; regular exercise >7 hours per week; and pregnancy.
All study visits were conducted between late January and early June to obtain serum samples during the seasonal nadir for 25(OH)D. 16 Test visits of all qualified, consented subjects were scheduled between 7 am and 11 am to control for diurnal variations; they were also instructed to refrain from exercise and fast for 8 to 10 hours prior to testing. On the day of the visit, all subjects of childbearing age took a urine pregnancy test to confirm non-pregnant status.
Anthropometric measurements and questionnaire data
Each subject's weight was determined to the nearest pound and height was measured to the nearest 0.5 inch. With this data, Body Mass Index (BMI) was calculated for each subject.
All subjects completed several questionnaires including a one-page medical history form to obtain data on previous health conditions, menopausal status, use of medications and exercise habits; a brief sun exposure questionnaire developed for this study that assessed incidental and intentional sun exposure; and a Fitzpatrick skin typing survey, a well-established method of determining skin pigmentation and sun sensitivity. 24 A Registered Dietitian also conducted a diet history interview which included the Harvard Food Frequency Questionnaire (88GP), a validated tool to assess habitual dietary intakes and a 24-hour dietary recall. 25
Serum measurements
All blood samples were drawn between 7:30 and 11:30 am. Serum 25(OH)D serum levels were measured using a125I radioimmunoassay (RIA) kit (Diasorin, Stillwater, MN, Intra-assay CV = 10.8%). Intact-PTH (iPTH) was measured using an iPTH (1–84) Enzyme-Linked Immunosorbent Assay (ELISA) (ALPCO Diagnositics, Salem, NH, Intra-assay CV = 2.5%). Serum estradiol and cortisol were also measured using commercially-available ELISA kits (ALPCO Diagnostics, Salem, NH; Intra-assay CV = 7.7% and 5.8% respectively).
Three serum markers of bone turnover were measured using commercially-available ELISA kits: bone-specific alkaline phosphatase (BAP) and osteocalcin (OC) (Quidel, San Diego, CA; Intra-assay CV = 5%–8% and 5%–10%, respectively); and degradation products of C-terminal telopeptides of Type l collagen (CTx-I) (Serum CrossLaps®, IDS, Fountain Hills, AZ; intra-assay CV= 1.8%-3%). An ELISA was also used to measure serum leptin (ALPCO Diagnostics, Salem, NH; Intra-assay CV = 5.5%).
Statistical analysis
Unpaired, two-tailed Students' t-tests were used to determine differences in subject characteristics and bone and serum measurements between tanning and non-tanning groups. For data not normally distributed or of unequal variance, a rank-sum test was performed. Multiple linear regression analysis was used to determine the relationships between serum 25(OH)D and serum measurements adjusting for age and menopausal status. The sample size was chosen to detect a difference of 50% in 25(OH)D concentrations and of >30% in serum bone markers. All statistics were performed using SigmaStat for Windows version 3.01a (Systat Software, Inc., San Jose, California). A p-value less than 0.05 was considered significant.
Results
Forty-nine of the women were classified as Non-Tanners and 20 women were classified as Tanners. There were no significant differences in age, BMI, serum estradiol or cortisol concentrations, or hormonal contraceptive use between groups (Table 1). The Fitzpatrick skin type score of the Tanners was significantly higher than that of the Non-Tanners. The mean serum 25(OH)D concentration of the Tanners was significantly greater than the Non-Tanners. Conversely, the mean serum iPTH concentration of the Tanners was significantly less than the Non-Tanners.
Subject characteristics and vitamin D status. Data are expressed as means ± SEM.
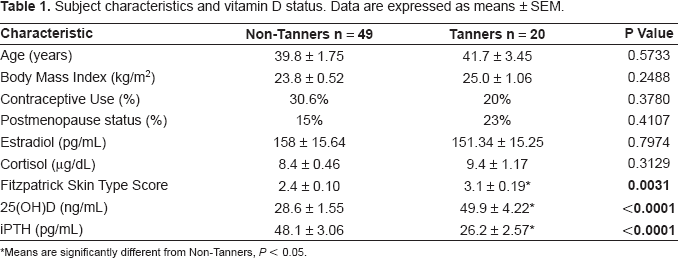
Means are significantly different from Non-Tanners, P < 0.05.
There were no differences between groups for selected bone-related nutrient intakes, including total energy, protein, fat, calcium, phosphorus, magnesium, and vitamin D. There were also no differences between groups for intakes of alcohol or caffeine which are agents known to affect bone.
Using the vitamin D status classifications proposed by Grant and Holick, 26 26.5% of Non-Tanners had deficient levels of serum 25(OH)D, 35.7% were insufficient, and only 38.8% had sufficient serum concentrations (Fig. 1). Of the Tanners, no one was classified as deficient, 15% had insufficient levels, and 85% had sufficient serum 25(OH)D concentrations.
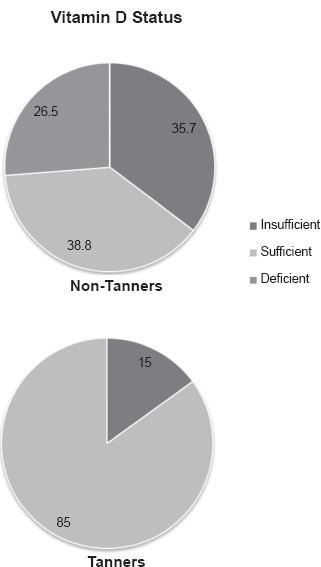
Distribution of vitamin D status as measured by serum 25(OH)D vitamin D concentrations, in tanning and non-tanning women. Categories: deficient (<20 ng/ml), insufficient (20–32 ng/ml), or sufficient (32–100 ng/ml) as suggested by Grant and Holick. 26
Serum bone marker data are shown in Table 2. Only serum osteocalcin concentration was significantly less in the Tanners compared with the Non-Tanners. There were no differences between groups for any of the other serum bone markers. Table 3 shows the results of the multiple linear regression analysis of the serum bone markers adjusting for age and menopausal status. There was a significant inverse relationship between serum 25(OH)D and iPTH concentrations. There was also a significant inverse relationship between serum 25(OH)D concentrations and serum osteocalcin concentrations and a significant positive relationship between serum iPTH and serum osteocalcin.
Serum bone marker concentrations in Non-Tanning and Tanning women. Data are expressed as means ± SEM.
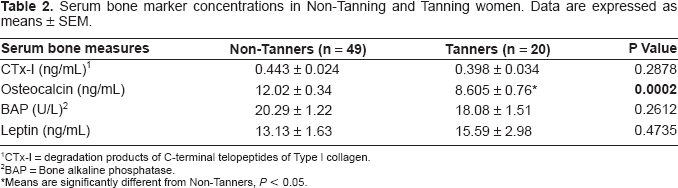
CTx-I = degradation products of C-terminal telopeptides of Type l collagen.
BAP = Bone alkaline phosphatase.
Means are significantly different from Non-Tanners, P < 0.05.
The relationship between serum 25(OH)D and serum iPTH concentrations and serum bone biomarkers in Non-Tanning and Tanning women adjusted for age and menopausal status.
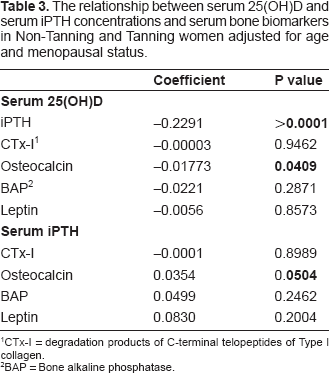
CTx-I = degradation products of C-terminal telopeptides of Type l collagen.
BAP = Bone alkaline phosphatase.
Discussion
The distribution of serum 25(OH)D concentrations we observed in our subjects is in agreement with the overwhelming number of reports documenting the prevalence of vitamin D deficiency and insufficiency in healthy populations.27–29 Moreover, in the only other study to examine the 25(OH)D concentrations of regular users of tanning beds, Tangpricha et al. noted in their subjects a similar distribution across vitamin D status classifications. 17
Undoubtedly, vitamin D plays an important role in achieving and maintaining a healthy skeleton through its function in ensuring an adequate supply of calcium to actively mineralizing bone. A deficit of vitamin D would be expected to impair calcium absorption efficiency and a lead to a rise in PTH production. 30 Our data showing a significant inverse association between serum concentrations of 25(OH)D and PTH is a reflection of this and is in accordance with numerous other reports on the relationship between vitamin D status, calcium absorption and circulating PTH concentrations.11,30–34
What's less understood, however, is the role that vitamin D plays in directly affecting bone remodeling and turnover. The measurement of serum biochemical markers can be employed to explore this function noninvasively in humans. 35 In our study, we assessed three bone markers: BAP and OC, markers of bone formation; and CTx, a marker of bone resorption. In addition we measured serum leptin, a hormone produced by adipocytes, shown to play an important role in bone metabolism, 36 including stimulating bone formation through its action on osteoblasts. 37 Although there were not significant differences in all of bone markers measured between groups, results from our study of healthy women ages 25–82 years of age, show that those with regular UVB exposure via tanning beds have significantly lower serum osteocalcin concentrations than those without and that there is a significant inverse relationship between serum osteocalcin and serum 25(OH)D. Furthermore, this relationship appears to be PTH-dependent.
In the published literature, data on the association between vitamin D status and serum osteocalcin concentrations is inconsistent. For example, studies of postmenopausal women without estrogen replacement therapy, show either no significant relationship10,31 or a significant inverse relationship between serum 25(OH)D and osteocalcin 13 while investigations including subjects of premenopausal status have reported both a significant weak positive31,38 and significant weak negative relationship. 39
Osteocalcin is a noncollageneous bone-specific protein produced by osteoblasts and incorported into the bone matix. 35 In vitro studies of human osteoblast cultures show 1,25(OH)2D to be a strong inducer of osteocalcin production, but it has also been described that the 1,25(OH)2D-induced stimulation of osteocalcin decreases toward the mineralization stage because of concurrent accumulation of osteocalcin in the bone matrix. 5 This timing of mineralization phenomenon observed in cell culture research, may in part explain the disparate results on vitamin D status and circulating osteocalcin concentrations. The process of bone remodeling and turnover during adulthood is continuous and is characterized by two distinct phases: bone resorption which results in the disintegration and release of bone mineral and bone matrix fragments; and bone formation which follows resorption and involves the construction of matrix followed by its mineralization. Our findings on PTH and bone marker concentrations indicate that at the time of sample collection, the bones of those with low serum 25(OH)D concentrations (<30ng/ml or so) were undergoing greater active bone formation than those with higher vitamin D status, mostly likely related to an overall increase in total bone turnover to maintain calcium homeostasis. 40
Another confounder in the interpretation of results reported in the literature is the varying ranges of vitamin D status studied, as well as the definition of hypovitaminosis D used. For example, Sahota et al. in comparing serum bone markers between two levels of vitamin D status used a serum 25(OH)D cut-off for vitamin D deficiency that is markedly lower than those published more recently; 13 most of the subjects categorized as “sufficient” would be categorized as “insufficient” in later studies. 26 In the report of Gannage-Yared et al. all of the subjects studied would be classified as “insufficient”. 38 In contrast, the subjects studied in the work described herein spanned the range of current vitamin D status classifications, from “deficient”, “insufficient” and “sufficient”. 26
The purpose of this study was to further explore the relationship between vitamin D status and serum markers of bone turnover in healthy women. To do so, we exploited the known superior vitamin D status of individuals who are regularly exposed to UVB radiation through the use of commercial tanning beds compared with controls. 17 Other than tanning bed use, there were no significant differences in dietary intakes or other lifestyle factors (i.e. smoking, alcohol or caffeine consumption, physical activity, medications) known to affect bone or vitamin D status between the tanning and non-tanning groups. So while it has been reported that women who tan regularly also engage in more high risk behaviors than non-tanners, 41 the present study was designed to control or account for these behaviors through well-defined subject inclusion/exclusion criteria and the collection of pertinent questionnaire data for analysis. We are reasonably confident, therefore that our results may be extended to the general population of healthy women older than 25 years.
Vitamin D insufficiency is a serious problem worldwide. 29 Its prevalence is attributed to few natural dietary sources compounded by a lack of sunlight exposure. Our findings, along with those of the only other published report examining the effects of chronic exposure to artificial UVB radiation on vitamin D status and bone health 17 indicate that regular tanning bed use results in higher 25(OH)D concentrations and more favorable bone measures including bone density and now, bone marker profiles. However, making recommendations to use tanning as a means to improve vitamin D status would not be prudent due to concerns about skin cancer42–45 nor should the results of this study be used to support or defend tanning. Rather, the results presented here should be used to further our understanding of the direct effects of vitamin D status, across a spectrum, on bone turnover.
Disclosure
The authors report no conflicts of interest.
Footnotes
Acknowledgments
This work was supported by the Department of Nutritional Sciences and the Food for the 21st Century program, University to Missouri; and the College of Human Environmental Sciences Maxine Seabaugh Schade Graduate Fellowship. The authors would like to thank Dr. Laura Hillman for her assistance with the vitamin D assays as well as the technical support of Mr. Ding Lee.