
Abstract
Background:
Despite the well-documented benefits of physical activity, particularly strength training, for managing menopause-related physiological changes such as muscle loss and weight gain, few interventions specifically target pre- and perimenopausal women using scalable, remote delivery methods.
Objectives:
The purpose of this pilot study was to examine the feasibility and preliminary efficacy of a group-based physical activity and strength intervention delivered via Zoom for pre- and perimenopausal women.
Design:
This study was a randomized controlled trial lasting 12 weeks.
Methods:
Low active pre- and perimenopausal women between the ages of 40–50 (n = 39) were randomly assigned to a 12-week physical activity strength intervention or a waitlist control. Participants attended the sessions twice per week, which included both a 40-min cardiovascular and strength training component and a 20-min motivational component informed by Self-Determination Theory and Habit Formation Theory. Participants were provided Apple Watch devices to monitor their physical activity.
Results:
The physical activity strength intervention appears feasible based on recruitment duration, adherence to the Zoom sessions, retention, and the consumer satisfaction survey. The intervention participants increased their physical activity by 21 min/week, and the control group decreased by 2 min, although the differences were not significant. The intervention participants reported greater positive changes on several of the psychosocial variables, including self-efficacy, habit formation, habit automaticity, self-regulation, goal setting, physical activity enjoyment, physical activity feeling, physical activity revitalization, and physical activity tranquility.
Conclusions:
Although there was no evidence that the intervention led to increases in physical activity, this study supports the feasibility of a group-based physical activity strength intervention delivered via Zoom. Additional studies that include larger sample sizes and a longer intervention are needed to better understand the efficacy of the intervention.
Plain language summary
The majority of physical activity intervention studies do not adequately integrate strength training. This is particularly problematic for women approaching menopause given menopause is often related to weight gain and loss of muscle.
Objectives:
The purpose of this pilot study was to examine the feasibility and preliminary efficacy of a group-based physical activity and strength intervention delivered via Zoom for premenopausal women.
Design:
This study was a single blind randomized controlled trial lasting 12 weeks.
Methods:
Low active premenopausal women between the ages of 40–50 (n = 39) were randomly assigned to a 12-week physical activity strength intervention or a waitlist control. The sessions included a 40 min cardiovascular and strength training component and a 20 min motivational component informed by Self-Determination Theory and Habit Formation Theory. Participants were provided Apple Watch devices to monitor their physical activity.
Results:
The physical activity strength intervention appears feasible based on recruitment duration, adherence to the Zoom sessions, retention, and the consumer satisfaction survey. There were no differences between the groups on physical activity, however, intervention participants reported greater positive changes on several of the psychosocial variables including self-efficacy, habit formation, habit automaticity, self-regulation, goal setting, physical activity enjoyment, physical activity feeling, physical activity revitalization, and physical activity tranquility.
Conclusions:
This study supports the feasibility of a group-based physical activity strength intervention delivered via Zoom. Additional studies that include larger sample sizes and a longer intervention are needed to better understand the efficacy of the intervention.
Introduction
Obesity is related to numerous health problems among women, including cardiovascular disease, type 2 diabetes, hypertension, arthritis, and depression.1,2 Rapid weight gain is particularly common during menopause (defined as 1 year after cessation of the menstrual cycle). 3 At the start of menopause, the rate of fat gain doubles, and lean mass declines. These gains and losses continue for 2 years after the final menstrual period. 3 Interventions are needed to prevent this weight gain that often occurs during and after menopause.
Regular physical activity (PA) is related to less weight gain during menopause. 4 However, many women still gain weight during menopause despite meeting the PA guideline of engaging in PA for 150 min/week. 5 Most women do not integrate strength training into their PA routine, which is problematic given that strength training results in reduced body mass, body fat, and increased fat-free and muscle mass among women.6 –8 Therefore, the lack of strength training may contribute to the weight gain associated with menopause.
Studies examining behavioral interventions for weight management during menopause have yielded small changes in weight. 9 However, many of these studies have not adequately addressed PA adherence, and virtually none have specifically addressed strength training. 7 Several studies have demonstrated that PA sessions that integrate strength training can be successful among women in highly supervised, lab-based settings with sophisticated equipment.6,7,10,11 In addition, a recent review indicated that lab-based circuit training alone led to weight loss among middle and older-aged women. 12 Some limitations of these studies are that they are expensive, the potential for real-world dissemination is low given that they tend to be lab-based, and long-term adherence to the PA program is unclear. Another limitation is that the studies tended to be with clinical populations, young women, and/or older women. With the exception of one small lab-based study, 13 none of the studies examined middle-aged women. This is a disservice to middle-aged women, which is when weight gain occurs most frequently. 3
The purpose of this study was to examine the feasibility and preliminary efficacy of a 12-week home-based PA intervention that included strength training among pre- and perimenopausal women ages 40–50. This study addressed several gaps in the literature by emphasizing strength training, delivering the intervention remotely, focusing on middle-aged women, and including behavioral strategies designed to increase adherence. The intervention was informed by Self-Determination Theory (SDT) and Habit Formation Theory.14,15 As suggested by Bowen et al., 16 feasibility studies should evaluate both acceptability and implementation, and limited efficacy testing should be conducted. We hypothesized that intervention participants would report more PA minutes per week than the waitlist control. We also hypothesized that participants randomized to the intervention group would report greater increases in psychosocial variables related to PA, including self-efficacy, habit formation, self-regulation, enjoyment, and exercise-induced feelings. Finally, an exploratory aim examined the relationship between group cohesion and attendance at the PA strength sessions.
Methods
Overview of study
This trial was a randomized controlled pilot study conducted from December 2022 to December 2023. Specifically, pre- and perimenopausal women (n = 39) were randomized 1:1 to either a 12-week group-based PA intervention focusing on strength training or a waitlist control group. Acceptability of the intervention and implementation were examined. Regarding preliminary efficacy, the primary dependent variable was PA minutes per week at 12 weeks. Secondary dependent variables included PA self-efficacy, habit formation, self-regulation, PA enjoyment, and PA feelings. The waitlist control group was given the option of receiving an individualized PA intervention program following the 12 weeks. The CONSORT Guidelines were followed. 17 This study was approved by the Institutional Review Board at the University of Minnesota (Code: #00016282) on July 22, 2022. Participants completed an online consent form prior to participating in the study. All participants provided written informed consent prior to enrollment in the study. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Participants
Pre- and perimenopausal, low-active women between the ages of 40 and 50 were recruited via worksite emails, social media, studyfinder, clinicaltrials.gov, and a previous study in the northern region of the United States. Eligibility was assessed via a telephone screening interview. Specific inclusion criteria included the following: (1) Engaging in <90 min of moderate to vigorous intensity PA per week (to ensure participants could benefit from the intervention); (2) adequate space at home to complete exercise sessions (to ensure consistent participation); (3) capacity to use Zoom via a mobile device or computer; (4) pre- or perimenopausal which was defined as being between the ages of 40–50 and having had at least one menstrual period during the last 12 months (the menstrual period criteria was included to ensure that pre- and perimenopausal women were included); (5) ability to read and write fluently in English; (6) access to an iPhone; (7) not been hospitalized for a psychiatric condition in the past 6 months; and (8) willing to be randomly assigned to either study condition. Exclusion criteria included the following: (1) Two people living together in the same household (to ensure there were not any contamination effects if both received different interventions—one of the two could participate); (2) pregnancy; (3) type 1 diabetes; and (4) history of heart disease, exercise-induced asthma, or another health condition that may be exacerbated by exercise. The remaining exclusion criteria were included because these medical conditions could interfere with PA.
Measures
Feasibility was assessed and is described in more detail below. Questionnaires were administered at baseline and 12 weeks except the demographics survey (baseline only), Consumer Satisfaction Questionnaire (post-test only), and Physical Activity Group Environment Questionnaire (PAGEQ; post-test only). 18 Each measure and the procedures for Apple Watch are described in more detail below.
Feasibility
Feasibility was assessed by evaluating both acceptability and implementation. 16 Acceptability was assessed based on attendance at the PA strength sessions administered twice per week over Zoom and the Consumer Satisfaction Scale (items were on a seven-point Likert scale). Acceptability was considered achieved if participants attended two-thirds or more of the intervention sessions on average and rated the intervention a five or higher on the consumer satisfaction scale (based on a seven-point Likert scale; five was chosen, given that indicates a 70% satisfaction rating). Implementation was based on recruitment (i.e., number of participants recruited each month) and retention rates. Also, as recommended by Eldridge et al., 19 we examined the number of eligible participants and percent of participants randomized among those who were eligible. Implementation was considered achieved if at least 10 participants/month were recruited during the recruitment phase and 90% of the sample was retained at 12 weeks. Ten participants per month were chosen because this would allow for a future trial to recruit 200 participants in <2 years.
Apple Watch
Apple Watch Series 8 was used to objectively measure PA and move calories. Participants reported exercise minutes and move calories for 7 days at baseline prior to randomization and at 12 weeks based on information they obtained from their Apple Watch. Move calories are based on active calories, which are calories burned via activity throughout the day (i.e., can include light activities). Move calories include any calories burned that are not burned via one’s basal metabolic rate, which refers to energy the body uses to function when at rest.
Research staff connected with participants via a scheduled telephone call. Participants utilized Apple’s Fitness app on their iPhone to report the information indicated above. Participants took a screenshot of each day (7 days at baseline and 7 days at 12 weeks) and emailed the information to the secure university study email address. Apple Watch is valid and reliable for measuring PA.20 –24 Participants who were not familiar with Apple Watch were provided information regarding how to wear it, check their activity minutes, and how to launch a workout session.
Physical activity self-efficacy
Self-efficacy associated with PA was measured using the 5-item Self-Efficacy for Physical Activity Questionnaire. 25 Participants were asked to assess their confidence in participating in PA in the presence of barriers such as feeling tired, being in a bad mood, not having time, vacation, and bad weather. This measure is based on a 5-point Likert scale ranging from not confident to extremely confident. The scale has acceptable reliability and validity.25,26
Habit Index
The Self-Report Habit Index (SRHI) 27 was used to measure habit strength related to PA. The SRHI consists of 12 items and is designed to assess characteristics of habitual behavior including automaticity, frequency of engagement in the behavior, and the link between behavior and self-identity. Participants were asked to rate the degree to which they agree with statements related to habitual exercise behavior on a scale from 1 (strongly disagree) to 7 (strongly agree), with higher scores indicating higher strength of habit. The SRHI has acceptable internal and test–retest reliability, and validity.27 –30
Self-regulation
Self-regulation was measured using the 31-item Short Form Self-Regulation Questionnaire (SSRQ). 31 Participants used a five-point Likert scale (1 = strongly disagree to 5 = strongly agree) to rate the degree to which they agreed with statements related to general self-regulation to achieve goals. Participants received a total score based on all of their responses as well as two subscale scores for impulse control and goal setting. The SSRQ has demonstrated good psychometric properties, including a Cronbach’s alpha of 0.92, and high correlations with the original SRQ and other measures of validity and reliability.31 –33
Physical activity enjoyment
The 18-item Physical Activity Enjoyment Scale (PACES) 34 was used to assess enjoyment for PA. Participants answered questions like “how you feel at the moment about the PA you have been doing” using a seven-point Likert scale. An overall enjoyment for PA score was determined by summing the items with higher scores reflecting higher enjoyment. Research indicates that the PACES is reliable and valid in diverse populations.34 –36
Physical activity feelings
Exercise-induced feeling was assessed using the 12-item Exercise-Induced Feelings Inventory. 37 Participants assessed their feeling states during acute bouts of PA on a scale from 0 (do not feel) to 4 (feel very strongly). Four feeling states were assessed, including revitalization, positive enjoyment, physical exhaustion, and tranquility. The subscales have demonstrated excellent internal consistencies and sensitivity to change in PA interventions. 37
The PAGEQ
Group cohesion among the intervention participants was examined using the 21-item PAGEQ. 18 This questionnaire uses a nine-point Likert scale ranging from strongly disagree to strongly agree. The four subscales for this measure include the following: (1) Individual Attraction to Group-Task (ATG-T); (2) Group Integration-Task (GI-T); (3) Individual ATG-Social (ATG-S); and (4) GI-Social (GI-S). The “individual” subscales refer to the motives related to the individual staying in the group, and cohesion is the unification of the group. The subscales also differentiate between the task (in this case PA) and social connections with each other. This questionnaire has been shown to have good reliability and concurrent validity. 18
Consumer Satisfaction Questionnaire
The Consumer Satisfaction Questionnaire is a seven-item questionnaire that assessed how satisfied the participants were with the PA strength intervention and the individual components of the interventions including the website, individual exercise session options, motivational messages sent via email, Apple Watch, and the Zoom sessions (the PA strength and motivational components of the Zoom sessions were rated separately). Participants were asked to rate their satisfaction on a seven-point Likert scale ranging from 1 = very dissatisfied to 7 = very satisfied (higher scores indicate higher satisfaction).
Procedure
Potential participants texted, emailed, or called a study line in response to our advertisements and emails. Potential participants completed a telephone screening interview to determine eligibility, which was adapted from the 10-item Physical Activity Readiness Questionnaire. 38 PA was self-reported during the telephone screening interview to determine eligibility. The Research Coordinator provided information regarding the study and reviewed the consent form. Interested and eligible participants were emailed the online consent form and baseline questionnaires. Once the online consent form and questionnaires were completed, participants were mailed exercise bands for resistance training and an Apple Watch, which was worn for 7 days prior to the intervention and throughout the intervention. Next, the randomization session was completed over the phone. Specifically, participants were randomized 1:1 to either the 12-week PA strength intervention or waitlist control condition. The random numbers scheme was randomly generated by the PI, and one of the research coordinators conducted the randomization sessions. Participants were randomized in cohorts of ~20 (10 participants in each condition). Participants were given $100 for completing the 12-week assessment session and were allowed to keep their Apple Watch.
PA intervention
The PA intervention consisted of group-based Zoom sessions, motivational email messages, and a website. Participants completed two group-based Zoom PA sessions per week (40-min exercise session and 20 min of motivational counseling) for 12 weeks. The exercise component included various aerobics (e.g., high knees, jogging/walking in place) and muscle strengthening exercises (e.g., lunges, body weight squats, burpees, push-ups). Participants modified the exercise depending on their ability (e.g., wall push-ups versus knee push-ups versus regular push-ups). Exercise bands were also used for resistance training. Participants were instructed to engage in two PA sessions per week outside of the group, which included a variety of options (walking/jogging outside, online exercise videos, prescribed exercise sessions listed on the website, or any other exercise). The intervention was led by a master’s level health coach who is a personal trainer and holds an American College of Sports Medicine Certified Exercise Physiologist® credential.
SDT and Habit Formation Theory guided the content of the counseling portion of the Zoom sessions14,15 as outlined in Table 1. According to SDT, there are five types of motivation, which range from external regulation (e.g., engage in PA for appearance reasons) to intrinsic regulation (e.g., engage in PA because it aligns with one’s values or goals). The goal of the intervention was to achieve intrinsic regulation. Therefore, the health coach emphasized positive affective responses to exercise sessions and strategized to make PA, a part of the participants’ self-identity. The ultimate goal was to experience high intrinsic motivation for PA (i.e., individuals engage in exercise due to inherent pleasure) since it is related to higher levels of PA. 39 Relatedness, another construct related to SDT, was addressed via the mutual support and social interactions in the group-based sessions. Habit formation was also emphasized in the intervention. 14 The health coach worked with the participants to create exercise habits (e.g., schedule an exercise session like an appointment, exercise at the same time each day). Habit formation theory postulates that long-term adherence to PA is related to PA becoming an automated habit. Group cohesion was enhanced by emphasizing empathy, active listening, and supportive feedback. The participants were encouraged to share personal stories about their journey with PA.
Summary of intervention components targeting psychosocial variables.

Motivational website
Participants received access to a mobile phone-friendly study website that included motivational messages, an online log to track completion of home-based sessions, and options for individual-based exercise sessions (e.g., full-length YouTube exercise videos, written out workouts to follow).
Motivational emailed messages
Participants received one motivational email message each week to remind them to complete the exercise sessions. The messages included strategies based on SDT and were tailored to life circumstances (e.g., strategies for adhering to exercise despite a demanding job) as well as the corresponding week’s behavioral session topic.
Waitlist control condition
Participants in the waitlist control condition received an Apple Watch and completed the same assessment sessions as the PA intervention. However, PA information was not provided until after 12 weeks. Participants were given the option of receiving an individualized version of the PA intervention once they completed the 12-week assessment.
Statistical analysis
Descriptive statistics were utilized to summarize the baseline variables. Unadjusted means were reported at baseline and 12 weeks for the primary and secondary dependent variables. Between-group analysis of covariance (ANCOVA) tests were used to examine the effect of the intervention on PA and the psychosocial variables, controlling for baseline. Bivariate correlations were used to examine the relationship between group cohesion and attendance at the PA strength sessions. The alpha level was set at 0.05, and adjustments were not made, given all comparisons were planned. The management and collection of the data was handled via REDCap, and the data analysis was run in SPSS 28.0 (IBM Corporation).
Results
Demographic data are summarized in Table 2. Participants were 44 years of age on average (range was 40–50), most were married (72%), college educated (69%), and all were employed. Thirty-one percent were from racially and/or ethnically diverse backgrounds.
Baseline characteristics by study arms.
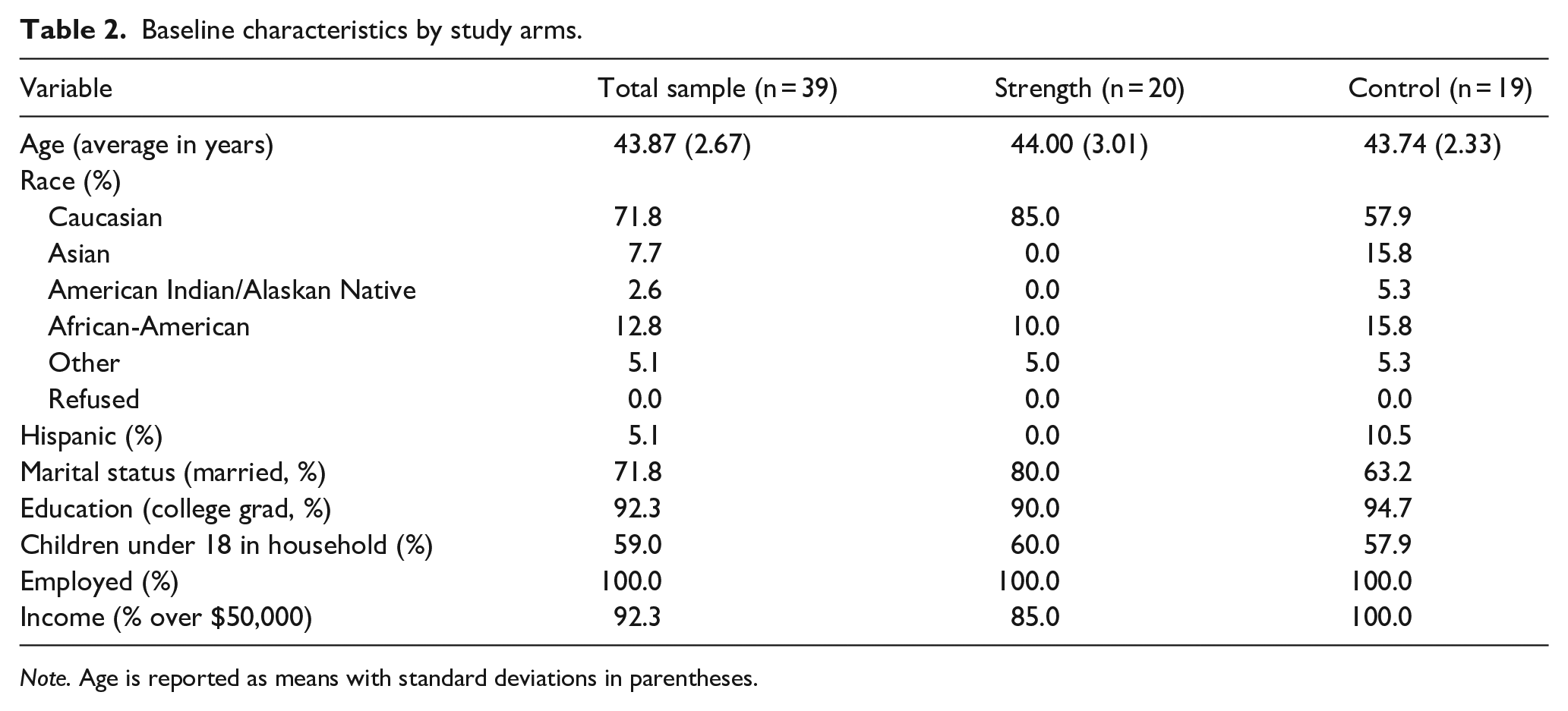
Note. Age is reported as means with standard deviations in parentheses.
Feasibility
Recruitment and retention are summarized in Figure 1. Sixty-six participants completed the telephone screening interview, and of these, 42 were eligible. Thirty-nine participants (93% of the eligible participants) were randomized to one of the two study arms. The first cohort was recruited in 1 month (December 14, 2022–January 13, 2023), and the second cohort over 2 months (June 27, 2023–August 30, 2023). All of the intervention participants and 95% of the control participants were retained at 12 weeks (defined as completing the post-test questionnaires). On average, participants completed 17 of the 24 intervention sessions. The overall rating on the consumer satisfaction scale was 5.34 (SD = 1.58) on a scale of 1–7 (see Table 3), which met the acceptability criteria of five or higher. The highest consumer satisfaction rating was for Apple Watch, and the lowest was for the motivational messages via email.

Flow chart.
Consumer satisfaction survey.

Note. SD are in parentheses. Participants were asked to rate their satisfaction regarding the above components of the intervention on a seven-point Likert scale ranging from very dissatisfied to very satisfied (higher scores indicate higher satisfaction).
SD: standard deviation.
Physical activity
PA minutes per week by study arm are summarized in Table 4. There were no differences between groups for “move” calories or for PA minutes per week at 12 weeks.
The effect of the intervention on physical activity.

Note. Standard deviations are in parentheses. Results are based on ANCOVA analyses.
Psychosocial variables
The effects of the intervention on psychosocial variables are reported in Table 5.
The effect of the intervention on the psychosocial variables.

Note. Values are means (standard deviations in parentheses). Results based on ANCOVA.
EFI: Exercise-Induced Feeling Inventory.
Relative to the waitlist control and after adjusting for baseline values, participants in the PA intervention reported higher levels of self-efficacy, habit formation, habit automaticity, self-regulation, self-regulation goal setting, exercise enjoyment, exercise revitalization, and exercise tranquility. There were no differences between the intervention and waitlist participants on impulse control, positive engagement, or physical exhaustion.
Group cohesion
Means for the subscales of the PAGEQ, which were on a 9-point Likert scale, were 6.49 (SD = 2.23) for ATG-T, 5.77 (SD = 1.94) for GI-T, 4.99 (SD = 2.10) for ATG-S, and 4.38 (SD = 1.86) for GI-S. The means are reported as averages per item since the number of items per subscale varied. Results indicated that higher scores on the GI-T subscale were related to better attendance at the PA strength sessions, r = 0.482, p = 0.031.
Discussion
The group-based PA strength intervention delivered via Zoom appears feasible based on the acceptability and implementation parameters. Our retention rate was 97% at 12 weeks, which far exceeded our goal of 90%. In addition, we were within one participant of meeting our goal of recruiting 40 participants. We met our goal of recruiting 10 participants/month on average (20 participants were recruited over 1 month for cohort 1 and 19 were recruited over 2 months for cohort 2). We randomized 93% of the eligible participants, which supports feasibility as well as generalizability of the sample. We also exceeded our intervention adherence goal (participants attended on average at least two-thirds of the intervention sessions). This was a significant accomplishment, since meeting at a specified time twice per week may have been challenging for some participants with work and/or family obligations. The mean score on the consumer satisfaction questionnaire was 5.34, which exceeded our goal of five points on the seven-point Likert scale. Participants rated Apple Watch and Zoom strength training sessions the highest and the emailed motivational messages the lowest, which suggests that technological barriers did not interfere with participation. These findings also suggest that future studies may want to focus on texting and app-based messaging instead of emails.
Contrary to our hypotheses, participants randomized to the PA strength intervention did not have greater move calories per day or exercise minutes per week than participants in the waitlist control condition. Even though it was not statistically significant, possibly due to the small sample size, participants in the PA strength intervention engaged in 28 more min/week of PA than those in the waitlist condition at baseline (143 min/week for the PA strength intervention versus 115 min/week for the control). Therefore, the PA strength intervention participants had less room to improve than the control condition, which could have impacted the results. One of the inclusion criteria was engaging in <90 min/week of PA, and therefore, both groups had higher PA minutes than expected at baseline. Eligibility was assessed via self-report, and the baseline data were objectively measured using Apple Watch, which may have accounted for this discrepancy. It is possible that participants underreported their PA at the telephone screening interview. Also, wearing Apple Watch and emailing their activity screen shots may have motivated them to increase their PA from prior levels. Future trials should consider a lower PA criteria for eligibility and/or assess PA objectively to determine eligibility.
Although not significant, the move calories decreased in the intervention group relative to the control. It is possible to have a low number of move calories throughout the day with high PA minutes if the participant engaged in a low amount of light activities but engaged in moderate to vigorous intensity activity. It is possible that the increased PA minutes were related to less light activities during the rest of the day. Participants may have been physically tired from exercising or felt justified not to engage in light activities throughout the day, given they had exercised. Additional research is needed to better understand the effect of PA minutes on light activities.
This trial was not powered to examine the mediating effect of the psychosocial variables. However, we still examined the effect of the intervention on various psychosocial variables to inform future trials. Relative to the waitlist condition, participants in the PA strength intervention reported increases from baseline to 12 weeks for PA self-efficacy, habit formation, habit automaticity, self-regulation, self-regulation goal setting, PA enjoyment, revitalization related to PA, and tranquility as a result of engaging in PA. This is consistent with previous research suggesting that behavioral interventions lead to improvements in psychosocial variables targeted by the intervention. 40 The psychosocial findings indicate that the intervention successfully intervened on the intended variables. Since these variables are related to PA increases and maintenance, perhaps future studies that are adequately powered would result in significant increases in PA both during the intervention and in the long term.
To inform future trials regarding the importance of group dynamics, we evaluated group cohesion. Results indicated that participants who rated the intervention as high on group integration related to the shared goal of engaging in PA had higher attendance at the PA strength sessions than those reporting lower ratings. Consistent with previous studies, 41 this finding suggests that the group dynamics can have an impact on individuals consistently attending group-based PA interventions. This result has important implications for future research in that studies should emphasize group bonding and social connections between the group members very early in the intervention (e.g., team building, icebreaker activities, collaborative exercises, encouraging empathy).
Study strengths
There were strengths related to this study. First, the methodology was strong in that the trial included a systematic evaluation of feasibility, randomization occurred between the study arms, an experienced health coach with appropriate credentials conducted the group-based intervention sessions, and validated measures were utilized. Second, evaluating the feasibility and potential efficacy of a group-based Zoom PA intervention focusing on strength is novel and addresses a gap in the literature. The group-based remote format allowed for social support from the other participants while addressing barriers typical for an in-person intervention (e.g., transportation, childcare, high time commitment). Third, the use of Apple Watch to motivate and assess PA has not been extensively studied previously. Finally, targeting pre- and perimenopausal women ages 40–50 is particularly important given the rapid weight gain that can occur as women approach menopause. 3
Study limitations
Despite these strengths, there were several limitations. First, data obtained from Apple Watch were not provided directly from Apple Watch devices but rather were provided indirectly through screenshots taken by the participant. This created reliance on participants adhering to the study protocol. We did not have resources to build a study app to passively read data from HealthKit on iPhone, so we relied on data communication via screenshots. Second, the intervention was relatively short in duration (i.e., 12 weeks). Third, there may have been selection bias due to the eligibility criteria, especially related to the technology requirements for the study. Fourth, sample size calculations were not completed for this trial, given it was considered a pilot study and efficacy was not a primary aim of the study. Finally, 28% of the sample was racially or ethnically diverse, which is representative of the recruitment area. However, higher levels of diversity would have enhanced the generalizability of the study.
The focus on strength training has often been ignored in previous PA intervention trials. 10 Typically, the goal of PA interventions is to achieve 150 min of moderate to vigorous intensity activity per week. Meeting the strength training criteria is often not addressed and/or assessed. 42 This is a disservice to individuals hoping to obtain the health benefits of strength training and is particularly problematic for women entering menopause who often experience a significant loss of muscle and an increase in weight. 3 Walking is the most common type of PA, 43 but research indicates that walking is not associated with preventing weight gain. 44 Future intervention trials should target both cardiovascular and strength training (separately or combined). Researchers should keep in mind that cardiovascular and strength training can be combined into one workout (e.g., walking or jogging while taking periodic breaks to do push-ups and air squats). As more research focuses on strength training, it will also be important for researchers and policymakers to determine if the current guideline of strength training at least two times per week is adequate. Finally, given the high consumer satisfaction rating for Apple Watch devices, additional research is needed that examines whether Apple Watch devices can be used for both intervention and assessment purposes or whether other types of accelerometers in which data cannot be seen by the participant, such as the ActiGraph (Ametris), should be added for assessment purposes.
Conclusions
In summary, the group-based PA strength intervention delivered via Zoom appears to be feasible based on recruitment duration, adherence to the Zoom sessions, retention, and the consumer satisfaction survey. However, there was no evidence that the intervention led to increases in PA. Participants were least satisfied with the motivational email messages, suggesting that additional research is needed to determine if these are necessary, or if other delivery modes might be considered. Additional studies could also use artificial intelligence to create more personalized messages, which may improve satisfaction. The group-based sessions were rated highly on the consumer satisfaction survey, which suggests that future studies should continue to examine group-based interventions. Group dynamics are important, as evidenced by group cohesion being related to higher attendance at the PA strength sessions. In addition, even though significant differences for PA were not found between the intervention and control participants, significant increases in key variables addressed in the intervention, such as habit formation and self-efficacy, were observed.
Taken together, even though there were no differences between groups for PA, given the changes in the psychosocial measures and the high retention rates and satisfaction scores, an examination of the intervention in larger, longer randomized controlled trials is warranted. Given the high use of Apple Watch devices among the general population, it will be important for future studies to explore Apple Watch devices as both an intervention tool and assessment method. The use of Apple Watch devices can reduce the burden of adding an additional device to monitor PA in randomized trials. Finally, to address the challenges of menopause, 3 PA studies that include a strength component are particularly needed for this population.
Footnotes
Acknowledgements
We would like to thank Laura Polikowsky for her assistance with this project. We are also very grateful to the study participants who made this study possible.
Ethical considerations
This study was approved by the Institutional Review Board at the University of Minnesota (Code: #00016282) on July 22, 2022. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Consent to participate
Participants completed an online consent form prior to participating in the study. All participants provided written informed consent prior to enrollment in the study.
Consent for publication
Participants provided written consent to publish the findings of the study via the consent form.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported through a grant from the University of Minnesota Grant-in-Aid program. Apple Inc. provided Apple Watch devices for the research.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: There are no conflicts of interest among any of the authors. Apple, Inc. provided Apple Watch devices for the research. Apple was not involved in the design of the research, nor was it involved in the collection, analysis, or interpretation of the research data.
Data availability statement
The dataset is available upon request to the first author of the study.