
Abstract
Background:
Balochistan, Pakistan’s most economically and health system-deprived province, hosts a significant portion of the Afghan refugee population. The province’s already fragile healthcare infrastructure faces additional strain due to the refugees.
Objective:
This study aimed to investigate the barriers to antenatal and intrapartum care seeking among Afghan refugee women in Balochistan during the Coronavirus disease 2019 (COVID-19) pandemic.
Design:
This study employed a cross-sectional survey approach to assess antenatal and intrapartum care-seeking behavior among Afghan refugee women residing in Balochistan, Pakistan. The study focused on refugee women living in Kharotabad Union Council in Quetta city to understand their barriers to accessing maternal healthcare services.
Methods:
The survey focused on antenatal and childbirth care-seeking behaviors among married women of reproductive age (MWRA) with at least one child aged 12–23 months born during the first four waves of COVID-19 in Pakistan.
Results:
Of 480 MWRAs, only 36.9% sought antenatal care (ANC); only 13.1% received at least four ANC visits. Furthermore, only 38.8% of MWRA had skilled birth attendance. Only 32.9% of MWRAs received at least one ANC and had skilled birth attendance (i.e., comprehensive care). Accessing comprehensive care was associated with maternal age less than 25 years (adjusted odds ratio (OR): 0.40; 95% confidence interval (CI): 0.21, 0.78), Tajik ethnicity (adjusted OR: 0.40; 95% CI: 0.23, 0.70) and large family size (adjusted OR: 0.58; 95% CI: 0.37, 0.93). Predictors of poor access were concern related to documentation of the refugee women they faced (adjusted OR: 1.52; 95% CI: 1.00, 2.34), women with no one at household to accompany them at health facility (adjusted OR: 1.75; 95% CI: 1.13, 2.70), myths and misconceptions related to available care (adjusted OR: 1.89; 95% CI: 1.18, 3.02), and the transport availability (adjusted OR: 1.76; 95% CI: 1.12, 2.77). Concerns related to COVID-19 had no association.
Conclusion:
The study highlights the barriers to maternal, neonatal and child health service utilization among Afghan refugee women in Balochistan. Tailoring healthcare services to consider age, ethnicity, cultural dynamics, and system constraints is crucial for improving access.
Plain language summary
Balochistan is Pakistan’s most underserved province in terms of healthcare and economic resources, and it is home to a significant number of Afghan refugees. The already weak healthcare system in Balochistan faces further challenges due to the needs of the refugee population. This study explored Afghan refugee women’s challenges in seeking maternal, newborn, and child health (MNCH) care during the COVID-19 pandemic. The research focused on married Afghan refugee women living in Quetta city who had given birth during the first four waves of COVID-19 in Pakistan. Out of 480 women surveyed, only 37% received antenatal care (ANC) during pregnancy, and just 13% completed the recommended four ANC visits. Additionally, fewer than 39% of women had skilled professional assistance during childbirth, and only 33% accessed both ANC and skilled birth attendance, which is considered comprehensive care. The study found that younger women under 25 years old, women from the Tajik ethnic group, and those with larger families were less likely to access comprehensive care. Barriers included concerns about legal documentation, lack of someone to accompany the women to healthcare facilities, myths and misconceptions about healthcare services, and lack of transportation. Interestingly, concerns about COVID-19 did not appear to impact healthcare-seeking behaviors. These findings emphasize the need for healthcare services that address the specific barriers faced by Afghan refugee women in Balochistan. Providing culturally sensitive healthcare, ensuring better transportation options, and debunking myths about healthcare services could improve access to essential MNCH care. Addressing these issues is critical to ensuring the well-being of Afghan refugee mothers and their children.
Introduction
Pakistan is home to nearly 1.4 million Afghan immigrants, representing 34% of the total displaced population from Afghanistan.1,2 Considering that many Afghans are undocumented, it is likely that these numbers underestimate the phenomenon. 3 For the vulnerable Afghan refugee population, especially women and children, healthcare access is paramount. In their own country, around 90% of Afghan women, newborns and children under 5 do not have access to quality essential health services. 4 In 2020, Afghanistan had a maternal mortality rate of 638 per 100,000 births, 5 Along with neonatal and under-5 mortality of 34 and 55.7 per 1000 births. 6 Moreover, the data from Afghanistan showed that more than 85% of pregnant women in the country do not have optimal four or more antenatal care (ANC) visits as recommended by the World Health Organization, and skilled health providers attend less than 50% of births in Afghanistan. 7 With the baseline vulnerability of being refugees from Afghanistan with suboptimal maternal, neonatal, and child health (MNCH) indicators, the overall health status of these women and children under-5 in Pakistan is even more crucial.
Refugee health is a global issue; they face significant barriers worldwide in accessing healthcare due to legal, economic, and social challenges. 8 Studies on Syrian refugees showed that they experience substantial barriers to healthcare, including fear of deportation, high out-of-pocket costs, and limited service availability.9,10 During the Coronavirus disease 2019 (COVID-19) pandemic, these issues have been exacerbated. 8 In Bangladesh, Rohingya refugees faced dire healthcare conditions worsened by the pandemic, with limited access to essential MNCH services.11,12 In sub-Saharan Africa, during public health emergencies like the Ebola outbreak, there was a marked decline in MNCH services, highlighting how conflict and crisis exacerbate health vulnerabilities. 13 A study in Turkey demonstrated that inclusive policies and coordination between international organizations and local health systems can mitigate adverse impacts on refugee health. 14 The pandemic has underscored the need to integrate refugee health into national health systems to ensure universal health coverage (UHC).8,15,16
Pakistan, which is already lagging behind in achieving Sustainable Development Goals, improving refugee health is of a great deal both in policy and practice. 17 Balochistan is the most economically fragile and health system-deprived province in Pakistan, hosting nearly 0.32 million Afghan refugees, 18 and the provincial capital, Quetta, has the biggest refugee settlements. 19 The healthcare experiences of residents or host communities and the refugee population are greatly influenced by geographic location and economic conditions. 20 Compared to other regions, considerable gaps in the healthcare infrastructure of Balochistan are noted.3,20 Better facilities are found in urban areas like Quetta. In contrast, healthcare inaccessibility in the rural parts of the province is often reported, mainly due to vast distances, lack of infrastructure, and a shortage of medical professionals.21 –24 Consequently, the province relies on outreach programs for basic healthcare. 25 Furthermore, MNCH indicators in the province are also lagging, with a maternal mortality rate of 298 per 100,000 births recorded in 2019, 26 and neonatal and under-5 mortalities standing at 34 and 78 per 1,000 live births, respectively. 27 Furthermore, 44.6% of pregnant women do not seek care from any qualified health provider in the antenatal period, and 65.1% of women deliver at home. 27 The compounding effect of Balochistan’s infrastructural fragility and MNCH challenges, added to the humanitarian needs of the Afghan refugee population, make this a critical setting.28,29
For this reason, primary healthcare (PHC), vaccinations, and maternal care are provided in the host province to registered Afghan refugees through the United Nations High Commissioner for Refugees (UNHCR) and its partner organizations, though not always in coordination with local establishments for specialized care. 17 On the other hand, undocumented refugees often end up seeking care at private entities with high out-of-pocket expenditures.29,30 Moreover, concerns about potential deportation or legal implications are believed to hinder healthcare-seeking behavior. 31 Under these circumstances, UHC is a huge challenge in such a context.29,31 Moreover, the recent COVID-19 pandemic has brought unparalleled challenges to healthcare systems globally, especially at the PHC level.8,32 These challenges are marked by resource diversion and a decline in healthcare utilization, especially in low- and middle-income countries (LMICs). 33 Furthermore, it is known that recent pandemics and public health emergencies like Ebola have impacted access to MNCH care among populations affected by conflict, including refugee women.15,34 Pakistan is among the countries where the COVID-19 pandemic has left strains on the economy and health system, especially regarding the overall delivery of PHC services. 35
Despite the increasing evidence on the impacts of the COVID-19 pandemic on populations, the question remains whether this same impact holds for regions already deprived of optimal health infrastructure, such as Balochistan. The paucity of evidence from such areas stresses the significance of this research. This study aimed to understand the antenatal and intrapartum care-seeking tendencies of Afghan refugee women in Balochistan during the pandemic and to document the multifaceted influences that shape maternal healthcare-seeking behaviors. .
Material and methods
Study design
This study employed a cross-sectional survey approach to document the coverage indicators across the continuum of care related to MNCH and assess factors potentially associated with poor utilization of MNCH services. This study is part of a broader project in which comprehensive data on MNCH domains, such as ANC, childbirth, postnatal and childcare, childhood immunization, nutrition, family planning and finally, knowledge, attitudes, and practices related to COVID-19 were collected. Only the components of antenatal and childbirth care seeking are reported in this article.
Study setting
The study was conducted in one of the union councils (UCs) of Quetta city, Kharotabad-1, one of the Super High-Risk UCs in Pakistan for polio cases and positive environmental samples. The study was conducted in Kharotabad-1, a UC in Quetta city, Balochistan, Pakistan. This area hosts a large population of Afghan refugees, many of whom have been residing in Pakistan for decades without formal legal status. The total population of this UC is 67,782, 36 with an estimated 31,176 Afghan refugees, mainly Pashtuns, Tajiks, and Uzbeks (unpublished). However, data from the government suggest that Quetta has 12%–15% of refugees across the city. 37 Kharotabad-1 has three government health facilities and around seven private health providers, further exacerbating healthcare access challenges for refugee women. 36 This study specifically targeted Afghan refugee women who met the inclusion criteria to ensure the findings reflect their unique healthcare-seeking experiences and barriers.
The reporting of this study followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. 38
Sample size
The sample size was calculated based on the modeling done by Roberton et al. to present the impact of COVID-19 on the coverage of key MNCH service domains. 39 The authors’ main assumption is that, in addition to the disruptions in the health system, the government-led movement restrictions, forcing families and nonessential workers to stay home, may have contributed to the coverage reduction of different MNCH domains, like family planning, ANC, postnatal care, early child curative care, etc., by 39.3%–51.2%. 39 Based on these assumptions, the estimated sample size for this study was 384 married women of reproductive age (MWRA) with at least one child aged 12–23 months. Furthermore, adjusting for the 20% non-respondent rate, the final sample size for the survey was 480 MWRA.
Population, sampling technique, and eligibility
The local partner, Trust for Vaccine and Immunization (TVI), has longstanding experience in the target community by providing MNCH care in several remote areas of Pakistan. TVI has a line listing of households with MWRA and under-5 children. Leveraging on this, the female social scientists paired with female local community health workers to collect the data between December 1, 2022 and January 10, 2023. A list of random households was generated from the line listing. A line listing of MWRAs residing in the UC was used as the sampling frame, which already had information on women’s nationality. A simple random sampling method was then applied to select participants from this predefined list. Afghan MWRA were approached at their households and screened for eligibility using available line listings from the existing MNCH services in the community. MWRA aged 18–49 years with the status of Afghan refugees who were residents in the catchment area, with at least one child aged 12–23 months and who provided written consent to participate, were enrolled in the study. Eligibility criteria were specifically formulated to capture participants’ maternity experience during the different waves of the COVID-19 pandemic in Pakistan. 40 This study considered the first four COVID-19 waves, from April 3, 2020 to November 29, 2021, as the maternal recall period. 40
The eligibility criteria for this study included Afghan refugee households with at least one married woman of reproductive age (18–49 years). Within these households, women were eligible to participate if they had been pregnant during the period of April 2020 to November 2021 and had at least one child aged 12–23 months at the time of the survey, that is, MWRA, who were pregnant and delivered a baby during that period. Only women who provided written consent were included in the study. Households or individuals who did not meet these criteria were excluded from participation.
Data collection tools
A questionnaire was developed under the guiding principles of Levesque’s Conceptual framework to cover the themes and dimensions of access to services, such as the approachability, acceptability, availability, accommodation, affordability, and appropriateness of MNCH-related PHC services. 41 The tool also considered the socioeconomic determinants corresponding to the abilities to perceive, seek, reach, pay, and engage to access basic PHC care, including challenges during COVID-19 and hurdles due to refugee status. Furthermore, satisfaction with the available services was assessed using a Likert scale.42 –44 Although the questionnaire was adopted from different published literature,41 –44 pilot testing was done on around 10% (n = 48) of the total sample among refugee women in a different Afghan settlement in Karachi, Pakistan. The purpose was to assess the clarity, cultural appropriateness, and feasibility of the questionnaire. The findings indicated that certain questions required refinement to improve comprehension and response accuracy. Based on the feedback, minor modifications were made, including simplifying complex wording, refining response options, and ensuring alignment with local dialects and cultural norms. No significant structural changes were needed, and the finalized questionnaire was used for the main study. The questionnaire was designed on the Kobo Toolbox, and each research staff member had a unique user ID and password to access the data collection application. Research staff interviewed the MWRAs and collected their responses on the application. The data were only accessible to the PI and senior research staff for quality assurance and analysis. The study questionnaire is provided in Supplemental Material Annexure 1.
Potential biases and mitigation
There are several potential biases and strategies to mitigate their impact. First, a simple random sampling method was applied to select participants from this listing, ensuring that all eligible women had an equal chance of selection. This approach inherently captured demographic diversity within the population, as random sampling minimizes selection bias and allows for natural representation across different ethnic groups, household sizes, and socioeconomic backgrounds. Second, there was a risk of response bias, where participants might provide socially desirable responses. To mitigate this, several strategies were employed. Female interviewers from the Afghan community were engaged to conduct the survey, helping participants feel comfortable discussing maternal health concerns. The questionnaire was carefully designed with neutral language to avoid leading responses. Interviews were conducted in private settings within participants’ homes to ensure that responses were not influenced by family members. Participants were explicitly informed that their responses would remain anonymous and would not affect their access to healthcare services, encouraging honest reporting. The study instrument was pilot-tested, and interviews were conducted in a culturally sensitive manner to foster openness and authenticity in responses. Furthermore, standardized protocols and training of data collectors helped mitigate the risk of inconsistencies in the data.
Data analysis
Data analysis was conducted using Stata version 18 (StataCorp, College Station, (TX) (StataCorp, 2023). Descriptive analyses were performed for basic demographic covariates, presented as frequencies and percentages. Four outcomes were assessed and presented sequentially in this article: (1) “optimal ANC care,” defined as at least four ANC received during pregnancy at any formal health provider, which could be at an either public or private hospital or PHC 27 ; (2) “skilled birth attendance or skilled facility,” defined as childbirth at formal health provider or with a skilled birth attendant which could be an either public or private hospital or PHC or home 27 ; (3) “comprehensive care,” defined based on whether women received at least one ANC visits plus had a skilled birth attendance; and (4) “satisfaction with comprehensive care” during the antenatal and childbirth periods. Satisfaction data were collected on a Likert scale as: “very satisfied,” “satisfied,” “neutral,” “dissatisfied,” and “very dissatisfied.” However, for the final analysis, the responses under very satisfied plus satisfied were re-coded as “satisfied,” unsatisfied plus very unsatisfied as “unsatisfied,” and neutral remained the same. The internal consistency (α) of the ANC satisfaction scale was 0.67, while the intrapartum satisfaction scale has reliability 0.78. When combined, the items for composite satisfaction scale showed internal consistency of 0.82.
Furthermore, the factors “COVID-19-related concerns/hurdles” was compositely created by merging several other variables: fear of getting the COVID-19 vaccine, fear of being exposed to the COVID-19 screening test, mask-related restriction at facility for the patients who are visiting, fear of being exposed to the COVID-19 infection, infected with COVID-19 recently, lack of ability to pay since COVID-19, services fees’ increase since COVID-19 and closure or rejection of services since COVID-19. The definition of different variables is provided in Supplemental Material Annexure 2.
Before model estimation, assumptions for binary logistic regression were evaluated. Multicollinearity was assessed using variance inflation factors (VIFs), and no variables exhibited high multicollinearity, as all VIF values were below the standard cutoff of 10. Influential observations and outliers were examined using Cook’s distance and leverage values, and no highly influential points were detected. Model fit was assessed using the Hosmer–Lemeshow goodness-of-fit test, ensuring model adequacy. For the main statistical analysis, unadjusted/crude odds ratios (ORs) of poor care seeking across different MNCH domains with 95% confidence intervals (CIs) were calculated in the univariable analysis. Variables with a p-value less than 0.25 in the univariable analysis were entered into the stepwise multivariable logistic regression analysis, and adjusted ORs for poor care seeking across different MNCH domains were calculated. Furthermore, ordinal logistic regression was used to understand the association of factors with different satisfaction levels. Adjusted ORs with p-values less than 0.05 were considered significant for reporting in the main result section. The model was adjusted for priori variables: maternal age, gravidity, ethnicity, maternal education, household size, ethnicity, and perceived low income. In case of missing data, the team reached out to the participants within 24 h of the first attempt of the interview, and where the missingness was high, the team approached the next random participant on the list. No further imputation method was performed in case of missingness.
Ethical considerations and written consent procedure
The research was conducted according to the ethical standards for research with human beings, thus adhering to the Declaration of Helsinki and relevant national ethical standards. Ethical approval was obtained from the Segreteria Tecnico-Scientifica Comitato Etico Interaziendale di Novara (reference number: CE214/2022) and the National Bioethics Committee of Pakistan (Ref: No. 4-87/NBC-843/22/559). Specialized ethical standards were created for this research due to the focus on Afghan refugee women to ensure the protection of this vulnerable population. Measures were taken to ensure confidentiality, voluntary participation, and cultural considerations while gathering the data.
Before participating in the study, all the eligible women were provided with extensive information about the objectives, potential risks, and benefits involved in the research. The written consent process was conducted in Pashto and Dari, the prevailing languages of the participant population, to allow easy understanding of the study. Participants were informed that their participation was entirely voluntary and that they were free to withdraw at any stage without any consequences. They were assured that all answers would be kept entirely confidential and their participation would not affect their access to healthcare services.
In order to cater to the varying levels of literacy among the participants, they were offered an option to consent either in a written manner (e.g., signature or thumbprint) or verbally, with the latter being audio-recorded by the data collector. For those who chose not to sign but were willing to take part, a witness, for example, a family member or community leader, confirmed their consent. All data collected were safely stored, with access limited to authorized research staff only to maintain both confidentiality and integrity of the information.
Results
Population characteristics
From December 1, 2022 to January 10, 2023, 557 MWRA were approached, out of which 533 (94.5%) met the eligibility criteria; 33 (6.3%) eligible women refused to participate and did not agree to consent, and 20 (3.8%) consented to be withdrawn at a later stage of the interview. New MWRA were also approached to complete the sample size of 480. Figure 1 presents the study flow diagram.
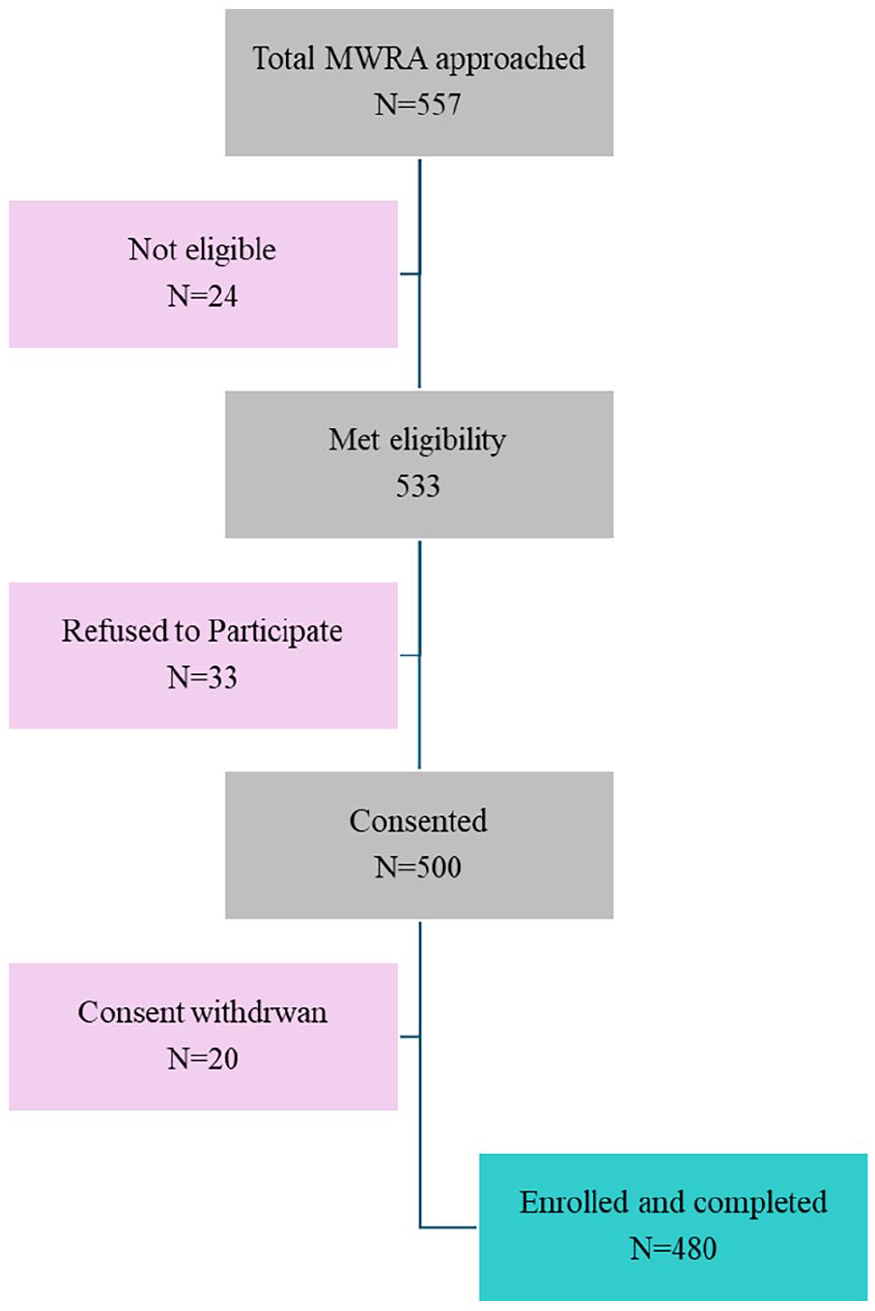
The study flow diagram.
Among 480 MWRA who consented and participated, the mean maternal age was 32.5 ± 6.8 years. The average number of members per household across the sample of families was 8.6. The ethnic composition of the study population was predominantly Pashtun, accounting for 64.4% of the total. Tajiks and Uzbeks followed, comprising 19.6% and 16.0%, respectively. Regarding maternal education, 71.9% had no formal education and 21.5% had at least primary education. Among enrolled MWRA, the mean gravidity and parity were 4.8 ± 2.0 and 4.6 ± 1.9, respectively (Table 1).
Baseline characteristics.

ANC: antenatal care; SD: standard deviation.
Explained as one of the concerns of not seeking care.
Healthcare seeking during pregnancy and childbirth
The health-seeking patterns showed that only 36.9% of the MWRA sought care during pregnancy during the COVID-19 pandemic, and only 13.1% received at least four ANC visits. Among those who did not seek care during ANC, 20.4% shared that fear of getting the COVID-19 vaccine was among the significant concerns. Fear of exposure to the COVID-19 screening test was mentioned by 15.4% of MWRA. Furthermore, at the time of childbirth, 38.8% of MWRA had skilled birth attendants at the facilities. A traditional birth attendant attended all the births at home. Among those who did not seek care during childbirth, 10.0% mentioned that they had a fear of being exposed to the COVID-19 infection. MWRA who received at least one ANC plus had skilled birth attendance were only 32.9% (Table 1).
Predictors of not receiving optimal visit (at least four visits) antenatal period
Demographic factors
Among different refugee ethnic groups, most Pashtuns did not seek ANC; 96.1% (out of 309) did not receive at least four ANC visits. Comparatively, among Tajiks (78.7%; adjusted OR: 0.24; 95% CI: 0.09, 0.52) and Uzbeks (62.3%, adjusted OR: 0.07; 95% CI: 0.03, 0.16), the patterns of better, although not optimal. MWRA residing in households with less than eight members were 93.1% of them did not have at least four ANC visits compared to those living in larger families (82.3%; adjusted OR: 0.34; 95% CI: 0.15, 0.78).
Refugee status
Many MWRA were concerned about their refugee status and experienced challenges in accessing care because of it. Among them, 90.5% reported not receiving the optimal ANC due to the challenges they faced due to their refugee status compared to 83.1% who did not have experienced the same challenges (adjusted OR: 2.83; 95% CI: 1.12, 6.29).
Decision-making and household support
Of women facing challenges to go outside to seek care without accompanying anyone, 92.6% were unable to seek care compared to those with no such constraints (adjusted OR: 2.16; 95% CI: 1.01, 4.63). Preference of traditional care (mostly from traditional birth attendants) of ANC among refugee women resulted in poor care seeking among 91.4% of women, compared to those who did not have this preference (adjusted OR: 2.56; 95% CI: 1.02, 6.41).
Availability and reach
Moreover, lack of availability of ANC services near households was reported in 93.8% who did not receive at least four ANC compared to 82.8% who did not have issues with the availability of ANC services (adjusted OR: 3.30; 95% CI: 1.44, 7.53).
Affordability
Among low-income refugee women, 93.2% did not receive at least four ANC visits compared to 81.5% in MWRA, who had no such financial barriers (adjusted OR: 2.71; 95% CI: 1.27, 5.76). Among refugee women who perceived healthcare has high costs, 92.3% did not receive at least four ANC compared to 82.2% of those who perceived that cost was low (adjusted OR: 2.52; 95% CI: 1.22, 5.19). Concerns related to COVID-19 did not appear as an associated factor (Table 2).
Factor explaining not receiving optimal visit (at least four visits) antenatal period.
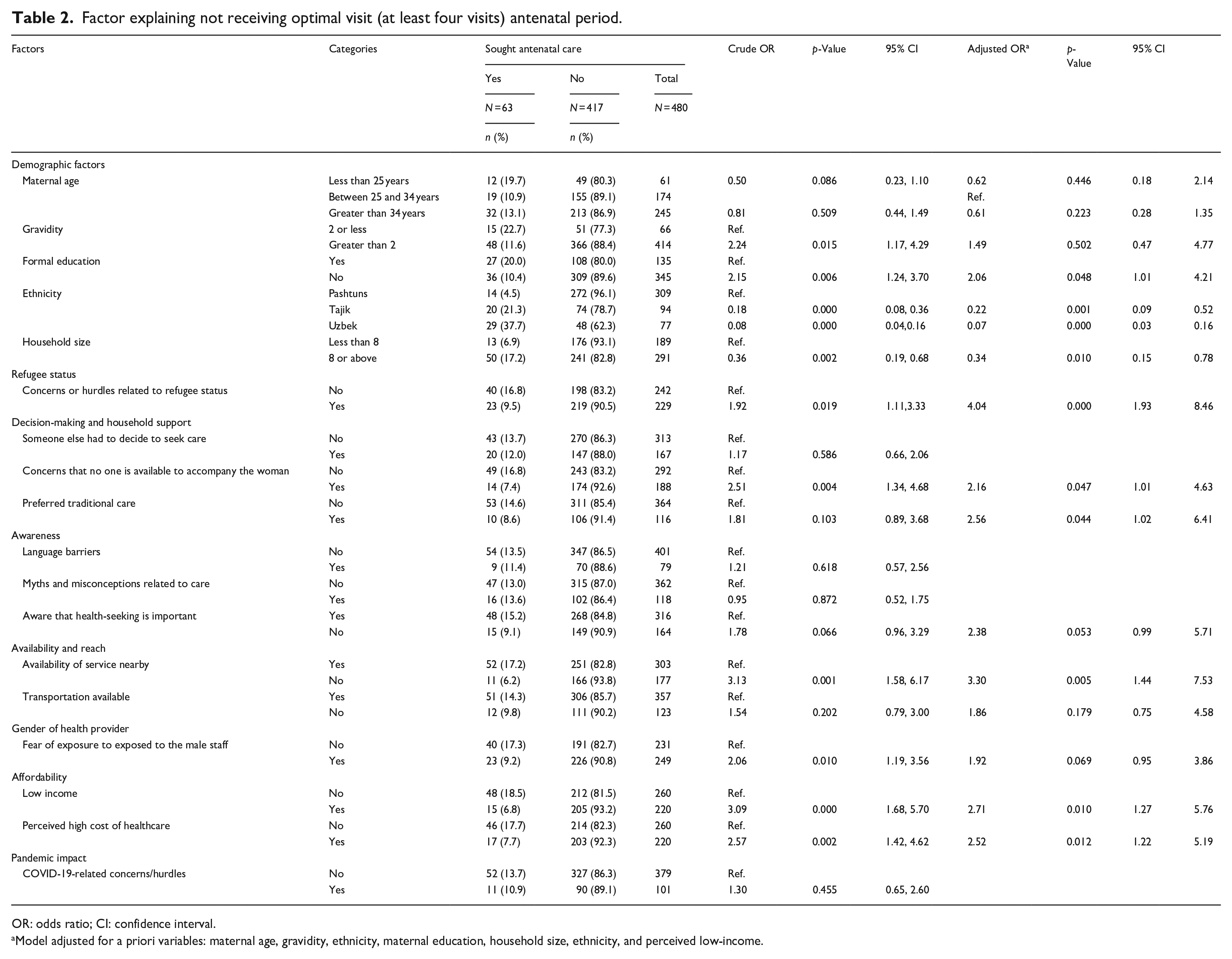
OR: odds ratio; CI: confidence interval.
Model adjusted for a priori variables: maternal age, gravidity, ethnicity, maternal education, household size, ethnicity, and perceived low-income.
Predictors of unskilled births (home births)
Demographic factors
Women aged less than 25 years had more home birth compared to the age group 25–34 years and greater than 34 years (29.5%; adjusted OR: 3.18; 95% CI: 1.22, 8.32). Among Pashtun ethnicity, 70.9% of women had home births compared to lesser proportions in Tajiks (48.9%; adjusted OR: 0.48; 95% CI: 0.26, 0.87) and Uzbeks (37.7%; adjusted OR: 0.31; 95% CI: 0.15,0.64).
Refugee status
Concerns about being a refugee remain highlighted as the major explaining factor for not seeking care during childbirth. About 86.9% of women with such concerns did not deliver at a formal health facility compared to 54.6% of those who did not experience challenges because of their refugee status (adjusted OR: 2.83; 95% CI: 1.27, 6.29).
Gender of health provider
Among those afraid of exposure to male staff, 87.2% did not have skilled birth attendance compared to 49.7% of those with no such fear (adjusted OR: 3.36; 95% CI: 1.70, 6.66).
Antenatal care seeking
Among MWRA who did not seek care during childbirth, 68.3% delivered at home compared to 14.3% of those who received ANC (adjusted OR: 11.60; 95% CI: 4.78, 28.16).
Pandemic-related concerns
Concerns related to COVID-19 remained an insignificant factor (Table 3).
Factor explaining not attending skilled facility during childbirth.

OR: odds ratio; CI: confidence interval.
Model adjusted for a priori variables: maternal age, gravidity, ethnicity, maternal education, household size, ethnicity, and perceived low-income.
Factor explaining no comprehensive care-seeking
Demographic factors
MWRA among refugees, who did not seek any care during ANC as well as childbirth, women with age less than 25 years, 82.0% of them had no care seeking compared to 63.2% in women aged between 25 and 34 years and 66.1% among women aged greater than 34 years (adjusted OR: 4.32; 95% CI: 1.71, 10.93). Among Pashtuns, 73.1% did not have comprehensive care compared to Tajiks (53.2%, adjusted OR: 0.37; 95% CI: 0.21, 0.65) and Uzbeks (59.7%, adjusted OR: 0.59; 95% CI: 0.32, 1.07). Women in small family sizes had poor comprehensive care, that is, 75.1% versus 61.9% in another group (adjusted OR: 0.61; 95% CI: 0.39, 0.97).
Decision-making and household support
Of women concerned that no one was available at the household to accompany them to the health facility, 73.6% did not seek care compared to 58.8% who had no such issue (adjusted OR: 1.78; 95% CI: 1.15, 2.76). If the MWRA had myths and misconceptions related to available care (related to quality, behavior of staff, and other characteristics of care), 72.9% of them did not seek comprehensive care compared to 64.0% of those who had no such myths (adjusted OR: 1.87; 95% CI: 1.17, 3.00).
Refugee status
Refugee concerns were important but became insignificant for comprehensive care; 69.8% of MWRA who had concerns did not have comprehensive care compared to 62.7% among those who had no such concerns (adjusted OR: 1.48; 95% CI: 0.96, 2.27).
Availability and reach
Transport availability was also a major concern; 74.6% had not sought the care who had this concern compared to 62.9% who had access to transport (adjusted OR: 1.79; 95% CI: 1.13, 2.82).
Affordability
Women are concerned about low income; 60.7% delivered at home compared to those with no such concerns (adjusted OR: 1.62; 95% CI: 1.05, 2.50).
Pandemic-related concerns
Concerns related to COVID-19 remained an insignificant factor for this (Table 4).
Factors explaining mothers’ lack of comprehensive care-seeking.

ANC: antenatal care; OR: odds ratio; CI: confidence interval.
Model adjusted for a priori variables: maternal age, gravidity, ethnicity, maternal education, household size, ethnicity, and perceived low-income.
Level of satisfaction with available care
The study examined satisfaction levels for healthcare services among three different groups. The first group comprises MWRA, receiving at least four ANC visits. Only 1.6% reported being very satisfied or felt satisfied, and 4.8% of respondents remained neutral. The largest group, that is, 55.6% and 36.5%, were dissatisfied and very dissatisfied. Of the level of satisfaction among the second group who delivered at a health facility, 8.5% were very satisfied, 16.4% felt satisfied, and 16.4% remained neutral. Among this group, 37.6% were dissatisfied with the healthcare services, and 21.2% were very dissatisfied. Lastly, among the group who sought comprehensive care, 6.3% were very satisfied, and 10.1% were satisfied, 27.8% were neutral, 32.3% dissatisfied, and 23.4% dissatisfied with the overall care. Figure 2 presents the level of satisfaction with services during pregnancy and childbirth.

The level of satisfaction with services during pregnancy and childbirth.
Factors explaining dissatisfaction with comprehensive care
Demographic factors
Among those seeking comprehensive care, 63.0% of women over 34 years were dissatisfied with the services compared to the rest of the aged groups (adjusted OR: 2.13; 95% CI: 1.03, 4.42).
Affordability
The major factor in satisfaction was the perceived high cost of healthcare, which resulted in 66.0% of women being dissatisfied compared to 45.0% of those who perceived the cost as low (adjusted OR: 2.30; 95% CI: 1.12, 4.72).
Health workforce
Satisfaction with the behavior of the staff at facilities was an important factor; women who were not satisfied with the staff’s behaviors resulted in overall dissatisfaction (64.9%) compared to 31.8% of those satisfied with the staff (adjusted OR: 0.25; 95% CI: 1.43, 7.16). Lastly, 64.3% of women were dissatisfied with the number of female staff compared to 31.0% who were satisfied (adjusted OR: 3.37; 95% CI: 1.52, 7.47).
Pandemic-related concerns
COVID-19-related concerns did not appear to be significant (Table 5).
Factors explaining dissatisfaction with comprehensive care.

OR: odds ratio; CI: confidence interval.
Model adjusted for a priori variables: maternal age, gravidity, ethnicity, maternal education, household size, ethnicity, and perceived low-income.
Discussion
Maternal healthcare utilization among Afghan refugee women
This study investigated maternal care tendencies among Afghan refugee women in Balochistan, uncovering that only a small portion of MWRA engaged with ANC services during the COVID-19 pandemic, with only a fraction receiving the recommended four or more ANC visits. Furthermore, the low proportion of skilled birth attendance highlights the limited alignment of MNCH among refugee women, reflecting deeply embedded barriers. The findings of this study are consistent with recent data from Afghanistan, which suggests that only 17.8% of women attended at least four ANC visits, and 53.6% utilized a skilled birth attendance. 45 Furthermore, the last 15 years’ trends show that only 13.3%–14.6% of Afghan women had received at least four ANC visits, 38.6%–46.1% had access to skilled birth attendance and facility births were around 38.7%. 7
Understanding the impact of COVID-19 on maternal healthcare access
Among different expected predictors, COVID-19-related concerns did not emerge as significant barriers to accessing care in this study. This suggests that Balochistan’s preexisting socioeconomic and infrastructural deficits might have already set a low baseline for healthcare access, rendering the pandemic’s additional apprehensions less visible in the study population. 29 Contrary to the initial assumption that the COVID-19 pandemic would significantly disrupt access to maternal healthcare,43 –45 the findings suggest that the pandemic’s impact was not as pronounced as expected in this setting. Literature from other LMICs anticipated and documented substantial disruptions in healthcare services due to COVID-19, especially among the population displaced as a result of conflicts.46 –48 A study conducted in Uganda in a refugee settlement also found no significant change in health service utilization for maternal care services. 49 Although some qualitative studies have highlighted some COVID-19-related barriers to accessing maternal care, for example, fear of exposure, new guidelines at the facility have been implemented to prevent the spread of the virus and new service delivery modalities, such as telemedicine clinics.
On the contrary, building on the findings that COVID-19-related concerns did not significantly impact maternal healthcare access in this study, existing literature suggests that refugee communities often develop resilience and adaptive strategies to navigate healthcare barriers during crises. 50 In many LMIC settings, low-baseline healthcare utilization, reliance on community networks, and informal healthcare-seeking behaviors helped sustain access despite pandemic-related restrictions. 51 Additionally, task-shifting approaches, in which health workers play a greater role in maternal care, have mitigated service disruptions, particularly in fragile health systems. 52 While global studies report severe healthcare disruptions due to COVID-19, the variation in lockdown enforcement, adaptation of telemedicine, and prioritization of obstetric services in some LMIC settings likely contributed to sustaining MNCH services in refugee communities. 51
Sociocultural and structural barriers to MNCH care
MNCH care disparities for refugee women in LMICs are substantial and multifaceted. 15 These disparities often stem from a complex interplay of socioeconomic, cultural, and systemic factors exacerbating this population’s vulnerabilities.16,34 Among these factors, access to MNCH care among the Pashtun ethnicity in Pakistan and Afghanistan is significantly hindered by a complex cultural and social norm. 25 The deeply embedded patriarchal values within these communities often limit women’s autonomy, restricting their ability to seek healthcare independently.53 –56 Decision-making about health services, including MNCH care, is predominantly controlled by male family members, which can delay or prevent timely access to necessary healthcare.57,58 Additionally, there is a notable shortage of female healthcare providers, which is crucial for Pashtun women, who are culturally and religiously inclined to seek care from female practitioners. 59 This scarcity not only exacerbates the challenge of accessing health services but also underscores the broader issue of gender disparities in healthcare provision within these communities.15,16,60
Discrimination in MNCH access among refugees in LMICs
Refugee women in Balochistan face some significant barriers that are commonly reported in other LMICs, such as legal and policy restrictions, language and cultural differences, limited mobility, and lack of awareness about available services. 61 Refugees in LMICs frequently face systemic discrimination that inhibits their ability to access MNCH services, further exacerbating their underlying health vulnerabilities. Empirical evidence suggests that refugee women in Uganda, Kenya, and South Africa commonly face denial of emergency obstetric care, are subjected to prolonged waiting periods, and are verbally abused because of their foreign status, as healthcare providers exhibit a preference for the indigenous population.62,63 Similarly, Rohingya refugee women in Bangladesh report widespread exclusion from government-run public health facilities, which require documentation of nationality in order to provide maternity services, thereby withholding life-saving care to undocumented refugees.64,65 Rohingya women also face gender-based discrimination within healthcare facilities, with numerous reports documenting intentional neglect during childbirth. 66 The exclusionary policies and systemic discrimination against African and Rohingya refugees are mirrored by the plight of Afghan refugees in Pakistan, where legal ambiguities, cultural prejudices, and limited availability of female healthcare professionals greatly impinge upon access to MNCH services.
Additionally, many refugee camps’ overcrowded and resource-constrained settings further limit the availability and quality of healthcare services. 67 For instance, the reluctance toward ANC visits and skilled birth attendance among the study population mirrors trends reported in other regions of Pakistan and LMICs, where limited healthcare infrastructure and sociocultural resistance to formal health interventions persistently undermine maternal and neonatal health outcomes.45,68 –72
Patient satisfaction and perceptions of healthcare services
The findings on maternal healthcare service satisfaction levels among refugee women in Balochistan further illustrate the complex interplay between service availability and perceived quality of care. Despite some access to healthcare services, the pervasive dissatisfaction underscores a critical gap between service provision and refugee women’s expectations or needs. This disagreement is not unique to Balochistan; literature from other refugee-hosting areas highlights similar issues, where the quality of interpersonal care, cultural sensitivity, and logistical barriers to accessing healthcare facilities significantly impact satisfaction levels.21,59,70,73 –75 The implication is that, beyond ensuring service availability, there is a pressing need to enhance the quality, culturally acceptable or appropriate, and accessibility of maternal healthcare services to meet the diverse needs of refugee populations effectively.
Gender dynamics in healthcare access
The underrepresentation of female staff in health facilities can lead to significant dissatisfaction among patients, particularly women.60,76 –79 Refugee women often feel more comfortable and understood when receiving care from female health professionals, especially for gender-sensitive issues such as MNCH. 80 The lack of female staff can deter women from seeking care, leading to delayed diagnoses and treatment. 81 Female health professionals are often perceived for their empathetic communication and patient-centered care approaches, which are critical for building patient trust and understanding. 82 The scarcity of such perspectives can lead to a less inclusive healthcare environment, potentially overlooking female patients’ specific health needs and concerns. However, this is contrary to the recent report published in Afghanistan, where the gender of the health staff was not highlighted as a crucial factor in accessing care. 83
Economic barriers and the role of perceived healthcare costs
Perceptions regarding the cost and quality of PHC facilities significantly influence patient satisfaction and healthcare-seeking behavior.15,57,58,70,83,83 High perceived costs can be a substantial barrier to healthcare services, particularly for individuals in low-income communities. 84 Even when services are nominally free or subsidized, hidden costs such as transportation, lost wages due to time off work, and incidental medical expenses can accumulate, making healthcare unaffordable for many. 85 Negative perceptions of these aspects can lead to dissatisfaction and a lack of trust in the healthcare system, discouraging patients from utilizing PHC services. 86 This can result in increased reliance on emergency services and advanced stages of illness, which are more costly and challenging to manage.
Strengths and limitations
This study has several strengths, including its focus on a highly vulnerable population of Afghan refugee women in Balochistan, a region often overlooked in academic research. Employing a cross-sectional survey approach enabled the collection of comprehensive data on maternal and neonatal healthcare access and utilization during a critical period, the COVID-19 pandemic, offering valuable insights into the healthcare-seeking behaviors of this population. Moreover, the study’s rigorous sampling technique and the reasonable response rate enhance the reliability of the findings. However, this study is not without limitations. Its cross-sectional design limits the ability to infer causality between identified factors and healthcare-seeking behaviors. This approach does neither allow for examining changes or trends in behavior over time, nor does it provide insights into the causal relationships between variables. The cross-sectional design is particularly limited in understanding the dynamic nature of healthcare access and utilization, especially in a protracted crisis like forced displacement compounded by a global pandemic. One limitation of this study is that the questionnaire used was not a previously validated tool. However, it was pilot-tested on 10% of the study population to assess reliability and clarity. Future studies should consider employing validated instruments for comparability across settings. Additionally, the reliance on self-reported data may introduce recall bias, particularly concerning past healthcare experiences and satisfaction levels. In this study, the criteria for comprehensive care were established as at least one ANC visit coupled with skilled birth attendance, diverging from the conventional benchmark of a minimum of four ANC visits. This adaptation was necessitated by the observation that a minimal proportion of women achieved the optimal threshold of four or more ANC visits. Employing a more stringent criterion would have significantly reduced the sample size available for analysis, potentially skewing the study’s findings and limiting the understanding of healthcare access among this population. The chosen definition thus reflects a pragmatic approach to capturing a broader spectrum of maternal healthcare engagement within the constraints of the study’s context.
Recommendations, policy implications, and potential implementation pathways
Based on the study’s findings, the following evidence-driven recommendations are proposed. In addition, several strategic recommendations are offered to support broader system-level improvements in maternal healthcare access for refugee populations.
Evidence-driven recommendations
Strengthen community-based and culturally sensitive maternal health outreach
Barriers related to gender norms, lack of female providers, and limited autonomy call for tailored community-level interventions. 87 Expanding the role of trained female health workers from within the refugee population can increase acceptability, foster trust, and facilitate timely care-seeking during pregnancy and childbirth.
Implementation pathways
○ Engage refugee women as health educators and link them with facility-based services.
○ Conduct home-based maternal health promotion, including birth preparedness and danger sign awareness.
○ Address decision-making barriers by involving male family members in outreach efforts.
Expand mobile and low-cost service delivery models
Access challenges related to distance, transportation, and perceived cost can be addressed through mobile clinics and targeted financial protection. Delivering services directly to refugee communities at low or no cost which can reduce logistical and economic barriers to antenatal and skilled delivery care. 88
Implementation pathways
○ Deploy mobile MNCH units in remote refugee settlements with female-led teams.
○ Provide free or subsidized maternal health services, covering both direct and indirect costs.
○ Introduce outreach-based ANC and immunization days aligned with community schedules.
Improve quality and gender-responsiveness of facility-based services
Low satisfaction with public healthcare, particularly related to provider behavior and privacy, indicates the need for system-level improvements in facility care. Enhancing infrastructure, staffing, and respectful care practices can boost service utilization and patient confidence.
Implementation pathways
○ Invest in upgrading MNCH units in urban centers serving refugee populations.
○ Recruit female staff and provide training on respectful, culturally sensitive care.
○ Establish feedback mechanisms to continuously improve patient experience.
Broader strategic and system-level recommendations
Institutionalize inclusive health policies for refugee populations
Legal, documentation, and entitlement-related concerns affect access to essential care. Maternal health services for refugees must be clearly integrated into national and provincial health frameworks, supported by inclusive policies and financing.
Implementation pathways
○ Enact policy provisions guaranteeing maternal healthcare access for undocumented refugee women.
○ Coordinate with humanitarian actors to align service delivery across agencies.
○ Integrate refugee health into UHC planning and budgeting.
Build Intersectoral Platforms for Sustainable MNCH Delivery
Addressing maternal health barriers requires coordination across health, protection, and development sectors. Multistakeholder platforms can facilitate joint planning, funding, and accountability for refugee-responsive health systems.
Implementation pathways
○ Establish MNCH task forces with representation from health authorities, UN agencies, non-governmental organizations (NGOs), and refugee communities.
○ Align MNCH strategies with broader refugee assistance efforts (e.g., shelter, nutrition, education).
○ Promote data-sharing, joint monitoring, and operational research partnerships.
Conclusion
This study contributes to a growing body of evidence highlighting the multifaceted and intersecting barriers to maternal healthcare access among refugee populations in LMICs, with Balochistan presenting a particularly challenging context. The findings emphasized the need for a comprehensive and context-responsive approach to healthcare provision that transcends traditional service delivery models, advocating for interventions that are gender-sensitive, community-embedded, and culturally adapted to the unique needs of refugee women. As the global community continues to contend with the growing health demands of forcibly displaced populations, the lessons from Balochistan offer valuable insights into designing inclusive, equitable, and resilient healthcare systems that serve Afghan refugees and similarly marginalized groups, ensuring that the most vulnerable populations are not left behind in the quest for universal healthcare access.
Supplemental Material
sj-doc-1-whe-10.1177_17455057251347081 – Supplemental material for Navigating challenges in access to antenatal and intrapartum care: Afghan refugee women’s experiences amidst the COVID-19 pandemic in Pakistan
Supplemental material, sj-doc-1-whe-10.1177_17455057251347081 for Navigating challenges in access to antenatal and intrapartum care: Afghan refugee women’s experiences amidst the COVID-19 pandemic in Pakistan by Yasir Shafiq, Ameer Muhammad, Zamir Hussain Suhag, Rehman Tahir, Abdullah Jan, Huba Atiq, Shayan Khakwani, Muhammad Ahmed, Dua Eva, Luca Ragazzoni, Francesco Barone-Adesi and Martina Valente in Women’s Health
Footnotes
Acknowledgements
This manuscript results from a study conducted in the International PhD in Global Health Humanitarian Aid and Disaster Medicine framework jointly organized by the Università del Piemonte Orientale (UPO). Therefore, the cost of data collection was covered through the university’s PhD funds.
Ethical considerations
Ethical approval was obtained from the Segreteria Tecnico-Scientifica Comitato Etico Interaziendale di Novara (reference number: CE214/2022) and the National Bioethics Committee of Pakistan (Ref: No.4-87/NBC-843/22/559).
Consent to participate
Written consent was taken from the participants in the local languages, explained all the study procedures and risks involved and to make sure voluntary participation.
Consent for publication
Not applicable. This study did not involve the publication of identifiable personal data, images, or case details requiring participant or guardian consent for publication.
Author contributions
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data used in the analysis of this manuscript are available as Supplemental Material.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.