
Abstract
Introduction:
Health inequities begin before birth with Black women being more likely to have low birth weight babies than White and Latina women. Although both Latina and Black women experience discrimination, only Black women appear to be affected.
Methods:
In this study using medical records and face-to-face interviews, we systematically examined the role of discrimination (daily, environmental, vicarious) on continuous birth weight (controlling for gestational age and baby’s gender) in a sample of 329 Black, Latina, and White pregnant women, as well as whether familism, prayer, and/or discrimination attribution buffered this association.
Results:
Linear regression analyses revealed that only prayer acted as a resilience factor, with Latina women appearing to benefit from prayer in the link between vicarious and daily discrimination on birth weight conditional on gestational age, whereas Black women showed no moderation and White women showed an exacerbation in the link.
Discussion:
The results of this study suggest that sociocultural norms may play a role in explaining the Latina epidemiological paradox, but more research is needed to understand the significance.
Introduction
Creating a healthy population begins before birth; integral to this goal is providing the medical and lay community with the necessary tools to assist women in healthy pregnancy and childbirth. Low birth weight (LBW) is one of the most important factors affecting infant mortality and puts those who survive at increased risk for significant health problems throughout life. 1 Socioeconomic status (SES), biological, medical, and behavioral risk factors are all related to LBW; 2 yet, surprisingly, none of these factors are able to account for the opposing prevalence rates seen in Latina and Black women. Nationwide, Black women have the highest prevalence of LBW, whereas Latina women (specifically White Latinas) tend to have the lowest prevalence of LBW. 3 Black women’s high prevalence of LBW has been attributed to prolonged exposure to both structural and interpersonal racial discrimination. Numerous studies have demonstrated the association between racial discrimination and LBW in (primarily low-SES) Black women, but no one to our knowledge has sufficiently explained why pregnant Latina women do not show this increased prevalence.4–7 Recently, sociocultural and psychosocial factors have been proffered to explain the resilience of Latina women with respect to LBW; 2 but, to date, no one has systematically compared the processes of resilience and discrimination on continuous birth weight in a sample of White, Black, and Latina women. Integrative and multi-method research is needed to go beyond simple risk factor analyses of LBW. In this study, we used a novel approach to understand how discrimination and resilience may lead to the contradictory racial disparities in birth weight. Specifically, we examined the intertwining and complex relation of sociocultural, environmental, and psychological factors involved in birth weight conditional on gestational age.
Racial disparities in LBW
Racial disparities in health outcomes are ubiquitous and begin prior to birth.1,8 Please note that we acknowledge there are substantial flaws in the system of racial/ethnic categorization, especially the lack of acknowledgment of heterogeneity within each group and individuals identifying with more than one race/ethnic group. Although this categorization system is imperfect, society tends to treat people as belonging to one group and stereotyping the whole group. 9 Thus, while we acknowledge the limitations, we feel that this single group categorization reflects how society treats the individuals. In comparison to White infants, Black infants face a far greater likelihood of LBW (less than 2,500 grams), very LBW (less than 1500 g), shortened gestation or fetal growth complications, and, finally, death within the first year of life.10,11 Significantly, LBW is the single most important factor affecting neonatal mortality (death within the first 28 days of life), and a major determinant of post neonatal mortality (death between 28 days through the first year). 1 Furthermore, LBW infants who survive the first year are at increased risk for health problems, ranging from neurodevelopmental disabilities to respiratory disorders. 1 LBW costs a society not just socially in terms of increased infant mortality and morbidity, but also economically at a per-patient cost of US$55,393 for premature/LBW births (i.e. less than 37 weeks gestation and/or less than 2500 g). 12 Moreover, the total estimated economic cost associated with premature birth in the United States is US$26.2 billion each year. 13
Initially, researchers believed the most likely explanation was Black women are disproportionately poor, which places them at a higher risk for LBW due to restricted access to prenatal healthcare and other relevant resources. Indeed, socioeconomic status and LBW do show a gradient; however, the findings are not consistent across SES indicators or birth outcomes. Specifically, a graded relationship between SES and LBW has been found for White, Latina, and Asian women, but no such relationship is found for Black women. Thus, it appears Black women do not “reap the same health benefits from higher levels of SES” 14 as do women from other race/ethnic groups. Other risk factors for LBW, such as biological differences, maternal behavior (e.g. smoking, alcohol/drug use), prenatal care, perinatal infection, and maternal stress, have all failed to account for this racial disparity in LBW.15,16 Even when examining multiple risk factors, residual racial differences in LBW remain; one study examining 46 different risk factors only explained about 10% of the variance in LBW, and differences between Black and White women persisted. 17 In other words, although Black women and LBW have been extensively studied, we are a long way from understanding what causes the greater prevalence of LBW in Black women.
Latina women, on the contrary, appear to be buffered from this health disparity—commonly referred to as the Latina epidemiological paradox.18,19 Even though there is significant intragroup variation in LBW, and research has consistently shown that US-born Black Latinas and Puerto Ricans have similar rates of LBW to Black women, White Latina women (especially immigrant Latinas) typically experience lower rates of LBW outcomes than non-Hispanic White and Black women. 3 The most frequently cited reason is sociocultural—that is, cultural norm and value differences. Even so, as with the research on Black women and LBW, the overwhelming majority of research on Latina women and LBW fails to provide a comprehensive, comparative analysis of the risk/protective factors and processes among the three main race/ethnic groups in the United States. It is important to note here that there is an intersectionality between race and ethnicity such that those who identify as Black Latina do not always experience the Latina epidemiological paradox. 20 Moreover, studies usually focus on immigrant Latina women versus Latina-American women, suggesting the important role played by nativity and acculturation in understanding LBW disparities and the paradox.18,21–23 However, this intersectionality is beyond the scope of this study, which seeks to first examine more basic racial differences—as discrimination is often based on societal perceptions of which racial group an individual is labeled.
If the racial variation in LBW is not due to biology, SES, or various other risk factors, then what puts Black women at a greater risk and Latina women at a reduced risk for LBW outcomes? Prolonged exposure to racial discrimination among Black women (across the SES spectrum) has emerged as a potential explanation for their disproportionately higher risk for poor birth outcomes. 24 Referred to alternately as the “cumulative pathway mechanism” 16 or “weathering hypothesis,” 24 this argument states that Black women are constantly vigilant due to their chronic exposure to stress and discrimination which, in turn, affects physiological pathways to health (i.e. allostatic load), 25 including reproductive health. Geronimus argued that physical consequences of social inequalities may explain why Black women experience a threefold increased risk for LBW between 15 and 34 years; 24 namely, Black women experience a marked deterioration in health as a “response to perpetual social and environmental insult or prolonged active coping with stressful circumstances.” 26 Since this seminal study, a number of studies have replicated that exposure to stress, and racial discrimination in particular, is a significant predictor of LBW and other deleterious birth outcomes.27–29 Surprisingly, this research has focused almost exclusively on racism in poor Black women. 30 Only a few studies have compared the role of discrimination in birth outcomes among Black and White women.27,28,31 In these studies, racial differences in LBW and preterm birth are only reduced to a small degree when controlling for racial discrimination.
Race/ethnicity and resilience
The existing research fails to answer the question of why Latina women (specifically those with non-US nativity and less acculturation) do not experience this particular outcome of “weathering” to the same degree as Black women. In other words, what makes Latina women more resilient to discrimination and stress? Sociocultural differences have been the primary explanation put forth for the Latina epidemiological paradox. 32 Among these differences, a focus on familism has been the most salient. Familism (broadly defined as a prioritization of and closeness/intimacy with one’s family) 33 has received limited empirical attention. In one study, Latina women (foreign-born and US-born) reported greater familism and social support than White women, but only general social support was associated with higher birth weight (and for foreign-born Latina women only). 34 Importantly, this study never looked at whether familism was specifically related to birth weight and the analytic strategy consisted of only simple bivariate correlations by group. Only one study, to our knowledge, has actually compared the role of familism on birth weight for Latina, Black, and White women. Using the US. Fragile Families dataset, only a main effect of familism on birth weight was found—that is, there was no interaction with race/ethnicity. 35 One possible reason is the study used a narrow operationalization of familism focusing on structure and obligation. Thus, it is unclear if a more comprehensive measure of familism would show similar results.
In addition to familism, Latina women may differ in two other important ways that might help to explain the paradox: religiosity and attributional style. First, Latinas tend to be more spiritual and religious (with Catholicism as the primary affiliation) than other race/ethnic groups and spirituality may be one reason for the lower prevalence of LBW in Latina women. 36 Magaña and Clark 37 argued that the religious symbol of the Virgin of Guadalupe is uniquely important for Mexican and Mexican American women and may be one factor related to better outcomes in pregnancy for Latinas. They propose that praying to the Virgin may be linked with a personal relationship to her, seeing her as a role model and personal source of comfort that positively influences their health behaviors and is connected with social support and care from other women who share this relationship with the Virgin. Yet, another study of Mexican American and Mexican immigrant women failed to find a correlation between religious identification and beliefs and birth weight. 21 Finally, although two other more recent studies (both using national datasets) found religious service attendance was related to less risky health behaviors during pregnancy and lower odds of LBW,38,39 surprisingly, both studies neglected to examine whether race/ethnicity moderated this relationship.
Although both Latina and Black women experience racial discrimination, their difference in LBW may also be explained by their attributions for discrimination. External attributions lead to a sense that the individual is not to blame, which can protect one’s mental health and social relationships and, potentially, empower the individual to overcome these barriers.40–42 Although research is lacking on whether Latinas are more likely to externalize discrimination experiences than Blacks, we argue that if Latina women make more external attributions for discrimination while Black women make more internal attributions, this difference may help to explain the opposing disparity in LBW. One way this differential may manifest is in their perceived treatment by medical/health professionals. In support of this argument, one study found Latina pregnant women report less discrimination with prenatal care, whereas Black women report more discrimination with prenatal care. 43 If attributional style can be connected with differences in perceived prenatal care, we may be able to develop interventions and training with medical professionals to address and limit this barrier in the patient–obstetrician relationship.
To move the research on racial disparities and LBW from the testing phase to identification and dissemination requires an understanding of the pathways involved. We propose using a psychosocial model as a unifying theoretical framework to understand how discrimination and resilience interact to impact birth weight. 2 Thus, the goal of this study was to ascertain whether specific resilience factors and/or discrimination experiences impact birth weight differentially based on one’s race/ethnic group. To our knowledge, there is no systematic, comparative research that examines the interaction between discrimination and resilience on birth weight among these three groups of women.
This study
LBW and other related birth outcomes have shown a consistent race/ethnic disparity in the United States, with Black women showing a higher prevalence for LBW than White or Latina women. Numerous explanations from SES to lifestyle factors to genetics have been ruled out as explanations for this disparity. Discrimination has emerged as the primary explanation, but it fails to explain why Latina women who also experience persistent discrimination do not suffer the consequence of LBW at the same rate as Black women. To date, comparative studies on race/ethnic differences in LBW have been limited in sample, measures, and analyses. This study had four primary aims: (1) to examine whether Black, Latina, and White pregnant women differed in their reports of discrimination (i.e. daily, vicarious, environmental), resilience (i.e. prayer, familism, discrimination attribution), and birth weight; (2) to examine whether discrimination experiences and resilience factors predict birth weight conditional on gestational age; (3) to examine whether the resilience factors moderate the association between discrimination experiences and birth weight conditional on gestational age; and, finally, (4) to examine race/ethnic differences in these associations.
Based on the prior literature, we hypothesized that Black women will report the most discrimination and lowest birth weight, Latina women will report less discrimination and greater birth weight than Black women but more discrimination than White women. We did not expect a difference in birth weight between Latina and White women. Second, we hypothesized that discrimination would predict lower birth weight, whereas resilience would predict higher birth weight. Third, we hypothesized that resilience (i.e. prayer, familism, and attributional style) would buffer the association between discrimination and birth weight. Finally, we predicted that Latina women would show the strongest buffering effect of resilience compared to Black and White women.
Methods
Participants
An a priori power analysis using G*Power was conducted to determine the appropriate sample size to test the three-way interactions of race/ethnicity, discrimination, and resilience (with up to four covariates) on birth weight. 44 Based on an estimated effect size of (f2) of .05, an alpha of .05, power of .90, and two tested predictors (i.e. the two three-way interactions for race/ethnicity controlling for covariates, all main effects, and lower level interaction terms), indicated that a total sample of 257 would be needed to detect small effect size. A sample of 356 pregnant women participated in the study. Participants were recruited from a regional healthcare organization located in Southwestern United States. Women had to be at least 18 years of age and speak either English or Spanish. The English survey was translated into Spanish and back-translated by a qualified individual who was fluent in Spanish. Participants ranged in age between 18 and 45 years (M = 28.63, SD = 5.33). Most participants in the sample had at least some college or higher education (71.4%), were married/cohabiting (74.1%), had a paid job (67.6%), and made US$50,000 or more in household income (56.1%). The majority of women lived in an apartment or house with family (78.3%), and had a household size of 2 or 3 individuals (55.5%; M = 3.50, SD = 1.83). Participant race/ethnicity consisted of the following groups: Latina (44.9%), White (35.5%), African American or Black (12.1%), Native American (3.1%), Asian (2.5%), and Other (1.7%). For this study, we excluded Native American, Asian, and Other from our analyses due to low sample sizes. Thus, our final sample consisted of a total of 329 women (Latina (n = 160; 48.6%); White (n = 126; 38.3%); African American or Black (n = 43; 13.1%), which is representative of the race/ethnic distribution for the medical facility from which the women were recruited and exceeds the recommended sample size based on the power analyses.
Procedures
The ethical standards of the American Psychological Association were followed in conducting this study and the study was approved by Dignity Health St. Joseph’s Hospital and Medical Center’s Institutional Review Board (IRB #PHXB-18-500-243-70-28) and Arizona State University’s Institutional Review Board (IRB #STUDY00003908). The study was a two-phase (prenatal interview; postnatal medical records) survey with a community sample and independent collection of medical records; data collection occurred between October 2018 and December 2020. Participants were screened for eligibility to take part in the study by an authorized medical professional and contacted to explain more about the study. Flyers were also posted in the waiting room and study team members were at a desk to answer questions from potential participants. If they agreed to participate, they were read the informed consent form by an authorized medical professional and gave their written consent to participate in the study. After obtaining informed consent and permission to access their medical records (N = 356), participants were directed to complete an electronic survey on a tablet (n = 355) as well as an in-person interview with a trained interviewer (n = 317). In-person interviews occurred between 22 and 36 weeks of gestation; if women were not available to complete the in-person interview on the same day as the electronic survey, they were scheduled to complete the in-person interview during a future prenatal appointment between 22 and 36 weeks of gestation. The electronic survey took approximately 15 min to complete and the in-person interview took approximately 45 min to complete. After delivery, medical staff completed a form based on the participant’s medical records and included birth outcomes, health conditions, and risk factors. Participants were compensated US$35 for their time (US$10 for the electronic survey and US$25 for the in-person interview).
Measures
Sociodemographics
Demographic characteristics were collected and included age, race/ethnicity, marital status, education, household income, and household composition. Age range in the sample was between 18 and 45 years. Race/ethnicity items included Asian, Black or African American, Latina, Middle Eastern, Native American, White, or Other. Marital status included married, cohabiting, never married, divorced, separated, or widowed. Participants also reported on their current employment status, number of hours worked per week, and if they had any difficulty affording rent/mortgage. Household composition included household size (from 1 to 10 or more individuals in household including self) and type of housing (e.g. apartment/house, temporary housing, homeless, or other). Education included the categories of less than high school, high school diploma/General Education Diploma (GED), some college/Associates degree, Bachelor’s degree, or post-college degree (e.g. MS, PhD). Total household income included 12 US$10,000 income increments from less than US$10,000 to more than US$150,000.
Baby’s birth weight
Baby’s birth weight was recorded in grams and we used the participant’s medical records to gather the information on the baby’s birth weight.
Discrimination
We assessed three types of discrimination for this study: daily, vicarious, and environmental. Daily discrimination was assessed using the Everyday Discrimination Scale, which consisted of nine items asking participants how often on a day-to-day basis they experience various types of discrimination (e.g. “treated with less courtesy than other people”; “people act as if they think you are not smart”). 45 Items were rated on a 4-point Likert-type scale (0 = not at all; 3 = often). Mean scores were calculated with higher scores indicating greater perceived daily discrimination (Cronbach’s α = .90).
Vicarious discrimination was assessed with two items on 5-point Likert-type scales created for this study: “In general, how frequently do you hear about incidents of discrimination from family, friends, co-workers, neighbors, etc.?” (0 = once a year or less; 4 = everyday) and “Think about people close to you, your family and friends. In general, how much has discrimination impacted their life experiences?” (0 = not at all; 4 = extremely). Mean scores were calculated with higher scores indicating greater perceived vicarious discrimination (Cronbach’s α = .82).
Finally, environmental discrimination was assessed with two items on 5-point Likert-type scales (0 = not at all; 4 = extreme) that were adapted from the Neighborhood Problems Scale: 46 “How much of a problem is pollution (e.g. litter in streets, smells and fumes) in your neighborhood?” and “How much of a problem is safety (e.g. walking around after dark, traffic and road safety) in your neighborhood?” Mean scores were calculated with higher scores indicating greater perceived environmental discrimination (Cronbach’s α = .79).
Resilience
We assessed three resilience factors: prayer, familism, and attribution style. For our measure of religiosity, we assessed prayer with one item asking about weekly frequency (0 = never; 4 = daily). For familism, we adapted an existing measure of familism. 47 Our measure was shortened to five items that asked about participant’s agreement with a series of statements on family (e.g. “A person should rely on his/her family if the need arises”; “A person should always support members of the extended family (e.g., aunts, uncles, in-laws) if they are in need, even if it is a big sacrifice”) rated on a 5-point Likert-type scale (0 = strongly disagree; 4 = strongly agree). Mean scores were calculated with higher scores indicating greater familism (Cronbach’s α = .82). Finally, attribution style for discrimination was assessed with a single item created for the study (“Do you feel that your experiences with discrimination reflect more about something related to you (or your group) or to society as a whole)?”), which participants rated on a 5-point scale (1 = reflect negatively on me/my group, 3 = reflect equally on me/my group and society, and 5 = reflect negatively on society).
Potential covariates
In addition to the sociodemographics, we also assessed a number of potential covariates that are related to birth weight, including mother’s body mass index (BMI), pregnancy comorbidities/complications (e.g. gestational diabetes, eclampsia, hypertension, etc.), and lifestyle factors (e.g. smoking, diet, etc.), baby’s gender, and baby’s gestational age at birth (in weeks).
Overview of analyses
We first tested for potential covariates (i.e. sociodemographics, pregnancy factors, and maternal characteristics) with baby’s birth weight by conducting linear regression analyses predicting birth weight with the sociodemographics entered simultaneously in one block and the pregnancy and maternal health factors entered simultaneously in a separate block. These preliminary linear regression analyses revealed that only baby gender and baby’s gestational age significantly predicted baby’s birth weight; both variables were controlled for in all subsequent analyses with birth weight. To test the study aims and hypotheses, we conducted linear regression analyses and used PROCESS for SPSS Macros for the two-way interactions (Model 1) and three-way interactions (Model 3) with bootstrapping. 48 In the PROCESS macro, interactions were assessed with a t-test of the interaction terms (controlling for covariates, main effects, and lower level interaction terms); a p-value of less than .05 was used to determine significance and a decomposition of the interaction for visualization was conducted by grouping the moderator at the mean and ±1 standard deviation. Preliminary examination of the data revealed that all of the assumptions of multiple regression (i.e. linearity, normality, homogeneity of regressions) were met in the current dataset. Examination of the bivariate correlation matrix did not reveal any problems with multicollinearity (see Table 1).
Bivariate correlations of main study variables.

p < .001; **p < .01; ***p < .05; †p < .10.
Results
Race/ethnic differences in birth weight, resilience, and discrimination
Examination of race/ethnic differences in the main study variables revealed no significant differences among the three groups in birth weight (controlling for baby’s gender and gestational age), likely due to the low number of Black women in the study (see Table 2). However, the data trends supported prior research such that Black women reported the lowest birth weight (M = 3268.25; SE = 65.61) with Latina (M = 3313.99; SE = 33.91) and White (M = 3327.98; SE = 39.23) women reporting similar birth weights. Only 6.1% of the total sample had babies that were classified as LBW (defined as less than 2500 g); as with birth weight, there were no significant race/ethnic differences in LBW (using a logistic regression analysis controlling for baby’s gender and gestational age). Even so, the trend supported the Latina epidemiological paradox, such that Latina women had the fewest LBW babies (4.4%) compared to White (8.1%) and Black (7.8%) women.
Race/ethnic differences in main study variables.
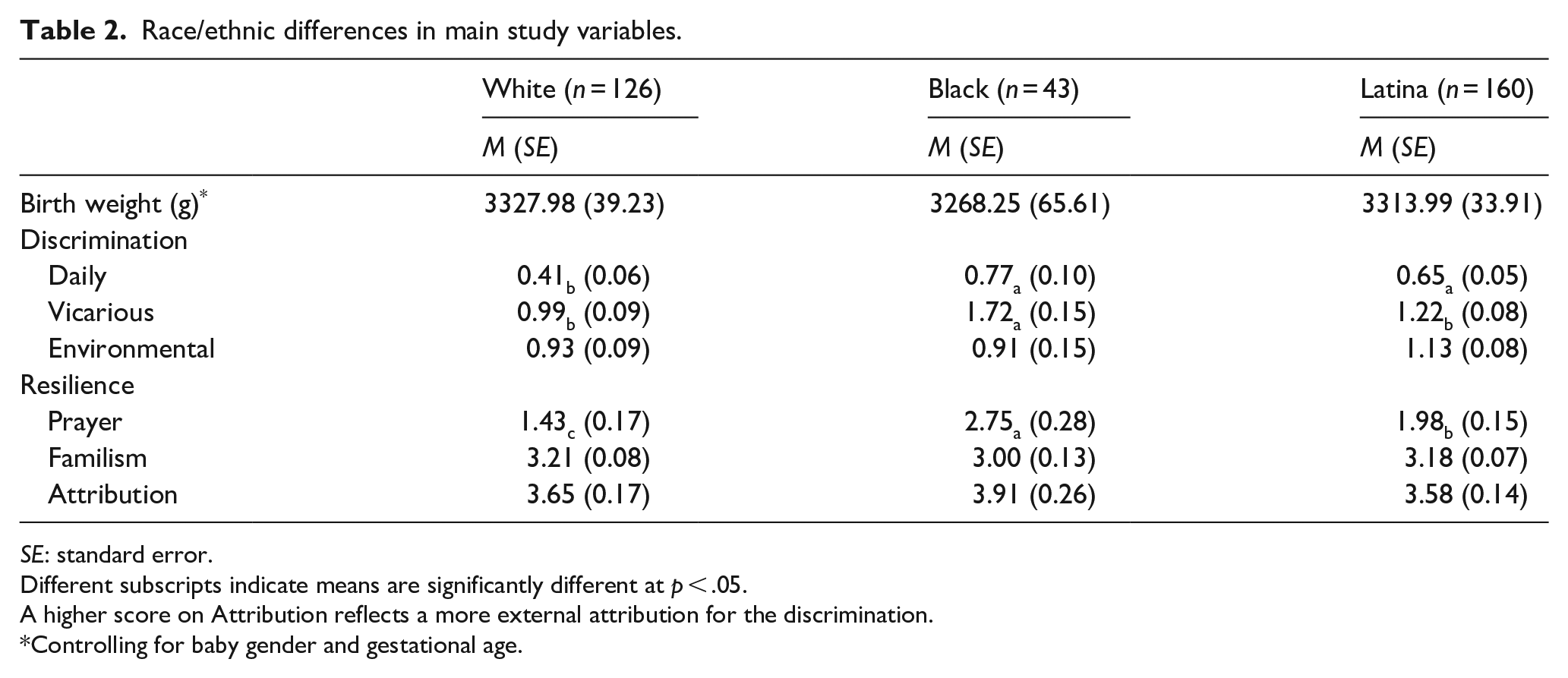
SE: standard error.
Different subscripts indicate means are significantly different at p < .05.
A higher score on Attribution reflects a more external attribution for the discrimination.
Controlling for baby gender and gestational age.
With respect to resilience, all three groups significantly differed from each other in prayer, with Black women reporting the most frequent prayer (M = 2.75; SE = 0.28), Latina women (M = 1.98; SE = 0.15) reporting more prayer than White women and less than Black women, and White women (M = 1.43; SE = 0.17) reporting the least prayer. There were no significant race/ethnic differences in familism or discrimination attribution.
Finally, with respect to discrimination, Black women (M = 1.72; SE = 0.15) reported significantly more vicarious discrimination than Latina (M = 1.22; SE = 0.08) and White women (M = 0.99; SE = 0.09). Black (M = 0.77; SE = 0.10) and Latina (M = 0.65; SE = 0.05) women reported more daily discrimination than White women (M = 0.41; SE = 0.06). There were no significant race/ethnic differences on environmental discrimination.
Role of discrimination and resilience on birth weight
To assess the role of resilience and discrimination on baby’s birth weight, we entered the three discrimination variables simultaneously in a multiple linear regression analysis controlling for baby’s gender and gestational age. Only environmental discrimination emerged as a significant predictor of baby’s birth weight (b = −67.57, se = 25.99, p = .01), such that greater perceived environmental discrimination was related to lower birth weight. In a separate analysis with all three resilience variables entered simultaneously in a multiple linear regression analysis controlling for baby’s gender and gestational age, none of the variables were significant. See Table 3 first column for total sample main effects.
Discrimination and resilience associations with birth weight.

All analyses controlled for baby gender and gestational age.
A higher score on Attribution reflects a more external attribution for the discrimination.
Models without gestational age and with other non-significant covariates are available upon request from the first author.
p < .05; **p < .01; †p = .054.
For the third aim, we examined whether any of the resilience factors moderate the association between discrimination and baby’s birth weight on the total sample (i.e. collapsed across race/ethnic groups). To test for this moderation, we conducted a series of PROCESS Model 1 analyses controlling for baby’s gender and gestational age. We tested each discrimination variable (daily, vicarious, environmental) with each resilience variable (prayer, familism, discrimination attribution). Only one significant interaction emerged between prayer and environmental discrimination (b = 33.61, se = 15.16, t = 2.22, p = .03). A decomposition of the interaction (shown in Figure 1) revealed that those who engaged in more frequent prayer were buffered against the negative association between environmental discrimination and baby’s birth weight.

Prayer and environmental discrimination on baby’s birth weight.
Race/ethnic differences in resilience and discrimination on birth weight
For our final aim, we examined whether there were any three-way interactions between race/ethnicity, discrimination and resilience (controlling for baby’s gender and gestational age) using PROCESS Model 3. A significant interaction emerged between Latina and White women for prayer and vicarious discrimination on birth weight (b = 104.61, se = 35.71, t = 2.93, p = .004). A decomposition of the interaction revealed that prayer buffered the association between vicarious discrimination and birth weight for Latina women (see Figure 2) but exacerbated the association for White women (see Figure 3); Black women showed no association between prayer and vicarious discrimination on birth weight (see Figure 4).

Prayer and vicarious discrimination on baby’s birth weight among Latina women.

Prayer and vicarious discrimination on baby’s birth weight among White women.

Prayer and vicarious discrimination on baby’s birth weight among Black women.
A similar, albeit marginally significant, interaction emerged between Latina and White women for prayer and daily discrimination on birth weight (b = 126.70, se = 65.77, t = 1.93, p = .055). A decomposition of the interaction revealed that prayer buffered the association between daily discrimination and birth weight for Latina women (see Figure 5) but exacerbated the association for White women (see Figure 6); Black women showed no association between prayer and daily discrimination on birth weight (see Figure 7).
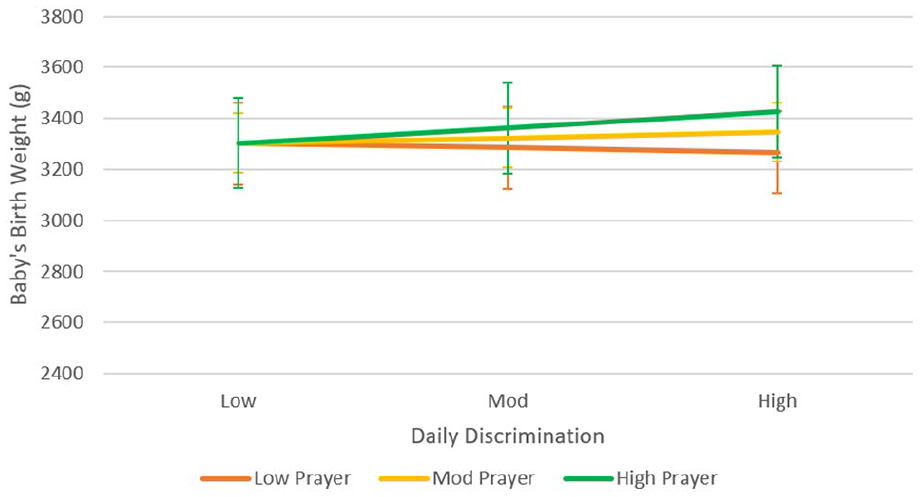
Prayer and daily discrimination on baby’s birth weight among Latina women.

Prayer and daily discrimination on baby’s birth weight among White women.

Prayer and daily discrimination on baby’s birth weight among Black women.
Discussion
The role of discrimination has been posited to explain the racial disparity in LBW for Black women. However, prior research has not explained the lack of racial disparity in LBW for Latina women. Furthermore, prior research has focused exclusively on racial discrimination and often in low-income samples. To our knowledge, our study is among the first to systematically examine the intertwining roles of different types of discrimination and various resilience factors on birth weight (conditional on gestational age) among Black, Latina, and White women. We found no significant difference in birth weight among the three groups; however, the trend supports prior research with Black women having lower birth weight babies than either Latina or White women. In addition, prayer emerged as the most salient resilience factor with discrimination and birth weight—but only Latina women appear to benefit from prayer. We discuss our main findings and implications, as well as limitations and future directions.
Race/ethnicity and birth weight
Although our data did not reveal significant race/ethnic differences in birth weight or LBW classification, likely due to the low number of Black women in the sample (n = 43) and the relatively low amount of LBW babies (6.1% total sample), we did see trends in the data that support prior research. Specifically, Black women had lower birth weight babies than White and Latina women. Moreover, Latina women had the fewest babies classified as LBW. Taken together, these trends support the racial disparity in birth weight for Black women and the Latina epidemiological paradox for Latina women.6,18 One area for future investigation is the inclusion of other race/ethnic groups that also experience discrimination on a daily basis, including Asian Americans, Native Americans, and Muslim Americans. In addition, as we were unable to conduct more nuanced analyses of the intersection of race and ethnicity or examine the role of nativity and acculturation, future research would benefit from examining these more complex intersections and aspects of ethnicity to determine whether the Latina epidemiological paradox is exclusive to White Latina women. Understanding the prevalence of LBW in these other groups will help us to untangle the racial disparities in LBW and whether it is restricted to Black women only.
Role of discrimination on birth weight
Prior researchers have posited that the greater prevalence of LBW in Black women is due to their ever-present experiences with discrimination. Specifically, Geronimus argues that Black women’s daily exposure to discrimination weathers their biological systems through chronic heightened cortisol levels, which leads to lower birth weight babies. 24 However, research testing this theory has primarily focused on low-income Black women and racism exclusively. This focus does not address the Latina epidemiological paradox of Latina women not experiencing this racial disparity and it also does not address the idea that women (regardless of race/ethnic group) may experience perceived discrimination on a daily basis. In this study, we examined the perceptions of discrimination among Black, Latina, and White women and from various sources (daily personal experiences, vicarious experiences of family/friends, and environmental experiences in their neighborhood). As expected, we found that Black women reported more daily and vicarious discrimination than White women, Latina women only reported greater daily discrimination than White women (but not vicarious). Interestingly, none of the groups differed in their reports of environmental discrimination; however, this is likely due to the sample being recruited from one hospital and most of the women living within the same county and neighborhoods. Future research would benefit from recruiting women from multiple locations to determine whether this lack of race/ethnic difference on environmental discrimination remains.
Aside from these race/ethnic differences in levels of perceived discrimination, more important is whether discrimination impacts birth weight and whether it similarly impacts for each group. When entered simultaneously only environmental discrimination significantly predicted lower birth weight, and a subgroup analysis shows this association was specifically only found for Latina women (see Table 3). As we know from the descriptive statistics although the three groups do not differ in their reports of environmental discrimination, pollution and safety concerns appear to be more worrying for Latina women. One possible explanation is that Black and White women may adapt to the environmental concerns in their neighborhood by engaging more in their local community and establishing stronger neighborhood relations (e.g. neighborhood watch groups, block parties). Morenoff found that while adverse neighborhood dynamics (e.g. violent crime, safety fears) negatively impact birth weight, it may be balanced out by the adaptive response of local community engagement. 49 Further research is needed to replicate this association and ascertain the mechanisms involved with birth weight for Latina women. For example, we only assessed the degree to which pollution and safety are problems in their neighborhood, not how worried they are about the pollution and safety concerns nor how involved each participant was in their local community. In addition, we did not assess whether individuals perceived the pollution and safety concerns as being a direct result of institutional/societal discrimination.
We were surprised that daily and vicarious discrimination did not emerge as significant predictors of birth weight, given the strong race/ethnic differences in these experiences. We were curious as to whether it was the overlap of the constructs that contributed to this lack of findings. Thus, we conducted a series of post hoc analyses to determine whether daily and vicarious discrimination were related to birth weight on their own (i.e. not controlling for the other types of discrimination). Even when entered alone, neither vicarious nor daily discrimination significantly predicted birth weight for the total sample. Thus, it appears that daily and vicarious discrimination (regardless of the source) are not the driving force behind the weathering hypothesis. One potential explanation may be due to the low levels of daily discrimination reported by all three groups—the means ranged from 0.41 to 0.77 on a scale of 0 to 4. However, vicarious discrimination had a slightly broader range (0.99 to 1.72) but still did not show a significant association. Future research trying to replicate these associations (or lack thereof) would help us to understand whether these results are sample driven or not. Moreover, future studies would benefit from examining other types of discrimination (e.g. major discrimination events, in-group discrimination) to see whether other dimensions of discrimination significantly predict birth weight.
Race/ethnicity and resilience
We proposed that the Latina epidemiological paradox may be explained by sociocultural differences. Specifically, we tested familism, 35 prayer (as a measure of religiosity), 37 and discrimination attributions, 42 as potential protective factors to explain race/ethnic disparities in the association between discrimination and birth weight. Contrary to predictions and prior research, we found no significant race/ethnic differences in familism and no buffering effect of familism on discrimination and birth weight. This lack of group differences may have been due to our measure, which focused primarily on familial support, whereas prior research has operationalized familism as a combination of support, interconnectedness, 47 and obligation/ responsibility. 50 Similarly, there were no differences in the attributions for discrimination—all three groups fell between the “reflects equally on me/my group and society” and “reflects somewhat negatively on society” with constrained variability around the mean. Thus, the lack of variability is likely to have contributed to attribution style’s non-significance. One limitation is that this construct was only measured with a single item. Future research would benefit from a more comprehensive assessment of discrimination attributions, as well as general attribution style (i.e. internal vs external) or perceived control over the discrimination.
While neither familism nor discrimination attribution were significant buffers, prayer did emerge as a strong buffer between discrimination and birth weight, especially for Latina women. First, contrary to our prediction, Black women reported the greatest frequency of prayer with Latina women falling in the middle and White women reporting the least prayer. Even so, prayer appears to buffer the impact of environmental discrimination on birth weight for the total sample (i.e. collapsed across race/ethnicity). Moreover, prayer buffered the impact of vicarious and daily discrimination on birth weight for Latina women only, and had no impact for Black women. These results suggest that religiosity provides some benefit for Latina women in dealing with the ramifications of vicarious and daily discrimination experiences that Black women do not reap. More surprisingly, prayer appears to exacerbate the association between vicarious and daily discrimination for White women.
Unclear is which specific religious beliefs are at play or if the content or practice of prayer differ by race/ethnic groups. For example, it would be interesting to know if prayer was typically performed alone or in a group. In other words, were Latina women praying while attending mass or having community prayer or was the prayer done primarily alone as silent prayer/meditation? Another possible explanation is that the content of the prayer may influence its efficaciousness. Whittington and Scher 51 found that prayers that express adoration and thanksgiving toward God are related to better psychological well-being, as are prayers where individuals meditate to be open to divine wisdom or guidance (i.e. reception). On the contrary, prayers that contain requests for God to intervene (i.e. supplication) and obligatory prayer are negatively related to psychological well-being. Thus, Latina women may seek comfort and peace or express gratitude through prayer, whereas Black women may ask for the discrimination to stop and are upset when it does not end and White women may express anger at God for the discrimination or engage in prayer out of obligation. Indeed, in a review by Page, prior research suggests that Mexican American women may be able to better handle stressors and “restore emotional balance” in their lives through prayer and that “intercession with God as well as optimism [allows them] to see the goodness around them and hope for the future.” 22 Finally, different religions might offer different teachings about prayer, which might make them more or less effective in their ability to offer support. Future research would benefit from further examining other dimensions of religiosity as well as the specific characteristics of prayer for each group to better understand the mechanisms behind this resilience.
Limitations and future directions
Although this study has several important strengths, including a comparison of the three main race/ethnic groups in the United States, inclusion of multiple measures of discrimination and resilience, and use of medical records for capturing birth weight and other health information, the findings should be interpreted with caution due to a number of limitations. First and foremost, while the sample size of Black/African American women was proportionate to the clientele at the hospital we recruited from, the sample size limited our power in making between group comparisons as well as the generalizability of the findings (or lack thereof) related to this group. In addition, the hospital clientele was primarily from the surrounding neighborhood, which likely accounts for lack of race/ethnic differences in reported environmental discrimination and the similar LBW rates. Thus, because of the limited power for group comparisons and the multiple hypothesis testing, we strongly recommend replicating these findings in larger, more equally sized race/ethnic groups recruited from multiple sites. Second, some of our measures consisted of only one or two items due to the lack of pre-existing measures (e.g. discrimination attribution, vicarious discrimination), thus limiting the reliability of these items. Future research needs to develop more comprehensive measures of the constructs. Finally, the sample was a relatively healthy group of pregnant women with few medical conditions and risk behaviors. As a result, the percentage of LBW babies was much lower than the average for the United States (8.3%). 52 Therefore, we examined the continuous measure of birth weight as opposed to classification as LBW versus normal weight. Even so, we were able to find a consistent and discriminatory set of findings with respect to the role of discrimination and resilience. Examining these issues in a matched comparison of women with LBW babies versus normal weight babies in various race/ethnic groups will allow us to fully investigate the intertwining effects of discrimination and resilience on LBW to help develop effective interventions.
Conclusion
Having healthy babies is key to the health of society. In this study, we systematically examined the role of discrimination (daily, vicarious, environmental) and resilience (prayer, familism, discrimination attribution) on birth weight conditional on gestational age in a sample of Black, Latina, and White women. We found preliminary evidence that prayer appears to buffer Latina women from the negative consequences of vicarious and daily discrimination on birth weight. Furthermore, environmental discrimination appears to play a more important role in birth weight outcomes (especially for Latina women) as compared to vicarious and daily discrimination. This study highlights the need to understand not only the risk factors in birth weight but, more importantly, the resilience factors that can protect women.
Footnotes
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant to the first three authors from Arizona State University and Dignity Health.