
Abstract
Background:
Adolescent pregnancy remains a critical global health challenge, disproportionately affecting low-resource settings and jeopardizing the health, well-being and socioeconomic prospects of young mothers and their children. Globally, 75% of adolescent births occur without adequate medical care, exacerbating risks of maternal and neonatal complications. In Zimbabwe, where cultural, economic and structural barriers further limit healthcare access, adolescent girls face heightened vulnerabilities.
Objectives:
This qualitative study explores the lived experiences and perceptions of adolescent mothers regarding maternal health services in Chiredzi district, Zimbabwe.
Design:
This study employed a phenomenological approach to capture diverse perspectives on maternal healthcare.
Methods:
In-depth interviews with 20 purposively sampled adolescent mothers (aged 15–19) attending Chiredzi General Hospital were conducted in March 2025, immediately after ethical approval was obtained (ethics number: NUST/IRB/2025/38). Data collection continued until thematic saturation was achieved. Interviews were transcribed verbatim and analysed using inductive thematic analysis.
Results:
Analysis revealed 4 primary themes and 24 subthemes, highlighting key barriers to maternal healthcare access. Financial constraints, inadequate transportation and fragmented health services were prominent structural challenges. Sociocultural factors, including stigma, discriminatory attitudes and restrictive gender norms, further deterred care-seeking behaviours. Participants emphasized the need for adolescent-friendly health services, community-based education programs and economic support to mitigate these barriers. Stakeholder engagement, involving policymakers, traditional leaders and healthcare providers, was identified as critical for developing sustainable intervention strategies.
Conclusion:
Addressing the maternal health disparities faced by adolescent girls requires a multifaceted, intersectional approach. Structural interventions, such as improving healthcare accessibility and affordability, must be coupled with community-level initiatives to combat stigma and promote gender equity. Empowering adolescents through education, economic opportunities and culturally sensitive support networks is essential to fostering long-term resilience. Policymakers and program implementers must prioritize adolescent-inclusive health strategies to ensure equitable maternal health outcomes in Zimbabwe and similar settings.
Plain language summary
This study investigated the difficulties young mothers aged 15–19 face when accessing maternal healthcare in Zimbabwe’s Chiredzi District. Through interviews with 20 adolescent girls, researchers identified key barriers including high costs, long distances to clinics, stigma from healthcare providers and communities, and cultural traditions that discourage clinic visits. Many girls reported skipping essential care due to transportation costs or fear of judgment, while others relied on traditional remedies instead of medical services. Participants suggested practical solutions like mobile clinics, youth-friendly health services, and community education programs to reduce stigma. The findings emphasize the urgent need for tailored interventions to help teenage mothers overcome these challenges and access life-saving care.
Keywords
Introduction
Adolescence (ages 10–19) represents a pivotal transitional phase characterized by profound biological, psychological and social development. 1 This period is increasingly marked by a concerning demographic shift where modern adolescents experience earlier sexual initiation but delayed marriage compared to previous generations, creating an extended window of vulnerability to unintended pregnancy. 2 These changes occur against a backdrop of uneven access to sexual and reproductive health education, particularly in low-resource settings where systemic inequities amplify risks.2,3
Globally, adolescent pregnancy remains an urgent public health challenge, with approximately 16 million girls aged 15–19 giving birth each year – accounting for 11% of all births worldwide. The burden falls disproportionately on developing regions, where 95% of adolescent pregnancies occur. 4 Sub-Saharan Africa faces particularly acute challenges, with nearly one-third of girls becoming mothers before age 18. 5 The complications of pregnancy and childbirth are the leading cause of mortality among adolescent girls in low-income countries, highlighting the intersection of biological vulnerability and structural disadvantage. 6
The determinants of adolescent pregnancy are complex and multifaceted. 5 While biological factors such as pelvic immaturity contribute to poorer birth outcomes, social determinants, including poverty, limited education and gender inequality, play equally critical roles. 7 In many settings, harmful traditional practices exacerbate these risks. Zimbabwe exemplifies this crisis, with national data showing that 20% of adolescents aged 15–19 are already mothers or pregnant. 8 Rural disparities are particularly striking, with fertility rates nearly double those in urban areas (120 vs 70 births per 1000 girls). 8
Chiredzi district, a rural region in Zimbabwe’s Masvingo Province, presents a microcosm of these challenges. The district reports (2019–2023 district health data) alarming reproductive health indicators, including:
A maternal mortality ratio of 443 deaths per 100,000 live births
An adolescent fertility rate of 104 births per 1000 girls aged 15–19
Twenty percent of institutional deliveries involving adolescent mothers.
These figures likely underestimate the true burden, as many adolescent pregnancies occur outside formal healthcare systems (2019–2023 district health data). Cultural factors compound the problem, with 58.4% of adolescent pregnancies in Zimbabwe linked to harmful practices, including child marriage and ‘kuzvarira’ (pledging of girls to settle disputes). 9 The district’s socioeconomic context – characterized by high poverty levels, limited infrastructure and seasonal labour migration – further restricts access to quality maternal care (2019–2023 district health data).
Despite global commitments to reduce maternal mortality (Sustainable Development Goal 3.1), adolescents remain underserved by existing health systems. In Zimbabwe, only 63% of pregnant adolescents receive antenatal care from skilled providers, compared to 78% of adult women. 10 Adolescent girls in Chiredzi district face significant barriers to quality maternal healthcare, resulting in suboptimal health outcomes. This research seeks to explore the lived experiences and perceptions of adolescent mothers regarding maternal health services in Chiredzi district, Zimbabwe.
Methods
Study area
The study was carried out in the Chiredzi district, located in southeastern Masvingo Province, Zimbabwe, which has a population of 275,311. 11 The district is primarily home to the Shangani people, a minority ethnic group with distinct cultural traditions, including initiation ceremonies that may contribute to early sexual debut among adolescents. Despite having Chiredzi General Hospital and 23 rural health centres, the district faces significant maternal health challenges, including a high maternal mortality ratio of 443 deaths per 100,000 live births and an elevated adolescent fertility rate of 104 births per 1000 girls aged 15–19 (2019–2023 district health data). These indicators are compounded by substantial unmet family planning needs and deeply rooted cultural norms that influence reproductive health behaviours. The geographic and cultural context of Chiredzi district makes it a critical setting for examining adolescent maternal health challenges. A map of the study area is shown in Figure 1.
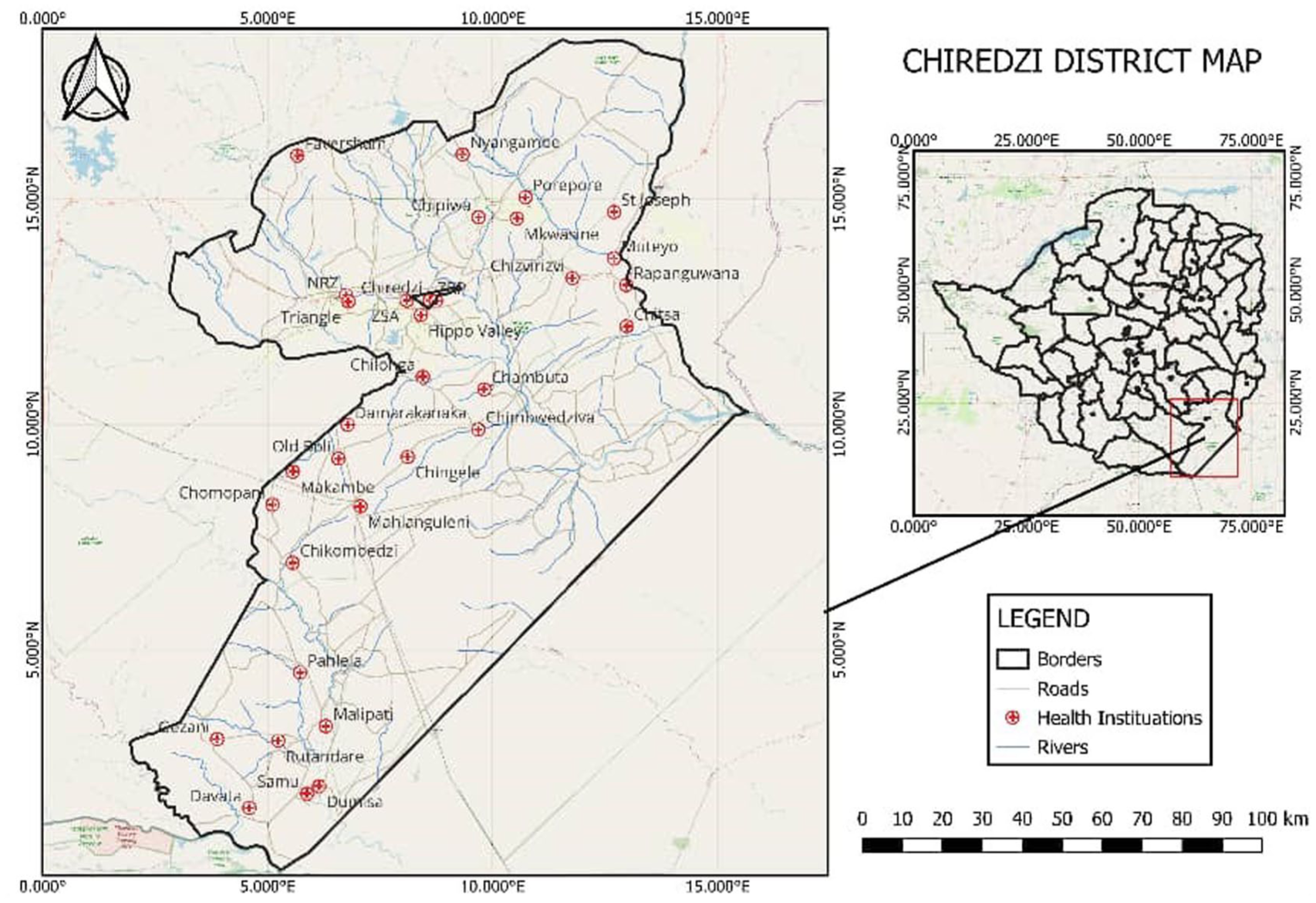
Study area map.
Study design
This study employed a qualitative phenomenological approach to gain an in-depth understanding of adolescent mothers’ experiences with maternal healthcare services. The study spanned from August 2024 to June 2025. The initial phase (August 2024–January 2025) was dedicated to study preparation, including finalizing the research protocol, developing data collection tools, pilot testing and seeking ethical approval. Formal data collection through interviews with participants commenced in March 2025, immediately after ethical approval was obtained (ethics number: NUST/IRB/2025/38). The qualitative methodology was particularly suited for exploring complex social phenomena as it allowed for detailed examination of participants’ lived experiences, perceptions and challenges through rich narrative data. 12 The study aimed to uncover barriers and facilitators to healthcare access, examine cultural and social influences on adolescent pregnancy, identify existing support systems and coping strategies, and gather participant recommendations for service improvement. Data collection continued until thematic saturation was achieved, ensuring comprehensive representation of diverse perspectives while maintaining methodological rigour.
Target population and sampling
The study focused on pregnant adolescents aged 15–19 receiving care at Chiredzi General Hospital, the district’s primary referral facility serving numerous rural clinics. Adolescents below 15 were excluded due to the exceptionally low prevalence of pregnancy in this age group within the study setting and additional ethical complexities involving very young mothers. Participants were selected through purposive convenience sampling, which enabled the recruitment of information-rich cases while accounting for practical constraints in this healthcare setting. Inclusion criteria were: (1) being aged 15–19, (2) being pregnant or in the postpartum period (up to 6 weeks after delivery), (3) receiving services at Chiredzi General Hospital or its linked clinics and (4) willingness to provide informed assent/consent. A total of 20 adolescent mothers were interviewed, with the sample size determined by reaching data saturation. This approach ensured the inclusion of participants with varied experiences across the district while maintaining ethical standards through voluntary participation and informed consent. The selection criteria specifically targeted adolescents who were either currently pregnant or in the postpartum period and were willing to share their experiences through in-depth interviews.
Data collection procedure and tools
The study employed in-depth interviews as the primary data collection method to comprehensively explore adolescent mothers’ experiences with maternal healthcare services. A semi-structured interview guide (provided as Supplemental File 1) was developed, consisting of six thematic sections: (1) introduction and background information, (2) access to and utilization of maternal health services, (3) challenges and barriers encountered, (4) available support systems and facilitators, (5) interactions with healthcare providers and community members and (6) economic considerations and future aspirations. The interview guide was pretested with five adolescents not included in the main study to check for comprehension, flow and cultural appropriateness; minor modifications to question phrasing were made based on this feedback. Prior to data collection, rigorous ethical protocols were implemented.
Interviews were conducted in private settings at Chiredzi General Hospital by the principal investigator, lasting between 20 and 40 min each. To accommodate linguistic diversity, interviews were conducted in participants’ preferred language (English, isiNdebele, or Shona). The interview instruments underwent rigorous translation procedures to ensure conceptual equivalence across languages. This involved forward-translation by native speakers, back-translation by independent translators and reconciliation of any discrepancies through expert review. The tools were pretested with five adolescents to verify comprehension and cultural appropriateness. With participants’ consent, all interviews were audio-recorded using digital recording equipment. In the few instances where participants declined recording (n = 2), comprehensive handwritten notes were taken during the interview and expanded immediately afterwards. Interviews were conducted by the first author.
Data management and analysis
The audio-recorded interview data were transcribed verbatim and imported into NVivo 12 (released in March 2018 by QSR International; https://www.qsrinternational.com) for systematic analysis. Two researchers (the principal investigator and a trained research assistant) independently coded the transcripts using a hybrid approach. A deductive coding framework was initially developed based on key concepts from the literature review and the interview guide, providing structure. This was complemented by inductive coding to allow novel them-59-es emerging directly from the participants’ narratives to be captured, which is consistent with a phenomenological approach seeking to understand the essence of lived experiences. Transcripts in local languages were subsequently translated to English for analysis, with back-translation verification conducted on 20% of transcripts to maintain translation fidelity. The initial coding utilized a combination of deductive codes derived from key concepts in the literature and inductive codes emerging from the data. An iterative process of open coding identified key themes, followed by axial coding, to explore the relationships between them. 13 The research team held weekly coding meetings to review and refine the codebook, resolve discrepancies through consensus and enhance interpretive consistency. The final thematic structure, comprising 4 primary themes and 24 subthemes, was rigorously developed to address all study objectives while remaining grounded in participants’ lived experiences. The research team adhered to the COREQ (Consolidated Criteria for Reporting Qualitative Research) checklist throughout the analysis and reporting process to ensure methodological transparency and rigor. 14 To enhance trustworthiness, member checking by sharing summaries of key themes with a subset of participants for validation was employed, maintaining an audit trail of analytical decisions and practicing reflexivity through team discussions to bracket preconceptions. The completed 32-item COREQ checklist is provided as Supplemental File 2.
Results
The study engaged 20 adolescent mothers between 15 and 19 years of age who were accessing maternal healthcare services at Chiredzi General Hospital. The participants included a diverse group of adolescent girls with varying backgrounds and experiences from different socioeconomic, educational and cultural contexts. This included girls from various ethnic and linguistic groups, such as Karanga and Shangani speaking people, allowing for a more comprehensive understanding of how cultural beliefs and practices influence their perceptions and experiences of maternal health services. Participants were from urban, rural areas, and resettlements representing a varying level of exposure to maternal services. Key demographic characteristics of the participants are summarized in Table 1.
Key informants.

Themes that emerged
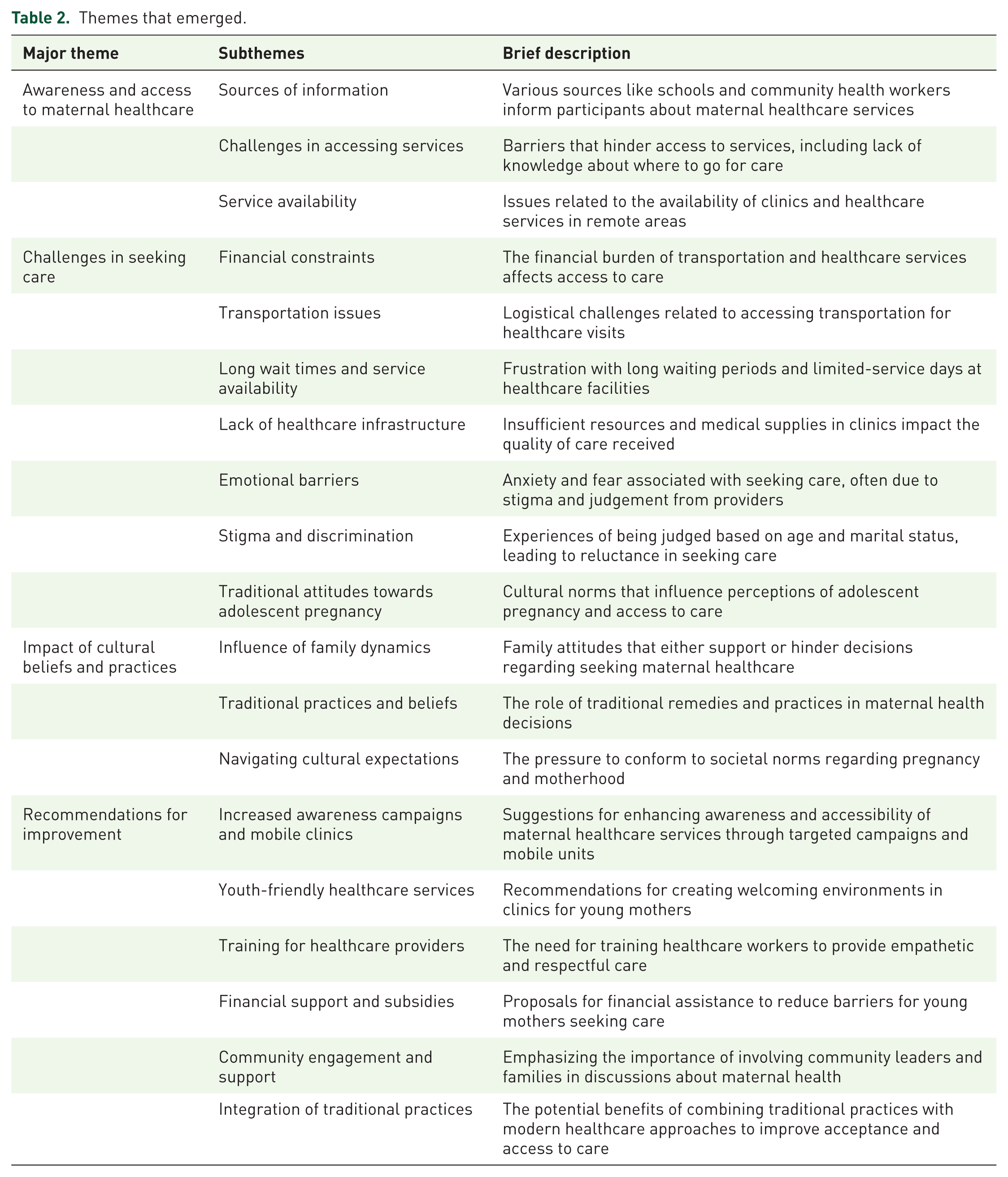
Four main themes were identified, guided by the study objectives and interview guide structure. Additionally, 24 subthemes emerged from the data. These findings are presented in detail in the following sections, as summarized in Table 2. These themes are discussed in detail in the following sections.
Themes that emerged.
Awareness and access to maternal healthcare
The participants exhibited a wide range of understanding regarding maternal healthcare services, which significantly influenced their ability to access the care they required. Those with more knowledge were better equipped to navigate the system and advocate for their needs, while those with less awareness often struggled to find the appropriate resources and support. This disparity in knowledge created varying levels of empowerment and accessibility among the individuals in the group, ultimately impacting their overall health outcomes during the maternal care process. These are detailed below.
Sources of information
Participants gained knowledge about maternal healthcare from multiple channels, including schools, community health workers, peers and family members. School-based health education was cited as a major contributor, especially for those still enrolled in formal education. Numerous girls stated that they learnt about maternal healthcare from a variety of sources, such as community health professionals and schools. Participants shared that:
I first heard about prenatal care in school during our health education classes. The teacher talked about the importance of getting regular check-ups when you are pregnant. But I didn’t know where to actually go for those services. I_01 The community health worker usually moves around the community sharing the importance of prenatal health care. The knowledge is also in the clinic’s picture and Infographics, which convey information about the goodness of prenatal care. The community health care workers usually put more emphasis on adolescent mothers who dropped out early from school since they know that they were missing out on the knowledge that they should have attained from school. I_11 There was a community health worker who works in our neighbourhood and explained what services were available at the clinic. She told us about family planning and where to go if you are pregnant. Without her, I wouldn’t have known much. I_05 One of my communities was like a mother to me from our religious sect, who was encouraging us to maintain a constant check-up of the pregnancy to avoid fatal complications. Our church devoted some significant time to incorporating either a nurse or community health care within the church to educate the health-related topics within girls’ fellowships. The youth leader, even our parents, shares significant knowledge, usually from their experience. The community presents itself as a source of knowledge. I_13
Challenges in accessing services
Despite some level of awareness, several participants noted obstacles that prevented them from accessing maternal healthcare. These included long distances to clinics, lack of transportation, cost concerns and fear of stigma, especially for unmarried adolescents. Despite these avenues for learning, participants faced several challenges when trying to access maternal healthcare services. Many expressed concerns about the availability and accessibility of clinics. Participants shared that:
The clinic is far from my home, and sometimes I don’t have enough money for transport and the area is too remote, I have to walk a distance of around 7 km to the tarred road where I could get a reliable transport system, and this is exhaustive and tiresome knowing that I will be expected to stand in queues after reaching the clinic. I know I need to go for check-ups, but it’s not easy to get there given the remote location, which is far from the road network and queues for service. I_02 The clinic is only open during the day, and if I have school, I can’t go. I wish they would have more hours, maybe even normalise working usual hours on weekends and public holidays. I_04 I didn’t know I could get free pregnancy tests at the clinic until my friend told me. I thought I had to pay, so I was hesitant to go. I_05
Overall, while participants demonstrated some awareness of maternal healthcare services being offered by community health workers and schools as well as the community, significant barriers remained that hindered their access, given the remote area, which includes some resettlement areas which has poor road networks. These included logistical challenges such as distance, transportation costs, availability of transport system and limited clinic hours. Enhancing awareness through targeted educational programs and improving accessibility to services are critical steps needed to support adolescent girls in Chiredzi district.
Challenges in seeking care
Participants identified several significant challenges when seeking maternal healthcare services, which impacted their ability to access timely and adequate care. These challenges ranged from financial constraints to logistical issues related to healthcare infrastructure – long wait times, service availability and emotional barriers.
Financial constraints
One of the most pressing barriers discussed was the financial burden associated with accessing maternal healthcare. Most of the participants reported that the costs of transportation and healthcare services were a prohibitive challenge they usually encountered, given that they rely on peasant farming, which usually has a payment season once a year, which is their main source of finance. Participants shared that:
Most of us in these areas rely on cotton farming and farming maize for consumption, which makes it hard to save enough money throughout the year. The proceeds of farming are supposed to cater for next season’s farming, school fees other food stuff, which is really a challenge. Medical bills are usually met by selling assets, and it is not feasible to sell the best to cater to maternal care. I often have to choose between spending money on food and getting to the clinic. If I don’t have enough for both, I skip the clinic visit by postponing, hoping in due time I will visit whenever I get an inevitable journey. To be honest, prenatal care comes as a secondary preference. I_12 Even when I manage to get to the clinic, I worry about paying for any tests or treatments. I’ve heard that some services can be expensive, and I don’t want to end up in debt because as a family, we’ll skip some essentials to balance the financially constrained budgets. Though it might deliver us into negligence predicament, we don’t have a choice. I_14
Transportation issues
Transportation emerged as a critical logistical challenge. Many participants lived in remote areas where public transport was scarce. Participants shared that:
The nearest clinic is over 30 kilometres away, and I am far better than others. Walking there takes a long time to the tarred road, which is 7 km away, till I get reliable transport, and if it’s raining, I can’t go at all. I need to rely on my family to drive me, but they are often busy since we rely mostly on farming. I_19 Sometimes I have to wait for days until someone can take me. I know it’s important to get checked, but I can’t always find a way to get there. I_01
Long wait times and service availability
Participants also expressed frustration with long waiting times at healthcare facilities in relation to long wait times and the limited availability of services. These issues were especially discouraging for adolescents who may already feel anxious or stigmatized when seeking maternal healthcare. Many girls recounted experiences where they had to wait several hours, sometimes without being attended to at all, which deterred them from returning to the facility in the future. The long queues were often attributed to a shortage of healthcare workers and high patient volumes.
When I finally get to the clinic, I often have to wait for hours just to be seen. It feels like a whole day is not enough since I will not be able to be home in time to travel home, and I don’t always have that time, especially with school. We need 2 days to get service usually, those who have relatives nearby clinics have to sleep nearby to get attended first so that they can travel early; otherwise, the travel back journey comprises my safety. I_20 Additionally, the limited availability of services on certain days posed a challenge. Interviewee 19 highlighted: I went to the clinic on a Monday, but they told me that the doctor only comes on Wednesdays. I had to go home and wait another two days. Most of the Chiredzi residents from rural areas rely on farming, and we don’t have time to waste, especially during the rainy season. I_19
Lack of healthcare infrastructure and utilities
The inadequacy of healthcare infrastructure was another significant concern. The interviewee reported a shortage of medical supplies and staff, which negatively impacted the quality of care. Interviewee 12 described a troubling experience:
When I went for a check-up, they ran out of pregnancy test kits. I had to come back another time, which was frustrating because I needed answers right away. I_12 Some of the efforts usually turn out to be fruitless, especially when I wanted a scan, which was a service that you would be referral to a private hospital, usually after sitting that the materials to be used were used up. This is disappointing, especially when you were referred by someone who said they had used the same facility before and after. I suggest that those who offer money, which is said to buy your utilities, are being attended to. I suspect the financial gains through giving service for money. I_15
Emotional barriers
Lastly, emotional barriers also played a role in seeking care. Many participants expressed feelings of anxiety or fear about visiting healthcare facilities. Interviewee 1 noted:
I feel nervous when I go to the clinic because I’m scared of what the staff might think of me. Sometimes I just avoid going altogether due to the nature of those who attend, as they keep reminding me that I’m out of time and better be fast, or I won’t be able to attend. It seemed they are overwhelmed, exhausted, and always busy some of the facilities are understaffed and a lot of members wend back home unattended and its now usually to them that they are no longer have desire to serve all. sometimes they serve less than usual citing that they cannot exhaust all of them no matter how hurry they might be due the understaffed. I_01
Overall, the challenges faced by adolescent girls in seeking care are multifaceted, combining financial, logistical and emotional barriers. Addressing these challenges is essential to improving access to maternal healthcare services and ensuring that adolescent girls receive the support and care they need. The resettlement areas are the most common areas in Chiredzi district, and in those resettlement areas that were established since 2000 to date, there exists no health facility, which makes it more remote to access health, as well as a poor road network and school facilities. They usually rely on the previously established facilities, which are a great distance from them.
Stigma and discrimination
Experiences of stigma and discrimination when seeking maternal healthcare were common among participants. Many expressed feelings of being judged by healthcare providers based on their age and marital status, which significantly impacted their willingness to seek care.
Most of the patients from our minority group were in the habit of being married at a young age, usually after the adulthood ceremony conducted in winter, which some nurse usually uses as a mockery, as they know that soon after that ceremony, most of them get pregnant, as the society considers them ready for handling marriage affairs. The frequency of the pregnancy seems to irritate the nurses whenever they hear your tone and language, and they would curse the burden that the ceremony brings to them. I_17
Judgement from healthcare providers
Participants reported instances where healthcare providers exhibited bias against them, often treating them with disdain or condescension. Participants shared that:
When I went to the clinic for the first time, the nurse looked at me and said, ‘You’re too young to be pregnant. What were you thinking?’ It made me feel so ashamed, and I didn’t want to go back. I_19 The nurse asked me why I didn’t just wait until I was older to have kids, though in a friendly manner. She treated me as her daughter because she said I was the same age as her daughter, and she gave me a lot of advice, which made me feel uncomfortable. It felt like he was blaming me for my situation instead of helping me, and I feel embarrassed to face her again. I_16
Fear of seeking care
The fear of encountering judgement or negative reactions from healthcare providers often deterred participants from seeking necessary services.
I sometimes avoid going to the clinic because I’m scared of what the staff will say. I don’t want to feel judged for being a young mother. I_12 This fear was compounded by the stigma associated with being an adolescent girl seeking maternal healthcare. Interviewee 14 noted: I’ve heard my friends say they were treated badly at the clinic, so I worry about going. It’s like there’s this unspoken rule that young girls shouldn’t be having babies. However, the community care worker in the neighbourhood is more friendly and they kept on pushing and advising me to do the right thing. I_14
Social stigma in the community
Beyond the healthcare setting, participants also faced social stigma from their communities. Participants described how societal attitudes influenced their experiences:
People in my neighbourhood talk behind my back. They think I’m irresponsible for getting pregnant at my age, and it makes me feel isolated. I_15 I can’t talk to my friends about my health or what I’m going through because I’m afraid they’ll judge me too. I_17
Traditional attitudes towards adolescent pregnancy
Participants articulated how cultural norms often stigmatize adolescent pregnancy, leading to feelings of shame and reluctance to seek care. Participants shared that:
In our culture, getting pregnant at a young age is seen as a failure. People talk about you, and it feels like you’ve let everyone down. This makes it hard to reach out for help. While others will be proceeding with their school life, pregnancy tends to end educational life for the girl child, while if the father has the chance to continue without ridicule. The parents will stop supporting you; they usually say you are a grown-up and it’s your own baby to carry, and facing in-laws is another burden that could lead to suicide if not handled well. The societal values make a pregnant girl an outcast. I_10 My family was very disappointed when they found out I was pregnant. They said I should have waited until I was older. It’s hard to ask them for support when I know they feel this way. I_09
Influence of family dynamics
Family attitudes played a crucial role in shaping participants’ decisions regarding maternal healthcare. Participants shared that:
I wanted to go for a check-up, but my mother told me to wait until after the baby was born. She believes that religious leaders can help more than doctors. I felt stuck because I didn’t want to upset her. I_03 My aunt encouraged me to go to the clinic and get proper care. She said it’s important for my health and the baby’s health, and I’m grateful for her support. I_06
Traditional practices and beliefs
Participants reported that traditional practices often dictated how they approached maternal health. Participants shared that:
Most of the people in my community believe that certain herbs can help with pregnancy. I’ve seen women relying on these remedies instead of going to the clinic. It appears to be the complementary of best alternative way to handle prenatal care. I_07 I’ve heard older women say that doctors don’t understand our bodies like traditional midwifery does. It makes me question whether I should trust the clinic or not. There is this common myth that nurses prefer to learn to perform a caesarean birth type, which is dangerous, while traditional midwifery is patient to handle normal birth. The COVID-19-orchestrated lockdown era gave more reverence to traditional midwifery, and it has proven their capacity and societal acceptance, though there are a few exceptional cases and there are reports of poor service delivery within hospitals, as most of pregnant women will be kept referred to other big hospitals, showing poor, under-resourced health facilities that are at risk of being attended to. The traditional midwiferies are concerned and caring as compared to overpopulated hospitals with reports that you can give birth unattended and usually, they lack beds. The first pregnancy is riskier and complicated to be taken to such a facility, though they might be best suited but under resources. I_02
Navigating cultural expectations
Navigating cultural expectations was a common theme among participants. One of the participants reflected on the pressure to conform:
There’s this expectation that young girls should focus on school and not get pregnant. When you do, you feel like you’re letting everyone down. It’s hard to balance those expectations with the reality of being a mother. The is usually denial from parents and expulsion from home to be with the husband, who also might face the same expulsion from his parents. I_16
Recommendations for improvement
Based on the findings of this study, participants provided valuable insights and recommendations aimed at improving maternal healthcare services for adolescent girls in Chiredzi district. These recommendations focus on enhancing awareness, accessibility and the quality of care.
Increased awareness campaigns and mobile clinics
Participants emphasized the need for targeted awareness campaigns to educate both adolescents and the community about available maternal healthcare services. Participants shared that:
Schools should have regular health education classes that include information on where to get maternal healthcare. It would help if we learned about it before we actually need it. Mobile clinics serve a lot, especially to address the issue of accessibility. The financial and logistic barrier will be solved by regular mobile clinics and well communicated for wider coverage. I_18 Community health workers can organize talks in neighbourhoods to explain the services available. They can make a big difference in spreading the word as well as campaigns that will help to spread the message not only to adolescents but inclusive to the parents and guardians. I_03
Youth-friendly healthcare services
Creating youth-friendly healthcare environments was a common recommendation. Participants expressed a desire for clinics to be more welcoming and accommodating to young mothers. Participants shared that:
If clinics had special hours for young girls, it would help us feel more comfortable. We wouldn’t have to worry about running into people who might judge us. I_20 Having staff who understand our needs and who are trained to talk to us without judgment would make it easier for us to ask questions and seek help any time. I_04
Training for healthcare providers
Training healthcare providers to be more empathetic and understanding was highlighted as crucial. One of the participants emphasized that:
Healthcare workers need training on how to treat young mothers with respect. They need to understand the challenges we face. If they could learn about the stigma we face and how to communicate better, it would make a huge difference. I_15
Financial support and subsidies
Addressing financial barriers was a significant concern for participants. Participants shared that:
The government should consider providing free or subsidized services for young mothers. This would encourage us to seek care without worrying about costs. I_08 Transportation assistance could also help. If we had support to get to the clinic, more girls would visit. I_03
Community engagement and support
Engaging community leaders and families in discussions about adolescent maternal health was seen as vital. Participants shared that:
Community leaders could hold meetings to talk about the importance of supporting young mothers. If families understood the challenges we face, they might be more supportive. I_04 Creating groups for young mothers to share their experiences could help us feel less alone and more empowered to seek care. I_11
Integration of traditional practices
Recognizing and integrating traditional practices within the healthcare framework could also improve acceptance. One of the participants stated that:
If clinics could work with traditional healers and find a way to combine both approaches, it might help girls feel more comfortable seeking care. During COVID-19, most of the patients honestly did not trust any health facility, and without working with traditional healers and religious healers, the health surveillance system was underinformed. I_09
Overall, these recommendations highlight the need for a multifaceted approach to improving maternal healthcare for adolescent girls. Improving awareness, accessibility, provider training, and community engagement will help stakeholders create a more supportive environment that encourages young mothers to seek the care they need.
Discussion
The findings highlight significant barriers to accessing maternal healthcare services for adolescent girls in Chiredzi district. Stigma, financial limitations and inadequate healthcare provider interactions emerged as critical issues. The results underscore the need for targeted interventions to improve service delivery and create a more supportive environment for adolescent girls seeking maternal healthcare. The results of this study highlight the many obstacles pregnant teenagers in Zimbabwe’s Chiredzi district encounter while trying to get maternity healthcare. Significant physical, emotional and social changes occur throughout the crucial adolescent years.15 –18 Teenagers navigating these transitions have increased chances of early and unplanned pregnancies, which can result in serious health issues and social disapproval.16,19
The study’s participants reported differing degrees of knowledge about maternal healthcare services, which they frequently learnt about from community health workers and schools. However, their access was severely restricted by logistical obstacles like the cost of transportation and the distance to clinics. This is consistent with research by Banke-Thomas et al., who highlighted that teenagers’ capacity to seek treatment is severely hampered by financial limitations and infrastructure issues. 2
Additionally, participants’ health-seeking behaviours were significantly influenced by the stigma attached to teenage pregnancy. In many communities, adolescent pregnancy is perceived as a moral failure or a sign of poor upbringing, which exposes young girls to public shame, judgement and social isolation. This negative perception created an emotionally hostile environment that discouraged adolescents from openly seeking maternal healthcare. Many participants feared being recognized at health facilities and being labelled or gossiped about by healthcare workers, peers or community members. As a result, they often delayed or completely avoided seeking care, even when they were aware of its importance. For some, the fear of stigma outweighed the perceived health risks of not receiving care. Due to a societal narrative that portrays adolescent pregnancy as abnormal, many people voiced fear of criticism from medical professionals and the general public. 20 In addition to discouraging young mothers from telling others about their pregnancies, this stigma also fosters a culture of non-disclosure, which causes delays in getting necessary prenatal care. 21
Access to care was also significantly impacted by cultural practices and beliefs. Shame and an unwillingness to seek help were common outcomes of traditional beliefs on adolescent pregnancy. Adolescent females’ vulnerabilities are made worse by detrimental cultural practices including forced marriage and specific initiation ceremonies, as stated by Nunu et al. In order to create a supportive environment that motivates young moms to seek vital healthcare treatments, it is imperative that these cultural aspects be addressed. 15
This study recommends more awareness campaigns and focused educational initiatives to educate teenagers about the maternal healthcare facilities that are accessible, in accordance with the suggestions made by Thomas et al. 3 Furthermore, establishing youth-friendly healthcare settings, as recommended by Erasmus et al., might lessen the discrimination and stigma faced by young moms. 4 Improving the quality of care requires educating medical professionals on how to treat teenage patients with compassion and dignity. 22
Last but not least, combining conventional methods with contemporary medical techniques may improve service acceptance and use. Mbizvo et al. noted that a more comprehensive approach to adolescent sexual and reproductive health may result from encouraging cooperation between traditional healers and medical professionals, as noted. 9 The implications of these findings are clear: interventions must be multi-level. At the structural level, reducing cost and distance barriers through subsidies and mobile clinics is crucial. At the service level, training providers in adolescent-friendly, non-judgemental care is essential. At the community level, programs are needed to combat stigma and engage families and traditional leaders in supporting adolescent mothers.
In conclusion, a comprehensive approach involving education, community involvement and systemic reforms is needed to solve the various obstacles that adolescents in Chiredzi area confront while trying to get maternal healthcare. Stakeholders can greatly enhance maternal health outcomes for young moms and help achieve the Sustainable Development Goals pertaining to gender equity and health by acknowledging and resolving these issues.
Limitations
While this study provides important insights, it had several limitations. The small sample size of 20 participants from a single hospital, while sufficient for thematic saturation, means the findings may not be representative of all adolescent mothers in Chiredzi district. The research primarily included urban and semi-urban perspectives, potentially overlooking the unique challenges faced by girls in remote rural areas. Although interviews were conducted in local languages, some cultural nuances may have been lost in translation. Additionally, participants might have withheld negative experiences due to lingering fear of judgement, despite the confidential setting. Finally, as the study focused on one district in Zimbabwe, the findings may not apply to other regions with different cultural or healthcare contexts. Future research should include a larger, more geographically diverse sample to enhance transferability. Despite these limitations, methodological rigour was pursued through the use of the COREQ checklist, member checking and reflexivity, and the research offers valuable guidance for improving maternal healthcare access for vulnerable adolescent populations.
Conclusion
This qualitative study reveals the multifaceted challenges faced by adolescent mothers in accessing maternal healthcare services in Chiredzi district, rooted in financial, logistical, cultural and emotional barriers. The findings suggest that addressing these challenges requires a multi-pronged strategy. This includes implementing targeted interventions such as improved healthcare delivery, regular mobile clinics to deliver tailored prenatal care services and the construction of health infrastructure in remote areas. Such measures are essential for promoting the health and well-being of adolescent mothers in hard-to-reach remote areas.
Supplemental Material
sj-docx-1-reh-10.1177_26334941251387213 – Supplemental material for Exploring the experiences and perceptions of adolescent mothers regarding maternal health services in Chiredzi district, Zimbabwe: a qualitative inquiry
Supplemental material, sj-docx-1-reh-10.1177_26334941251387213 for Exploring the experiences and perceptions of adolescent mothers regarding maternal health services in Chiredzi district, Zimbabwe: a qualitative inquiry by Gladmore Muchemwa and Methembe Yotamu Khozah in Therapeutic Advances in Reproductive Health
Footnotes
Acknowledgements
None.
Author’s note
GM is a Master’s student at the National University of Science and Technology in Zimbabwe. This manuscript is part of a partial research project, the fulfilment of the Master’s Degree in Environmental Health. MYK is an MSc Environmental Health holder at the National University of Science and Technology (NUST) in Zimbabwe. The author is also a lecturer at the Department of Environmental Health at NUST. This manuscript is part of a partial research project, the fulfilment of the Master’s Degree in Environmental Health.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.