
Abstract
Despite advocacy and recommendations to improve health care and health for persons who identify as women, women continue to face inequities in access to and quality of care. Person-centered care for women is one approach that could reduce gendered inequities. We conducted a series of studies to understand what constitutes person-centered care for women and how to achieve it. The overall aim of this article is to highlight the key findings of those studies that can inform policy, practice, and ongoing research. We conducted a narrative review of all studies related to person-centered care for women conducted in our group starting in 2018 over a 5-year period, which was general at the outset, and increasingly focused on racialized immigrant women who constitute a large proportion of the Canadian population. We organized study summaries by research phase: synthesis of person-centered care for women research, exploration of existing person-centered care for women guidance, consultation with key informants, consensus survey of key informants to prioritize strategies to achieve person-centered care for women, and consensus meeting with key informants to prioritize future research. We conducted the reported research in collaboration with an advisory group of diverse women and managers of community agencies. Our research revealed that little prior research had fully established what constitutes person-centered care for women, and in particular, how to achieve it. We also found little acknowledgment of person-centered care for women or strategies to support it in medical curriculum, clinical guidelines, or healthcare policies. We subsequently consulted women who differed by age, ethno-cultural group, health issue, education and geography, and clinicians of different specialties, who offered considerable insight on strategies to support person-centered care for women. Other diverse women, clinicians, healthcare managers, and researchers prioritized issues that warrant future research. We hope that by compiling a summary of our completed research, we draw attention to the need for person-centered care for women and motivate others to pursue it through policy, practice, and research.
Background
Many national and international agencies and initiatives have advocated for equitable access to high-quality care for persons who identify as women (henceforth, women). For example, the 1995 World Conference on Women of the United Nations, 1 and the 2009 World Health Organization report, Women and Health, 2 focused attention on the need to reduce healthcare disparities experienced by women. In 2002, the Johns Hopkins University Women’s and Children’s Health Policy Center led an initiative that issued recommendations for an increased focus on women’s health, and healthcare programs and services to address the unique needs of women beyond pregnancy alone. 3 In 2011, the Canadian Women’s Health Strategy consulted with women’s health experts, health system leaders, and over 200 women in Canada to issue recommendations for strategies needed to improve healthcare for women. 4 However, research shows that women continue to face structural determinants of health in social and healthcare systems, leading to disparities in access to and quality of care in both higher- and lower-income countries.5,6 Because of this, the United Nations prioritized women’s health as one of the 17 goals in the 2030 Agenda for Sustainable Development. 7 This priority aims to ensure that women access comprehensive healthcare that is responsive to gender and the life course.
Complex interacting factors contribute to the ongoing healthcare disparities faced by diverse women including but not necessarily limited to the disproportionate prevalence or severity of certain diseases or health issue, social determinants of health, and structural inequities in the healthcare system. For example, dementia is a disease that disproportionately affects women: two-thirds of persons aged above 65 years with dementia are women, and most caregivers of persons with dementia are wives or daughters.8,9 However, analysis of dementia strategies in 29 countries found that they did not address intersectional factors, such as gender or culture. 10 Compared to men, women are more likely to develop hand, knee, and hip osteoarthritis, and experience greater arthritis severity, pain, and disability. 11 Despite this, women are less likely to receive recommended osteoarthritis care, particularly racialized women of color with lower income or education.12,13
Women who had hypertensive disorders of pregnancy have a high risk of premature cardiovascular disease, particularly those with a first pregnancy at the age of 40 years or above or of certain visible minorities.14 –16 However, women have reported that physicians dismissed their queries about concerning symptoms, attributing them to stress or humid weather.17,18 It is also well-established that women are less likely to receive appropriately intensive medical therapy, lifestyle counseling, or cardiac rehabilitation compared with men, particularly women of visible minorities.19,20 Migrant women have far lower physical activity rates in comparison to immigrant men and non-immigrants. 21 Physical activity has been implicated as an important modifiable risk factor that can reduce the risk of developing cancer, cardiovascular disease, hypertension, type 2 diabetes, anxiety, depression, dementia, poor bone health, and overall mortality. 22 Determinants of low physical activity rates may include gender roles (self-care not prioritized over household/childcare responsibilities), culture (PA not typical or promoted), and socioeconomic (poverty, low-paying/multiple jobs) factors.23,24 Among more than 1.2 million women in Canada from 2014 to 2017, being an immigrant was a key determinant of missing breast, cervical, and colorectal cancer screening along with having no primary care provider. 25 Interviews in 2017 with 29 Canadian women from 15 different countries revealed many barriers of accessing healthcare services (e.g. language, no transportation, and child care) and dissatisfaction with communication from healthcare professionals. 26 Colonial structures have contributed to social, economic, and political disadvantages among Indigenous communities that also extend to health inequities, such as chronic illness and mental health crises, which, combined with systematic discrimination and lack of knowledge among healthcare systems and providers, has resulted in poor and sometimes traumatic healthcare experiences among Indigenous women. 27 This includes maternal health services in Canada and elsewhere.28,29 Sexually/gender-diverse persons who identify as women also face challenges in accessing the care they need. A 2019 survey of 2217 trans and non-binary Canadians found that 52% had a primary care provider with whom they were comfortable discussing trans health issues, and 44% reported an unmet healthcare need. 30 Trans women experience differences in health outcomes due in part to gender discrimination and poor provider education on the care of trans persons. 31 Furthermore, gender differences in health risks were amplified during the COVID-19 pandemic, with increased risk of negative health outcomes, reduced healthcare access, and poor mental health outcomes among diverse women. 32 For example, more women than men are front-line workers, such as nurses, who are directly responsible for patient care and thus susceptible to infection and unable to recover due to unpaid sick leave; due to home-based isolation, women were more often exposed to intimate partner violence; and women lacked access to pre-, peri- and post-natal care.
Further insight is needed to understand the policies, practices, and research that could enhance access to and quality of care for diverse women. Person-centered care (PCC) has long been established as an approach that can reduce inequities by tailoring care to an individual’s healthcare needs and personal preferences. 33 PCC was defined by the Institute of Medicine as a partnership between practitioners, patients, and their families to ensure that providers and systems deliver care that is attentive to the needs, values, and preferences of patients. 34 PCC has been demonstrated to improve patient healthcare experiences and health outcomes for numerous health issues relevant to primary, emergency, acute, and intensive care.35 –37 McCormack et al. employed rigorous methods involving patient and healthcare professional consultation to conceptualize PCC at the patient-provider interface, leading to comprehensive robust PCC framework comprising multiple approaches within six broad domains: foster a healing relationships, exchange information, recognize and respond to patient emotions, manage uncertainty, share decisions, and enable self-management. 38
Given well-documented disparities in women’s health and healthcare, we embarked on a series of studies to understand what constitutes person-centered care for women (PCCW) and how to achieve it. The overall aim of this article is to highlight the key findings of those studies that can inform policy, practice, and ongoing research. The specific objective is to describe the series of studies, briefly summarizing the results including recommendations for strategies to support PCCW and for future research on how to optimize PCCW.
Methodological process
Approach
We conducted a narrative review, sometimes labeled a perspective review, to summarize key findings of our completed research. While increasingly common, there are no standard methods for conducting narrative reviews. However, a narrative review is characterized by including studies selected because they address a broad aim, studies are conceptual and empirical in nature, there is no critical appraisal of study quality, and synthesis involves a narrative summary of study results. 39 We chose this approach because it allowed us to discuss the series of studies we conducted. By compiling the key findings, we generate a more holistic picture of the current landscape and share ideas that can inform policy, practice, and research to support and optimize PCCW. This differs from a meta-narrative review, which is a systematic type of review that includes studies of qualitative or mixed methods research design. 40 Because this was not a synthesis that involved systematic searching, screening, and data extraction, summary, and analysis, we did report findings according to criteria commonly used for such reviews. 41 While there are no reporting criteria for narrative reviews, we ensured that we addressed items included in the recently developed Scale for the Assessment of Narrative Review Articles. 42 As a narrative review of select, publicly available research, we did not require ethics approval.
Included studies
We included all studies related to PCCW conducted in our group starting in 2018 over a 5-year period. This included research based on a range of study designs, and involving diverse women and healthcare professionals. Initially, conceptual work broadly focused on women in general, and over time, we began to focus on ethno-culturally diverse women. We adopted this lens because the estimates suggest that, by 2036, nearly 50% of Canadians will be immigrants or their Canadian-born children, 43 and many other higher-income countries are facing unprecedented levels of migration. 44 Furthermore, racialized women are at higher risk of developing certain conditions and of experiencing healthcare inequities.12 –16,19 –21,23 –26 We purposefully did not pursue research involving Indigenous or sexually/gender-diverse persons who identify as women. While there is a need for PCCW in those communities,27 –31 such research requires partnership with community members, and knowledge of and experience with research approaches that are sensitive to Indigenous customs, which we did not possess. Furthermore, women are not homogeneous, so it is not appropriate or feasible to fully explore healthcare experiences, needs, and preferences across multiple groups. Instead, we aimed to include ethno-culturally diverse women of the immigrant groups most common in Canada. 43
Summary of studies
For each study, using a brief narrative, we described study design, included documents or participants, and key high-level results. We organized studies based on research phase: summary of published PCCW research, exploration of existing PCCW guidance, consultation with key informants to identify strategies need to achieve PCCW, consensus survey involving key informants to prioritize strategies to achieve PCCW, and consensus meeting with key informants to identify and prioritize future research. We also developed a figure to illustrate the progression of studies and included tables adapted from our published research on prioritized PCCW strategies and research topics.
Key informant engagement
While we did not involve diverse women or other key informants in the preparation of this article, we conducted the research described in collaboration with a 50-member advisory group of diverse women who volunteered time to help us with all aspects of the research including but not limited to reviewing eligibility criteria for reviews and interview guides for interviews or focus groups, refining the wording of strategies included in the Delphi survey, and taking part in the consensus meeting to generate research priorities. As the research progressed, we also formed partnerships with community agencies, such as immigrant settlement services or cultural groups, who helped us to recruit women or host focus groups.
Summary of PCCW research
Figure 1 illustrates the series of studies we conducted, which characterized gaps in knowledge, and in so doing, identified research needed in future to support PCCW. Broadly, we investigated (1) how PCCW has been conceptualized;45 –49 (2) existing and needed guidance on PCCW for healthcare systems and professions;50 –53 (3) recommendations from diverse women and clinicians on strategies to achieve PCCW;54 –56 (4) consensus among diverse women and healthcare professionals on strategies to achieve PCCW; 57 and (5) consensus among diverse women and healthcare professionals on future research needed to optimize PCCW. Following is a brief summary of our completed research that investigated PCCW (or concepts with synonymous terms).
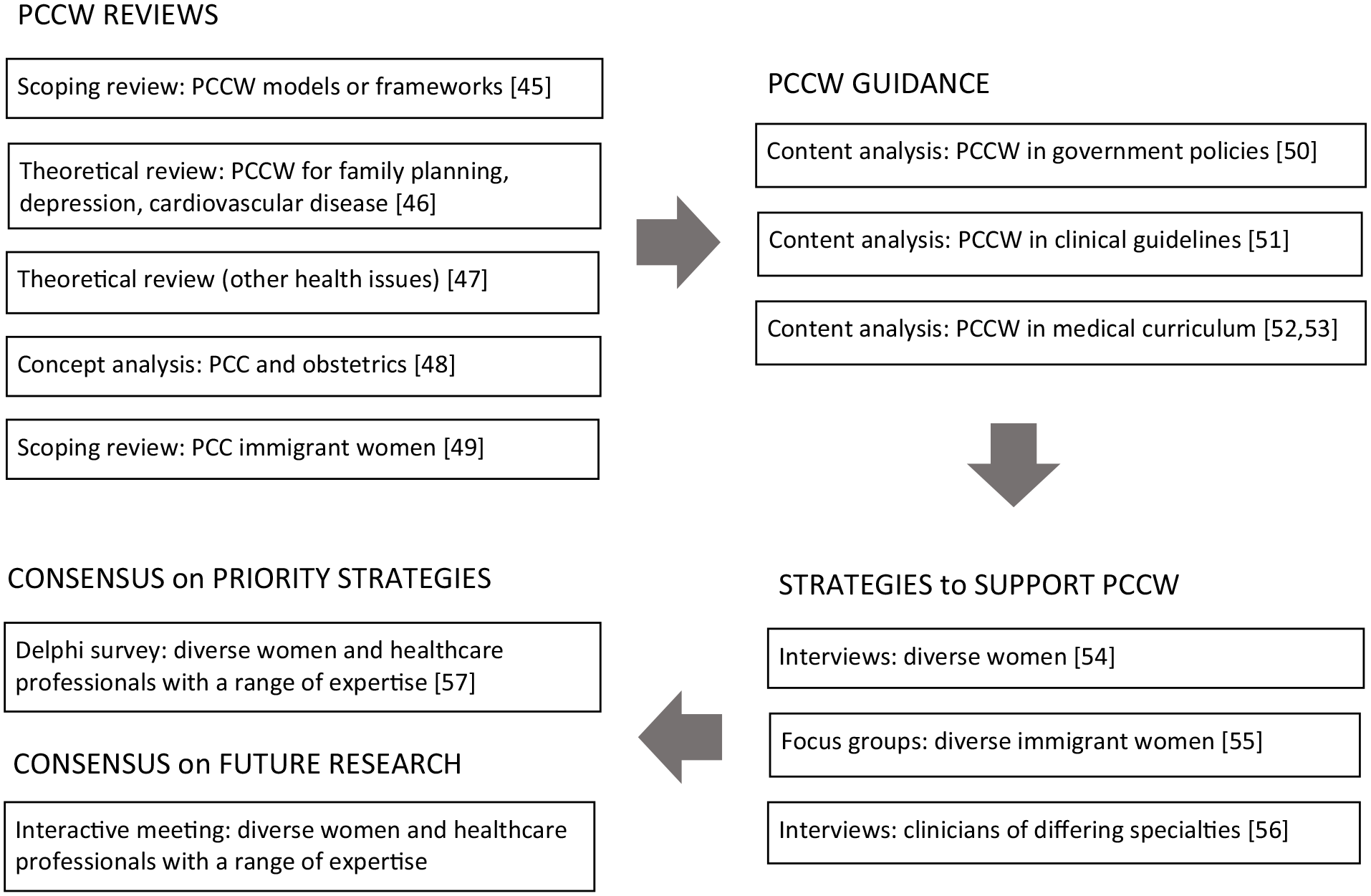
Series of studies that conceptualized PCCW and how to achieve it.
PCCW conceptualization
We performed several reviews to examine how PCCW was defined, assessed, or supported. First, to identify existing models or frameworks of PCCW, we conducted a scoping review that included 11 studies published from 2008 to 2018. 45 None were based on or generated a PCCW framework, included solely women, or analyzed or reported findings by gender. While all studies explored or described PCC components through qualitative research or surveys, none comprehensively examined PCC according to the existing framework rigorously developed by McCormack comprising multiple actions organized in six domains. 38
We then conducted a theoretical review of PCCW that included 14 studies published from 2008 to 2018 on family planning, depression and cardiovascular disease, conditions with proven inequities by gender, or other intersectional factors. 46 Apart from revealing a paucity of research, this review revealed inconsistency in how PCC was defined and operationalized. Seven studies found a positive association of PCCW with appropriate health service use, disease remission, health self-efficacy, and satisfaction with care, but none tested approaches or interventions to support PCCW
Next, we expanded the theoretical review of PCCW research, including 39 studies published from 2008 to 2018 on a range of clinical topics: maternal care, cancer, diabetes, HIV, endometriosis, dementia, distal radius fracture, overactive bladder, and lupus erythematosus. 47 Similar to the prior review, studies narrowly and inconsistently conceptualized or evaluated PCCW. Many studies identified barriers of PCCW; for example, racism and lack of training among clinicians; and language challenges and lack of confidence among women. A mere four studies tested strategies to support PCCW (e.g. nurse navigation for HIV, person-centered maternal care model), demonstrating beneficial impact on patient knowledge, satisfaction, well-being, self-care, and clinical outcomes.
Two additional reviews examined PCCW for specific populations. Given that labor and delivery is a common reason for hospitalization, we conducted a comparative concept analysis of PCC and high-quality obstetrical care to identify intersections. 48 We included 11 PCC and 9 obstetrical care concept analyses published from 2010 to 2021. Shared defining attributes included respect and dignity, informed decision-making, the therapeutic alliance, effective communication, coordinated continuity of care, social relationships, and empowerment and autonomy, suggesting the relevance of PCC to obstetrical care. Given high rates of migration and disparities in healthcare faced by migrant women, we conducted a scoping review of 16 studies published from 2010 to 2019 that assessed PCC for immigrants and refugees from 19 countries of origin. 49 Only five studies focused solely on women. PCC was not fully addressed, largely referring to exchange of information. Most studies reported barriers of PCC at the patient (e.g. language), clinician (e.g. lack of training), and organization/system level (e.g. lack of interpreters). No studies evaluated strategies or interventions aimed at either migrants or clinicians to improve PCC.
Overall, little prior research had fully established what constitutes PCCW, and in particular, how to achieve it.
PCCW guidance
We evaluated if and how healthcare professionals and systems are supported to provide PCCW. We analyzed the content of government policies published in Canada from 2010 to 2018 relevant to depression (n = 20) and cardiac rehabilitation (n = 10), conditions with known gendered inequities. 50 Among 30 included policies, few (7.23%) acknowledged healthcare disparities experienced by women, and even fewer offered guidance for PCCW, which was brief and vague; for example: “Women want care that is collaborative, woman- and family-centered, and culturally sensitive.”
Similarly, we analyzed the content of 27 Canadian and international clinical guidelines on depression (n = 18) or cardiac rehabilitation (n = 9). 51 About half (14, 52%) of the guidelines mentioned women, largely referring to social determinants of health, and none offered guidance on how to support or tailor care for disadvantaged women, including guidelines specific to women; for example, peri- or post-natal depression. Even when included, guidance was minimal; for example: “PCC should take into account patients’ needs and preferences,” with no further instruction of how.
We also reviewed the curriculum at 16 Canadian medical schools.52,53 Among 1459 documents analyzed, few (301, 21%) mentioned or described PCC or related concepts apart from foster a healing relationship (244, 79%) and even fewer (125, 9%) mentioned or addressed women’s health or related concepts apart from social determinants of health (88, 70%). Thus, medical students may not be exposed to PCCW concepts or approaches.
Overall, despite considerable evidence of the need to address gendered healthcare inequities,12 –16,19 –21,23 –26 and international recommendations to do so,1 –4,7 there is little acknowledgment of this in physician training, or in guidance subsequently used by clinicians and healthcare leaders to organize and deliver healthcare services.
Key informant recommendations for strategies to achieve PCCW
To address these gaps in knowledge, we next consulted with diverse women and clinicians to identify what constitutes PCCW and how to support it.
We interviewed 33 women aged 18–87 years who varied in healthcare issue, age, education, ethno-cultural group, and geographic setting within Canada, but articulated similar experiences. 54 Women commonly said that clinicians often dismissed their healthcare concerns. They recommended numerous strategies to support PCCW, 27 at the care interface (e.g. assume a nonjudgmental disposition, demonstrate active listening, elicit questions, acknowledge emotions, explore preferences for treatment, and offer self-care information) and 3 at the system level (e.g. education for women/girls and clinicians about PCCW, widespread access to women’s-only services or women clinicians). To ensure that we explored the perspectives of ethno-culturally diverse women, we conducted three focus groups with 23 immigrant women aged 25–78 years of different ethno-cultural groups from 10 countries of origin. 55 These women said that physicians rushed through discussions, and ignored or dismissed their concerns, and as a result, they no longer asked questions and sometimes avoided seeing a doctor, believing they would not get the help they needed. They recommended 28 physician behaviors to improve their healthcare experience that we mapped to McCormack’s six PCC domains. 38 In particular, they emphasized the domain of exchanging information, and associated actions they recommended included: listen to reason for visit, ask and welcome questions, provide detailed explanations, communicate clearly, ensure privacy, and provide information about prevention and screening.
We conducted qualitative interviews with 37 clinicians across seven specialties, such as family physicians, cardiologists, cardiac surgeons, obstetrician-gynecologist, psychiatrists, nurses, and social workers, who manage conditions that affect women across the life span. 56 Clinicians described 39 approaches they used to tailor PCC for women that we mapped to McCormack’s six PCC domains. 38 They identified additional ways to facilitate PCCW: ensure privacy, provide access to female clinicians, facilitate transport to health services, accommodate children, and offer flexible appointment formats and schedules. Clinicians also recommended medical training and continuing professional development in PCC and women’s health, and system-level enhancements, such as funding models for longer appointment times and multidisciplinary teamwork to enable and optimize PCCW.
Diverse women and clinicians of different specialties offered considerable insight on strategies that could enable PCCW.
Key informant priorities for strategies to support PCCW
We integrated the strategies recommended by diverse women and clinicians through aforementioned interviews,54 –56 which formed the basis of a two-round Delphi survey to generate consensus on the strategies that should be implemented to achieve PCCW. 57 Panelists included 21 women of varied age, ethno-cultural group, education, and urban/rural residence; and 21 healthcare professionals including clinicians of differing specialty, healthcare managers, and researchers with expertise in PCC or women’s health. Both groups agreed on 44 recommendations, of which 13 recommendations were prioritized by 100% of both women and healthcare professionals, organized by PCC domain: foster a healing relationship (n = 11), exchange information (n = 10), respond to emotions (n = 4), manage uncertainty (n = 5), share decisions (n = 8), and enable self-management (n = 6).
Table 1 summarizes the recommendations that represent the range of PCC domains, are based on evidence gathered from diverse women and clinicians in our primary research, and reflect high concordance between women and healthcare professional panelists. They can inform the development of policies, guidelines, programs, and performance measures that foster PCCW.
Recommendations for strategies to support PCCW by PCC domain. 57

PCC: person-centered care; PCCW: person-centered care for women.
Key informant priorities for research to support PCCW
On February 27, 2019, 40 key informants (17 diverse women, 23 healthcare professionals with a range of expertise) participated in a one-day meeting to review research accumulated to that date and offer recommendations for ongoing research based on small-group and full-group discussions. Women varied by age, ethno-cultural group, ability, gender identity, and health status; and healthcare professionals included family physicians, cardiologists, psychiatrists, a geriatrician, nurses, and a social worker, and researchers with expertise in women’s health or PCC, and representatives of government, research funding, charitable, academic, professional and advocacy organizations at the regional and national levels. Table 2 shows the full list of research recommendations. Top-ranked ongoing research priorities were as follows:
Explore how appointments or consultations could be structured and staffed to overcome time limitations and better address PCCW;
Assess how women could be empowered to voice questions and concerns during appointments or consultations in a way that is feasible given time limitations;
Interview women and clinicians about PCCW for a range of healthcare concerns to learn if and how PCCW differs by condition and stage in life span;
Examine how to implement the priority strategies recommended by diverse women and clinicians to enhance PCCW;
Implement and evaluate the approaches and strategies recommended to reduce gendered healthcare inequities;
Demonstrate a relationship between implemented PCCW strategies and healthcare outcomes;
Address the most vulnerable populations (e.g. lower socioeconomic status, racialized, immigrants, sexually/gender-diverse persons who identify as women).
Recommendations for research on how to achieve PCCW.

PCC: person-centered care; PCCW: person-centered care for women.
Discussion
We conducted a series of studies to describe PCCW, and how it is and could be better supported. We found little guidance for PCCW in prior research, policies, guidelines, or medical education curriculum, but diverse women and healthcare professionals with a range of expertise offered considerable insight on strategies that could enable PCCW, and prioritized strategies and topics that warrant ongoing research.
Similar to our study, prior research has commented on the lack of conceptualization of women’s health, acknowledging the challenge of doing so due to the complexity of intersectional factors, such as race, class, sexuality, and disability, that affect access to and quality of healthcare for women, and ultimately, women’s health.58,59 Because of this complexity, other efforts focused on particular types of health issues or populations. For example, the US National Institutes of Health developed a framework that itemizes chronic debilitating conditions in women to inform further strategic planning of health services for women. 60 Focus groups in Malawi explored women’s perspectives on the quality of maternal care as a way of understanding how to improve services. 61 Another narrative review discussed health disparities among Black women in the United States and contributing socioeconomic factors. 62 None of these initiatives generated action items needed to improve women’s access to and quality of care as we did via the series of studies summarized in this article. However, this appears to be changing. Other research reviewed evidence on strategies to improve quality of care among women for specific conditions. For example, analysis of interventions used to improve maternal and newborn health identified some successful community-oriented approaches (e.g. community mobilization, women’s support groups, community health workers, and traditional birth attendants) but limited research on multi-level strategies, and as a result, the authors issue several recommendations for research (e.g. evaluate more interventions, used mixed methods approaches). 63 In Australia, the Department of Health issued a national women’s health strategy that included high-level system (e.g. increase access to information, diagnosis, treatment and services for sexual and reproductive health) and public health (e.g. enhance gender-specific mental health awareness) goals toward improving healthcare and health for all women. 64 In contrast, our work generated insight on multi-level (patient, clinician, organization, and system) strategies that could be implemented to support PCCW.
Compilation of the results of our accumulated research gives rise to several implications for policy and practice. For instance, we found very little acknowledgment of or guidance for PCCW in policies issued by government as the blueprint for healthcare organization and delivery, clinical guidelines used by practicing clinicians to inform care delivery, or curriculum for physician training.50 –53 While exemplar curriculum and other resources are available to assist medical schools in enhancing the PCCW content of their curriculum,65,66 it may be difficult to convince medical schools to add additional content to already-full curriculum, thus further research is needed to consult with medical students, deans of medical schools, and practicing physicians on how to expose medical students to PCCW concepts. With respect to guidelines, development methods are already evolving to incorporate patient perspectives, often by including patients or family on guideline development panels so that the guideline recommendations reflect patient needs and preferences.67,68 Our research found that PCCW was more likely to be addressed in guidelines when patients were included as panel members. 51 However, to address diverse needs and preferences requires that developers include persons with a wide range of attributes on the development panel, something that developers have noted is a challenge. 69 Policies are entirely another matter, as policymakers consider many factors when formulating policy. Tools are available that policymakers can use to assess if policies support gender equity, 70 but prior research found that considerable efforts are needed to influence the issues that policymakers consider, with no guarantee that the ultimate policy will reflect those issues. 71 Further research is needed for insight on how to ensure that policies consider PCCW, along with other structural determinants of health and well-being, perhaps by identifying exemplar policies, and working backward to consult with those that developed the policy to understand their motivations and processes. The diverse women, clinicians, and healthcare professionals we consulted recommended and prioritized numerous strategies to support PCCW that are not necessarily reliant on system-level policy changes. Many of the strategies can be enacted by individual clinicians at the point-of-care necessitating a dissemination campaign that could include continuing professional development at conferences and endorsement by professional societies.
With respect to research, our prior studies identified numerous issues that warrant future investigation, and diverse women and healthcare professionals prioritized several of those topics. For example, assess how to empower women to self-advocate during healthcare interactions, and explore what constitutes PCCW and how to achieve it for different clinical issues across the life span, and in particular, among the most vulnerable populations, such as Indigenous women and sexually/gender-diverse persons who identify as women. However, additional gaps in knowledge emerged by reflecting on the accumulated research summarized in this article. For example, gendered healthcare inequities have been recognized as a problem at least the 1995 World Conference on Women of the United Nations, 1 if not before, so why do these inequities continue to exist? Given the paucity of research on PCCW revealed by our studies, why are healthcare research funders not prioritizing funds for women’s health research?
This article features several strengths. It is based on an accumulation of empirical research that was conducted and reported based on rigorous methods and standards. All of our referenced publications are available through open access. Some limitations must also be noted. First and foremost, this narrative review includes only our research, thus it does not address the wide range of factors contributing to gendered healthcare inequities, populations of persons who identify as women and differ in many ways by intersectional factors, or strategies needed to support PCCW. Also, our research involving key informants was conducted in Canada and the results may not be relevant to women, clinicians, or healthcare systems in other jurisdictions. However, we hope that by compiling a summary of our completed research, we draw attention to the need for PCCW and motivate others to pursue it through policy, practice, and research.
Conclusion
Our research revealed that further research is needed to generate insight and guidance on how to feasibly incorporate PCCW concepts in policies, guidelines, and medical training and continuing education. Women research advisors and research participants, including women and healthcare professionals, also recommended research on how to empower women to self-advocate during healthcare interactions; and to explore what constitutes PCCW and how to achieve it for different clinical issues across the life span, and in particular, among the most vulnerable populations, such as Indigenous women and sexually/gender-diverse persons who identify as women. To enable ongoing research, sources of healthcare research funding must prioritize competitions or funds for women’s health research.