
Abstract
Background:
Postpartum depression is a public health issue affecting both maternal well-being and child development. While it is the most common mental health disorder following childbirth, data on its prevalence and associated risk factors in developing countries, including Ghana, remains limited.
Objectives:
This study determined the prevalence of postpartum depression and identified its associated risk factors among pregnant women who developed hypertensive disorders of pregnancy at the Adabraka Polyclinic in the Greater Accra Region of Ghana.
Design:
This study was a hospital-based cross-sectional study.
Methods:
This hospital-based cross-sectional study was conducted on 159 postnatal mothers who delivered between March 31, 2023 and May 31, 2023 at the Adabraka Polyclinic in the Greater Accra Region of Ghana. Participants were selected using purposive sampling. The data collection instrument were developed to gather information on sociodemographic, psychosocial, obstetric, and newborn characteristics. The Edinburgh Postnatal Depression Scale was used to investigate depressive symptoms in the mothers. Mothers with Edinburgh Postnatal Depression Scale scores above 12 or 13 were considered likely to be experiencing depression.
Results:
Out of the 159 women followed to term, 74 were diagnosed with postpartum depression (Edinburgh Postnatal Depression Scale scores above 12 or 13), indicating a prevalence rate of 46.5%. The majority of these women were aged between 25 and 30 years (46.5%), engaged in informal occupations (52.2%), had multiple children (71.1%), pregnancies (69.2%), and normal blood pressure levels (62.3%). After adjusting for potential confounders in a multivariate logistic model, several factors were found to be independently associated with postpartum depression: informal occupation (adjusted odd ratio = 0.12, 95% confidence interval (0.02–0.62), p = 0.012), Ga ethnicity (adjusted odd ratio = 5.27, 95% confidence interval (1.25–22.11), p = 0.023), sub-optimal financial support from partner (adjusted odd ratio = 27.54, 95% confidence interval (4.63–164.00), p < 0.001), and experience of cesarean section (adjusted odd ratio = 22.10, 95% confidence interval (3.90–125.08), p < 0.001).
Conclusion:
Pregnant women with hypertensive disorders may face a heightened risk of experiencing postpartum depression. Timely recognition and intervention are vital for enhancing the health and welfare of both mothers and their children.
Introduction
Hypertensive disorders of pregnancy (HDP), including preeclampsia and chronic hypertension, are significant global causes of maternal and fetal morbidity and mortality. 1 Each year, HDP collectively result in ~30,000 maternal deaths and 500,000 perinatal deaths globally, making them the primary cause of maternal and neonatal morbidity and mortality worldwide. 2 HDP affect 3%–10% of pregnancies globally. 3 Recent estimates show that maternal causes are the leading global cause of death among women aged 15–49, with sub-Saharan Africa bearing the brunt of these fatalities. 4 Globally, 260 women die from every 100,000 live births, with sub-Saharan Africa accounting for the majority of these deaths. 5 Despite efforts made worldwide to improve maternal health, maternal mortality remains a serious public health issue, particularly in low-income nations such as Ghana 4 where it occurs three to four times more frequently than in high-income countries. 6 HDP include preeclampsia, gestational hypertension, chronic hypertension, and preeclampsia superimposed on chronic hypertension. 7
The severity of HDP, in combination with other perinatal factors like prematurity, newborn hospitalization in the neonatal intensive care unit, and fetal death, may also increase the risk of mothers developing postpartum depression (PPD) or anxiety. 8 Due to the stress and challenges associated with HDP, mothers are more prone to developing PPD, which in turn may worsen the negative health consequences of these disorders. This combined burden can lead to adverse effects on the postnatal mother, such as difficulties with mother–infant bonding, breastfeeding challenges, and a decline in the mother’s overall well-being.8 –10 PPD is the most frequent psychological ailment following childbirth and can be detrimental to the social and cognitive development of mothers, partners, newborns, and children, particularly in areas like emotional regulation, communication skills, and parent–child bonding. 11 The incidence of PPD varies across and within countries, with rates being highest in regions with greater income disparity, maternal mortality, or infant mortality. 12
Although the precise causes of PPD are unknown, it likely results from a complex interaction of physical, emotional, genetic, and social factors, such as lack of social support or financial strain. 13 This limited understanding of the link between HDP and PPD makes it challenging to develop effective treatments. 12 PPD typically begins within 1–4 weeks after delivery. 14 While the core symptoms of sadness, hopelessness, and fatigue are common to both PPD and other forms of depression, 15 some research suggests that PPD can also manifest through experiences unique to childbirth and motherhood, such as anxieties about infant care or difficulty bonding with the baby. 16 Untreated PPD can have significant long-term consequences, potentially leading to chronic or recurring depression in mothers, and negatively impacting children’s cognitive, emotional, and social development.17,18 Despite the lack of definitive knowledge regarding the link between HDP and PPD, 19 research suggests that women diagnosed with HDP might experience PPD more frequently than those without HDP. 19 Understanding the prevalence and associated risk factors of depression symptoms following HDP is crucial for improving postpartum care for women at risk. Therefore, this study aimed to determine the prevalence and associated risk factors of PPD among pregnant women who developed HDP.
Materials and methods
Study design and setting
This study employed a cross-sectional design to estimate the prevalence and factors associated with PPD among postnatal mothers who developed hypertensive disorders during gestation at the Adabraka Polyclinic, Accra-Adabraka between March 31, 2023 and May 31, 2023.
Survey instruments
Data collection involved face-to-face interviews using a structured questionnaire with pregnant women who developed hypertensive disorders during gestation. The questionnaire covered demographics, psychosocial characteristics, 20 pregnancy-related and newborn characteristics, 8 and measures based on the Edinburgh Postnatal Depression Scale (EPDS). 21 The principal investigator and trained assistant conducted the interviews. The questionnaire was written in English but was carefully translated into the local language to ensure clarity. It was pretested with 10 pregnant women who developed hypertensive disorders during gestation. Problems identified from the pretesting phase were corrected and the final draft was prepared for collection of data. The interviewer administered the questionnaires during the study period. All survey instruments can be found as the Supplemental Material.
Study population and participant selection
The study recruited 159 postnatal mothers who had developed HDP (including gestational hypertension, preeclampsia, chronic hypertension, and superimposed preeclampsia) between 4 and 12 weeks postpartum. The sample size was estimated using Charan and Biswas,
22
formula, thus; N =
Ethical approval
The study was approved by the Committee for Human Research, Publication, and Ethics (CHRPE/AP/632/23) of the School of Medicine and Dentistry (SMD), Kwame Nkrumah University of Science and Technology (KNUST). Additionally, approval was obtained from the authorities of Adabraka Polyclinic. Written informed consent was obtained from all prospective participants. In instances where participants were unable to provide consent themselves, their legally authorized representatives or literate guardians were approached for consent. The purpose of the study was explained to all participants, and written consent was obtained. The study adhered to the core principles outlined in the Declaration of Helsinki and its latter amendments.
Inclusion and exclusion criteria
This study included postnatal mothers (4–12 weeks postpartum) who had developed HDP (including gestational hypertension, preeclampsia, chronic hypertension, and superimposed preeclampsia). HDP is characterized by a systolic blood pressure of 140 mm Hg or higher and/or a diastolic blood pressure of 90 mm Hg or higher occurring after 20 weeks of pregnancy. Pregnant women and postnatal mothers without HDP were excluded from the study.
Data collection
A questionnaire was designed specifically to investigate the prevalence of PPD at 1–3 months postpartum among women who developed HDP during gestation. The questionnaire had five sections: sociodemographic section, pregnancy- and birth-related section, newborn characteristics section, psychosocial and psychological history, and EPDS, 21 which was used to screen mothers for postnatal depressive symptoms indicative of PPD. The reporting of this study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines for cross-sectional studies. 25
Statistical analyses
Data entry was done using Microsoft Excel 2016, and analysis was performed using SPSS version 26.0 (IBM SPSS Statistics for Windows,Version 26.0 Armonk,NY:IBM Corp.) and GraphPad Prism 8.0.1 (GraphPad Software Inc). Descriptive statistics were used to examine the distribution of the study variables. Categorical variables were presented as frequencies (N) and percentages (%). The association between various sociodemographic, psychosocial, and obstetric characteristics and mothers’ EPDS categories was examined using the chi-square test and logistic regression models, respectively. Significant variables identified through the chi-square test were incorporated into the univariate model to evaluate their independent associations with PPD. The forward addition method was employed, iteratively removing non-significant variables until only statistically significant predictors remained, ensuring a more concise and interpretable model. The significant predictors identified through the forward addition method were then combined into a multivariate model to assess their combined effect on PPD. A p < 0.05 was considered statistically significant.
Results
Sociodemographic and obstetric characteristics of study participants
Table 1 shows that out of the 159 mothers with a history of hypertensive disorders, majority were aged 25–30 years (n = 74, 46.5%). Most of the women (n = 88, 55.3%) had received secondary education while a few (n = 34, 21.4%) had assessed tertiary education. The majority of women (n = 8, 52.2%) worked in the informal sector while a few (n = 34, 21.4%) were unemployed. Akans (n = 85, 53.5%) were the largest ethnic group. Majority of the women were married (n = 94, 59.1%). Most of them were multiparous (n = 113, 71.1%). More than half (n = 110, 69.2%) were multigravida, whereas 18 (11.3%) were primigravida. Normotensives had the largest proportion (n = 99, 62.3%), whereas 60 (37.7%) of them were hypertensives.
Sociodemographic and obstetric characteristics of the study participants.

IQR: interquartile range.
Data are presented as frequency (N) and percentage (%).
Prevalence of PPD amongst postnatal mothers
Figure 1 shows the distribution of postnatal mothers based on their PPD status. The prevalence of PPD among the study participants was 46.5%.

Prevalence of postpartum depression among the study participants.
Association of sociodemographic characteristics with PPD among study participants
Table 2 demonstrates the association of sociodemographic characteristics with PPD among study participants. There were no significant association between participants age category (p = 0.607), level of education (p = 0.817), and PPD. However, there were significant associations between occupation (p = 0.006), ethnic group (p = 0.024), marital status (p = 0.023), and PPD.
Association of sociodemographic characteristics with PPD among study participants.

NPPD: no postpartum depression; PPD: postpartum depression.
Data are presented as frequency (%); chi square/Fisher’s exact test, p < 0.05 was considered statistically significant for women with PPD and NPPD.
Association of psychosocial characteristics with PPD among study participants
Table 3 shows the association of psychosocial characteristics with PPD among study participants. No significant association was found between financial support from family (p = 0.170) and PPD. Those receiving financial support from partners had significantly lower rates of PPD compared to those without support (p < 0.001). Participants experiencing stressful life events were more likely to have PPD compared to those without such experiences (p = 0.002). Moreover, planned pregnancies were associated with lower rates of PPD compared to unplanned pregnancies (p = 0.004).
Association of psychosocial characteristics with PPD among study participants.

NPPD: no postpartum depression; PPD: postpartum depression.
Data are presented as frequency (%); chi square/Fisher’s exact test, p < 0.05 was considered statistically significant for women with PPD and NPPD.
Association of obstetric/fetal characteristics and maternal complications with PPD among study participants
Table 4 shows the association of obstetric/fetal characteristics and maternal complications with PPD among study participants. The study found no significant association between birth weight category (p = 0.206), gestational age category (p = 0.082), parity (p = 0.862), and gravidity (p = 0.424) with PPD. However, the mode of delivery showed a significant association with PPD (p = 0.002). Participants who underwent a cesarean section (CS) were more likely to experience PPD compared to those who had a normal delivery. The diagnosis categories, both specific and general, also demonstrated significant associations with PPD (p < 0.001). Specifically, participants diagnosed with gestational hypertension, preeclampsia, chronic hypertension, or HDP were more likely to experience PPD compared to those with normotension.
Association of obstetric, fetal characteristics, and maternal complications with PPD among study participants.
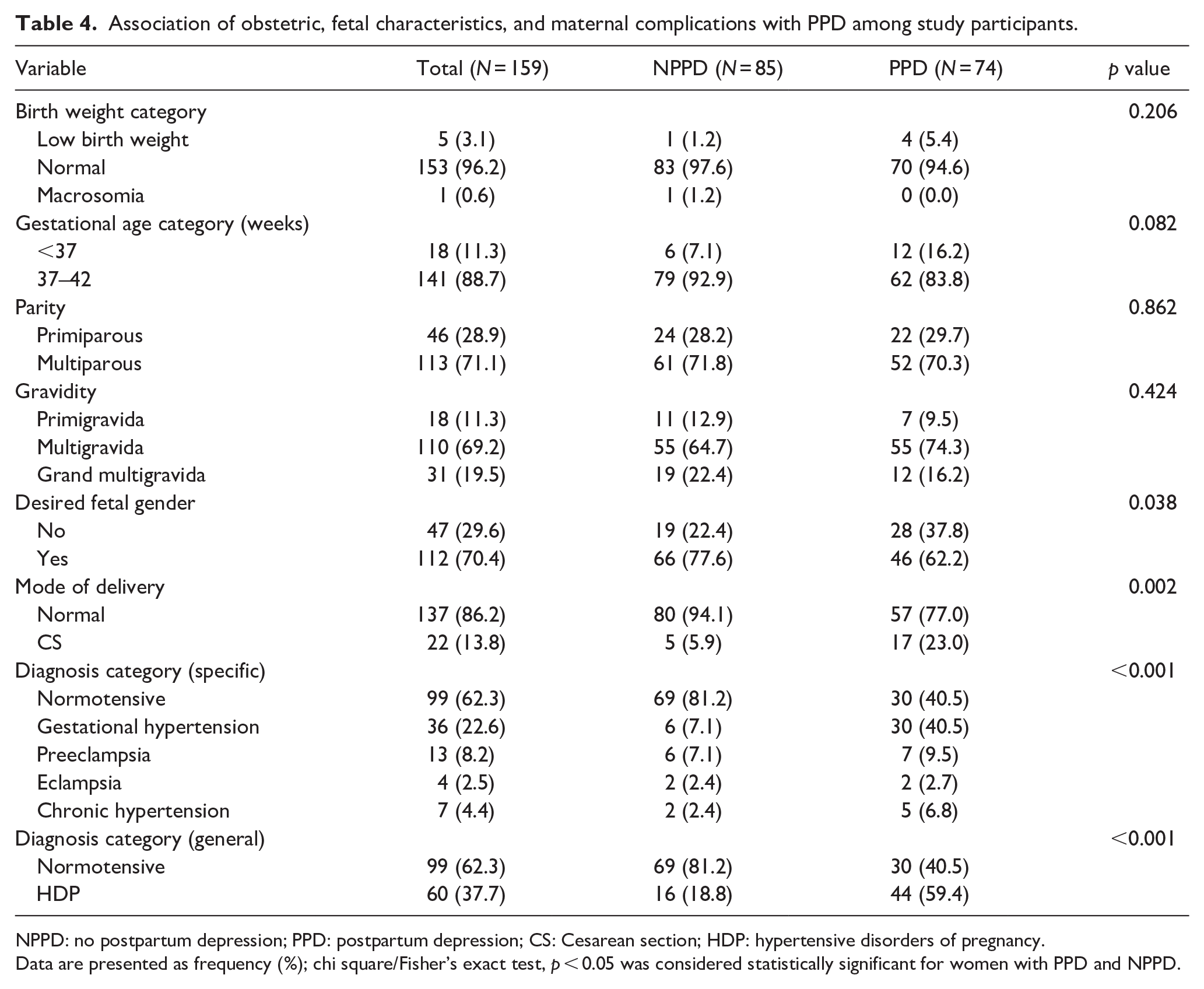
NPPD: no postpartum depression; PPD: postpartum depression; CS: Cesarean section; HDP: hypertensive disorders of pregnancy.
Data are presented as frequency (%); chi square/Fisher’s exact test, p < 0.05 was considered statistically significant for women with PPD and NPPD.
Sociodemographic characteristics as predictors of PPD among study participants
In a univariate logistic regression model, occupation, ethnic group, and marital status were predictors of PPD. Specifically, postnatal women in the informal sector (crude odds ratio (cOR) = 0.44, 95% CI (0.21–0.95), p = 0.035) had 56% lower odds of developing PPD when compared with postpartum women in the formal sector. Postnatal Ga mothers (cOR = 3.50, 95% CI (1.41–8.66), p = 0.007) had 3.5 times increased odds of developing PPD compared to Akan mothers. Also, mothers who were cohabiting (cOR = 3.08, 95% CI (1.33–7.12), p = 0.009) were significantly associated with 3.1 times increased odds of having PPD compared to those who were married. After adjusting for maternal age and level of education in multivariate logistic regression model, having an informal occupation (adjusted odd ratio (aOR) = 0.12, 95% CI (0.02–0.62), p = 0.012), and being in the Ga ethnic group (aOR = 5.27, 95% CI (1.25–22.11), p = 0.023) were the independent sociodemographic characteristics of PPD (Table 5).
Univariate and multivariate logistic regression model of sociodemographic factors as predictors of postpartum depression among study participants.

cOR: crude odd ratio; CI: confidence interval; aOR: adjusted odd ratio; 1.00: reference.
Data are presented as odd ratio (95% CI). Variables included in the multivariate model for adjustment were age, level of education, occupation, ethnic group, and marital status. Binary logistic regression analysis performed to obtain odd ratios. p < 0.05 was considered statistically significant.
Psychosocial characteristics as predictors of PPD among study participants
Table 6 shows psychosocial characteristics as predictors of PPD among study participants. In a univariate logistic model, financial support from partner, stressful life activity, planned pregnancy, and desired fetal gender were predictors of PPD. Specifically, postpartum mothers who did not receive financial support from their partners (cOR = 13.05, 95% CI (4.31–39.48), p < 0.001) were significantly associated with 13.05 times increased odds of developing PPD compared to those who received financial support from partners. Mothers who had stressful life activities (cOR = 3.03, 95% CI (1.49–6.17), p = 0.002) were significantly associated with 3 times higher odds of developing PPD compared with those who had no stressful life activity. Also, postpartum mothers who did not plan their pregnancies (cOR = 2.57, 95% CI (1.35–4.88), p = 0.004) were significantly associated with 2.6 times increased odds of developing PPD compared to those who had planned their pregnancy. Postpartum mothers who did not get their desired fetal gender (cOR = 2.11, 95% CI (1.06–4.23), p = 0.034) were significantly associated with 2.1 times increased odds of PPD compared to those who had their desired fetal gender. After adjusting for maternal age and level of education in multivariate logistic regression model, no financial support from partner (aOR = 27.54, 95% CI (4.63–164.00), p < 0.0001) was the independent psychosocial characteristic of PPD.
Univariate and multivariate logistic regression model of psychosocial characteristics as predictors of postpartum depression among study participants.
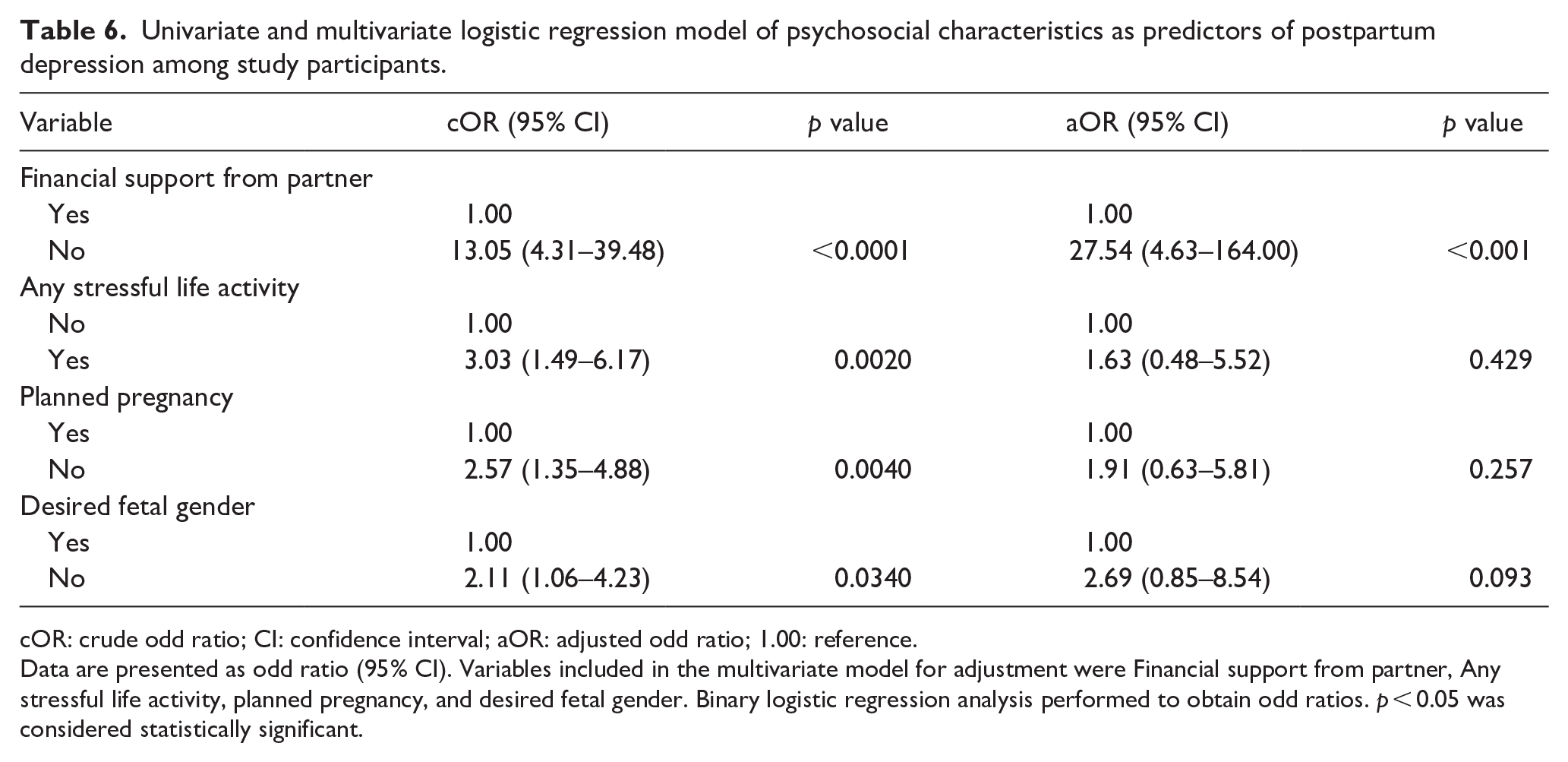
cOR: crude odd ratio; CI: confidence interval; aOR: adjusted odd ratio; 1.00: reference.
Data are presented as odd ratio (95% CI). Variables included in the multivariate model for adjustment were Financial support from partner, Any stressful life activity, planned pregnancy, and desired fetal gender. Binary logistic regression analysis performed to obtain odd ratios. p < 0.05 was considered statistically significant.
Obstetric characteristics and maternal complication as predictors of PPD among study participants
Table 7 shows obstetric characteristics and maternal complication as predictors of PPD among study participants. In a univariate logistic model, mode of delivery and diagnosis (complication) were predictors of PPD. CS (cOR = 4.77, 95% CI (1.66–13.68), p = 0.004) was significantly associated with 4.8 times increased odds of developing PPD compared with normal delivery. Moreover, all the HDP (cOR = 6.33, 95% CI (3.09–12.93), p < 0.0001) were significantly associated with 6.3 times increased odds of having PPD compared with normotensives. After adjusting for maternal age and level of education in multivariate logistic regression model, having CS (aOR = 22.10, 95% CI (3.90–125.08), p < 0.0001) was the independent obstetric and maternal complication of PPD.
Univariate and multivariate logistic regression model of obstetric characteristics and maternal complication as predictors of postpartum depression among study participants.

cOR: crude odd ratio; CI: confidence interval; aOR: adjusted odd ratio; 1.00: reference.
Data are presented as odd ratio (95% CI). Variables included in the multivariate model for adjustment were Mode of delivery and diagnosis. Binary logistic regression analysis performed to obtain odd ratios. p < 0.05 was considered statistically significant.
Discussion
The global prevalence of PPD ranges from 4% to 25%. 12 It is found to be 25% more prevalent in low- and middle-income nations than in developed countries. 26 Evidence suggests that PPD for women and their children may be more common and serious in low-income countries although mental health is frequently not prioritized as a problem in these settings. 27
To the best of our knowledge, this study is the first in Ghana to investigate the prevalence of PPD among women with recent history of pregnancy-related hypertensive disorders . Our findings reveal a significantly high prevalence of PPD at 46.5% in this population. While the scarcity of data on PPD specifically among hypertensive mothers limits direct comparisons, the prevalence reported in this study is markedly higher than rates observed among postpartum mothers in general. For instance, the prevalence in our study surpasses the rates reported by Anokye et al. 23 (7%) in Kumasi, Cadri et al. 28 (32.6%) in Hohoe, Saeed and Wemakor 29 (16.8%) in Bole District, and Buabeng 30 (22.3%) in Kumasi. Similarly, our study’s prevalence surpasses rates reported in Nigeria (22.9%), 31 and Ethiopia (33.82%), 32 while prevalence in Bahrain (37.1%), 33 Saudi Arabia (38.5%), 34 and Brazil (10.8%) 35 were higher than that of our study. The increased prevalence in our study may be attributed to psychological and social factors, as noted by Yim et al. 36 and Liang et al. 37 in developing countries. Moreover, factors such as poverty, lack of social support, experiences of partner violence, a history of pregnancy loss, and unintended pregnancies have been found to be associated with PPD. 37 These findings underscore the need for targeted interventions and support systems to address the psychological well-being of postpartum women, particularly in resource-constrained settings.
In this study, informal occupation was independently associated with PPD. Thus, postpartum mothers with informal occupation had risk of PPD than postpartum mothers who had formal occupation. Experiencing job insecurity is believed to elevate the risk of depression in postpartum mothers with informal occupation. 38 Mothers who undergo childbirth may find it challenging to control this situation and are more likely to experience PPD. It was also found in this study that the Ga ethnic postpartum mothers had increased risk of PPD. The findings found in this study could be as a result of e low socioeconomic living conditions among the Ga ethnic postpartum mothers.
In this study, we found that having no financial support from partners was independently associated with PPD. Thus, postpartum mothers who had no financial support from their partners had increased risk of PPD than those who had financial support from their partners. Overall findings from this study are in line with studies done in Saudi Arabia, 34 Brazil, 35 Egypt, 39 Ghana, 40 and Bahrain 33 which showed that not receiving financial support from partner have emotional, social and mental trauma on mothers, thereby increasing their risk of PPD. However, studies by Ayoub 41 in Palestine and Almuqbil et al. 42 in Saudi Arabia found no association between having no support from partner and PPD. The differences in findings could be due to the differences in the socioeconomic living conditions of the postpartum mothers in these settings.
To improve the quality of life for both mothers and newborns, male spouse or partners should financially support their female partners during pregnancy and also after childbirth.
Our study findings showed that undergoing a CS was independently associated with PPD. Thus, postpartum women who had undergone CS had increased risk of PPD than having normal vaginal delivery. Although the exact mechanism is not known, it is reported CS has adverse effects on psychosocial outcomes, especially concerning post-traumatic stress disorder which could lead to PPD. 43 Findings of this study is comparable to a study conducted by Al Nasr et al. 34 in Saudi Arabia and Benton et al. 43 in China which also found a significant association between having undergone CS and PPD. This finding could be as a result of the physical trauma postpartum mothers go through after childbirth which may have an effect on their psychological well-being.
Limitations
This study had several limitations that should be considered when interpreting the findings. First, data on body mass index and physical activity levels were not collected. Since both factors could have influenced HDP and PPD, their omission may have introduced potential confounding effects. Future studies should account for these variables to improve the accuracy of findings. Second, the study did not include important mental health-related factors such as bipolar disorder, recent use of antidepressants, substance abuse, or lifetime treatment for depression. The exclusion of these variables may have limited a comprehensive understanding of PPD within the study population. Third, the reliance on self-reported questionnaires introduced the possibility of reporting bias or misinterpretation of questions, which may have affected response accuracy. Self-reported data were inherently subjective and could have been influenced by recall bias, stigma, or misunderstanding of survey items. Another major limitation was the cross-sectional design of the study, which prevented the establishment of causal relationships between HDP and PPD. Future research should consider longitudinal approaches to better assess the direction and strength of these associations.
Finally, the study sample was limited to a specific geographic region, which may have restricted the generalizability of the findings. Expanding data collection to multiple districts, municipalities, and metropolitan areas in future research would provide a broader and more representative perspective on PPD prevalence and its associated risk factors.
Conclusion
Pregnant women with hypertensive disorders may have an increased risk for PPD. Early identification and treatment of PPD are crucial for improving the health and well-being of both mothers and their children. We recommend that hospital authorities, in collaboration with the Ministry of Health and Ghana Health Service, partner with non-governmental organizations to implement routine screening programs for PPD. Additionally, the Ministry of Health through the Ghana Health Service should implement public education initiatives focused on raising awareness about PPD. These efforts are essential for early detection, support, and intervention to mitigate the impact of PPD on maternal and child well-being.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251338938 – Supplemental material for Prevalence and risk factors of postpartum depression among postnatal mothers with hypertensive disorders of pregnancy in a developing country
Supplemental material, sj-docx-1-whe-10.1177_17455057251338938 for Prevalence and risk factors of postpartum depression among postnatal mothers with hypertensive disorders of pregnancy in a developing country by Wina Ivy Ofori Boadu, Enoch Odame Anto, Edmund Mintah Wiafe, Michael Nyantakyi, Joseph Frimpong, Emmanuel Ekow Korsah, Ezekiel Ansah, Afia Agyapomaa Kwayie, Elizabeth Aboagye, Christian Obirikorang, Emmanuel Timmy Donkoh and Kwame Ofori Boadu in Women’s Health
Footnotes
Acknowledgements
The author’s express their gratitude to Mrs. Esther Opoku, the labor in-charge, along with all the midwives and laboratory staff at the Adabraka Polyclinic, for their invaluable support and guidance throughout this study.
Ethical considerations
The study was approved by the Human Research, Publication, and Ethics (CHRPE/AP/632/23) of the School of Medicine and Dentistry (SMD), Kwame Nkrumah University of Science and Technology (KNUST). Additionally, approval was obtained from the authorities of Adabraka Polyclinic.
Consent to participate
Written informed consent was obtained from all prospective participants. In instances where participants were unable to provide consent themselves, their legally authorized representatives or literate guardians were approached for consent.
Consent for publication
Informed consent for publication was provided by the participants.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data and materials generated and analyzed during this study are included in the article and can be requested from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.