
Abstract
Background:
In the United States, only 15% of women with postpartum behavioral health (BH) conditions receive timely treatment. Peer support, an evidence-based strategy deploying nonclinical individuals with lived experience to provide support, may improve postpartum BH service delivery and can serve as a critical linkage for individuals who lose care access through prenatal structures. Yet, implementation barriers have hindered integration and scaling of postpartum peer support. We conducted a scoping review to synthesize implementation strategies for postpartum peer support interventions.
Methods:
Eleven interventions were identified through comprehensive searches of four databases. The study analysis identified contextual factors and implementation outcomes according to the Practical, Robust Implementation and Sustainability Model framework.
Results:
Successful programs incorporated flexible delivery formats, consistent supervision, and structured peer training to support fidelity while accommodating participant needs. Feasibility and acceptability were high among both participants and peer supporters; however, reach remained limited by exclusion of non-English-speaking individuals and those without technology access. Implementation was further influenced by local public health infrastructure, availability of clinical supervision, and societal norms. Sustainability challenges, including cost and integration within existing health systems, were common.
Conclusions:
While peer support interventions may improve postpartum depressive symptoms, their reach to vulnerable populations and sustainability are limited. Further work is needed to strengthen the implementation of peer support interventions in limited-resource communities and non-English-speaking populations. Tailored strategies include adaptation of intervention components to local contexts, enhancing supervision of peer supporters, and identification of sustainable models for integration within existing systems.
Introduction
Behavioral health (BH) conditions are the leading cause of maternal mortality in the United States,1,2 but national initiatives to resolve the U.S. maternal morbidity and mortality crisis often fail to address behavioral health care. 3 One in five peripartum individuals, defined as those in the period shortly before, during, and immediately after giving birth, experience a BH condition, with perinatal mood and anxiety disorders (PMADs) being the most common.4–6 In particular, the postpartum period is a season of increased vulnerability due to physiological symptom exacerbation and loss of ongoing prenatal care structures. Beyond the initial postpartum period, PMADs have been associated with long-term health risks, such as increased cardiovascular disease.1,6,7 Furthermore, PMADs can have generational consequences; children of mothers with untreated PMADs are at higher risk for developmental and behavioral disorders. 8 These findings highlight the critical need for timely intervention, emphasizing that addressing maternal mental health is essential not only for the mother’s well-being but also for the health of the entire family unit. 6
Despite these consequences, only 10%–15% of affected individuals receive timely, evidence-based treatment (e.g., counseling and pharmacotherapy), and even fewer achieve full symptom remission.1,6,9 Evidence-based guidelines from the American College of Obstetricians and Gynecologists, the American Heart Association, and the U.S. Preventive Services Task Force recommend routine postpartum screening, counseling, integrated care, and pharmacotherapy when indicated.6,10 However, low rates of BH screening and management, particularly in the postpartum period, persist due to systemic gaps in the United States, including fragmented postpartum care, lack of standardized screening and management protocols, insufficient BH integration, and constrained health care capacity, which are factors needed to implement evidence-based guidelines into clinical practice.1,11,12 Limited health care access and maternity care deserts, defined as counties with no hospitals or birth centers offering obstetric care (obstetricians, midwives, or nurse-midwives), reduce intervention reach.13,14 Beyond systemic barriers, individual postpartum barriers to BH care, including childcare, transportation access, language barriers, fragmented insurance coverage, and fear of child protective service involvement, further prohibit close postpartum follow-up for many individuals with BH conditions.11,12,15 Notably, those experiencing conditions that make BH care more challenging to access, such as poverty, housing and food insecurity, complex medical conditions, lack of insurance coverage, limited parental leave, and intimate partner violence, have an increased vulnerability to BH conditions,11,12 further emphasizing the need for care models that integrate evidence-based BH interventions, improve accessibility, and address structural determinants of health.
Peer support, defined as support provided by a family member, friend, or another patient who is either receiving treatment for a similar condition or has a relationship with the primary patient, can address community- and individual-level barriers to postpartum BH care.16,17 Peers can offer emotional and practical support, share personal experiences, participate in self-help and mutual aid activities, and collaborate with other community members or health care providers to meet patient needs, including prevention and treatment. 16 Peer support programs help connect individuals with lived experience of BH conditions to those currently navigating similar challenges. 18 They have emerged as part of the broader recovery movement in BH 18 and function as a complementary care strategy by filling gaps in traditional health systems through outreach to underserved populations, addressing stigma, facilitating engagement for those with limited access to services, and providing culturally relevant guidance.19–22 Evidence has shown peer support interventions can reduce symptoms of postpartum BH conditions, particularly among high-risk, early postpartum women, while providing social connection, emotional support, and empowerment to recipients and peer providers.23,24 The ability of peer supporters to fill these gaps is closely linked to their lived experience, which allows them to connect authentically with patients and navigate challenges that formal health systems may not fully address.16,25
Peer support interventions have demonstrated positive clinical outcomes, including reductions in the incidence and severity of PMAD.23,26 These interventions have shown promise in particularly benefitting populations facing health care access barriers, bridging the gap between postpartum BH care and those who need it most.12,26 With the increased symptom burden and waning support of the postpartum period, peer support serves as a promising linkage to BH services during postpartum. However, despite promising outcomes, gaps remain in optimal delivery and implementation related to heterogeneity in program design, limited training and resources, and barriers in integrating peer support within existing health care infrastructures.26–28 This review aims to identify and analyze the key facilitators and barriers that shape the delivery and effectiveness of peer support interventions targeting postpartum BH conditions. By examining how these interventions are implemented in real-world settings, the review seeks to clarify the factors that enable successful uptake, scalability, and sustainability, as well as the individual, organizational, and contextual barriers that constrain their impact in postpartum care.
Materials and Methods
This scoping review seeks to (1) describe the types and components of peer support interventions implemented during the postpartum period; (2) summarize available evidence on their implementation outcomes, barriers, and facilitators; and (3) identify gaps in the literature to inform future research and practice. The scope was limited to postpartum populations in high-income, English-speaking countries to account for differences in health care infrastructure, access, and cultural context to synthesize peer support implementation barriers and facilitators applicable to U.S. health care settings. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews guided the reporting of this review. 29
Search strategy
Four electronic databases, PubMed, Cochrane Library, Cumulative Index to Nursing and Allied Health, and APA PsycInfo, were searched using controlled vocabulary terms (e.g., Medical Subject Headings) and relevant keywords related to postpartum mental health (e.g., “postpartum depression,” “perinatal anxiety,” “maternal mental health”) and peer support (e.g., “peer mentoring,” “support groups,” “lay health worker”). Searches began in 2023 and were refined, including a search of the final strategies through January 2024. Searches included articles published in database from 2013 through January 2024 and were restricted to English-language publications. Search strategies were refined in consultation with a medical librarian, and the final search strings are available in the Supplementary Appendix. A bridge search was conducted from May 11, 2023 to October 2, 2025, to capture recent literature across the same four databases.
The Sample, Phenomenon of Interest, Design, Evaluation, and Research type framework informed eligibility criteria (Table 1). 30 Exclusion criteria included studies without primary evaluation data, interventions not involving peer support, and populations outside the postpartum period. Studies were included regardless of control or comparison group presence. Papers describing only methods were eligible if they clearly detailed the intervention implementation. Reference lists of included articles and relevant systematic reviews were searched to identify additional eligible studies.
SPIDER Framework

SPIDER, Sample, Phenomenon of Interest, Design, Evaluation, and Research.
Study selection
Search results were imported into Covidence 31 ; duplicates were removed automatically prior to screening. Independent screening was conducted at both the title/abstract and full-text stages by two reviewers. Reasons for exclusion at full text were recorded, and study selection was documented in a flow diagram (Fig. 2).
Data extraction
Studies were abstracted by one reviewer, followed by a secondary review by a separate study member to ensure accuracy and completeness. Extracted items included author and year of publication, study setting, sample demographics, guiding theory or framework, detailed description of the intervention, BH outcomes, implementation outcomes, equity considerations, implementation facilitators and barriers, and study limitations.
Linking multiple publications to a single study
When multiple publications reported findings from the same underlying study, we linked these articles and treated them as a single study unit for the purposes of data extraction and synthesis. Publications were considered to originate from the same study if they shared key characteristics, including study design, sample population, setting, intervention components, and study timeframe. In such cases, data were consolidated across articles to capture all relevant outcomes and methodological details while minimizing the risk of double-counting participants. Discrepancies across publications were resolved through team discussion.
Data analysis
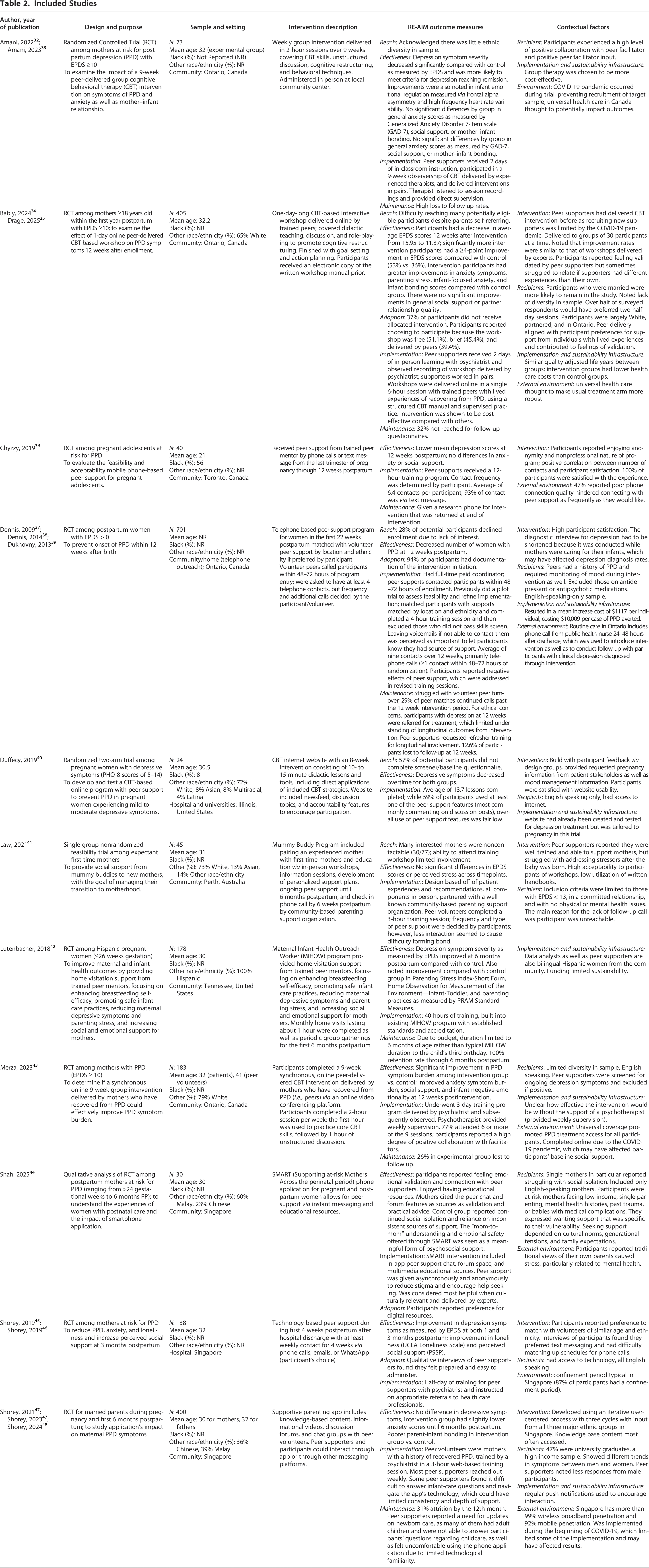
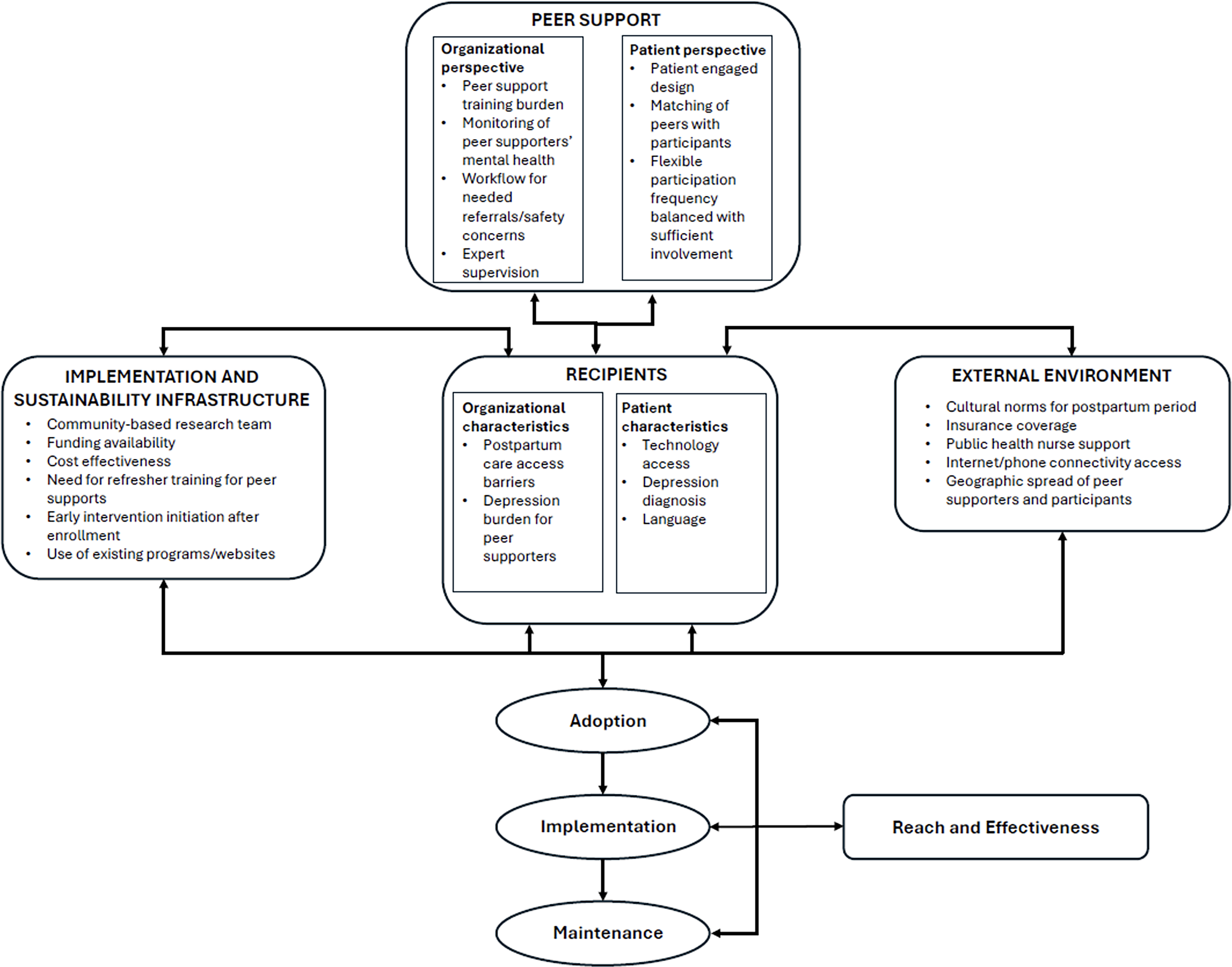
Extracted data were synthesized descriptively and summarized in Table 2. Implementation evaluation was guided by the Practical, Robust Implementation and Sustainability Model (PRISM) framework (Fig. 1). The PRISM framework has been widely applied across health care settings, including primary care, BH integration, and maternal health, to identify multilevel barriers and facilitators to implementation. 49 Its emphasis on the dynamic interaction between context and intervention makes it well suited for evaluating real-world implementation. Compared with other implementation frameworks, PRISM captures both system-level influences and patient-centered perspectives, which aligns with our focus on understanding the delivery and sustainability of BH interventions in complex postpartum care settings. Its inclusion of contextual determinants makes it particularly useful for identifying barriers and facilitators within the postpartum setting. 49 PRISM has been successfully used to guide implementation of community health interventions, 50 making the findings of this review translatable to inform implementation of peer support in a variety of postpartum settings. PRISM builds upon the well-established Reach, Effectiveness, Implementation, and Maintenance (RE-AIM) framework, which has been a mainstay of implementation evaluation for the last 25 years, and integrates the implementation outcomes of reach, effectiveness, adoption, implementation, and maintenance. 51 The PRISM framework adds contextual factors to understand how both internal and external features may impact the implementation of an intervention, which allows for integration of structural drivers of health inequities. 52 The PRISM framework includes four domains: (1) perspectives on the intervention; (2) characteristics of the implementers, recipients of the intervention, and setting; (3) external environment; and (4) implementation and sustainability infrastructure. 52 Collectively, these domains highlight how contextual factors shape implementation and outcomes.
Included Studies

Practical, Robust Implementation and Sustainability Model (PRISM). PRISM showing the relationships between contextual factors, intervention design, implementation processes, and outcomes.
In this review, reach captured the number and demographic characteristics of participants (i.e., age, race/ethnicity, and language), which could influence participation or engagement with the interventions. Contextual features about recipients included internal and external factors that may affect engagement and outcomes, such as social support, cultural norms, access to technology, or structural barriers. Distinguishing between these elements allowed us to consider the individual and external factors shaping participation.
Results
A total of 741 records were screened for the scoping review, with 18 manuscripts (2.4%) describing a total of 11 separate interventions meeting inclusion criteria for synthesis (Fig. 2). An additional study, by Dennis et al., 37 was not captured in the initial search due to a publication date prior to 2013; however, it was included in the data analysis as it described an intervention that was included within the captured manuscripts. The included interventions included nine randomized controlled trials, a single-group nonrandomized trial, and a randomized two-arm trial (Table 2). Studies were conducted in the United States, Singapore, Canada, and Australia and included sample sizes ranging from 24 to 701 participants. Interventions were delivered via phone or text, online or web-based CBT, home visits, group sessions, and peer-pairing programs. Peers provided a range of support, including emotional validation, CBT instruction, skill-building, parenting guidance, advocacy, and service navigation, with content and intensity varying across programs.

PRISMA Flowchart. PRISMA flowchart showing the identification, screening, eligibility assessment, and inclusion of studies (n = 11). PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension.
Outcome measures
Reach
Five interventions measured reach32,34,35,38,40,41; multiple studies noted recruitment challenges40,41 driven by difficulty contacting potential participants, participants’ inability to attend in-person study activities, and lack of interest. Studies also reported limited diversity in their sample.32,43,45
Effectiveness
All 11 interventions discussed effectiveness, most commonly measured by depressive symptoms [Edinburgh Postnatal Depression Scale (EPDS), Patient Health Questionnaire–8 (8-item depression scale-PHQ-8)]. Peer support interventions generally improved depressive symptoms and, in some studies, improved loneliness, parenting stress, and infant emotional regulation (Table 2). Five studies reported statistically significant reductions in PPD32,38,42,43,45; most studies measured depressive symptoms at 12 weeks postpartum, with one study showing improvement in postpartum depression symptom severity at 6 months postpartum. 42 The peer support interventions had variable effect on stress and anxiety symptoms,36,41–43 and one intervention reported decreased feelings of loneliness. 45 Four interventions that reported on infant outcomes reported positive improvements with peer support interventions, including infant emotional regulation32,43 and infant home environment. 42 However, one study reported poorer infant bonding in the intervention group compared with control. 47
Adoption
Four interventions detailed adoption.38,45 These studies reported variable adoption, with 37% 34 to 94% of participants initiating the intervention 38 and peer supporters reporting they felt prepared and found the interventions easy to administer. 45 Lower adoption was noted with group interventions, 34 and participants reported it was easier to adopt digital interventions. 44
Implementation
All 11 interventions detailed their implementation. Interventions were delivered via phone,36,38 text (mobile or WhatsApp),36,45 online platforms (i.e., websites or smartphone applications), 40 synchronous online groups, 43 and in-person group or home visits.32,41,42 Training for peer supporters was most often provided by clinical professionals who often offered ongoing supervision32,43,45; however, some studies implemented peer training into existing community programs. 42 Training requirements for peer supporters were variable from 3 hours41,45 to over 9 weeks 32 ; training requirements tended to be lower for those providing unstructured support, whereas interventions involving peers providing cognitive behavioral therapy-based interventions required more extensive training and occasionally observerships. 32 Peer support roles varied by study: some were volunteer-based, while others were paid positions. Interventions were delivered one-on-one or in groups. Fidelity was supported through strategies implemented by the researchers including supervision from clinicians, session recordings, review of negative effects of peer support, and structured manuals. Unstructured phone support interventions often did not specify frequency of contact and were individualized to the needs of individual participants; however, less interaction seemed to cause difficulty forming a bond with their peer supporter. 41 Some interventions were designed or refined by pilot trial feedback from participants.38,41 Specific feedback provided by participants included matching participants with supporters matched by location and ethnicity, 38 leaving voicemails if participant not reached to show they have a source of support 38 and partnering with a well-known community organization to improve acceptability. 41 Implementation was typically facilitated by training peer supporters and integrating interventions into existing programs when possible.
Maintenance
Maintenance was described in seven interventions32,36,38,42,43,47 and was a challenge for all interventions. Long-term sustainability was often limited by insufficient funding, volunteer turnover, and intervention constraints. For example, Dennis noted peer supporter turnover and ethical requirement to refer those with depression for clinical treatment as limitations to understanding the intervention’s long-term effects. 38 One study had to decrease the planned intervention from 3 years to 6 months due to budget limitations, 42 while another gave phones to participants for the intervention that were returned at the end of the intervention, limiting ongoing peer support contact. 36 Retention rates were variable,42,43 but one study reported that 29% of peer matches continued contact beyond the intervention period. 38
Contextual features
Intervention
Seven interventions discussed intervention features that impacted implementation.36,38,40,41,45 Participants reported enjoying the informal nature of peer support 36 and a preference for peer supporters of similar age and ethnicity as well as text messaging support due to difficulty scheduling phone calls. 45 Participant design groups for the intervention described in Duffecy et al. requested general pregnancy information be provided alongside mood management information. 40 Peer supporters reported feeling well trained but struggled to address postpartum stressors 41 and having to shorten interventions to allow participants to care for their infant. 38 Of note, one intervention found that CBT intervention delivered by peer supporters had improvement rates in depression scores similar to an intervention delivered by clinicians.34,35
Recipients
Seven interventions described contextual features about their recipients.32,34,38,40,41,43–45,47 Nondiverse participant samples were often driven by exclusion of non-English speakers40,43,45 and reliance on participants having access to technology for virtual interventions.36,40,43 Notably, some studies were limited to only those with negative depression scores,40,41 while others were conducted among those who met the diagnostic criteria of PPD. 38 Two interventions involved peer supporters who had a history of PPD, which required the research team to monitor their mood symptoms as well to ensure no worsening of their depressive symptoms related to the intervention.38,43 Acceptability of interventions tended to be high for both participants38,43 and peer supporters. 45
External environment
Eight interventions described external environment features that impacted their implementation.32,36,38,43,45 Four interventions discussed that they were completed in countries with universal health coverage,32,34,35,38,43 which affected their participants’ ability to access behavioral health care if needed and may have strengthened the control arm’s access to care. Health care and societal norms were also noted to be key features in implementation; for example, one intervention used the routine public health nurse phone calls provided to all Canadian postpartum women to introduce the intervention as well as provide follow-up for those diagnosed with depression through the intervention. 38 Another intervention was tailored to the external environment in Singapore, where most postpartum women traditionally have a postpartum confinement period during which the intervention took place. 45 The COVID-19 pandemic affected three interventions and led to decreased recruitment and transition to online formats.32,34,43 One study found that poor phone connection quality affected peer support interactions for almost half of their participants. 36
Implementation and sustainability infrastructure
Implementation and sustainability infrastructure captured the strategies used to support intervention delivery and fidelity. This included implementation strategies such as supervision, structured manuals, session recordings, and monitoring for adverse effects, all of which were used across studies to promote consistency. Seven interventions discussed their implementation and sustainability infrastructure.32,38,40,42,43 One intervention focused on providing peer support for Hispanic women employed both data analysts and peer supporters, who were all bilingual Hispanic women from the community to support intervention implementation. While one intervention utilized a psychotherapist to provide weekly supervision for group peer support sessions, they acknowledged that this could be cost-prohibitive long term and the effectiveness of the intervention without their support is unclear. 43 Two interventions discussed the role of sustainability in their study design; one study chose to utilize group therapy to make their intervention more cost-effective, 32 while another online intervention tailored an existing website previously tested for depression towards pregnancy. 40 One intervention completed an economic analysis and found the intervention resulted in a mean cost of $1117 per individual, reporting that the intervention cost $10,009 per case of PPD averted. 38
Discussion
In this review, we characterize the implementation features (Fig. 3) and outcomes of peer support interventions for postpartum BH. Our review is consistent with previous systematic reviews that peer support interventions are largely effective complementary interventions for prevention and management of postpartum BH conditions while evidence for broader clinical outcomes has been mixed. 53 Our review also suggests that these interventions may have benefits for infant emotional regulation, potentially through multiple pathways; improved maternal BH may enhance sensitivity and responsiveness, while some programs also incorporated parenting support, suggesting more direct behavioral effects.1,28 Future work should explore whether infant benefits arise from reduced maternal symptoms, parenting changes, or the unique contributions of peer support. 54 This review builds upon prior literature by specifying the defining implementation features of peer support interventions, which were successfully delivered through multiple formats, demonstrating flexibility of implementation to specific populations and care settings. Despite this, limited reach and challenges with long-term maintenance continue to restrict both the scalability and overall impact of these interventions. Implementing these programs brings important considerations for the mental health and well-being of peer supporters, 38 along with ethical questions about using peer support as an adjunct to standard care, including risks of exploitation through inadequate compensation or support, role ambiguity, and the potential for peers to be treated as substitutes rather than complements to professional services.21,22 Overall, these findings show the potential of peer support and the real-world challenges that must be addressed to improve postpartum BH.
Implementation features of postpartum peer support. Implementation features of postpartum peer support interventions mapped to the PRISM.
Several recurrent challenges for the interventions included in this scoping review can inform future peer support interventions. While peer support shows promising effectiveness, evidence remains limited regarding their generalizability and long-term sustainability. Recruitment and retention are persistent challenges, often limiting program reach and representativeness. Many programs relied on self-referral or word of mouth, which can underrepresent populations most at risk for postpartum BH conditions including racial and ethnic minority women, low-income mothers, adolescents, rural populations, and non-English speakers.1,7 Differences in participant selection reflected not only methodological choices but also underlying systemic structures. Clinically based studies primarily reached women already engaged in formal postpartum care, whereas community-embedded programs captured more socially vulnerable families who access support outside clinical systems. Digital recruitment relied on internet access and smartphone use, reinforcing technology-driven systems that may exclude women with limited digital literacy or resources. Future work should focus on strategies to enhance equity in access, improve recruitment methods, and ensure peer support programs are adequately resourced and supported. Collaboration between community organizations to support recruitment and provide infrastructure, with health care organizations to provide necessary oversight and adjunct medical care for both participants and peer supporters, is critical to responsible, sustainable peer support interventions. While peer turnover was not widely reported across the included studies, several interventions emphasized that structured training, clear role expectations, and ongoing supervision strengthened peer confidence and fidelity. Programs embedded within supportive community or health care organizations also facilitated retention and effectiveness, highlighting the importance of adequate organizational and management support.
An additional consideration is that many community-based organizations may be implementing effective, culturally responsive postpartum transition care strategies that are not reflected in the published literature. These programs often address barriers faced by vulnerable populations through tailored outreach, peer support, and integration of BH and social services. Strengthening collaboration between researchers and community-based organizations could help bridge the gap between evidence and practice, ensuring that the full range of effective postpartum care models is recognized and disseminated. Many of the interventions used platforms that were not clinically embedded (e.g., electronic health records), making integration with clinical services as well as evaluation of clinical outcomes more difficult. Further embedment of peer support into academic-community partnerships will promote both clinical team activation and understanding of their impact on patient outcomes.
Peer support for postpartum BH is unique compared with other conditions in several ways. Postpartum peer support often occurs during a sensitive and time-limited period and frequently addresses not only mental health symptoms but also parenting skills, infant care, social support, and family adjustment.54,55 Consistent with other reviews of peer support, our findings indicate that these interventions can improve depressive symptoms, social support, and coping skills.21,22 However, similar to prior literature, benefits are not uniform across participants, and implementation challenges—including training, supervision, and sustainability—are common. 1 These parallels and distinctions highlight the need to tailor peer support interventions to the specific developmental, clinical, and social context of the perinatal period, while learning from established best practices in broader peer support programs.
There are limitations to our study. The exclusion criteria for our study may have limited studies with effective interventions. For example, evaluating only manuscripts written in English and interventions in high-income countries may have limited our assessment of evidence-based interventions in non-English-speaking individuals. In addition, heterogeneity in intervention design, study setting, outcome measures, and follow-up time points limited direct comparisons across studies. Given that the goal of the study was to understand implementation features of peer support intervention, we did not complete risk of bias analysis of the interventions included. Although the included studies were conducted in high-income countries, significant income differences within these settings likely influenced who was able to participate, particularly when access relied on technology, consistent health care engagement, or community-based resources. International studies were included in our study, which enhances generalizability but introduces challenges for interpretation given the wide variation in health care systems, cultural contexts, and postpartum care structures across countries. However, interpretation must be approached cautiously due to substantial differences in health care systems, cultural contexts, and postpartum care structures across countries. Several interventions were facilitated by universal or highly resourced national health systems, contexts in which comprehensive postpartum services are routinely covered and accessible. These structural advantages may limit the direct applicability of such findings to U.S. settings, where fragmented coverage and variable access could affect implementation and impact.
Conclusions
While postpartum BH needs remain undertreated, this scoping review indicates that peer support interventions can be an effective and adaptable strategy to address postpartum BH, with potential benefits for infant well-being. These interventions demonstrate flexibility in design and delivery, making them applicable across various care settings and populations. However, limited reach, sustainability challenges, and ethical considerations related to the well-being of peer supporters continue to limit widespread implementation. Closing these gaps will require integration into existing systems, stronger support structures for peer providers, and strong approaches to scaling that maintain program fidelity.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under cooperative agreement (UR650351), Maternal Health Research Collaborative for Minority Serving Institutions. The information, content, and/or conclusions are those of the authors and should not be construed as the official position or policy of, nor should any endorsements be inferred by, HRSA, HHS, or the U.S. government.