
Abstract
Background:
Retention of weight postpartum increases risk for long-term morbidity, including cardiometabolic disease. Although retained weight postpartum is a complex problem, interventions generally address individual diet and activity behaviors.
Objectives:
We investigated the impact of social-network factors on postpartum health behaviors and weight.
Design:
We used an explanatory-sequential mixed-methods approach. This article reports our quantitative findings.
Methods:
Childbearing people receiving care at university-based clinics were eligible if aged 18+, 12–15 months postpartum, with a pre-pregnancy BMI ⩾ 25 kg/m2. An online survey collected participants’ demographic and outcome data and structured surveys collected personal social-network data. Block stepwise linear regression identified associations between social-network features and postpartum health behaviors and weight.
Results:
One hundred women completed both surveys; 62% did not return to pre-pregnancy weight. Multivariable models found: (a) participants with lower postpartum weight ate meals with more people in their network (β = −0.173, p = 0.063); (b) lower consumption of sugar-sweetened beverages was associated with greater proportions of the network who were siblings (β = −0.231, p = 0.011), and who were perceived to eat a healthy diet (β = −0.201, p = 0.031); (c) higher consumption of fruit was associated with a greater proportion of the network who helped with participants’ healthy-lifestyle goals (β = 0.288, p = 0.004), a smaller proportion of the network who were friends (β = −0.229, p = 0.022), and greater betweenness centrality (β = 0.302, p = 0.002); (d) lower consumption of fat was associated with smaller proportions of the network who were perceived to be sedentary (β = 0.288, p = 0.005), were friends (β = 0.311, p = 0.002), and were perceived to be normal weight (β = 0.202, p = 0.052) and with greater proportions of the network who encouraged participant goals (β = −0.257, p = 0.012) and were perceived to eat a healthy diet (β = −0.258, p = 0.015); (e) increased levels of activity were associated with a greater proportion of the network who were perceived to eat a healthy diet (β = 0.192, p = 0.044).
Conclusion:
Results revealed evidence for the role of social-network norms, support, and structure in postpartum health behaviors and weight. Understanding social environments’ impact on postpartum health behaviors and weight is essential in approaching the problem from a multilevel/domain approach.
Plain language summary
Weight that is retained after pregnancy increases a person’s long-term risk for poorer health outcomes, such as the development of type 2 diabetes. The problem of retained pregnancy weight is common. Three out of four people who give birth will have retained weight one-year after delivery. The postpartum year is a critical time to interrupt weight gain across the lifespan and support postpartum weight loss. However, the postpartum period poses unique challenges for childbearing people, including changes to social networks. Despite additional birth-related challenges, intervention efforts have generally focused on the dietary and activity behaviors of postpartum people, and rarely have these efforts addressed the social environment. Our study measured characteristics of childbearing people’s social relationships to help expand the current focus on health behaviors, which has allowed us to investigate the impact of the social environment on postpartum health behaviors and weight. Our study recruited people receiving care at university-based clinics who were aged 18+, were 12–15 months postpartum, and had a pre-pregnancy BMI categorized as overweight/obese. Participants completed an online survey so we could collect demographic information and data about their diet, activity, and weight. Participants then had a structured one-on-one interview with a researcher for the collection of data about the participants’ social relationships. Block stepwise linear regression was used to identify statistical associations between features of participants’ social relationships and their postpartum health behaviors and weight. One hundred participants completed the study. Of those, 62% had not returned to their pre-pregnancy weight, and the average postpartum weight change at one-year postpartum was 11.2 pounds greater than pre-pregnancy weight. Among the studies’ many findings, we found that as the participants’ total dietary fat per day increased, the proportion of the people in their social network who had healthy diets and who provided the participant with encouragement for their lifestyle goals decreased. Additionally, as participants’ fat intake increased, the proportion of their social networks who were sedentary most of their day increased. The study’s findings provide important preliminary information for the development of interventions that incorporate social-environment considerations. This information will help with tailoring of interventions to ensure that they are designed to effectively address postpartum health behaviors and healthy weight.
Keywords
Introduction
Weight that is retained postpartum is a common and complex problem that increases morbidity risk for childbearing people. About three-quarters will have retained pregnancy weight at 1-year postpartum. Of these, about half will retain an excess of 10 pounds, and a quarter will retain more than 20. 1 Moreover, people who begin pregnancy with a BMI categorized as overweight or obese have elevated risk for retaining weight postpartum.2,3 Childbearing people with overweight or obesity are twice as likely to gain weight in excess of gestational weight-gain guidelines.4,5 They also have up to four times greater risk of retaining weight postpartum. 1 Retained weight from pregnancy is associated with increased morbidity risk for diseases such as cardiometabolic disease.6 –8 Elevated maternal BMI has implications for the family, as well. Overweight and obesity associated with pregnancy are risk factors for postpartum weight retention, and are associated with children’s risk for overweight and obesity. Twenty-two percent to 42% of childhood overweight/obesity prevalence is attributable to perinatal overweight/obesity. 9 Finally, weight that is retained postpartum is a complex problem. Numerous predictors of postpartum weight retention have been identified in the literature, including gestational weight gain, 3 sleep, 10 breastfeeding, 11 mental health, 12 and social support, 13 which is a feature of social networks.
A person’s social network is composed of the people with whom they have relationships, and the social ties among those people (in this context, “social network” does not refer to a person’s online social-media network, though it could include important online relationships). 14 Social-network analysis provides a means for formally assessing the composition and structure of a person’s interconnected network of relationships, which have been shown to impact a person’s health behaviors. 15 For example, evidence for a “ripple effect” among significant others has been found, where partners of individuals participating in a lifestyle-change program also had healthy outcomes, including weight loss and healthier dietary behaviors. 16 While individual-level factors, such as postpartum diet 11 and activity, 17 have often been the focus of intervention efforts targeting weight retained postpartum, rarely have efforts used a multilevel/domain approach to the problem, such as a focus on the social environment. 18 This study harnessed the theory of normative influence to identify structural and functional features of social networks that are associated with postpartum health behaviors and weight. 19 Social norms serve as the foundation of the concept of normative influence, where behaviors common within a social network may be adopted by members of that network. 19 The study’s use of social-network analysis helps to expand the current focus on individual-level dietary and activity factors to also include the investigation of social-network factors’ impact on postpartum health behaviors and weight.
Therefore, the aim of this study was to investigate how structural features (density, centrality, constraint, and transitivity) and functional features (network norms and support) of social networks were associated with diet, physical activity, and postpartum weight change at 1-year postpartum among a sample of childbearing people who had a BMI categorized as overweight or obese pre-pregnancy.
Methods
Study design and participants
We conducted a cross-sectional, explanatory-sequential mixed-methods study 20 from December 2022 to December 2023. This article reports the quantitative results of the study. We recruited participants from University of Utah Health (UUHealth) clinics through a research partnership with UUHealth’s Obstetrics and Gynecology Research Network (OGRN). This partnership was established to support the study’s goal to recruit a racially and ethnically diverse sample of postpartum people in order to represent a wide range of participant experiences in the study’s findings. UUHealth includes more than 120 obstetric-care providers, and its patient population is more racially and ethnically diverse than the state of Utah overall.
Study inclusion criteria were: (1) aged 18 or older; (2) 12- to 15-month postpartum after giving birth to a live-born infant; (3) pre-pregnancy BMI (kg/m2) greater than or equal to 25 based on the electronic health record (EHR); (4) read and understood English; and (5) received care at a UUHealth site. The study exclusion criterion was that the person did not have access to web-based technology. We identified eligible participants in the UUHealth system through the university’s Electronic Data Warehouse (EDW). An OGRN research coordinator assessed interest in study participation by sharing an information sheet through the online electronic health-record app of potential participants. The coordinator gave the study’s primary investigator (JK-M) a list of eligible people who were interested in participating so they could be contacted for consent and enrollment procedures. Enrollment was tracked within racial and ethnic categories and capped as enrollment goals were met to ensure racial and ethnic representation in sampling. Participants digitally signed the informed consent document before taking the study’s online survey.
Also note that the authors have attempted to use inclusive language in this report. 21 We choose to use gender-neutral language in order to support inclusivity of childbearing people who do not identify as women. As we did assess gender identity in our individual-factors survey, and because all participants identified as women, we use this term when referring to the study’s results.
Procedure
Following the explanatory-sequential mixed-methods design, we began the study with the quantitative phase 20 which had two parts: (1) an individual-factors survey and (2) a structured personal social-network survey. The individual-factors survey was housed in the secure Research Electronic Data Capture22,23 environment and participants were sent survey links. Once a participant had completed their individual-factors survey, the primary investigator contacted the participant to find a time to meet by Zoom video conferencing 24 for the one-on-one structured personal social-network survey. The personal social-network survey was facilitated by the Network Canvas app, which is an open-source software created for the collection of social-network data. 25 This structured survey was composed of three parts and lasted between 45 min and 1 h. First the participant was prompted to list approximately 15 people who were in their lives during the postpartum period. Second, the participant then gave information about the characteristics of each of those people so that functional characteristics of the network could be created. In the third and last part of the survey, participants provided information about the connections between each of the people in their networks so that network structural features could be created (the personal social-network survey has been included in the Supplemental material section, Appendix A).
Upon completion of the social-network survey, participants were offered a $75 gift card as a thank you for their participation in the study.
Variables
Participant individual-level data were collected through the individual-factors survey containing validated tools. Refer Table 1 for details about these tools. Individual-level data included participant demographics that have been identified as common predictors of postpartum weight retention (i.e., age, race/ethnicity, partnered status, number of children, education, annual household income, pre-pregnancy and current height/weight, and maternal mental wellbeing). These data were used to control for individual-level factors during the study’s block stepwise regression analyses.
Study variables and measurement tools.
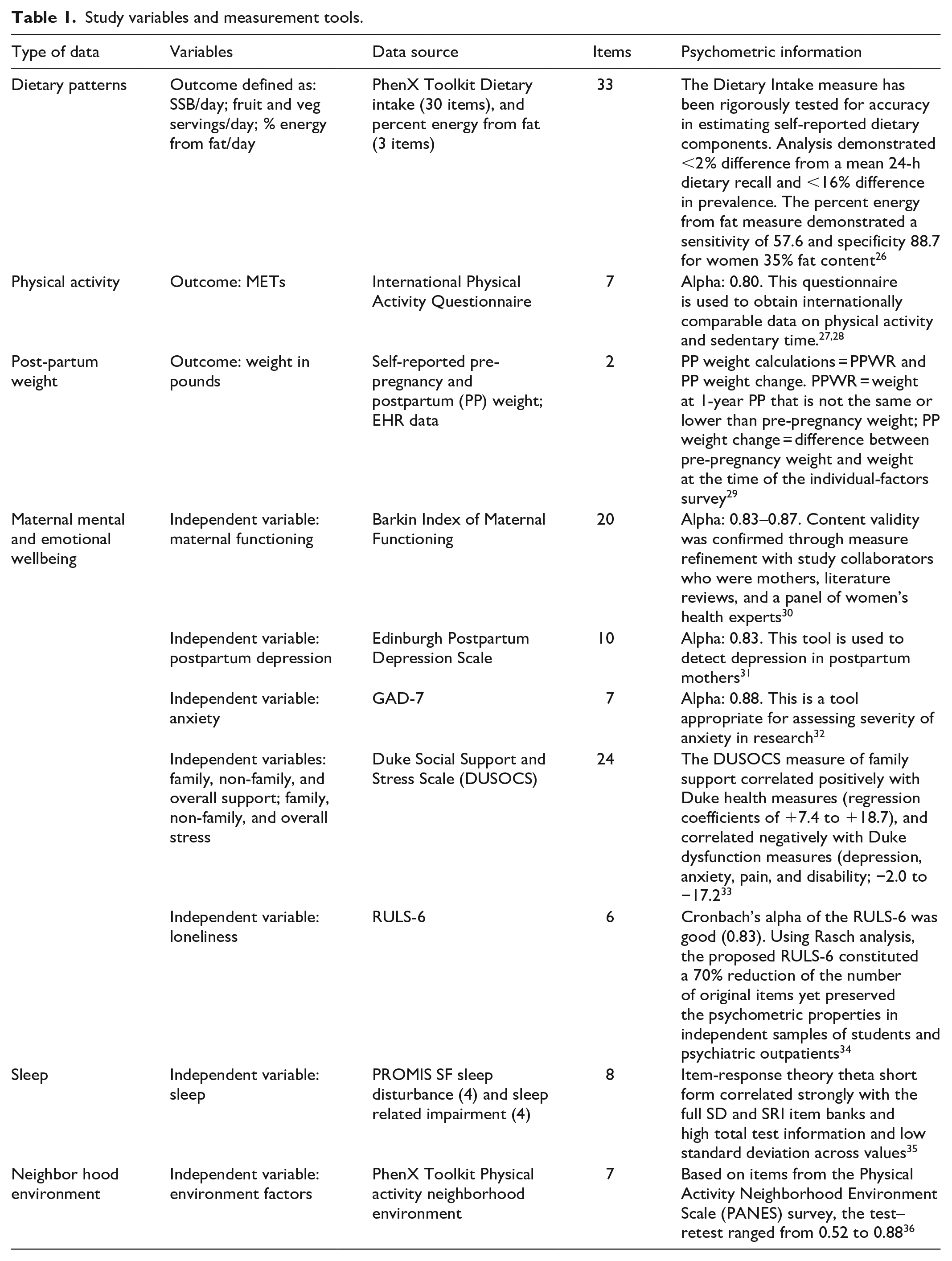
The study’s outcome variables were diet, physical activity, and postpartum weight change. We assessed dietary patterns using validated scales available from PhenX Toolkit. 37 The dietary outcomes were daily intake of (1) sugar-sweetened beverages (SSB), (2) fruit, (3) vegetables, and (4) percent energy from fat. The physical activity outcome was assessed using the 7-item International Physical Activity Questionnaire.27,28 Participant weight data came from self-reporting and health-system records. Postpartum weight change was calculated by finding the difference between participants’ pre-pregnancy weight and their weight at the time of the individual-factors survey.
We collected details about the structural and functional features of participants’ networks through the study’s structured personal social-network survey. There were four structural features of interest. They were: (1) density (i.e., the extent of network member interconnectedness or sparsity), (2) centrality (which measures three different types of centralities—degree, closeness, and betweenness centrality—and assists with identifying influential alters within a network), (3) constraint (which assesses the degree to which the participant is connected to alters who are highly connected to one another), and (4) transitivity (which is the assessment of the presence of triad clusters within a network, where friends of friends are friendly).15,19
The functional features of interest included details about the participants’ network members. These functional characteristics included the demographics of participants’ network members (e.g., network members’ approximate age and sex), participants’ frequency of contact with their network members, the types of relationships participants had with their network members (e.g., mother, partner), perceived health attributes of the network members (e.g., perceived weight status), and whether their network members provided health-related social support (e.g., encouragement for the participants’ healthy-lifestyle goals). Refer Table 2 for details about the personal social-network variables.
Personal social-network variables.

The individual-factors and personal social-network surveys were reviewed prior to participant recruitment by the study’s community advisory board (CAB), which was composed of two postpartum women, a community health worker, and a Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) nutrition coordinator. The CAB provided feedback on the surveys’ content. The feedback was then integrated, and the CAB deemed the surveys appropriate for the study’s population.
Sample size
Our a priori power analysis was based on the presence of network members who made it difficult to achieve weight-related goals and the outcome of weight loss based on data from Winston et al. 38 We determined that a sample size of 100 postpartum people would result in a Cohen’s d effect size of 0.57. This large effect size indicated a sample size of 100 would have sufficient power (80%) to detect a significant difference between groups. Our study was not powered to test differences between racial and ethnic groups.
Statistical analysis
Data were reviewed for missingness and normality and determined to be completely missing at random. Therefore, as missingness for each scale totaled less than 5%, we handled missing data per the guidelines for the individual scales. Social-network variables for network-member attributes, network norms, and social support were created in the igraph package in R version 1.4.1717 from the network data representing proportions of the network (i.e., percentages of the network who had a particular characteristic, such as the percentage of the network who were perceived to eat a healthy diet).39,40 We used descriptive statistics to describe participant characteristics, such as their age, race/ethnicity, postpartum weight, etc. To explore relationships between variables, we created bivariate analyses between the study’s independent variables (demographic-level and network-level) and outcome variables (diet, activity, and postpartum weight change).
Last, SPSS 29.0.1.0 was used for the block stepwise regression approach to assess network-level predictors for each outcome. 41 As this was an exploratory study, the alpha was set at 0.10 for model retention. A separate regression model was made for each of the study’s outcomes (i.e., one each for servings of SSB, servings of fruit, servings of vegetables, daily percent energy from fat, physical activity reported in METs [multiples of resting energy expenditure], and postpartum weight change). We first regressed on the participant individual-factors data (block one) and then on the social-network variables (block two), allowing for the individual-factor covariates of the study to be controlled prior to analyzing the social-network variables. The demographic-level data that were loaded into the stepwise analysis as the first step were: participant age, race/ethnicity, education, income, parity, breastfeeding, pregnancy complications, maternal functioning, social support, social stress, postpartum depression, anxiety, neighborhood environment, sleep disturbance, and sleep impairment. Next, the social-network variables were added to the stepwise analysis. These network-level variables were: network structure (i.e., density, betweenness centrality, constraint, and transitivity), network support (i.e., provision of health information, healthy-lifestyle encouragement, sharing of meals, mutual engagement in physical activity, and help with/difficulty toward healthy-lifestyle goals), network norms (i.e., normal weight among network members, engagement in regular physical activity, regular sedentary behavior, and healthy dietary behaviors), and network-member characteristics (i.e., closeness of relationship with participants, age, sex, relationship type, and proximity to the participant).
The Strengthening the Reporting of Observational Studies in Epidemiology guidelines for cross-sectional studies was followed when preparing the manuscript for publication. 42
Results
Sample characteristics
The EDW identified 590 potentially eligible people. Figure 1 presents the flow of participant screening and enrollment, and completion of the study’s procedures. In total, 108 of the 112 people who began the individual-factors survey completed it. Of the 108 participants who completed the individual-factors survey, 100 participated in the structured social-network survey.

Participant flow for study enrollment and completion of study procedures.
Table 3 provides participant descriptive statistics. All participants identified as women. Their ages ranged between 20 and 43 years (M = 31.69, SD = 5) for the 108 participants who completed the individual-factors survey. Most participants were White and not Hispanic or Latino (42.6%), were married (75.5%), and had a median of two children. The most commonly reported highest level of education was a Bachelor’s degree (26.9%), followed by having some college (17.6%). Just over half of participants (51.4%) reported their financial situation as comfortable. The median household income was $73,000 (SD = $30,000). Approximately one-third (n = 34) were WIC recipients.
Descriptive statistics of participant demographics (N = 108).

At the time of the study, participants’ average BMI (kg/m2) was 32 (SD = 6.49); 94% had a weight classified as overweight or obese; 62% had not returned to their pre-pregnancy weight by 1 year; and the average weight change at 1 year postpartum was 11.2 pounds greater than pre-pregnancy weight. On average, participants consumed less than one-half serving of SSB per day (M = 0.42 serving, SD = 0.84). Their daily fruit intake was just less than one-and-a-half servings per day (M = 1.44 servings, SD = 1.18), and daily vegetable intake was nearly two servings (M = 1.98 servings, SD = 1.38). The average level of activity, reported in multiples of resting energy expenditure per week (METs), was 2852.99 (SD = 3398.22).
Network-level characteristics
Participants’ average network size was 14.74 network members (SD = 2.21). Participants generally shared close relationships with their network members (M = 0.90, SD = 0.15). The network norms among participants’ network members included the norms for perceived normal weight (M = 0.52, SD = 0.17), regular exercise (M = 0.53, SD = 0.19), and healthy diets (M = 0.57, SD = 0.23). Participants received social support from their network members in the form of encouragement for participants’ healthy-lifestyle goals (M = 0.53, SD = 0.22). See Figure 2 for a diagram modeling all 100 participants’ network support. Of note, however, a majority of participants (n = 72) also reported that their network members made it difficult for them to attain their healthy-lifestyle goals. The average proportion of the network who created difficulty was 0.25 (SD = 0.20). The standard deviations indicate there was variability among participants, where some women had more or less positive health norms or social support. For network structure, the average density was 0.56 (SD = 0.17), the average betweenness centrality was 2.83 (SD = 1.57), the average constraint was 6.10 (SD = 1.34), and the average transitivity was 0.76 (SD = 0.13).

The figure models the characteristic of network encouragement for healthy-lifestyle goals. The dots represent the participant (in red) and their network members, and the lines indicate a relationship between two people in the network. Orange dots represent a network member who provided health and encouragement for the participants’ healthy-lifestyle goals. Blue dots represent a network member who did not.
The following subsections will outline the demographic-level and network-level factors that were significantly associated with the study’s outcomes of diet, activity, and postpartum weight change.
Associations between network characteristics and the weight outcome
There was one network-level finding and seven demographic-level findings associated with the outcome of postpartum weight. The one network-level finding associated with lower postpartum weight was the proportion of the network with whom the participant ate regularly. That is, the finding indicates that participants with lower postpartum weight ate meals with more people in their network (β = −0.173, p = 0.063). The seven demographic-level findings indicate that lower postpartum weight was associated with higher income (β = −0.210, p = 0.035), fewer sleep disturbances (β = 0.275, p = 0.003), White race (β = −0.352, p < 0.001), Hispanic ethnicity (β = −0.349, p < 0.001), longer duration of breastfeeding (β = −0.259, p = 0.070), higher social-support score on the Duke Social Support and Stress Scale (β = −0.186, p = 0.050), and less friendly neighborhood environment for outdoor activity (β = 0.165, p = 0.070). Table 4 presents the results of the stepwise linear regressions between the demographic-level and network-level factors and the weight outcome.
Stepwise linear regressions of associations between demographic-level and network-level factors and the weight outcome.

Associations between network characteristics and the dietary outcome of sugar-sweetened beverages
There were two network-level findings and two demographic-level findings associated with the outcome of SSB consumption. The network-level findings indicate lower consumption of SSB was associated with a greater proportion of the network who were siblings (β = −0.231, p = 0.011), as well as a greater proportion of the network who were perceived to eat a healthy diet (β = −0.201, p = 0.031). The demographic-level findings indicate that lower consumption of SSB was associated with greater participant education (β = −0.621, p < 0.001) and younger age (β = 0.231, p = 0.020). Table 5 presents the results of the block stepwise linear regressions between the demographic-level and network-level factors and the dietary outcome of daily SSB consumption.
Stepwise linear regressions of associations between demographic-level and network-level factors and the outcome of diet—SSB.

Associations between network characteristics and the dietary outcome of fruit
There were three network-level findings and two demographic-level findings associated with the outcome of fruit consumption. The network-level findings indicate that higher consumption of fruit was associated with a greater proportion of the network who helped with participants’ healthy-lifestyle goals (β = 0.288, p = 0.004), a smaller proportion of the network who were friends (β = −0.229, p = 0.022), and greater betweenness centrality (β = 0.302, p = 0.002). The demographic-level findings indicate lower consumption of fruit was associated with Hispanic ethnicity (β = −0.253, p = 0.013) and higher scores on the Edinburgh Postnatal Depression Scale (β = −0.176, p = 0.070). Table 6 presents the results of the stepwise linear regressions between the demographic-level and network-level factors and the dietary outcome of daily fruit consumption.
Stepwise linear regressions of associations between demographic-level and network-level factors and the outcome of diet—fruit.

Associations between network characteristics and the dietary outcome of vegetables
Statistically significant associations were not found between network variables and the outcome of vegetable intake. The demographic-level findings indicate lower consumption of vegetables was associated with Hispanic ethnicity (β = −0.272, p = 0.010), less education (β = 0.191, p = 0.075), less friendly neighborhood environment for outdoor activity (β = 0.231, p = 0.023), and shorter duration of breastfeeding (β = 0.173, p = 0.097). Table 7 presents the results of the stepwise linear regressions between the demographic-level and network-level factors and the dietary outcome of vegetable consumption.
Stepwise linear regressions of associations between demographic-level and network-level factors and the outcome of diet—vegetables.

Associations between network characteristics and the dietary outcome of percent energy from fat
There were five network-level findings and one demographic-level finding associated with the outcome of fat consumption. The five network-level findings indicate lower consumption of fat was associated with smaller proportions of the network who were perceived to be sedentary (β = 0.288, p = 0.005), were friends (β = 0.311, p = 0.002), and were perceived to have a normal weight (β = 0.202, p = 0.052). They also indicate lower consumption of fat was associated with greater proportions of the network who provided the participant with encouragement for the attainment of their healthy-lifestyle goals (β = −0.257, p = 0.012) and were perceived to have a healthy diet (β = −0.258, p = 0.015). The one demographic-level finding indicates that lower consumption of fat was associated with fewer sleep disturbances (β = 0.213, p = 0.023). Table 8 presents the results of the stepwise linear regressions between the demographic-level and network-level factors and the dietary outcome of daily percent energy of the diet from fat.
Stepwise linear regressions of associations between demographic-level and network-level factors and the outcome of diet—fat.

Associations between network characteristics and the physical-activity outcome
There was one network-level finding and four demographic-level findings associated with the outcome of physical activity. The one network-level finding associated with participant physical activity indicates that increased levels of activity were associated with a greater proportion of the network who were perceived to eat a healthy diet (β = 0.192, p = 0.044). The four demographic-level findings indicate that increased levels of activity were associated with fewer sleep impairments (β = −0.308, p = 0.001), a greater number of live births (β = 0.383, p < 0.001), less friendly neighborhood environment to outdoor activity (β = −0.188, p = 0.045), and fewer pregnancy complications (β = 0.169, p = 0.069). Table 9 presents the results of the stepwise linear regressions between the demographic-level and network-level factors and the physical-activity outcome.
Stepwise linear regressions of associations between demographic-level and network-level factors and the activity outcome.

Discussion
Discussion of results
We identified preliminary associations between social-network characteristics and postpartum diet, activity, and weight. A scoping review of 45 publications found that social contagion, social capital, and social selection were mechanisms important to social-network characteristics and overweight/obesity in general. 43 Although the cross-sectional nature of the current study precludes the identification of causal mechanisms between social-network characteristics and postpartum health behaviors, the use of qualitative exploration and mixed-methods triangulation sheds some light on possible processes. Specifically, for postpartum diet, this study found some evidence of the importance of network norms, structure, and support. For physical activity, this study suggests the importance of network norms; and for postpartum weight, network support was identified as an important network feature. These factors may have an important role in future intervention efforts and mechanistic studies.
For the outcome of postpartum weight, we identified network support as an important network feature. Specifically, a greater proportion of the network who ate regularly with participants was associated with lower postpartum weight. It is difficult to interpret this finding in the context of previous research, as limited research exists that has investigated proportions of the network with whom participants ate. In our study, network shared eating was conceptualized as a form of social support and as a context in which exposure to social influence may occur, such as the establishment of higher-in-quality or lower-in-quality eating norms among a group who eat together. In the single other study investigating social networks and postpartum health behaviors, De la Haye et al. 44 found that participants’ healthier weight outcomes were associated with network encouragement for participants’ healthy behaviors. This finding backs the role of social support as important to postpartum weight.
For postpartum diet, we found evidence for the role of network norms, structure, and support. Network-norm features had associations with the dietary outcomes of SSB and percent energy from fat. Specifically, the network norms associated with lower SSB intake were (1) the proportion of the network who were perceived to have a healthy diet, and (2) a greater proportion of the network who were siblings. While the association between a lower intake of SSBs and a greater proportion of the network who were perceived to have a healthy diet may be a logical finding, the siblings finding may seem less intuitive. A potential explanation for the negative relationship between SSB intake and siblings could relate to the SSB intake patterns of the participants’ siblings. Pachucki et al. 45 found sibling-related dietary correlations, where brothers were correlated on soda intake and a healthier dietary pattern, and sisters were correlated on a healthier dietary pattern.
There were three network norms associated with the fat-intake outcome. They were proportions of the network who were perceived (1) to be sedentary most of the time, (2) to have a normal weight, and (3) to have a healthy diet. Here, participants’ lower percentage energy intake from fat was associated with lower proportions of the network who were perceived (1) to be sedentary most of the time and (2) to have a normal weight, and a greater proportion of the network who were perceived (3) to have healthy diets. While the finding about network normal weight might seem unintuitive (where a lower proportion of network normal weight was associated with participants’ lower intake of fat), the mixed-methods phase of our study identified a potential explanation for this finding. Some participants who had lower daily fat intake had greater proportions of the network with overweight or obesity. These participants described a strong sense of self-determination and commitment to their healthy-lifestyle goals that was established through their recognition of the norm for overweight among their network members. They said witnessing the negative health impacts of excess weight had helped them to establish ownership of their behaviors.
One network-structure feature was found to have an association with the dietary outcome of fruit. Specifically, greater network betweenness centrality was associated with greater fruit intake. Measures of network centrality help with the identification of influential network members. 15 Greater control of the flow of information and resources through a network have been associated with networks with high betweenness centrality. 15 At the level of the network, those network members with a high betweenness centrality are often perceived as important people who interact across the participants’ various social contexts. 46 Interventions using a network approach have targeted these central network members with high centrality in order to support health-behavior change among the network. For example, these key network members have been used as peer educators to support increased intake of fruit and vegetables among their peers. 47 Our finding suggests that the network centrality may be a useful factor to harness in intervention work targeting postpartum diet.
Last for the dietary outcome, network social-support features had associations with the dietary outcomes of fruit and fat intake. Specifically, greater support for participants’ healthy-lifestyle goals was associated with greater intake of fruit. Similarly, this network support for participants’ healthy-lifestyle goals was also associated with lower daily intake of fat. One single other study has investigated postpartum social networks and health behaviors. This study had similar findings to the present study. It found network support was associated with higher-in-quality dietary outcomes, such as increased vegetable intake. It also found that healthier weight outcomes were associated with network support in the form of encouragement for healthy behaviors. 44
For physical activity, we found evidence of the importance of network norms. Specifically, a greater proportion of the network who were perceived to have a healthy diet was associated with participants’ increased activity. Although it is known that the activity norms of a person’s social network is predictive of their own activity, and that, similarly, the dietary norms of a person’s social network are predictive of their own dietary behaviors, 48 we do not know if associations exist between activity and dietary norms among networks, as was found in our study. Exploration of the co-occurrence of higher-in-quality and lower-in-quality patterns of health behaviors among network members could be the focus of future studies.
Implications for clinical practice
The results from the quantitative phase of our mixed-methods study provides healthcare professionals with details about how the social environment plays a role in postpartum health behaviors and weight. The study’s findings support family- and network-centered approaches to interventions designed to support postpartum health behaviors and weight. This is an important first step in expanding our current focus on individual-level factors, such as diet and activity, to also incorporate multilevel and domain considerations, such as the impact of relationships on postpartum people’s ability to engage in healthy behaviors.
The study’s mixed-methods analysis provides additional insight for those wishing to develop interventions that consider the social environment for postpartum people. To illustrate this point, we will briefly outline our mixed-methods findings. We found stronger network norms for regular exercise engagement and healthy diets, more network encouragement for healthy behaviors, and increased participant self-determination to attain lifestyle goals among participants who had lower fat intake. Similarly, participants who were more active described stronger network norms for physical activity and healthier diets, while the participants who were less active described weaker network norms for physical activity and more pressure to conform to unhealthy network dietary behaviors (e.g., overeating at gatherings centered around food). Common features among the more active group which supported their lifestyle goals were social selection of network members who could support their goals, social support, less network difficulty toward participants’ lifestyle goals from network members, and the participants’ self-determination. Last, participants who retained more weight postpartum described stronger network norms preferring unhealthier foods and more pressure from network members to overeat and to match their eating behaviors with those of network members. Participants who lost most weight when compared to their pre-pregnancy weight described stronger network norms for healthy diets and physical activity. They also used social selection of network members who could support their healthy-lifestyle goals. Additionally, these participants’ self-determination and commitment to their lifestyle goals appear to have been important buffers to the network difficulty they encountered. In sum, we believe the use of social-network methods could be a promising approach for assessing network strengths and weaknesses. For example, once a postpartum person’s network has been assessed for network resources and barriers to healthier behaviors, this information could then be used in a motivational interview to help the person leverage network strengths while problem-solving network barriers (refer the publication’s Appendix B in the Supplemental materials section to view a file of the mixed-methods meta-inferences).
Strengths and limitations of the study
This study has limitations related to its social-network methods. First, because this was not a longitudinal study, we were not able to test mechanisms related to social-network theory. However, our use of mixed methods did allow us to investigate women’s perceptions about their networks’ social norms and support related to their postpartum health behaviors and weight (refer our study’s companion article in this issue, which reports our qualitative findings). This contributes to an area of research with limited investigations among a population that has rarely been studied from a social-network perspective. Second, the participant-focused (i.e., ego-centric) methods of this study relied upon participant self-report to determine network norms, support, and structure. Although this study used self-reporting, individuals’ perceptions of their network members’ behaviors has been shown to be an important determinant of participants’ own behaviors and motivations. 49 Third, although our sample represents greater racial and ethnical diversity than the UUHealth system and the state of Utah overall, we recruited only English-speaking people. This limits the generalizability of our results. Future studies should use community-engaged approaches to understand social-environment impacts of postpartum people within specific communities. Fourth, future studies focused on postpartum social networks and diet could more comprehensively assess dietary patterns using a 24-h recall screener, such as the National Institutes of Health’s Automated Self-Administered 24-h (ASA-24) Dietary Assessment Tool. 50 Last, the study’s weight outcome primarily relied on data obtained through participant self-report. This may have introduced some bias, such as recall bias or social-desirability bias in the underreporting of weight that may have impacted our calculations of postpartum weight retention. 51 A systematic review on the self-reporting of maternal weights found errors in self-reporting did not significantly bias resulting associations between pre-pregnancy weights and outcomes. 52 We anticipated the limitation of self-reporting through strategies shown to be effective in prior research including the use of non-threatening language, use of confidential self-administered surveys, and collaboration with a CAB.53,54
Conclusion
We found several associations between social-network characteristics and postpartum health behaviors and weight. These findings shed light on and provide some evidence for the role of social-network norms, support, and structure in postpartum health behaviors in weight. These findings provide important preliminary information that can help inform future longitudinal study designs that can measure network mechanisms. Additionally, these results can help guide intervention development that incorporate network considerations and that are designed to effectively address postpartum health behaviors and healthy weight. Understanding the impact of the social environment on these outcomes is an essential first step in approaching the problem from a multilevel approach.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251321872 – Supplemental material for Associations between social-network characteristics and postpartum health behaviors and weight among a sample of women who were overweight/obese pre-pregnancy
Supplemental material, sj-docx-1-whe-10.1177_17455057251321872 for Associations between social-network characteristics and postpartum health behaviors and weight among a sample of women who were overweight/obese pre-pregnancy by Jacqueline Kent-Marvick, Bob Wong, Sara E Simonsen, Kristin G Cloyes, Michelle Precourt Debbink, Cristina Creal and Kayla de la Haye in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057251321872 – Supplemental material for Associations between social-network characteristics and postpartum health behaviors and weight among a sample of women who were overweight/obese pre-pregnancy
Supplemental material, sj-docx-2-whe-10.1177_17455057251321872 for Associations between social-network characteristics and postpartum health behaviors and weight among a sample of women who were overweight/obese pre-pregnancy by Jacqueline Kent-Marvick, Bob Wong, Sara E Simonsen, Kristin G Cloyes, Michelle Precourt Debbink, Cristina Creal and Kayla de la Haye in Women’s Health
Supplemental Material
sj-docx-3-whe-10.1177_17455057251321872 – Supplemental material for Associations between social-network characteristics and postpartum health behaviors and weight among a sample of women who were overweight/obese pre-pregnancy
Supplemental material, sj-docx-3-whe-10.1177_17455057251321872 for Associations between social-network characteristics and postpartum health behaviors and weight among a sample of women who were overweight/obese pre-pregnancy by Jacqueline Kent-Marvick, Bob Wong, Sara E Simonsen, Kristin G Cloyes, Michelle Precourt Debbink, Cristina Creal and Kayla de la Haye in Women’s Health
Footnotes
Acknowledgements
We are grateful to the Network Canvas team for developing their superlative open-access app that made it possible for us to collect our network-level data. We are appreciative of our community advisory board members’ time, guidance, and their commitment to the health and well-being of the postpartum population. Last, we are thankful to our study’s participants for their collaboration on and interest in this research topic.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.