
Abstract
Background:
The coronavirus disease 2019 (COVID-19) pandemic has significantly impacted the health of pregnant women and their unborn babies.
Objective:
To explore the impact of COVID-19 on intrapartum care in Ethiopia.
Design:
A concurrent mixed-methods design was employed.
Methods:
An interrupted time series analysis was implemented using a Poisson regression model to estimate monthly changes in the incidence rates of institutional childbirth, instrumental vaginal birth, caesarean section, stillbirth, institutional neonatal death, institutional maternal death and availability of essential medical supplies before and during COVID-19. The dataset included data from all women who gave birth in 15 public hospitals, and the total number of childbirths in the cohort study before COVID-19 (12 months of data from March 2019 to February 2020) was 24,478, while during COVID-19 (6 months of data from March to August 2020), the total number of childbirths in the cohort study was 11,966, forming a combined final dataset of 36,444. Simultaneously, a descriptive qualitative study using a purposive sampling technique was conducted through in-depth interviews until data saturation was reached, with data were collected from 14 February to 10 May 2022. Data from the interviews were imported into NVivo 12 Plus to perform an inductive thematic analysis. Quantitative and qualitative data were integrated using joint display methods to identify corroboration or contradiction between the different forms of evidence.
Results:
Our findings indicate that the incidence rates of caesarean sections and instrumental vaginal births significantly increased in the first 6 months of COVID-19. Three themes were identified: ‘Barriers to providing intrapartum care during COVID-19’, ‘Delays to provision of intrapartum care during COVID-19’ and ‘Inadequate COVID-19 preventive measures’.
Conclusion:
In combination, the three themes contributed to a considerable increase in neonatal and maternal deaths. Interventions such as fully equipped labour wards and obstetric triage systems are needed to restore disrupted maternal and perinatal care during the ongoing and future pandemics. In addition, stakeholders should inform the public that blood donations can help the community recover from recent shocks in emergency health and future pandemics. Further research should investigate the long-term impact of COVID-19 on maternity care and maternal and infant outcomes.
Keywords
Introduction
The provision of quality intrapartum care is pivotal to lowering maternal death 1 ; hence, where women give birth in a health facility or assisted by healthcare providers, childbirth-related maternal and neonatal mortality is typically lower.2,3 To illustrate, a study in 37 sub-Saharan African and South Asian countries showed that institutional childbirth substantially decreased neonatal deaths. 4
Every day, 810 women die worldwide from preventable complications related to pregnancy and childbirth, such as haemorrhage, preeclampsia, puerperal sepsis and unsafe abortion. 5 Similarly, 6500 neonates die every day worldwide. 6 In 2017, low-resource countries accounted for over 86% of all maternal deaths, with 66% of all maternal deaths worldwide occurring in sub-Saharan Africa. 5 In Ethiopia, there were 14,000 maternal deaths in 2017, 5 three-quarters occurred during childbirth and the immediate postnatal period. 1 Factors contributing to maternal deaths in low- and middle-income countries (LMICs) include poverty, long distances to health facilities, lack of information, inadequate quality of care, cultural beliefs and practices and shortages of medical supplies and human resources in health facilities.7 –9
Improving the quality and quantity of skilled birth attendants is a fundamental pillar in reducing maternal and newborn mortality. 10 In LMICs, a range of multifaceted strategies have been employed to promote institutional childbirth and enhance access to skilled birth attendants 11 including interventions to improve access to institutional birth, 12 deploying community health workers, 13 mass media campaigns 14 and providing free healthcare for pregnant women.11,15 Other strategies include building hospitals; scaling up the training of nurses, midwives, general practitioners and obstetricians and building their capacity through continuous professional development training.11,16 Many women, however, still give birth without assistance from skilled healthcare providers, 17 and the quality of intrapartum care does not reach the desired level in LMICs. 18
Globally, coronavirus disease 2019 (COVID-19) has disrupted health systems and services, 19 especially in LMICs. 20 According to studies in these countries, institutional births declined during COVID-19,21,22 while caesarean sections increased.23,24 However, home births also increased in LMICs 25 due to fear of contracting the virus, delays in receiving care and poor coordination in the referral system.26,27 Consequently, the pandemic significantly increased stillbirths and maternal deaths in LMICs. 28
COVID-19 has made it more challenging to implement and maintain proven strategies for improving institutional births and the quality of intrapartum care in resource-scarce countries such as Ethiopia. 19 Consequently, an overwhelming number of countries seem unlikely to meet their targets of lowering maternal mortality to below 70 per 100,000 live births and neonatal mortality to below 12 per 1000 live births by 2030. 29 The existing studies in Ethiopia on the impact of the COVID-19 pandemic have not rigorously explored its effects on intrapartum care. Additionally, while the studies in Ethiopia have described the impact of COVID-19 on intrapartum care, none of them have data from care providers’ voices, to explain the impact on their experiences and to tell the full story of what the data is suggesting. The integration of different data collection methods aims to provide a rich and deep understanding of intrapartum care. Therefore, it is crucial to quantify and explore barriers to institutional childbirth and intrapartum care uptake and provision during the pandemic, thereby contributing to the design of evidence-based interventions.
Methods
Study settings and design
This study is part of a larger mixed-methods investigation of the impact of COVID-19 on maternal and perinatal care in Ethiopia during the period from 14 February to 10 May 2022. Further details about study settings can be found in the following project. 30 Concurrent mixed-methods design was applied to examine the impact of COVID-19 on intrapartum care at 15 public hospitals in the Sidama region. Interrupted times series design was used for quantitative study, and quantitative and qualitative data were gathered between 14 February and 10 May 2022 and analysed separately. The data were integrated in the reporting and interpretation stages using joint display methods, exploring whether the qualitative findings corroborated or contradicted the quantitative findings. 31
Data sources for quantitative study
Quantitative data were extracted from monthly reports on intrapartum care outcomes. A free, open-source software platform called District Health Information Software 2 (DHIS2) is widely used in healthcare facilities for data collection, reporting, analysis and dissemination at both the aggregate and individual levels. According to Arsenault et al., 32 two-thirds of Ethiopia’s health institutions use the DHIS2 to report on institutional births. We extracted routine monthly reported data from DHIS2 on institutional childbirths, assisted vaginal births, caesarean sections, institutional maternal deaths, stillbirths, institutional neonatal deaths and essential drug availability for the 12 months before COVID-19 (March 2019 to February 2020) and the first 6 months of COVID-19 (March to August 2020). The start of the latter period is based on the fact that Ethiopia’s first official case of COVID-19 was reported on 13 March 2020, which we treat as the disease outbreak. The total number of childbirths in the cohort study before COVID-19 (from March 2019 to February 2020) was 24,478, while during COVID-19 19 (from March to August 2020), the total number of childbirths in the cohort study was 11,966, forming a combined final dataset of 36,444.
Outcome variables
Institutional birth, mode of birth, stillbirth, neonatal death and maternal death. Availability of essential medication (fluids, oxytocin, ceftriaxone, magnesium sulphate, calcium gluconate and hydralazine) in hospitals were extracted from each DHIS2 for the period from March 2019 to February 2020 (12 months of data) before COVID-19 and from March to August 2020 (6 months of data) during COVID-19.
Independent variable
COVID-19.
Statistical analysis
The monthly data extracted from hospital DHIS2 reports were cleaned, checked for consistency and exported from Microsoft Excel into Stata version 17 (Stata Corp LLC, a software, College Station, Texas, USA) for statistical analysis. We carried out an interrupted time series analysis (ITSA) to estimate monthly changes in intrapartum care and its outcomes in the first 12 months before COVID-19 and during the first 6 months of COVID-19. A time series comprises continuously recurring sequential observations routinely gathered from populations across various intervals. 33 ITSA is a robust quasi-experimental design used to evaluate a time series of data at the population level; it is commonly employed in studies of public health interventions, policy changes and disease outbreaks over a defined time period.34,35 A single ITSA 36 was implemented for each of two periods: March 2019 to February 2020 (before COVID-19) and March to August 2020 (during COVID-19).
We measured time as a dummy variable taking the value 0 for months before COVID-19 and 1 for months during COVID-19 (the intervention period).
A Poisson regression model 37 was used to determine monthly changes in the incidence rates of institutional childbirth, assisted vaginal birth, caesarean section, stillbirth, institutional neonatal death and institutional maternal death, and availability of essential drugs. A p-value <0.05 and a 95% confidence interval (CI) not including zero were considered to indicate significant differences in intrapartum care and its outcomes from before to during COVID-19.
Study approach for qualitative data
A qualitative descriptive design38,39 was applied to explore how maternity care providers perceived the impact of COVID-19 on intrapartum care in four public hospitals in the Sidama region.
Participant recruitment and sampling techniques
Four public hospitals (including one primary hospital, two general hospitals and one specialised hospital) were chosen based on the caseload maternity care services provided and the order in which COVID-19 cases were initially reported in the Sidama region. Purposive sampling technique was used to recruit staff (midwives, Integrated Emergency Surgical Officers (IESOs), obstetric/gynaecology residents and obstetricians/gynaecologists) who had experience in providing maternity care before and during COVID-19. Before data collection began, written informed consent was obtained from all participants, and permission was secured from the medical directors of each hospital.
Data collection
Face-to-face, in-depth interviews (IDIs) were conducted between 14 February and 10 May 2022, ensuring full compliance with the Ethiopian COVID-19 prevention policy. An interview guide was prepared based on the study objectives. The first author conducted semi-structured interviews in Amharic, Ethiopia’s official language. Each participant was interviewed in their duty room or office while not on duty, and all interviews were digitally audio-recorded. The interview guide was piloted with midwives who were not included in this study, and it contained various open-ended questions concerning (i) the accessibility and availability of maternal and perinatal care, (ii) whether there was a set protocol for providing maternal and perinatal care in the context of COVID-19 and (iii) the availability of medical supplies in maternity care units. After 24 interviews, participant recruitment ceased due to data saturation. Four further interviews were then performed to confirm that no new insights could be uncovered, bringing the total number of participants interviewed to 28 Each interview lasted approximately 30 min.
Data processing and analysis
The first author listened and transcribed the audio recordings iteratively. Simultaneously, bilingual researchers transcribed the recordings and translated transcript into English to check consistency. Transcribed (translated) data were cleaned and imported into NVivo software (version 12 Plus; QRS International Pty Ltd., Melbourne, VIC, Australia) for storage and analysis. The first author read and re-read the transcriptions to gain deep familiarity with the dataset, before then performing reflexivity thematic analysis using Braun and Clarke’s approach, 40 including dataset familiarisation; systematic coding; initiating themes; developing and reviewing themes; refining, defining and naming themes and writing reports. An inductive approach was used to generate codes, subthemes and themes. All authors revised the codes and themes iteratively to ensure accuracy, and all agreed the final themes. This study is reported according to the Standards for Reporting Qualitative Research 41 (Supplemental File 1) to ensure that essential details are reported and the thematic analysis is of sufficient quality. 42
Results: trends in intrapartum care and its outcome in 15 hospitals during the pandemic
In the Sidama region, the monthly estimated incidence rate ratio (IRR) of institutional childbirth decreased by 1.4% in the 12 months before COVID-19 (IRR = 0.986, 95% CI (0.982–0.989); p = 0.0001) and declined more dramatically during the first 3 months of COVID-19, dropping by a further 7.8% (IRR = 0.922, 95% CI (0.879–0.968); p = 0.001). However, overall trends of institutional childbirth in the first 6 months of COVID-19 did not significantly differ between before and during COVID-19 (p = 0.277) (Table 1 and Figure 1). The monthly estimated IRR of assisted vaginal birth (forceps or vacuum) significantly decreased in the first 12 months before COVID-19 (from March 2019 to February 2020) by 7.6% (IRR = 0.924, 95% CI (0.910–0.938); p = 0.0001) then dropped massively during the first 3 months of COVID-19, with a 54.4% decline (IRR = 0.456, 95% CI (0.368–0.566); p = 0.0001). However, overall trends of assisted vaginal birth showed a significant increase of 10.6% during the first 6 months of COVID-19 compared to the 12 preceding months (IRR = 1.106, 95% CI (1.052–1.164); p = 0.0001) (Table 1 and Figure 1). Similar patterns were found for caesarean births: the monthly estimated IRR significantly decreased before COVID-19 by 2.1% (IRR = 0.979, 95% CI (0.970–0.987); p = 0001) and declined further by 15.4% during the first 3 months of COVID-19 (IRR = 0.846, 95% CI (0.756–0.947); p = 0.004), but overall trends during the first 6 months of COVID-19 showed a significant rise of 5.9% in caesarean births from before to during COVID-19 (IRR = 1.059, 95% CI (1.033–1.086); p = 0.0001) (Table 1 and Figure 1).
Trends of intrapartum care and maternal and perinatal outcomes before and during COVID-19 at public hospitals in the Sidama region (March 2019 to August 2020).

Note: * = Significant at 0.05; ** = Significant at 0.01; *** =Significant at 0.001.
CI, confidence interval; COVID-19, coronavirus disease 2019; IRR, incidence rate ratio; NICU, neonatal intensive care unit.

Mean trends of intrapartum care and its outcomes at public hospitals in the Sidama region, Ethiopia, March 2019 to August 2020.
In terms of the monthly estimated IRR, stillbirths significantly decreased by 4.9% in the 12 months before COVID-19 (IRR = 0.951, 95% CI (0.921–0.982); p = 0.003), but did not significantly change during the first 3 months of COVID-19 (IRR = 0.890, 95% CI (0.594–1.333); p = 0.573). In terms of overall trends in the first 6 months of COVID-19, there was no significant difference in stillbirths between the periods before and during COVID-19 (IRR = 1.006, 95% CI (0.915–1.107); p = 0.889) (Table 1 and Figure 2).
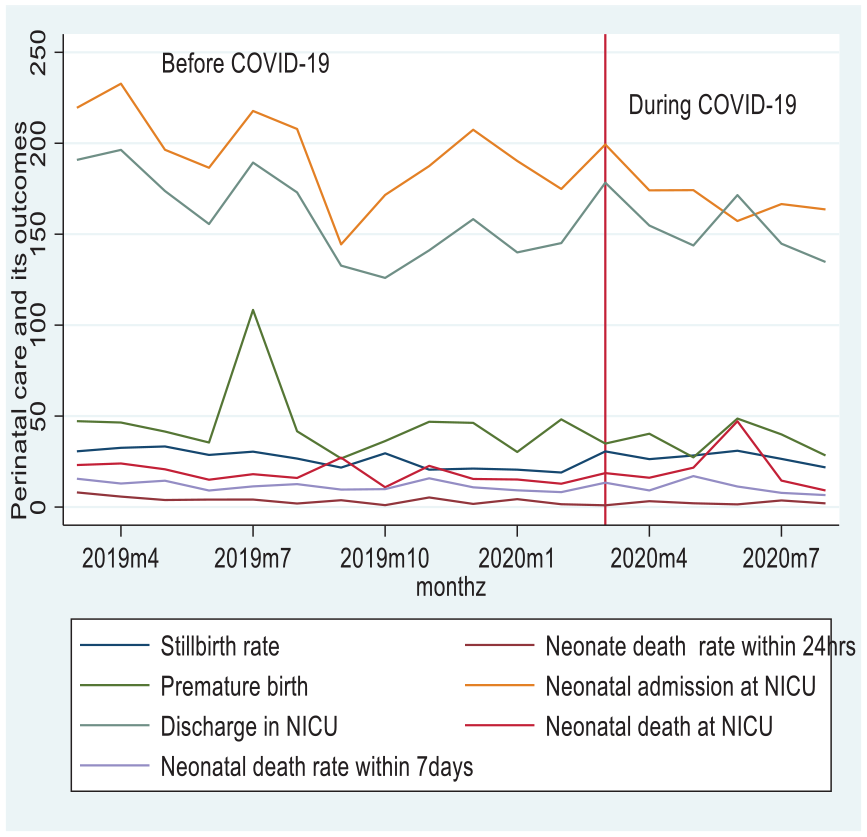
Mean trends of perinatal care and its outcomes at public hospitals in the Sidama region, Ethiopia, March 2019 to August 2020.
The monthly estimated IRR of neonatal deaths significantly decreased by 9.1% in the 12 months before COVID-19 (IRR = 0.909, 95% CI (0.833–0.991); p = 0.032). However, during the first 3 months of COVID-19, the monthly estimated IRR of neonatal deaths did not significantly change (IRR = 0.253, 95% CI (0.062–1.031); p = 0.055). There was also no significant difference between before and during COVID-19 in overall trends during the first 6 months of the pandemic neonatal deaths (IRR = 1.187, 95% CI (0.856–1.647); p = 0.302) (Table 1 and Figure 2).
Views and experiences of maternity care providers of the impact of COVID-19 on the provision of intrapartum care in the Sidama region of Ethiopia
Face-to-face interviews were performed with 28 maternity care providers, comprising 15 midwives, 2 IESOs, 4 obstetric/gynaecology residents and 7 obstetricians/gynaecologists. The inductive thematic analysis of the interview data led to the emergence of three themes: ‘Barriers to providing intrapartum care during COVID-19’, ‘Delays to provision of intrapartum care during COVID-19’ and ‘Inadequate COVID-19 preventive measures’ (Figure 3).

Visual representation of themes.
Barriers to providing intrapartum care during COVID-19
Maternity care providers noted various obstacles to providing intrapartum care. These barriers were categorised into four subthemes, ‘Discrimination against hospital care providers’, ‘Shortage of resources for intrapartum care provision during COVID-19’, ‘Fear of contracting COVID-19 while providing intrapartum care’ and ‘Lack of evidence-based guidelines for intrapartum care provision during COVID-19’.
Discrimination against hospital care providers
Maternity care providers reported that they faced discrimination for providing services in hospitals. Some community members perceived that healthcare providers were a source of COVID-19, due to the high risk of infection in their workplace. The existence of discrimination within the community against healthcare providers has posed challenges for healthcare providers in the provision of services. This discrimination has impeded the provision of optimal care during COVID-19 within the community:
They [the community] consider COVID-19 to be living in the hospital, so they discriminated against healthcare providers . . . House owners ordered healthcare providers not to contact their children . . . There were healthcare providers who were ordered to leave their rented houses. There was a considerable divide between the healthcare providers and the community. (IESO ALTP15)
One midwife reported that after she contracted and recovered from the virus, her landlord displayed a negative attitude towards her family and forbade the midwife’s child from playing with other children in the compound:
The landlord of my home did not have a good attitude towards me; I had not been feeling well when I returned home. I was frightened to meet the community and neighbours. After I contracted and recovered from COVID-19, my child also did not play with the neighbours’ children, and they isolated him; all these things were too challenging at that time for me. (Midwife RMP221)
Shortage of resources for the provision of intrapartum care during COVID-19
Participants frequently reported shortages of beds and medical equipment, such as surgical and disposable gloves, oxytocin, personal protective equipment (PPE), and essential drugs such as antibiotics and normal saline. One midwife stated that ‘medications like Pitocin (oxytocin) ran out in this hospital’ (Midwife MALTP17). Similarly, an IESO recounted:
There was a shortage of gloves and antibiotics such as ceftriaxone and metronidazole in the hospital during COVID-19. Furthermore, there was a shortage of other essential drugs, such as ergometrine and misoprostol, used to manage postpartum haemorrhage. (IESO ALTP14)
Another midwife reported a lack of beds and operating tables in hospitals. Isolating women was impossible, and often, more than three women were put in the same room to labour:
We had shortages of beds in the labour ward. No more than three women were allowed in one room during COVID-19, but it was impossible to implement that. So, we were admitting the women without considering the standards of the COVID-19 prevention policy. (Midwife MRP11)
Reported reasons for such lack of medical equipment included ‘the budget was being transferred to the COVID-19 centre’ (Midwife MRP2) and ‘caesarean sections also increased’ (Midwife MRP3). Another midwife stated:
The majority of medicines could not be found in the hospital, so women had to buy them elsewhere. For example, ampicillin, ceftriaxone, and normal saline might be available one day but not the next. (Midwife MRP6)
Obstetricians noted that medical equipment shortages disturbed their operating theatre schedules. A shortage of blood products was compounded by uncertainty over whether COVID-19 could spread through blood transfusion. Screening for COVID-19 was also challenging as potential donors were reluctant to be tested, and the testing processes were limited. One obstetrician reported that:
In the labour ward, we needed oxygen for resuscitation; at that time, since there was high oxygen consumption, we had a shortage . . . there was [also] a shortage of blood. In blood donation, it was not a settled issue whether COVID-19 was transmitted through blood transfusion or not . . . Second, the blood donor should be screened for COVID-19, and people were [reluctant] to screen for COVID-19. (Obstetrician SRP19)
The lack of equipment and drugs exposed women to higher risks of morbidity and mortality, as one obstetrician described:
The general anaesthetic medicine [vecuronium bromide] was unavailable in the hospital and the city. I do not know whether this was because of the country’s situation [war] or COVID-19 . . . we did procedures without gloves. There were no medicines; one woman died due to the absence of general anaesthetic in the hospital and the city. If general anaesthetic had been given to that woman, she could have been saved . . . ICU beds and mechanical ventilators were filled. There were no extra ventilators in the ICU. COVID-19 brought resource limitations. (Obstetrician SRP21)
Fear of contracting COVID-19 while providing intrapartum care
Maternity care providers highlighted their own fear of contracting the virus and described the challenge this posed to caring for women in labour. In particular, it was difficult for them to communicate with women in the labour ward, a situation compounded by the lack of PPE. One midwife explained as follows:
Communication between women and midwives decreased due to fear of the virus. Since I was closest to the COVID-19-suspected woman, counting her contractions was challenging for me. We lacked enough gloves; we simply wore a mask while we cared for the woman. I feared . . . the virus could transmit through personal contact. (Midwife MAP12)
Midwives also noticed that women regarded hospitals as a source of the COVID-19 virus, and so were afraid to attend to utilise maternity services, even if they experienced complications. There were examples of women refusing to be admitted, not complying with the treatment, and even leaving the hospital after being referred from other health facilities. A midwife explained that:
The community perceived the hospital as an epicentre of COVID-19 and believed that all people who attended/worked at the hospital contracted COVID-19. Women were forced to come to this hospital by being referred from other hospitals, against their choice. This indicated women’s fear of coming here. (Midwife MRP1)
Similarly, IESOs, residents and obstetricians shared their experiences of fear while caring for and treating women during the peak of COVID-19. As one resident observed, ‘When the woman came with complications, maternity care providers feared performing a caesarean section and handed over [her care] to other maternity care providers’ (Resident RPP9). Similarly, an obstetrician recalled:
I remember one woman came because she was labouring. Only some healthcare providers volunteered to participate in the [caesarean] surgery. (Obstetrician SAP22)
Lack of evidence-based guidelines for intrapartum care provision during COVID-19
Maternity care providers cited the absence of evidence-based guidelines for providing intrapartum care in the context of COVID-19. They endeavoured to remained updated by consulting other sources, including other health professionals and, ‘Ministry of Health platforms on social media such as Telegram channels’ (Obstetrician SRP22). During the pandemic, there were no specific hospital guidelines for intrapartum care. Only COVID-19 prevention guidelines for the general population were displayed on the walls, as illustrated below:
I did not know . . . whether the guidelines were available in the hospital [at the senior level]. Our hospital had no guidelines at the bottom [ward level], but brochures and pamphlets cautioning about COVID-19 symptoms were posted on the wall. There were no unique guidelines. (Resident RPP7)
The lack of hospital infection-control protocols specific to COVID-19 resulted in COVID-19-suspected women being treated in the same operating room as other women – a mix that endangered patients:
There was no specific guideline prepared in this hospital. Nevertheless, for COVID-19-suspected or -infected women, operations were done in the same operating theatre used for non-infected women. (Obstetrician SAP21)
Delays to provision of intrapartum care during COVID-19
Within this theme, two subthemes emerged from the qualitative analysis of interviews: ‘Long waiting times’ and ‘Childbirth complications during COVID-19’.
Long waiting times
The lack of PPE during COVID-19 caused delays in triage procedures for women. Because women could not be seen and evaluated immediately, more severe obstetric complications may have resulted. As one midwife stated:
When I was working in triage, one woman arrived in need of immediate attention, and there was a shortage of gloves; then, we had to wait until the family bought gloves; we were observing the woman. Her breathing rate was very high; she had an antepartum haemorrhage. (Midwife MAP12)
Most maternity care providers indicated that if a woman had the virus and/or COVID-19 symptoms, she was not attended to immediately. Women were sent from one hospital to another to receive care, which sometimes cost them their lives. One midwife illustrated this problem:
One COVID-19-suspected woman visited different hospitals and was referred to the COVID-19 centre. The COVID-19 centre operating theatre was not working, and she was referred [to our hospital]. The woman waited a long time in the emergency room and passed away [in this hospital] while in the operating theatre. When we received her COVID-19 result, it was negative. She was neglected in a different hospital and lost her life. (Midwife MRP3)
Similarly, an obstetrician reported that a woman had the virus and had symptoms, but nurses and midwives had not measured her vital signs nor administered medication on time. the obstetrician stated:
Nurses and midwives did not administer medication on time or closely monitor the neonates. I performed a caesarean section without the woman’s vital signs being measured. Convincing them to comply caused a delay from the decision to the operating time, which resulted in a negative outcome for the neonate. (Obstetrician SAP20)
Another obstetrician cited a case in which lack of PPE caused a 2-h postponement to surgery: ‘a woman with an antepartum haemorrhage stayed for about 8 hours without being evaluated’ (Obstetrician SRP19), potentially leading to maternal morbidity or mortality. A further troubling incident was recalled by an obstetrician:
A COVID-19-suspected woman was admitted here while I was on duty, and there was no one to help her. Since I took responsibility and gave the medication, I did the nurses’ tasks . . . decided to operate, and needed PPE to do the procedure . . . they brought two set of PPE with masks; . . . who would wear PPE? . . . We were debating who should wear PPE; after two hours, two extra sets of PPE were brought to us. We did the surgery without sufficient PPE. In the end, her COVID-19 result was negative. (Obstetrician SAP20)
Childbirth complications during COVID-19
Participants reported that neonatal and maternal mortality substantially increased during COVID-19, attributing this to increased births outside facilities. Maternity care providers explained how pregnancy and childbirth complications occurred at home because many women did not attend hospitals during COVID-19: for example, ‘there were sometimes home births that came with retained placenta’, which resulted in ‘maternal and neonatal death’ (Resident RRP7). The situation was described by a midwife as follows:
Homebirths increased, leading to more complications and maternal deaths during COVID-19. Many women had preeclampsia and did not come and manage it early in the hospital due to COVID-19 . . . Last year [2021], at least 6–7 women died due to eclampsia in this hospital, and they had no follow-up, so this is the effect of COVID-19. (Midwife MRP1)
Obstetricians noted that it could be challenging to identify the cause of non-reassuring foetal heart rate patterns in labouring women. There was uncertainty over whether COVID-19 caused foetal distress. Another challenge was a woman arriving at hospital with complications such as ‘uterine rupture’ (Obstetrician SAP22), leading to maternal death. One early neonatal death occurred because ‘the scrub nurse and anaesthetist delayed coming to the operating theatre after the decision was made to perform [a caesarean section]. The neonate could have been saved if the surgery had been done within 30 minutes’ (Obstetrician SRP21). Another obstetrician recalled a different challenging case:
It was a fetal heartbeat abnormality in a woman with confirmed COVID-19. We were confused about whether the abnormality was due to COVID-19 or not and could not prove it. It was hard to decide on doing the surgery. There were more complications with COVID-19-confirmed pregnant women than for other women. (Obstetrician SAP20)
Inadequate COVID-19 preventive measures
Two subthemes emerged within this theme: ‘Inadequate COVID-19 PPE’ and ‘COVID-19 vaccine hesitancy’. Maternity care providers complained that inadequate COVID-19 preventive measures were a persistent problem.
Inadequate COVID-19 PPE
Participants underscored the challenges of promptly providing optimal care while adhering to COVID-19 prevention protocols. These challenges stem from a shortage of PPE and inadequate implementation of COVID-19 prevention measures. Obstetricians noted that ‘a shortage of PPE, gloves, and sanitisers and other physical barriers were widespread in the hospital during COVID-19’ (Obstetrician SRP23). Another illustrated how a lack of PPE could hinder care:
Most of the time, we worked without maintaining COVID-19 prevention protocol. We could not get PPE, so how could we keep to the protocol without PPE? Most of the time, we used only facemasks and gloves. (Obstetrician SRP22)
COVID-19 vaccine hesitancy
Some participants lacked confidence in the efficacy of the COVID-19 vaccine and thought there was no need for vaccination if someone had been infected and recovered. Obstetric /gynaecology residents indicated that they did not get COVID-19 vaccination due to their concern about the vaccine’s effectiveness. The following quotes illustrate these attitudes:
I did not get the vaccination; I did not believe in it because I already contracted and recovered from it. Second, according to a rumour, the vaccine offered protection for a year, and that time had already passed. (Resident RPP10) I did not get the vaccine because no vaccine is accepted uniformly across the globe. The origin of the virus and its source are still unknown. The vaccine administered in our country has an effectiveness rate of 60–70%. (Resident RPP9)
Integrating quantitative and qualitative data with joint display methods
Using a joint display approach, the quantitative and qualitative findings were integrated. According to the quantitative data, the monthly supply of essential drugs did not significantly differ in the 12 months before and the first 6 months during COVID-19. By contrast, the qualitative responses revealed a general shortage of medical supplies during COVID-19. Regarding artificial oxytocics, the quantitative data suggest no significant difference in availability between before and during COVID-19, whereas interviewed healthcare providers perceived that the supply completely ran out. Most participants described how a lack of essential medical supplies – including oxytocin, parenteral antibiotics, disposable and surgical gloves, general anaesthesia medicine, blood and blood products and PPE – resulted in the provision of inadequate care from obstetric triage to the labour ward. They also highlighted that the lack of medical supplies during COVID-19 contributed to delays in care provision that may have contributed to maternal morbidity and mortality. The ability for data to be entered only as binary responses (i.e. available or unavailable) in the DHIS2 form and a lack of complete details regarding quantities of essential drugs may have led to inaccurate reporting of medication supply that rendered the quantitative findings unreliable (Table 2).
Joint display of quantitative and qualitative findings for each theme and subtheme on impact of COVID-19 on intrapartum care, and mixed-methods meta-inferences.

CI, confidence interval; COVID-19, coronavirus disease 2019; DHIS2, District Health Information Software 2; IRR, incidence rate ratio; MPDSR, maternal and perinatal death surveillance and report; PPE, personal protective equipment.
Both quantitative and qualitative findings indicate that the likelihood of women giving birth in an institutional setting did not significantly differ between before and during COVID-19. There was no statistically significant difference in mean monthly institutional birth rates between the two periods (p = 0.277), and maternity care providers reported no change in the volume of women attending the hospital to give birth. Interestingly, though, home births did increase during COVID-19, thought to be because of a lack of labour ward beds, fears of contracting the virus, lack of transport and a shortage and inflated costs of medicines (Table 2). The stable rates in hospital births were thought to be due to a rise in primary health centres sending labouring women to hospitals, due to primary healthcare providers’ fear of contracting the virus. In this study, data were not collected on birth rates at primary health centres and so this cannot be confirmed statistically.
Caesarean birth rates significantly increased in the first 6 months of COVID-19, according to both quantitative and qualitative findings. The latter provided evidence that suboptimal care was associated with fear of contracting the virus and inadequate preventive measures for COVID-19. This fear was believed to have led to decisions to shorten labour by performing interventions without indication, such as amniotomy, induction, augmentation and instrumental and caesarean births (Table 2). The quantitative data confirmed this, demonstrating that caesarean births significantly increased by 5.9% in the first 6 months of COVID-19 (IRR = 1.059, 95% CI (1.033–0 1.086); p = 0.001).
The quantitative and qualitative findings were contradictory regarding institutional maternal deaths. The former suggest that rates of institutional maternal deaths significantly reduced during COVID-19, with a decrease of 21.4% (p = 0.0001). However, interviewees reported an increase in maternal deaths in hospital settings. The discrepancy could be attributable to the reduction of human resources and a decrease in meetings such as maternal and perinatal death surveillance and report and DHIS2. The decreased volume of meetings may have led to further challenges in discussing the causes of maternal death and reporting during the peak of COVID-19, ultimately resulting in underreporting of maternal deaths (Table 2). In addition, at the peak of COVID-19, The DHIS2 unit may have faced a shortage of human resources and a lack of supervision leading to the underreporting of maternal deaths (Table 2).
Inconsistencies were found between quantitative and qualitative findings on institutional neonatal deaths. According to statistical data, neonatal deaths did not significantly differ before and during COVID-19 but were perceived to have increased by participant interviewees. Again, these inconsistencies could have arisen from underreporting as a result of shortage of human resources, and lack of supervision in the DHIS2 unit during the COVID-19 peak (Table 2).
There were no quantitative data available to corroborate or contradict qualitative findings on ‘Fear of contracting COVID-19 while providing intrapartum care’, ‘Lack of evidence-based guidelines for intrapartum care provision during COVID-19’, ‘Discrimination against hospital care providers’, ‘Long waiting times’, ‘Inadequate COVID-19 PPE’ and ‘COVID-19 vaccine hesitancy’, which were all reported by participants as interfering with the provision of intrapartum care (Table 2).
Discussion
The quantitative data show that the monthly incidence rates of caesarean and instrumental births significantly increased during COVID-19. Meanwhile, the qualitative findings indicated that the numbers of maternal and neonatal deaths increased during the first 6 months of COVID-19.
Identified barriers to providing intrapartum care include community discrimination against healthcare providers, fear of contracting COVID-19 while providing care, shortage of resources and a lack of evidence-based guidelines on providing intrapartum care during COVID-19, leading to increased maternal and neonatal complications and deaths. Most maternity care providers reported a shortage of essential medical supplies, consistent with the finding of a study in Southwest Ethiopia. 43 The reallocation of financial resources to COVID-19 prevention, economic crisis and political unrest in the country may have led to an acute shortage of hard currency that affected procurement of essential drugs from abroad, in turn leading to shortages of urgent medical supplies on hospitals.
A lack of medical resources in the obstetric triage system contributed to delays in identifying women’s health status. This was also found in studies conducted in Nigeria and Iran,44,45 which identified deficiencies in supplies and equipment, proper physical space, standard procedures and processes and trained human resources as contributing factors to delays in the obstetric triage process. Obstetric triage with adequate equipment could reduce delays in intrapartum care from 40 to 5 min, hence potentially reducing maternal mortality. 46 Similarly, our qualitative findings indicate that the referral system from low-level to high-level care lacked adequate communication and coordination processes, resulting in care delays that caused maternal and neonatal complications. These findings are consistent with those of a worldwide review mapping the challenges in transport and referral for maternal and newborn health during COVID-19. 26 Maternal and neonatal death rates can be reduced with effective communication between low- and high-level care in referring obstetric emergencies, which helps the receiving health facility understand the referral reason before a woman arrives, and thus ensure the necessary human resources and treatment facilities are promptly available to provide optimal care.47,48
Our quantitative and qualitative findings show that caesarean births significantly increased during COVID-19. This finding is similar to those from studies in Ethiopia, 49 Sierra Leone, 24 Sierra Leone 23 and Iran. 50 Such an increase could lead to more preterm births and stillbirths. 51
Women’s strong demand for caesarean births associated with fear of contracting the virus, 52 and a lack of transport during lockdowns made it challenging to make timely referrals to emergency care units, 51 plausibly explaining the significant increase in caesarean births during COVID-19. Similarly, our findings show that instrumental vaginal births also considerably increased during COVID-19, consistent with a study in the Dominican Republic. 53 Wearing a mask while in labour can impede gaseous exchange and impose an additional burden on the metabolic system. 54 It also makes it difficult for labouring women to express their emotions; compromised communication with maternity care providers may result in greater discomfort and difficulty while giving birth, which could explain the higher incidence of interventions such as instrumental birth.
Our findings demonstrate that long waiting times negatively impacted maternal and neonatal care, which can trigger increased obstetric complications during intrapartum care. These findings align with those of a study in Nigeria, 55 which reported long waiting times in hospitals to access maternal and neonatal care. Lack of PPE, medical supply shortages, depleted human resources, and fear of contracting the virus could all have contributed to increased waiting times for accessing maternal and neonatal care during COVID-19. In turn, our findings indicate increases in complications during childbirth as a result of delays in receiving optimal intrapartum care. Admittedly, our quantitative findings indicate that institutional maternal deaths significantly decreased during COVID-19 during its first 6 months. However, the interviewed maternity care providers reported that maternal deaths increased during COVID-19. Contrary to our quantitative data, a global systematic review and meta-analysis demonstrated that maternal mortality increased in LMICs. 28 However, an earlier review in West Africa 56 reported that maternal mortality decreased during the Ebola outbreak. The statistical decrease in maternal deaths in our study could be attributed to underreporting, reporting errors and/or increased numbers of home births, for which there was no reporting process. 57
Study participants indicated that a shortage of blood and blood donations affected intrapartum care during the pandemic. This was also found in studies in Latin America 58 and the Eastern Mediterranean region 59 . In LMICs, shortages of blood products have a real impact on intrapartum care, increasing maternal morbidity and mortality as a result of obstetric haemorrhaging. 60
Participants reported inadequate COVID-19 preventive measures across the hospitals. Ineffectiveness in COVID-19 prevention due to supply shortages, increased demand, misuse and financial crisis was also found to impact medical supplies in Pakistan 61 and Nigeria. 44 Mistrust of the COVID-19 vaccine was expressed by maternity care providers in this study. Vaccine hesitancy may have stemmed from healthcare providers’ concerns about potential long-term sides in relation to their future pregnancies and other medical complications. This vaccine hesitancy could also be attributed to efficacy uncertainty, inadequate vaccine trials prior to human administration. 62
Strengths and limitations of the study
The strength of this study is that we employed a concurrent mixed-methods approach integrating quantitative findings on intrapartum care and its outcomes with the experiences and perceptions of maternity care providers. We included 15 public hospitals in Sidama that provide caesarean births. Through IDIs, we explored how various maternity care providers perceived access to and uptake of intrapartum care during COVID-19.
Conversely, our study has several limitations. It is possible that the DHIS2, our source of administrative data, contained errors. The data may have been over- or under-reported, there were no population-level denominators, and we did not estimate maternal and perinatal care indicators at the community level, where there may have been increased numbers of maternal and neonatal deaths. Moreover, the pandemic could have further reduced the accuracy of health management information system (HMIS) reporting. Furthermore, there might be a potential for selection bias among participants, and the themes identified and interpreted may be influenced by the researchers’ perspectives, which could lead to biased conclusions. As we primarily focused on hospital data, future studies should evaluate intrapartum care and its outcomes at the primary health centre level.
Conclusion
Our study’s findings indicate that barriers to providing intrapartum care, delays to provision of intrapartum care, and inadequate COVID-19 preventive measures led to considerable increases in neonatal and maternal deaths. To sustain and improve the positive trends in intrapartum care experienced before COVID-19, targeted interventions are needed that ensure the availability of medical supplies during a pandemic. The responsible bodies should prepare and equip obstetric triage systems and labour wards with PPE and equipment for births and caesarean sections to avoid delays in intrapartum care during present and future pandemics. Finally, future research is needed to investigate the long-term impact of COVID-19 on women and babies.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241296614 – Supplemental material for Impact of COVID-19 on intrapartum care at public hospitals in the Sidama region, Ethiopia: A mixed-methods study
Supplemental material, sj-docx-1-whe-10.1177_17455057241296614 for Impact of COVID-19 on intrapartum care at public hospitals in the Sidama region, Ethiopia: A mixed-methods study by Zemenu Yohannes Kassa, Vanessa Scarf, Sabera Turkmani and Deborah Fox in Women’s Health
Footnotes
Acknowledgements
First and foremost, we would like to express our gratitude to study participants, health bureau officials, HMIS data managers and hospital chief executive directors for cooperating during the study. The first author would like to thank the Royal Society of Tropical Medicine and Hygiene for funding the study.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.