
Abstract
Background:
The COVID-19 pandemic, drought and internal conflict have worsened Ethiopia’s already weak healthcare system. Antenatal and intrapartum care are especially prone to interruption under these circumstances.
Objective:
To explore women’s experiences receiving antenatal and intrapartum care during the pandemic.
Design:
A descriptive qualitative approach was utilised.
Methods:
We conducted in-depth interviews with 17 women and held 4 focus group discussions with women who gave birth at 4 public hospitals during the pandemic. A study was conducted at four public hospitals in the Sidama region of Ethiopia, during which data were collected from 14 February to 10 May 2022. Thematic analysis was performed to generate themes.
Results:
The peak of the COVID-19 pandemic in Ethiopia presented several barriers to access and uptake of antenatal and intrapartum care at public hospitals. Four themes and 10 subthemes emerged from the thematic analysis. The themes were ‘Barriers to maternity care uptake during COVID-19’, ‘Shortage of resources during COVID-19’, ‘Delays in maternity care uptake during COVID-19’ and ‘Mistreatment of women during maternity care during COVID-19’. The subthemes included ‘Fear of contracting COVID-19’, ‘People in the hospital neglecting COVID-19 prevention’, ‘Women losing their job during COVID-19’, ‘Shortage of beds in the labour ward’, ‘Shortage of medical supplies’, ‘Delays in seeking care’, ‘Delays in receiving care’, ‘Complications during childbirth’, ‘disrespectful’ and ‘suboptimal care’.
Conclusion:
The findings of this study underscore the impact of COVID-19 on antenatal and intrapartum care, leading to delays in seeking and receiving care due to reduced rapport, resource shortages, companion restrictions, disrespectful care and suboptimal care. These factors contribute to increased obstetric complications during COVID-19. It is imperative for policymakers to prioritise essential resources for antenatal and intrapartum care in the present and future pandemics. Moreover, healthcare providers should maintain respectful and optimal care even amid challenges.
Plain Language Summary
The COVID-19 pandemic has posed a significant challenge in seeking and receiving care of antenatal care and institutional childbirth. Women could experience delays in booking antenatal care appointments, postponing antenatal care visits, and facing delays in receiving care at hospitals, which has disrupted their access to routine antenatal care and institutional birth during the pandemic. This study highlights a range of barriers that hinder access to and utilisation of antenatal care and institutional birth, including lack of transport, shortage of resources, fear of contracting the virus, companion restrictions, disrespectful care and suboptimal care that leads to increased obstetric complications during COVID-19. This study provides recommendations for policymakers to prioritise resources and enhance respectful and optimal care for pregnancy and institutional birth to lessen the indirect impact of present and future pandemics on pregnant women and their unborn babies.
Introduction
The primary strategy for reducing maternal and newborn mortality in low- and middle-income countries (LMICs) is providing quality antenatal care (ANC) and intrapartum care. 1 Despite tremendous progress over the past two decades, a newborn or pregnant woman still dies every 11 s due to preventable pregnancy and birth complications. 2 It thus seems unlikely that developing countries will achieve the sustainable development goal (SDG) targets for reduced maternal and neonatal mortality by 2030. 2
In 2017, 66% of global maternal deaths occurred in sub-Saharan Africa, with an estimated 542 maternal deaths per 100,000 live births. The primary complications, accounting for nearly 75% of all maternal deaths, were severe bleeding, infection (puerperal sepsis), high blood pressure during pregnancy (preeclampsia), pregnancy complications from birth and unsafe abortion.2,3
Ethiopia has made great strides in reducing maternal and newborn mortality during the last two decades 2 : the maternal mortality rate declined from 865 per 100,000 live births to 401 between 2005 and 2019, while the neonatal mortality rate dropped from 39 per 1,000 live births to 30 during the same period. 2 A significant reduction in maternal and neonatal mortality could occur by prioritising the enhancement and expansion of ANC coverage. This is largely attributed to the increased presence of skilled birth attendants throughout the country. 4 Considerable work is still required to meet the relevant SDG targets by 2030. 5 Early detection and management of pre-existing pregnancy-related complications is essential for reducing maternal and neonatal morbidity and mortality.3,6 This requires providing all pregnant women with high-quality ANC and skilled birth attendants.7,8
In combination, the COVID-19 pandemic, drought and internal conflict have worsened Ethiopia’s already weak healthcare system. 9 In the early stage of COVID-19, the Ethiopian government’s emphasis was placed on containing the spread of the virus by implementing measures such as school closures, reducing passengers on public transport by half, lockdowns, recommending the population to stay at home and closing non-essential services, 9 which considerably impacted on the provision of ANC and skilled attendants at birth. 10 Early evidence indicates that COVID-19 interrupted the uptake of ANC and skilled birth attendants in LMICs, 11 while also directly contributing to an increase in pregnancy complications among women who test positive for COVID-19. 12
Existing qualitative studies provide little information on women’s experiences and perceptions of ANC and intrapartum care during COVID-19 in Ethiopia. The insights from the qualitative findings in this study may inform the restructuring, adjusting and restoring of services in present and future pandemics, seeking to fill the existing research gap.
Methods
Study design and setting
We conducted a descriptive qualitative study 13 to explore women’s experiences and perceptions of receiving ANC and intrapartum care during COVID-19 at four public hospitals in the Sidama region. This study took place from 14 February to 10 May 2022 as part of a larger mixed-methods investigation of the impact of COVID-19 on maternal and perinatal care in the Sidama region, Ethiopia. Further details about study settings can be described in the following project. 14
Study participants
The four hospitals (Aleta Wondo Primary Hospital, Leku General Hospital, Adare General Hospital and Hawassa University Comprehensive Specialised Hospital) were purposively selected as those in which the first cases of COVID-19 were reported in the region. Women were purposively selected based on the following inclusion criteria: at least 18 years of age, availability, informed consent to participate and recently having given birth in the public hospital in the Sidama region during the COVID-19 pandemic. Women who experienced neonatal loss were excluded from the focus group discussions (FGDs) but included in the in-depth interviews (IDIs).
The first author recruited two research assistants with suitable qualitative research experience, then trained them on the study’s objective and how to recruit participants.
Together, the first author and research assistants explained the study’s purpose to each hospital’s medical director, chief executive director and maternity ward head to secure their agreement for collecting data from clients. The research assistants invited eligible women to participate in IDIs or FGDs and gave them detailed information on the purpose of the study. Women who were interested in participating were given personal information sheets to read and sign to confirm their informed consent. The research assistants organised the data collection and gave participants information on how long the IDI or FGD would take. Participants were compensated for their travel expenses and time spent engaging in IDIs or FGDs. Data saturation appeared to be reached after 15 IDIs as no new insights arose, and the information was repeated. Two additional IDIs were then conducted to verify data saturation. Seventeen IDIs and four FGDs were conducted with women, each containing six or seven women.
Data collection
Semi-structured interviews were conducted with women through IDIs and FGDs adhering to the Ethiopian COVID-19 preventive and control rule. An interview guide was prepared by reviewing different literature on the impact of the Ebola virus disease and COVID-19 on maternal and perinatal care. The interview guide contains the following topics: maternal and perinatal care during the pandemic, accessibility and availability of hospital supplies and the interaction between women-healthcare providers and communications during COVID-19. The interview guide was approved by the Ethics Committees at UTS HREC and IRB Hawassa University (Supplemental Appendix 1). The first author, who is fluent in the local language, Amharic and English, conducted IDIs and FGDs. The audio recordings were used for IDIs and FGDs. The IDIs lasted 30 min, and FGDs also lasted 60 min. Data were collected from 14 February to 10 May 2022.
This study is reported according to the Standards for Reporting Qualitative Research 15 and to ensure that the essential parts are reported and the quality of reflexivity thematic analysis assessed. 16
Data analysis
Data were transcribed verbatim from the audio recordings of IDIs and FGDs in Amharic and English. Data transcriptions were imported to NVivo software (version 12 plus; QSR International Pty Ltd, Vic, Australia. Data were analysed using Braun and Clarke’s 17 reflexivity thematic analysis that follows six phases: data familiarisation and writing familiarisation notes; systematic coding; generating initial themes from coded data; developing and reviewing themes; refining, defining and naming themes and writing the report. Inductive analysis was used to derive the data’s codes, subthemes and themes. The codes, subthemes and themes were reviewed and approved by all authors.
Theoretical framework
Theories and conceptual frameworks have a crucial role in research, providing a method to explain and interpret the phenomenon under study. 18 In this study, the three delays framework helped identify the challenges in seeking, reaching and receiving maternity care. 19 The social ecological framework provided an approach to exploring how human behaviour was influenced by multiple domains, including at individual, family, community, health facility and government levels. 20 By incorporating the concepts of three delays into the social ecological framework to create what will be referred to herein as the hybrid framework, we were able to identify and address delays at a range of levels of influence, as demonstrated in Figure 1.

Visual representation of the hybrid framework in relation to the impact of COVID-19 on maternal and perinatal care in LMICs.
Results
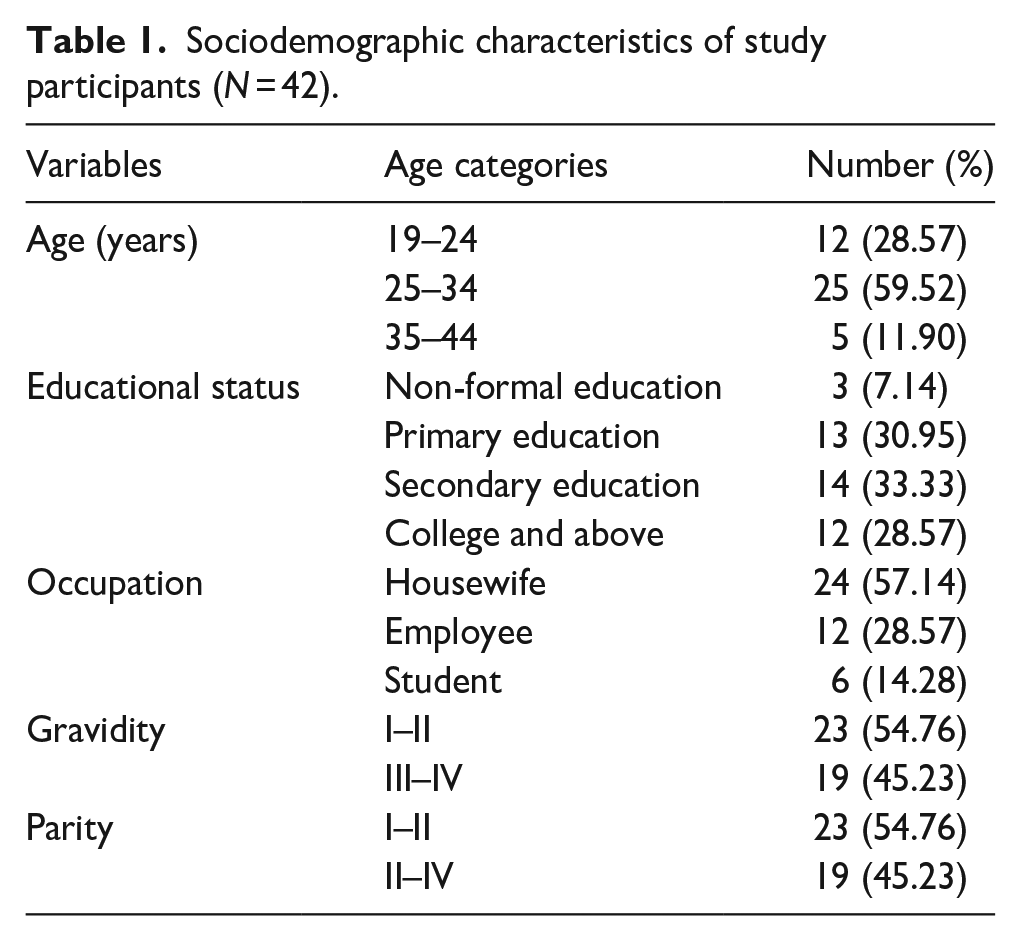
The minimum and maximum ages of study participants were 19 and 37, respectively; over half were aged 25 to 34. One-third of the participants had completed secondary education, and over half were housewives (Table 1).
Sociodemographic characteristics of study participants (N = 42).
Four themes were constructed from the thematic analysis, and these are displayed in Figure 2: within these themes, 10 subthemes were identified: ‘Fear of contracting COVID-19’, and ‘People in the hospital neglecting COVID-19 prevention’ are subthemes under the theme, ‘Barriers to maternity care uptake during COVID-19’. ‘Shortage of beds in labour wards’, ‘Shortage of medical supplies’ and ‘Women losing their jobs during COVID-19’ are subthemes under the theme ‘Shortage of resources during COVID-19’. ‘Delay in seeking care’, ‘Delay in receiving care’ and ‘Complications during childbirth’ are subthemes under the theme, ‘Delays in maternity care uptake during COVID-19’. ‘Disrespectful care’, and ‘Suboptimal maternity care’ are subthemes under ‘Mistreatment of women during maternity care during COVID-19’ (Figure 2).
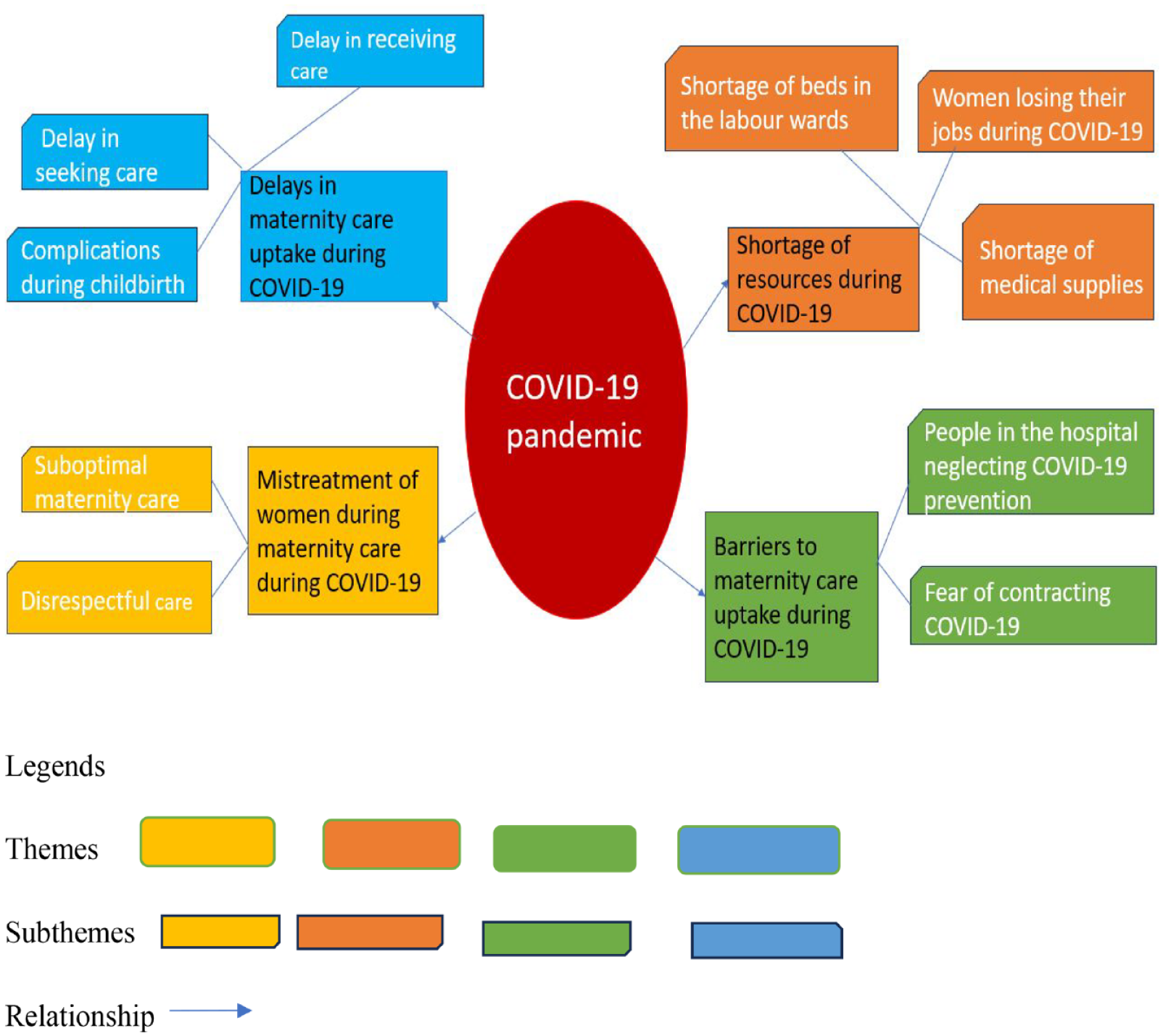
Visual representation of thematic analysis.
The visual presentation of findings on women experiences on ANC and intrapartum care during the pandemic is depicted in Figure 3, using the hybrid framework.

Visual presentations of findings in the hybrid framework.
Barriers to maternity care uptake during COVID-19
This theme incorporates women’s experiences of ANC during COVID-19 and the effects on their ANC follow-up. Two subthemes were identified: ‘Fear of contracting COVID-19’ and ‘People in the hospital neglecting COVID-19 prevention’.
Fear of contracting COVID-19
Participants raised the issue of how COVID-19 fear affected their uptake of ANC. They were reporting their own activities, which included missed ANC appointments and leaving the hospital without receiving the necessary care. Women were concerned that they would catch the virus via physical contact with healthcare providers while being assessed in the hospital. Similarly, participants reported not using public transport to travel to the hospital for ANC follow-up due to fear of contracting the virus. These issues are exemplified by the following quotes:
‘Based on the order of arrival, healthcare providers allocated numbers to the women for ANC appointments. . .Healthcare providers asked to measure my vital signs; however, I declined and went home to avoid getting the virus in the clinic. Due to my fear of COVID-19, I frequently skipped ANC follow-up visits’ (Woman F2R1). ‘I used to wear a mask during COVID-19 because I feared getting close to people, like in a taxi. . ., To maintain physical distance, I walked rather than travel by taxi to a health facility for an ANC follow-up’ (Woman WAD4).
Participants reported ‘living like prisoners’ and having no interactions with their neighbours; some did not leave their homes for any reason, including ANC follow-up, during the peak of the pandemic. As one woman recalled:
‘We could not go out anywhere because we were afraid and lived like prisoners. I closed my door and prayed to God. We did not go to the others’ homes, and others did not come to our homes’ (Woman F4R5).
People in the hospital neglect COVID-19 prevention
Participants expressed concerns about the hospitals’ lack of adherence to COVID-19 prevention measures during the pandemic. They reported that many women and over half of the healthcare providers they encountered were not wearing facemasks, especially in the medical records storage unit. Participants also noted that the postnatal waiting area was frequently overcrowded with women and their companions, creating an environment in which the virus could easily spread. As a result of these conditions, women were hesitant to seek maternity care during COVID-19. The following quotes are illustrative:
‘More than half of healthcare providers who worked in the medical record storage unit were not wearing facemasks, while it was crowded with people getting medical record folders’ (Woman F1R6). ‘. . . . The birthing room did not receive adequate attention to COVID-19 prevention measures. The number of clients was high, and none were using hand sanitiser or facemasks, and the room was not clean’ (Woman WAD5).
Shortage of resources during COVID-19
This theme encapsulates women’s experiences of intrapartum care during COVID-19 and the effects on their maternity care. Three subthemes were identified: ‘Shortage of beds in labour wards’, ‘Shortage of medical supplies’ and ‘Women losing their jobs during COVID-19’.
Shortage of beds in the labour wards
Most IDI and FGD participants raised significant concerns over the shortage of beds in labour wards during COVID-19. This shortage may have been a consequence of hospitals implementing the COVID-19 prevention strategies at COVID-19 peak, such as reserving rooms for isolating suspected cases and limiting the number of women per room. As a result, women had to spend much time travelling from hospital to hospital searching for available beds, which was especially difficult for those in labour, particularly if experiencing leakage of amniotic fluid. Two women described their experiences as follows:
‘There was a heavy leakage of amniotic fluid . . . . When I entered, they never helped me. I shouted at them, “Please help me!” Then they responded, “We do not have a bed, so you should go to another hospital.” . . . . Then, I said, “So give me an ambulance to go there.” They said, “If we provide you with an ambulance, they will send you back, so you had better use a Bajaj.” I went to another hospital by Bajaj and gave birth’ (Woman F4R1). ‘. . . . I phoned my catchment area hospital to request a bed as well as another hospital, and they both replied that no beds were available, so I called a third hospital; again, there was no bed. I was sad’ (Woman WR6).
Shortage of medical supplies
Most participants in the FGDs and IDIs reported that they had purchased their own essential medical supplies for birth. Before COVID-19, hospitals had provided all necessary medical supplies for labouring women. Participants mentioned that they were not informed about the need to purchase medical supplies for labour, and believed that the hospitals would continue to provide all necessary supplies free of charge. The following experiences are illustrative:
‘I even purchased sutures and gloves, and we had to purchase all the medicines. Although maternal healthcare was free of charge previously, this was not the case in this hospital. I did not know the reason; I spent over 4,000 Ethiopian birr [$80USD] to buy medicine during this birth’ (Woman WALT19).
Participants mentioned that healthcare providers even instructed them to buy several medical items that were not necessary during birth, causing them to incur large expenses. Specifically, women described the following:
‘A healthcare provider ordered me to buy medicine, and my family purchased the necessary medical supplies for my birth. . .Healthcare providers took my drugs without my consent; when I asked them about it, they denied doing so. It was unacceptable for them to take my expensive medication’ (Woman WAD10).
Women losing their jobs during COVID-19
Participants indicated that travel restrictions and business suspensions during COVID-19 caused many women to lose their jobs, especially in hotels, cafes and grocery stores where most worked. This impacted their ability to meet daily financial demands, such as transport expenses for follow-up appointments and the cost of meeting their children’s basic nutritional needs. Women explained their circumstances:
‘COVID-19 made us jobless, especially those who worked in hotels as managers, cashiers, hostesses, etc. Our jobs were suspended for about six months. Therefore, COVID-19 impacted our lives, jobs, and social interactions’ (Woman F3R1). ‘It was difficult for us during COVID-19. It restricted people’s interaction with colleagues, especially given the challenges of finding employment. We were unable to feed our children. We could not find work, and our children’s schools were closed’ (Woman F2R5).
The pandemic affected the lives of participants in various ways, one woman describing the situation by saying ‘losing our job and spending the whole time inside the home, and my husband was a mason, so there was no work for him’ (Woman F2R4). These challenges disrupted their daily routines and posed difficulties in accessing public transport during emergencies. Women explored these impacts:
‘Even if the labour pain is complex and needs transport, it was difficult for labouring women to access transport such as mini-taxi and Bajaj during COVID-19. . . . if you begged neighbours who had cars, they said, “We have no fuel”’ (Woman F2R6).
Delays in maternity care uptake during COVID-19
This theme incorporates women’s experiences of delays in antenatal and intrapartum care during COVID-19. Within this theme, three subthemes were identified: ‘Delay in seeking care’, ‘Delay in receiving care’ and ‘Complications during childbirth’.
Delay in seeking care
Participants acknowledged the importance of scheduling ANC appointments within 3 months of becoming pregnant, but many disclosed that they delayed initiating their ANC appointments during COVID-19. One woman said, ‘I started the follow-up after 5 months and 15 days of conception/pregnancy because I was afraid of COVID-19’ (Woman WAD3). Such concerns led to lower ANC uptake during COVID-19. Another woman reported similar issues:
‘I put off obtaining my ANC follow-up for three months after the pregnancy was confirmed because it was too terrible to go to the hospital. People then pressured me to double-check because I had already confirmed my pregnancy when I started my follow-up, it was a terrible time because of COVID-19’ (Woman F2R2).
Likewise, participants reported calling for an ambulance long after the start of labour pain, leading to some giving birth in the ambulance en route to a hospital. On arrival, women were met with expressions of disappointment from healthcare providers that they had not come sooner. Women illustrated this experience as follows:
‘We called an ambulance, but it took longer than expected to arrive, so we found alternative transport to the hospital. . .my husband pleaded with his colleague to give us a car, and during the trip, I gave birth, and my colleague received the baby. . . . healthcare providers brought a birthing set and cut the umbilical cord in the hospital parking area’ (Woman F3R2).
Delay in receiving care
Most participants complained that staff at the medical records storage unit did not provide a prompt service in transferring their records, preventing women from accessing ANC and intrapartum care on time. As one woman recalled:
‘When I went there [the medical records storage unit] during my ANC appointment, they were not interested in acting quickly. In short, there was a delay in transferring my medical records to the ANC clinic’ (Woman F2R3).
Participants also complained that when healthcare providers prescribed ultrasound scanning for their pregnancies, these scans were not checked at the requested time:
‘My physician told me to have an ultrasound scan to check the fetus’s health. But I did not get an ultrasound until the five-month mark. . .I begged him, but he insulted me and left the office without performing the ultrasound. “I cannot check it right now,” he said. Fortunately, I got this service after a week’ (Woman WR6).
Complications during childbirth
Participants indicated that a lack of beds in labour wards led to women having to give birth on a metal floor outside the ward, receiving suboptimal care. This made it more challenging to manage the birth of the placenta, leading to women experiencing heavy bleeding. Participants also encountered difficulty obtaining blood for transfusion, as there was no blood in the hospital or blood bank during COVID-19. Women described the consequences:
‘The healthcare providers did not help me at the right time during childbirth. . .I had lost a lot of blood from my body, and . . . . I needed blood. My blood type is O+, I suffered a lot until I got the transfusion. I was even convulsing. Finding this blood was difficult; they looked for it in different hospitals’ (Woman F4R3). ‘I gave birth on a metal floor. There was excessive bleeding. Then, another female healthcare provider came and checked me. She examined me and noticed that half of the placenta was left in the uterus. She was shocked. . .She searched for it, and finally removed it’ (Woman WAD4).
Mistreatment of women during maternity care during COVID-19
The final theme incorporates women’s experiences of mistreatment during maternity care during COVID-19. Two subthemes were identified: ‘Disrespectful care’ and ‘Suboptimal maternity care’.
Disrespectful care
Participants noted that healthcare providers only offered ANC follow-up to pregnant women who lived close to the hospital, refused to provide services to residents of other areas and did not give care to pregnant women based on their order of arrival. Some healthcare providers appeared to offer care based on their relationships with pregnant women, rather than who had been waiting longest. This caused some women to leave the public hospital and turn to private healthcare for ANC follow-up. Women told how they were affected by this behaviour:
‘I came from another town to this hospital to start the follow-up, but a healthcare provider told me to return to “that town” for an ANC follow-up. . . . I told them there was no medical equipment at “that town health centre” as they had been stolen. She did not listen to us. Then, we went to the private health centre and started the follow-up there’ (Woman WAD10). ‘The maternity care unit staff exhibit ugly behaviours; they do not treat all women equally, and they prioritise according to their relationships with women’ (Woman F1R5).
Participants also reported being mistreated when receiving intrapartum care: healthcare providers insulted them, used abusive language and abandoned women in the labour ward. The following examples are illustrative:
‘Though they do not provide medication, they should at least treat and speak to women appropriately. I heard healthcare providers saying, “Go away, woman, we do not have a bed.” Such women may lose hope and stop going to the hospital’ (Woman WAD4). ‘Sometimes, healthcare providers leave us alone. . . They should have been there to encourage us. it was my first pregnancy, so I needed an assistant around me, but they were not there. In addition, they left a newborn alone’ (Woman WALT21).
Suboptimal maternity care
Participants understood that the health of a pregnant woman and her unborn baby depends on optimal maternity care. They complained that healthcare providers repeatedly conducted digital examinations and often ruptured the amniotic sac, causing the release of fluid and distress to the foetus. Participants also noted that healthcare providers did not pay sufficient attention during procedures to avoid unforeseen outcomes during those procedures. Examples of their experiences are as follows:
‘They counted down the number of minutes remaining, commenting on whether the labour was long or short. However, they were not concerned about whether all my amniotic fluid had leaked due to repeated digital examinations, meaning the fetus could not move back’ (Woman WAD10). ‘Healthcare providers talked and laughed with one another in person and on the phone while doing surgery. I was upset about their activities because I was semiconscious when they operated. They should feel responsible while carrying out this work: human life is in their hands’ (Woman WAD5).
Another woman felt that the carelessness of some staff with equipment demonstrated disrespect towards their profession, and being allowed a family member to be present might have helped protect her:
‘One family member should be allowed to enter the birthing room, but this was not there for me and others. It would be good. . ., in case healthcare providers may use the equipment for more than one woman. So, the family member may help to control this’ (Woman WAD11).
Participants highlighted the importance of healthcare providers maintaining infection prevention strategies to reduce the transmission of COVID-19 and other hospital-acquired diseases. Some claimed that when they underwent physical examinations and gave birth, the hospital did not clean beds ready for them. Women’s experiences included the following:
‘The cleaner was not around in the labour ward, and I encountered a challenge because the bed was not ready. . .it needed to be cleaned promptly’ (Woman F1R5). ‘During ultrasound scanning, healthcare providers did not use hand rubs and sanitiser before touching a woman’s abdomen. Healthcare providers did not rub the examination bed with sanitiser before the woman laid down’ (Woman WR1).
According to participants, healthcare staff pressured women to use family planning before discharge and refused to provide discharge letters unless they agreed:
‘Healthcare providers told women to get discharge papers from the hospital; it is mandatory to take contraceptives. Giving a contraceptive to a woman who has a newborn is not good because it might impact her breast milk production and her health. It might be suitable for some women but not others’ (Woman F4R5).
Finally, participants asserted that healthcare providers should always obtain consent before drawing blood samples and performing an episiotomy. Women complained that inexperienced first-round apprenticeship students [intern] should not permitted to undertake any procedure related to birthing. A woman voiced her indignation:
‘Students [intern] should not be allowed to apply stitches and do other activities with women. They might hurt women when suturing. One of them tried to take blood from me, he struggled a lot to find a vein, even though it was clearly visible. Finally, someone else took the blood’ (Woman WAD11).
Discussion
This study explored women’s experiences of accessing and utilising ANC and intrapartum care in public hospitals in Ethiopia during COVID-19. Women need to have access to ANC and intrapartum care; however, COVID-19 has made access and uptake of these services challenging. Our findings indicate that women were hesitant to seek ANC early and often delayed their appointments due to fear of contracting COVID-19. Our findings are similar to a study conducted in Sierra Leone 23 which found reduced uptake of non-COVID-19 services during the first wave of COVID-19, due to fear of contracting the virus. As illustrated in Figure 3, the hybrid framework depicts a multifaceted interaction that substantially impacts the individual seeking care during COVID-19. Fear of contracting the virus, due to media encouragement to stay home led to postponing and cancelling appointments. As a result, there has been a decrease in the rate of ANC attendance during COVID-19.
Our study revealed that women reported instances of carelessness regarding COVID-19 prevention by some pregnant women, attendants and healthcare providers. They, for instance, ignored physical distancing measures and failed to wear face masks while waiting in line for medical record folders and services. Under these circumstances, some women decided to leave the hospital without receiving the essential care to measure their fundal height, weight and blood pressure and undergo medical exams and laboratory tests during the pandemic’s peak.
In 2016, the WHO recommended 24 that all women attend at least eight antenatal contacts with maternity care providers, accessing various services, including measuring body weight, blood pressure, fundal height and other physical examinations. They should also receive counselling, iron-folic acid supplements and laboratory tests. Our findings are similar to a study in India, 1 which demonstrated that a decline in ANC and intrapartum care access and uptake could be driven by mistrust of the public health system and functions during the first wave of COVID-19.
Hospitals offer ANC and birthing services and free medical supplies to all women, in an effort to enhance the coverage of ANC and institutional childbirth and reduce maternal and newborn mortality. However, a shortage of medical supplies, rooms and beds in labour wards was a common problem during COVID-19. These issues could have occurred due to hospital resources having been shifted to the provision of a COVID-19 prevention and recovery centre. Consequently, pregnant women faced challenges accessing intrapartum care during COVID-19.
COVID-19 caused the loss of jobs, which led to women being unable to pay for transport or the materials needed for pregnancy care and childbirth. Evidence from Nigeria 25 supports our findings that the overstretched health system and increased medical costs could be difficult to access ANC and intrapartum care during COVID-19.
As demonstrated in our findings, many women experienced delays in seeking and receiving care for ANC and intrapartum care during COVID-19, leading to complications like excessive bleeding during childbirth. Delay in seeking care could have happened due to transport issues, and their ambivalence about going to the hospital. Women who arrived at the hospital reported delays in getting ANC and intrapartum care because of a staffing and medical supply shortfall, mainly because they had to wait a long time to obtain medical record folders and ultrasound services. Consistent with our study, a study in London 26 explored delayed decisions to seek care and delays in receiving care that could have happened during COVID-19. Delays in seeking and receiving care can be affected by numerous complex factors at the individual, community and hospital levels. These factors include unemployment, fear of acquiring the virus, shortage of beds in labour wards and shortage of medical supplies, as displayed in the hybrid framework in Figure 3.
Disrespectful and suboptimal care can reduce the quality of ANC and intrapartum care. 27 In this study, women frequently experienced disrespectful and suboptimal care during COVID-19, which may have decreased the quality of ANC and intrapartum care. Our findings correspond with other research28,29 demonstrating that COVID-19 decreased emotional and physical support, restricted companionship during childbirth, compromised standards of care and greater exposure to unnecessary interventions during ANC and intrapartum care.
The strength of our study is that we conducted qualitative interviews and focus groups with a large sample of 42 women, to explore their experiences with ANC access and intrapartum care during COVID-19. Semi-structured interviews allowed women to speak openly about their experiences receiving ANC and intrapartum care during COVID-19 and its challenges. Limitations include that these findings may not be generalisable of women’s experiences in other settings, and that we did not include the experiences of women receiving ANC and intrapartum care in private health facilities during COVID-19.
Conclusion
The findings of this study underscore the impact of COVID-19 on antenatal and intrapartum care, leading to delays in access and uptake due to reduced rapport, resource shortages, companion restrictions and suboptimal care. These factors contribute to increased obstetric complications during COVID-19. It is imperative for policymakers to prioritise essential resources for antenatal and intrapartum care in the present and future pandemics. Moreover, healthcare providers should maintain respectful and optimal care even amid challenges.
Supplemental Material
sj-pdf-1-whe-10.1177_17455057241274898 – Supplemental material for Women’s experiences of receiving antenatal and intrapartum care during COVID-19 at public hospitals in the Sidama region, Ethiopia: A qualitative study using the combination of three delay and social-ecological framework (hybrid framework)
Supplemental material, sj-pdf-1-whe-10.1177_17455057241274898 for Women’s experiences of receiving antenatal and intrapartum care during COVID-19 at public hospitals in the Sidama region, Ethiopia: A qualitative study using the combination of three delay and social-ecological framework (hybrid framework) by Zemenu Yohannes Kassa, Vanessa Scarf, Sabera Turkmani and Deborah Fox in Women’s Health
Footnotes
Acknowledgements
Authors acknowledge study participants, health bureau officials, research assistants and hospital chief executive directors for cooperating during the study. The first author also acknowledges the Royal Society of Tropical Medicine and Hygiene for funding the study.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.