
Abstract
Introduction:
Intimate partner violence is one of the most common psychological, physical, and sexual assaults toward women which suit the entire life of women, and nowadays, the magnitude accelerates due to coronavirus pandemic. Hence, this study was aimed to examine the prevalence of intimate partner violence and predictors during coronavirus among childbearing-age residents in Debre Berhan.
Methods:
A community-based cross-sectional survey was employed from 1 May to 1 July 2020. Eight items of women abuse screening tool were used to estimate intimate partner violence. Trained data collectors directly interview randomly selected participants. The data were entered using Epi-info V. 7 and analyzed using SPSS V. 23. Descriptive statistics were used to determine the prevalence of intimate partner violence and the frequency distribution of other variables. During bivariate analysis, predictor variables with a p-value less than 0.25 were nominated to further analysis. An adjusted odds ratio with a 95% confidence interval was used and a p-value less than 0.05 was considered statistically significant.
Result:
A total of 700 participants were included with a response rate of 95.1%. The prevalence of intimate partner violence in the past single year was 19% with 95% confidence interval = 16.1–21.9. Besides, the prevalence of emotional (19.9%, 95% confidence interval = 16.9–22.8), sexual (10.9%, 95% confidence interval = 8.6–13.2) and physical (9.4%, 95% confidence interval = 7.3–11.6) violence was reported. Women with depressive symptoms, overweight, suicidal ideation, and body image disturbance were significantly associated with intimate partner violence, but not educational status, employment, income, stressful life events, lifetime alcohol use, suicidal attempt, and abortion.
Conclusion and recommendation:
Nearly one out of five interviewed participants had intimate partner violence. Being overweight, having poor body image, and having depression increase intimate partner violence. Special preventive measures and treatment, and other legal services should be taken to alleviate the predictor variables and intimate partner violence.
Introduction
Intimate partner violence (IPV) is defined as a self-reported experience of one or more incidents of physical, psychological, and/or sexual violence within an intimate relationship. 1 It is one of widely spread harm or assault toward women,2,3 and a significant public health issue including violation of many human rights.4 –6 Since IPV harms individuals, families, communities, and society as a whole,2,7 eradicating any harm toward women is a vital tool for the Sustainable Development Goals (SDG 5.2). 8 It is also identified as an important cause of premature death and morbidity. 1 Globally, approximately one in three (30%), and 13% of women experienced physical and/or sexual IPV or non-partners sexual violence in their lifetime, and in a year, respectively.9 –11 According to the World Health Organization (WHO) report, the minimum prevalence of IPV (20%) was reported in the western Pacific whereas the maximum (33%) was in the African region. 9
In Ethiopia, violence against women at home is a daily reality for women. A systematic review done in Ethiopia published in 2015 found that lifetime experience of any type of IPV among women was ranged from 19.1% to 78%, while the lifetime physical abuse of spouses and intimate partners ranged from 31% to 76.5%. 12 Across a year, the prevalence of IPV ranged from 42% to 62.4%.13,14
There are a variety of root causes of spousal harm/violence toward women and there is no single factor that further explains why some people are violent or why violence is more widespread in some communities than in others.3,5,15 Examples of such factors include gender and/or economic inequality, social norms around masculinity, harmful use of alcohol, and child maltreatment.5,16,17 However, violence is not only an expression of gender disparity, it is also used to maintain that unequal balance of power. In some instances, abusers knowingly use violence as a means of subordination (e.g. used to demonstrate and impose the position of a man in charge of the household or relationship).18,19
Violence can harm the physical, sexual, mental, and reproductive health of women and may increase the risk of HIV infection in some settings.9,10 There are several problems that cause pregnancy-related complications such as miscarriage, premature labor, and low birth weight if violence happed during pregnancy.5,20 IPV also has an undesirable outcome on child feeding; IPV reduces the adequate diet of children by 65%. 21
In its worst form, violence kills women. Globally, around 40%–70% and more femicide happened as a result of violent relationships by intimate partners. 16
Globally, the coronavirus pandemic causes a huge impact on physical and psychological health due to strict stay-at-home orders and other related risk factors, especially IPV was the most persistently hidden pandemic problem. 22 Different studies revealed that the prevalence of IPV increased during COVID-19 and in Ethiopia, it ranges from 7.1% among prenatal women to 41.1% and more23 –26 and the incidence in Peru was 48%. 27 COVID-19 prevention strategies like staying at home, minimizing day-to-day activities which had social contact, and government focused on controlling the disease besides overlooking the legal system exacerbate IPV. 22
Facilitating access to quality services, including medical care and psychosocial support, accommodation, law enforcement, and legal services was important to treat women who were victims of violence and avert future risks.4,5 Although IPV had a serious immediate and long-term high public health problem and staying at home due to COVID-19 exacerbate the problem, not enough study revealed the prevalence and related factors of IPV in North Shewa. Therefore, this study intended to examine the prevalence of IPV and predictors during coronavirus among childbearing-age residents in Debre Berhan town. This study will be a critical alarm for healthcare providers and other stakeholders to routine screening for early detection and prevention of IPV.
Methods and materials
Study design, period, and setting
A community-based cross-sectional study design was conducted in Debre Berhan town from 1 May to 1 July 2020. Debre Berhan is located in the North Shewa zone, Amhara region, Ethiopia, and far from about 130 km North of Ethiopia. As the current statistical data revealed, there are 23,093 childbearing-age women in Debre Berhan town. 28 In the town, 4.6% of reproductive women were unable to read and write, 46.7% educated up to secondary school and the rest 48.7% had diploma and degree and the majority 40% of women were employed followed by 29.2% as housewife. 29 Even though different health institutions are found in the town, only the specialized comprehensive hospital renders psychiatric services and it has four psychiatric out-patient departments.
Participants
All women of childbearing age who are residing six or more months in Debre Berhan town were the source population. The study population was all women of reproductive age at randomly selected kebeles and available during the study period. Whereas, those who are unable to communicate, not have intimate partners, high degree edema which affects weight measurement, and spinal problems were excluded.
Sample size determination
In this study, the sample size was computed using the single population proportion formula. A 24.6% proportion of IPV was taken from a related study done in Ethiopia, 24 95% confidence level (CI), design effect 1.5, 4% margin of error, and 10% non-response rate were assumed to get the final sample size

where n is the sample size, Za/2 is the value under the normal standard table for the given confidence level, p is the estimated of the population proportion, and d is the margin of error, using the above equation the sample size was calculated as follows

n = 445.35~446 by considering the design effect and the non-response rate the last sample included became 736.
Sampling technique
Multi-stage sampling was employed to select study participants. First, from nine administrative kebeles, randomly by lottery method four kebeles were selected. Then, the list of households was taken from each selected kebeles administrative body, and the sample size was proportionally allocated to each four kebeles based on the number of households. After that, a simple random sampling technique was used to get the allocated sample size from each kebeles using the lottery method. On condition of more than one eligible woman being found in the selected households, the lottery method was used to pick only one woman in the family.
Data collection procedures and measures
Data were collected using the interviewer-guided questionnaire by local (Amharic) language using six BSc nurses’ data collectors and one MSc midwife as supervisor. IPV was measured using Woman Abuse Screening Tool (WAST) and IPV declared, from eight items Woman Abuse Screening Tool (WAST) score 4 or more symptoms in the last year. The tool was validated by WHO to use a multi-country study on violence against women. WAST compute physical, sexual, and emotional abuse. It scored as 0 (never), 1 (sometimes), and 2 (often). The sensitivity is 91.7% and specificity of 100%.30 –32 Suicidal behavior was assessed using WHO composite international diagnostic interview (CIDI), and it was validated in Ethiopia both in clinical and community settings. 33 Depression was detected using Patient Health Questionnaire 9 (PHQ-9) and depression has considered if the participants’ assessment score was ⩾5. 34 The weight status of the participants determined from data collectors measured weight and height and classified as either normal weight (body mass index (BMI) from 18.5 to 24.9 kg/m2) or overweight (BMI from 25 to 29.9 kg/m2) was categorized into normal and overweight, respectively. 35 Weight-related stigma was detected by 10 items Stigmatizing Situations Inventory (SSI) within the past month.36,37 Body image disturbance (BID) was determined by the question, how often you have been feeling satisfied with the shape of your body over the last month? And the feedback score ranged from never (5) to always (0). 38 Stressful life events were considered when the list threatening experience questionnaire scores ⩾1.39,40 Three-item Oslo social support scale was used to examine the participants’ social support status and mentioned range from poor to strong. 41 Whereas substance use was screened by Alcohol, Smoking, and Substance Involvement Screening Tool. 42 Other variables like diagnosed psychiatric and another medical disorder (HIV/AIDS (yes/no), hypertension (yes/no), diabetes mellitus (yes/no), epilepsy (yes/no), and other chronic medical illnesses (yes/no)), abortion (yes/no), stillbirth (yes/no) and also socio-demographic data (educational status: unable to read and write, primary school, and secondary school and college/university graduate; occupational status: housewife, the government employed, self-employed, and others; income: above the poverty line and below poverty line) were verified during interview.
Data processing and analysis
The data were transcribed and clean-up with Epi-info version 7 statistical program. Then, analyzed using the Statistical Package for Social Science version 23. Descriptive statistics were used to summarize the socio-demographic and other predictor variables. A bivariate test was conducted to show the unadjusted association between outcome and predictor variables and its p-value < 0.25 was considered to the candidate for multivariable regression analysis and it was implemented to verify the adjusted significant associative factors of IPV. Hosmer and Lemeshow test (0.996) was used to check the model fitness. The finding was presented using narration and table with adjusted odds ratio (AOR) and corresponding 95% confidence interval (CI). All significant associations were evaluated at a p-value < 0.05.
Result
Descriptive statistics
A total of 700 study participants were successfully interviewed with a response rate of 95.1%. The mean age of study participants was 33.04 (with standard deviation ±7.5) years with a minimum age of 17 years and a maximum of 49 years. The majority 284 (40.6%) of participants’ age were in the age group of 30–39. The largest proportions of respondents (91%) were Orthodox Christian followers and Amhara (98.1%) ethnicity. Half and more women were college/university employed (Table 1).
Socio-demographic characteristics of reproductive age women in Debre Berhan town, 2020.
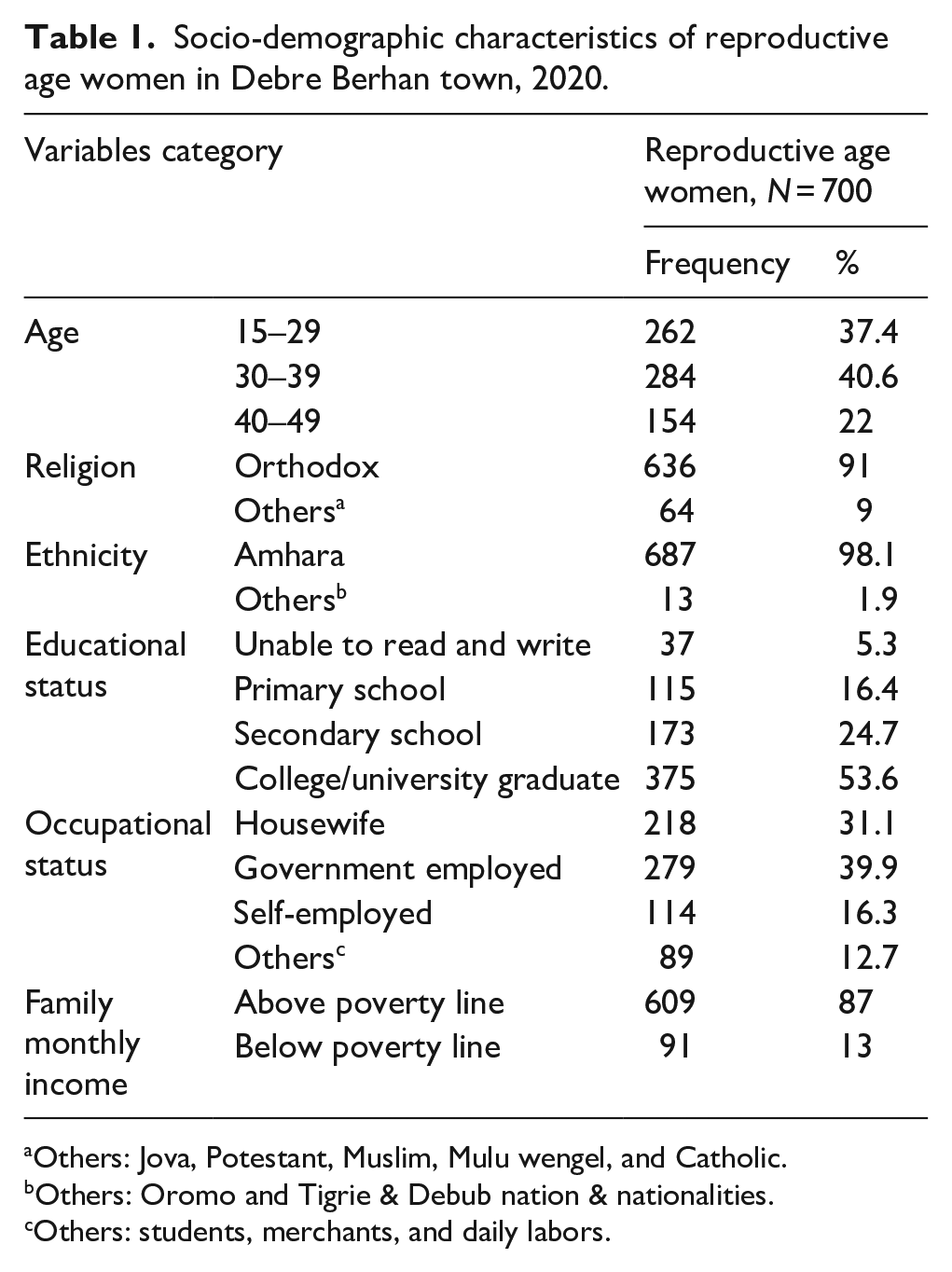
Others: Jova, Potestant, Muslim, Mulu wengel, and Catholic.
Others: Oromo and Tigrie & Debub nation & nationalities.
Others: students, merchants, and daily labors.
Clinical and substance use-related factors
Of the total participants, 87 (12.4%) experienced abortion, while stillbirth was 29 (4.1%). In addition, 31 (4.4%) reproductive age women had a chronic medical illness. From those women, hypertension was the most common medical illness 21 (3%), and diabetes mellitus 7 (1%) and others (HIV/AIDS and epilepsy) 3 (0.4%). However, out of the total participants, 564 (80.6%), 7 (1%), and 1 (0.1%) were used alcohol, khat, and cigarette in their lifetime, respectively. Only 2 (0.3%) participants had alcohol use disorder, while 7 (1%) had khat use disorder. Moreover, the majority of the participants 381 (54.4%) had normal weight, whereas 319 (45.6%) had been overweight during the study time.
Psycho-social factors of study participants
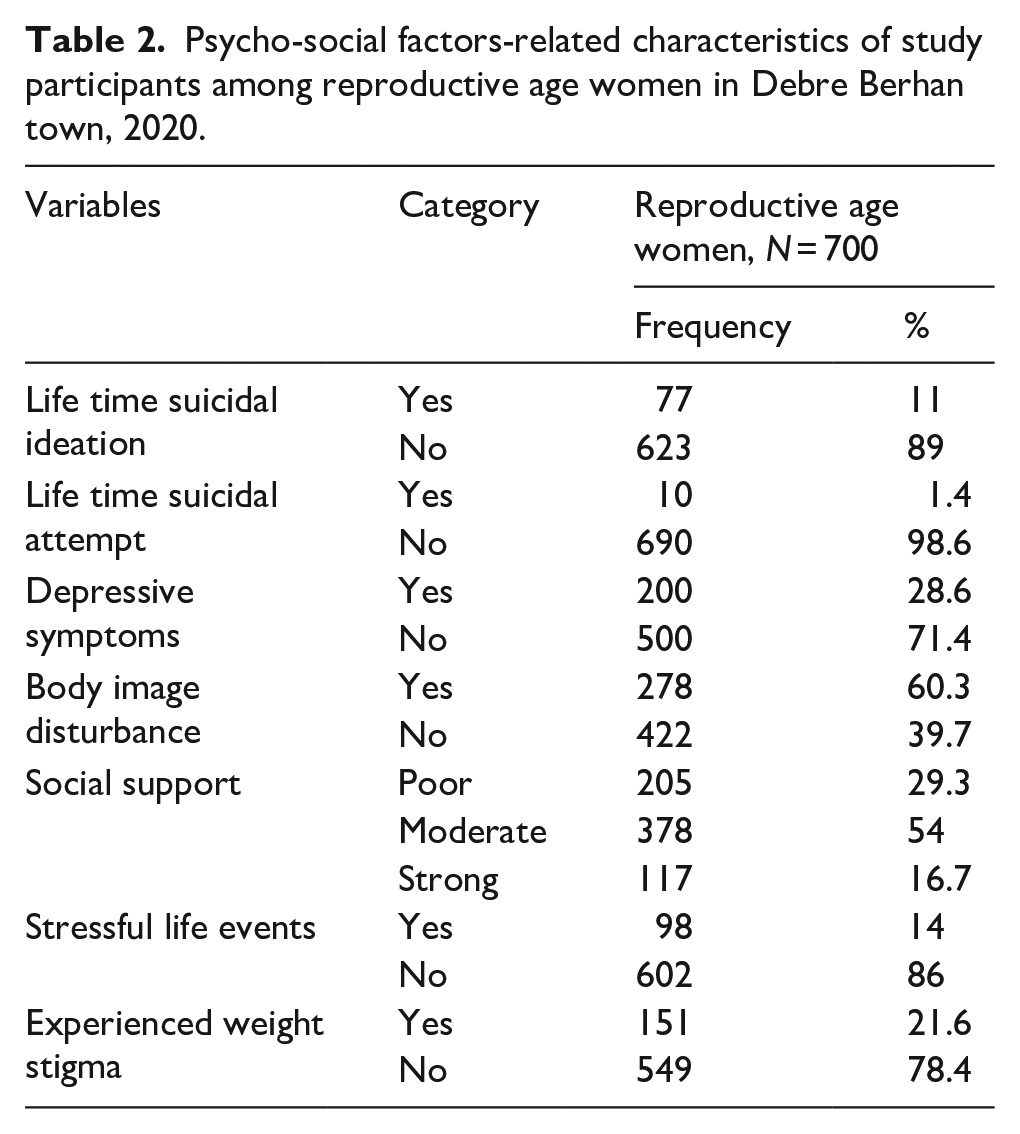
Seventy-seven (11%) of the participants had suicidal ideation and only 10 (1.4%) were experienced suicidal attempts. Furthermore, out of the total participants, 98 (14%) had stressful life events, 200 (28.6%) depressive symptoms, and 151 (21.6%) experienced stigma (Table 2).
Psycho-social factors-related characteristics of study participants among reproductive age women in Debre Berhan town, 2020.
Prevalence of IPV
In this study, 133 (19%, 95% CI = 16.1–21.9) of 700 women had IPV within the last 1 year. Besides, 139 (19.9%, 95% CI = 16.9–22.8) of women experienced emotional abuse, 66 (9.4%, 95% CI = 7.3–11.6) physical abuse, and 76 (10.9%, 95% CI = 8.6–13.2) were experienced sexual assault in the study area along the past single year.
Associated factors of IPV among reproductive age women
Based on bivariate and multivariable analyses, women with depressive symptoms, overweight, suicidal ideation, and BID were significantly associated with IPV whereas occupational status, stressful life events, abortion, and income were not associated with IPV.
Accordingly, the odds of IPV among women who had depressive symptoms were 6.5 times higher than women who had no depressive symptoms (AOR = 6.5, 95% CI = 4.1–10.2). Furthermore, IPV among overweight reproductive women was nearly twice more likely as compared to normal-weight women (AOR = 1.9, 95% CI = 1.2–2.9), stressful life events, abortion, and experienced weight stigma were not significantly associated in this study (Table 3).
Bivariate and multivariable analyses of associated factors of intimate partner violence among reproductive age women in Debre Berhan town, 2020.

IPV: intimate partner violence; COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio.
Others: students, merchants, and daily labors.
The variable is not candidate to bivariate analysis due to one cell (2) less than 5 and not fulfill chi-square assumption.
NB. Hosmer and Lemeshow test value = 0.996.
Discussion
This study revealed that the prevalence of IPV among childbearing-age women was 19%. Associated factors were found being overweight, depressive symptoms, suicidal ideation of the women, and BID.
Based on this study, the prevalence of IPV (19%) was comparable with studies conducted in Wondo-Genet district (21%), 43 Hossana town (23%), 44 and South Africa (20%), 45 but lower in studies in Debre Markos town, Ethiopia (41.1%), 26 Kenya (44.5%), 46 and Abay Chomen district, Ethiopia (37%). 47
Physical violence was the least prevalent 66/700 (9.4%) of respondents. This finding was almost similar to a study conducted in North West Ethiopia 48 and Mumbai, India. 49 However, it was higher in studies done in Hosanna town 44 and Yirgalem town 50 in Ethiopia, and in Brazil. 51 This variation could be seen because of differences in a study setting, communities’ view of IPV in this study since all the three studies were institutionally based, while this study is community-based. The difference also might be the differences in the time at which the data were collected and the screening tool they used.
This study exposed that about 20%, of women, experienced emotional abuse. Likewise, a study in Mumbai, India 49 showed that 19% of study participants were harmed emotionally.
Being overweight women were twice more likely to experience IPV than those who had normal weight. This finding is supported by research done in Saudi Arabia 52 which showed that the obese women had significantly higher levels of IPV severity. This also might be explained indirectly by a previous study finding of low-satisfied women who had higher BMIs and lower exercise. 53 So, if the women are unsatisfied with the marriage, it could be lead to conflict.
In this study, women with suicidal thoughts were three times more likely to suffer from IPV than their counterparts. Similarly, in a study done using data from the National Comorbidity Survey in the United States, 54 the odds of individuals with suicide thought were 2.2 times higher to be exposed for IPV than persons who never thought suicide; yet it was not significant. In addition, a study done in South Africa 55 found that those who had suicidal ideation had an association with IPV. Different articles5,56,57 found IPV as a risk factor for suicidal ideation; however, this could be both the result of IPV and the cause of it.
Women with depressive symptoms had 6.5 times more likely to develop IPV than those who did not have depressive symptoms. This is supported by studies done in Wondo-Genet district and Debre Markos, Ethiopia,21,26 China, 17 and Ghana 58 which showed those women who had depressive symptoms were 4.5, 2.57, and 1.06 times more likely to be exposed to IPV, respectively. This might be due to a change in behavior, emotion, and thinking due to depression and it affects the smooth interaction of the partners. 59 Although it is impossible to differentiate which one is the cause and which one is the effect, both IPV and depression could occur in an individual. Concerning BID, in our finding, the odds of having BID were 1.6 times higher than their counterparts.
Limitations of the study
Since data collection was done by face-to-face interviews, IPV might be underestimated due to recall and social desirability bias because of the sensitive nature of IPV and cultural barriers to disclose partners’ issues to third person. The study does not incorporate underweight and obese women. The temporal causal association cannot be visible using a cross-sectional design.
Conclusion and recommendation
Nearly one out of five interviewed participants experienced IPV. In addition, this study revealed being overweight, having poor body image, having depression, and having suicidal ideation increase IPV, special preventive measures, and treatment should be taken to alleviate the predictor variables. Moreover, community screening for IPV especially socially hindered predictors like depression and suicidal ideation help to reduce IPV and increase the quality of life of women in Debre Berhan town.
Supplemental Material
sj-docx-1-whe-10.1177_17455065211068980 – Supplemental material for Intimate partner violence and COVID-19 among reproductive age women: A community-based cross-sectional survey, Ethiopia
Supplemental material, sj-docx-1-whe-10.1177_17455065211068980 for Intimate partner violence and COVID-19 among reproductive age women: A community-based cross-sectional survey, Ethiopia by Abayneh Shewangzaw Engda, Abate Dargie Wubetu, Fetene Kasahun Amogne and Tebabere Moltot Kitaw in Women’s Health
Footnotes
Acknowledgements
First, the authors thank God for giving them the courage and wisdom to do their work. Then, the authors mention and pass their thanks to Bahir Dar University, friends, and colleagues. Finally, the authors thank Debre Berhan town administrative body for their positive cooperation.
Author contribution(s)
Data sharing statement
The data utilized used to support the result of this research will be available from the corresponding author upon request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
The study was approved by the ethical Institutional Review Board (IRB) of the health science faculty, Bahir Dar University with ethics approval/protocol no. 00209/2020 and a formal permission letter was taken from the administration of the town and also assent and written consent taken from the participants. Participants who are at serious risk were referred to the hospital for further assessment and treatment plans. The research was conducted according to the Declaration of Helsinki.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The whole required cost for this study was covered by Bahir Dar University.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.