
Abstract
Background:
Violence during childbirth indirectly contributes to maternal and neonatal morbidity and mortality. It also causes intrapartum health consequences such as prolonged labor, postpartum hemorrhage, and postpartum psychological problems, including postpartum depression, post-traumatic stress disorder, and other negative feelings that lead to a decreased desire for facility delivery and increase the events of home deliveries which reduce the quality of life. In Tanzania, several efforts have been made to promote respectful maternity care. However, violence during childbirth continues to create a critical barrier for facility-based delivery and is in need of considerable attention throughout the health system.
Objectives:
This study aimed to assess types of intrapartum violence and its determinants among postnatal women in the Dodoma Region, Tanzania.
Design:
A cross-sectional study using a questionnaire to interview postnatal women at the exit point after being discharged from the health facility to assess intrapartum violence and its determinants.
Methods:
This study was conducted in Dodoma Region involving 307 postnatal women from April to June 2022. A simple random method was used to select respondents. The Chi-square and Fisher’s exact tests were used to assess the association between the categorical variables. The predictors of intrapartum violence were determined using binary logistic regression analysis. Statistical analysis was performed using Statistical Package for Social Science version 25.0. P < 0.05 was considered to be significant.
Results:
Overall, 307 postnatal women participated in the study. Among them, 158 (51.5%) postnatal women experienced at least one form of intrapartum violence. The most common forms of intrapartum violence included breach of confidentiality 205 (66.8%), undignified care/verbal abuse 178 (58%), physical abuse 139 (45.3%), and denial or neglected care by midwives 113 (36.8%). Husband employment, urban residence, and being referred from primary hospitals were significant determinants associated with intrapartum violence (adjusted odds ratio = 0.233, 95% confidence interval = 0.057–0.952, p = 0.043, adjusted odds ratio = 2.67, 95% confidence interval = 1.13–10.93, p = 0.026 and adjusted odds ratio = 3.673, 95% confidence interval = 1.131–11.934, p = 0.030, respectively).
Conclusion:
Violence during childbirth was highly prevalent in this study. Understanding the prevalence and types of intrapartum violence is important in order to promote changes in all levels of the health system. This study reveals the need for key interventions to effect change at many levels; including an interventional study to educate women and birth partners on client rights, and strengthening the health system to meet the needs of women during labor and childbirth. Policies and systems that support respectful maternity care are urgently needed in this setting, including universal training of health professionals in respectful maternity care
Keywords
Introduction
Intrapartum violence is a global health issue related to disrespect and abuse of women’s rights and dignity during facility-based childbirth. 1 Childbirth violence can cause unnecessary pain, 2 increased risk for perineal laceration, cesarean section, and fetal distress. 3 It also led to prolonged labor, postpartum hemorrhage, and postpartum psychological problems, including postpartum depression. Post-traumatic stress disorder and other negative feelings lead to distrust in and hatred of the maternity care system and decreased desire for facility delivery and increased events of home deliveries,3 –6 and other preventable complications which result from physical and verbal abuse, lack of confidentiality, unconsented care, lack of privacy, and neglected care. 1 One in three women worldwide has been subjected to one or more types of violence. 7
The World Health Organization in its Organic Law on Women’s Right to a Violence-free Life defines obstetric violence (OV) in Article 15
8
as:
the appropriation of a woman’s body and reproductive processes by health personnel, in the form of dehumanizing treatment, abusive medicalization and pathologization of natural processes, involving a woman’s loss of autonomy and the capacity to freely make her own decisions about her body and her sexuality, which has negative consequences for a woman’s quality of life.
Several factors are documented as contributing factors to intrapartum violence. Examples include facility norms and practices that prohibit relatives’ involvement during labor and birth process (birth companionship), limited space in the labor rooms, limiting women’s choice of positions during labor and delivery, lack of competence of midwives on respective care is also considered a considerable factor in intrapartum violence.3,5,9,10 Sociodemographic factors of the woman such as maternal age, level of education, antenatal visits, and mode of delivery for previous pregnancy are also associated with childbirth violence.5,11 The occurrence of obstetric and intrapartum violence can also be grounded in healthcare systems with political and financial foundations that encourage inequality in patients’ purchasing power. 12
In the present study, the researcher adopted the Humanistic Nursing Theory to provide a theoretical basis for assessing intrapartum violence and its determinants. Originally, Humanistic Nursing Theory emerged from Patterson’s and Zderad’s research that aimed to make things better for nurses and their patients as they interacted in the daily activities of nursing practice. 13 The main constructs of Humanistic Nursing Theory include: “The Call” “And” and “The Response” (Figure 1). The call encompasses the person (patient), family members, and community. The “And” indicates the dialogue between the healthcare provider and the patients. On the other hand, “The Response” includes the individual healthcare provider, or group of healthcare providers who have the responsibility to hear and recognize the call and respond appropriately to the call in respectful manner. 13 The fundamentals of Humanistic Nursing Theory ensures humanistic values are translated into attitudes and behaviors geared to protecting, enhancing, or preserving woman dignity. 8
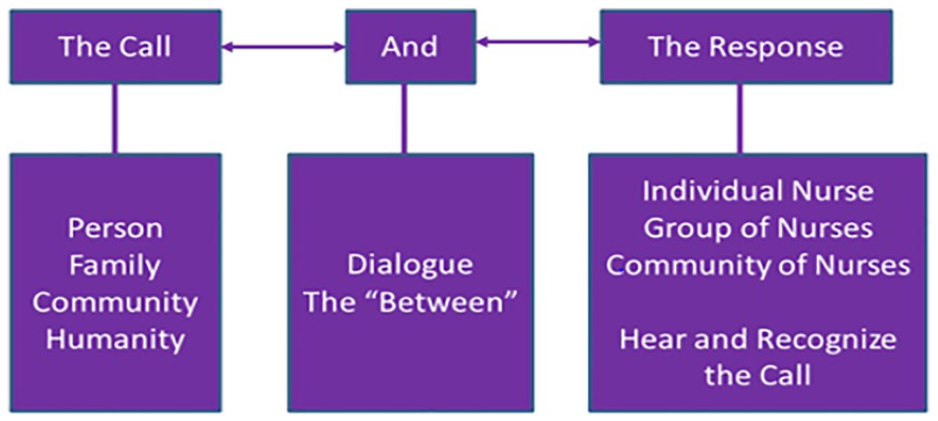
Humanistic nursing theory.
In the current study, the intrapartum violence (Disrespect and Abuse) may emerge when the healthcare provider hears the call but does not respond to the call in a respectful manner. Sometimes, the patient may define the environment in which the dialogue takes place as disrespectful; for example, the maternity environment when it does not favor for privacy and confidentiality of care. Sometimes, even if the healthcare provider responds to the patient, she or he may be harsh to such extent that the patient (laboring woman) perceives it as disrespectful and uncaring. Because the Humanistic Nursing Theory is built in two important aspects: humanism and existentialism, humanism tries to take a broader perspective of the individual’s potential and tries to understand each individual through their personal experiences. On the other hand, existentialism aims to justify that patients (as human beings) must have the ability to exercise a free-choice, self-determination, and self-responsibility to planned healthcare delivery. According to this statement, receiving maternity care without consent from the patient herself can be defined as obstetric and intrapartum violence (Figure 1).
Regarding health systems, there are some conditions that do not support healthcare providers with provision of appropriate care. Such conditions include high ratio between patients and providers (too few providers, too many patients), lack of access to life saving medications and supplies,14,15 lack of involvement of birth partners (companionship) due to adapted colonial policy,16 –18 limited preparation or knowledge at the community level about pregnancy/labor/birth, 19 these conditions leads to stressful and often traumatic to healthcare provider, which sometimes might be associated with childbirth violence.20,21 The observed poor behaviors from some providers may be learned behaviors from other health workers and also likely a result of chronic stress and trauma from hard-working environmental and other factors. 20
Respectful maternity care (RMC) is a universal right of childbearing women as every woman should be treated with dignity and respect. 1 This right can be achieved through undertaking several initiatives. One of the initiatives is the provision of ongoing education to healthcare providers on respectful maternal care together with designing institutional norms that support respectful obstetric services to both the laboring woman and relatives. 22 Another important initiative to eliminate obstetric and intrapartum violence is through modification of the environment of maternity ward as numerous studies have reported that the maternity ward environment may increase or decrease the potential for obstetric and intrapartum violence. 23
Tanzania as a country has taken measures by working with a professional organization such as TAMA and AGOTA to promote RMC. According to RMC workshop meeting report, done in 2015, Tanzania through the Ministry of Health and Social Welfare showed commitment to ensuring that advocates for respective maternity care (RMC) at regional and district levels, restructure facilities to accommodate RMC practices by establishing quality improvement teams, liaising with pre-service education and encouraging community involvement, reinforcing client charter and reorganization of the facility to ensure privacy and confidentiality, and provision of motivational incentives for healthcare workers working at maternity ward. 24 Researchers and policy-makers have addressed disrespectful care by capacity building of human resources, strengthening professional organizations, and by educating midwives in low-resource countries, like Tanzania on RMC. 25
The number of efforts invested in dealing with other violence such as gender-based violence needs to be redirected to intrapartum violence as well. Research evidence documented by Mayra et al., 2 demonstrates that intrapartum violence has not received a considerable effort. Furthermore, although OV poses a critical barrier for institutional delivery, it has not been well addressed in many settings, including Sri Lanka, 26 Chile 27 and India. 28 Similar observations exist in Tanzania, especially in the study area, Dodoma Region, which is a fast-growing region with cultural diversity where little is known about intrapartum violence prevalence and its determinants. This justifies the need for the current study. Therefore, we aimed to assess intrapartum violence during facility-based childbirth and its determinates among postnatal women in Dodoma.
Methodology
Study design and setting
A hospital-based cross-sectional study using a questionnaire to interview postnatal women during their exit after discharged from health facilities to assess intrapartum violence and its determinants. The study was conducted between April and June 2022 in Dodoma Region, Tanzania. Dodoma Region is one of 31 regions of Tanzania. Being the capital city of Tanzania, it is bordered by 4 neighboring regions namely Manyara of the North, Iringa on the South, Morogoro on the East, and Singida on the West. The region has seven districts: Chemba, Kondoa, Kongwa, Chamwino, Bahi, Mpwapwa, and Dodoma City. The region is located in the central part of Tanzania, with estimated population of 3,085,625 of whom 1,512,760 and 1,572,865 were males and females respectively, with fertility rate 12.2%. 29 Maternal mortality ratio 417 per 100,000 live birth. 30 Regardless of free charge of maternal healthcare services including childbirth in Dodoma region the proportion of home delivery was reported to be 46.5%. 31 The facility-based birth strategy has the aim of reducing maternal and neonatal morbidity and mortality. However, one of the reasons of home deliveries is obstetric and intrapartum facility-based violence. 15 Currently, in the study area there is no data concerning intrapartum violence as one of the main reasons of home delivery. Therefore, this justifies the need for conducting this study.
Study population
The study population comprised of all postnatal women who give birth at public and private health facilities and were interviewed during the exit from hospitals to prevent under-reporting of intrapartum violence while in the wards. Postnatal women who declined participation in the study and those who experienced severe illness like being unconscious during the hospital stay, were excluded from the study to prevent the hallo effect.
Sample size determination and sampling method
We calculated the sample size using the Kish Leslie formula for quantitative studies as it was used in our previous study. n = Z² p(1−p)/e². Where n = minimum required sample size, z = confidence level at 95% (standard value of 1.96), and p = proportion of the estimated level of knowledge, and marginal error of 0.05. We assumed the proportion to be 76.3 % as was reported in the previous study which was done in Northwest Ethiopia by Mihret. 32 Therefore, the sample size was 276 and by assuming a 10% non-response rate, the final sample size (i.e. 276 * (1/1 – 0.10)) turned to be 307. Dodoma regional was selected conveniently due to high number (46.6%) of home delivery. 31
The regional hospital was selected purposively. Four out of seven districts were selected by using simple random sampling. Three district hospitals and four health centers from selected districts were selected using simple random sampling. We reviewed records of deliveries in a month from the eight selected hospitals, we found there were 2293, 459, 227, 176, 128, 96, 67, and 60 deliveries at the eight selected health facilities. Proportionate sampling technique was used to obtain the required study participants from each selected hospital using ni = (Ni/Nt) × n as used in the previous study. 33 Where ni = required number of study participants from a given hospital, Ni = required sample size for the study, Nt = total number of deliveries from all the selected hospitals, and n = number of deliveries as per hospital. The total number of deliveries in the selected health facilities (n = 3506) the sample size of 307 was proportionately allocated to the eight health facilities selected and therefore, 201, 40, 20, 15, 11, 8, 6, and 5 study participants were selected from each of the selected hospitals. Study participants from the selected hospitals were selected using convenience sampling method.
Definition of variables
In this study, women were considered to have experienced intrapartum violence during labor and childbirth if they answered “yes” to any form of disrespect or abusive care. The disrespect and abuse items in the questionnaire were posed to the respondents during the exit from hospital after discharge. The questionnaire included many forms of disrespect and abusive care including physical abuse, verbal insults, non-confidential care, neglectful care, non-consensual care, bribery, and care discrimination. The possible responses for each question were “yes” and “no.” Any response of “yes” to at least one question signaled that the woman had experienced obstetric violence,32,34 as detailed below (Table 1).
Categories of intrapartum violence.

Data concerning maternal and fetal birth outcomes were collected through a review of records from the outpatient antenatal cards (RCH no. 4). Women who had blood loss of greater than 500 ml for vaginal delivery and more than 1000ml after cesarean section were classified as having had a postpartum hemorrhage (PPH). Primiparous women who experienced labor pain for more than 18 h and multipara women who had experienced labor pain for more than 12 h were considered as having had prolonged labor. Perineal injury included perineal tears or episiotomy and birth asphyxia defined using Apgar score with a normal Apgar score being greater than 7 at 1 and after 5 min. This information was retrieved from RCH card no. 4 from each woman who participated in our study.
Data collection methods and tools
We used an interviewer-administered questionnaire to collect relevant data. Questionnaire was adapted after an extensive literature review of similar studies.32,34 –36 The questionnaire was in English, translated into Kiswahili language (national language spoken in Tanzania) and then back-translated to English for consistency. The tool was pretested on 30 (10%) of the total respondents from a different area. Postnatal women included in the pre-test were not included in the study. Following the pre-test, corrections to items that had any ambiguity were made. The internal consistency of the tool for data collection was determined by the Cronbach’s alpha test, where alpha was found to be 0.78 for the tool assessing intrapartum violence. The respondents were interviewed at the exit point after being discharged from the facility. The interview was done in one of the rooms in the outpatient department to maintain privacy. Each exit interview took approximately 25 to 30 min. Three trained research assistants were used for data collection. The questionnaire comprised of closed-ended questions. The questionnaire had five sections that included sociodemographic characteristics, obstetric history, experiences of intrapartum violence during childbirth, and maternal and fetal immediate birth outcomes.
Sociodemographic characteristics included age (years), marital status, residence, education, occupation and tribe (ethnicity) and residence. We also include obstetric history included mode of delivery, birth position and ANC visits in the current pregnancy. Experiences of disrespectful and abusive maternity care during childbirth included verbal insult, physical abuse, non-dignified care (neglected care), non-confidential care, non-consented care, bribe, and discriminated care. Maternal and fetal birth outcomes included occurrence of postpartum hemorrhage, prolonged labor, perineal injury, birth asphyxia, fetal trauma, fresh stillbirth.
Statistical analysis
Statistical analysis was performed using Statistical Package for Social Science (SPSS) version 23. Descriptive statistics were used to analyze the sociodemographic characteristics and the results were presented in proportions. Pearson’s chi-square statistical test was used to assess the association between categorical variables. Inferential statistics comprised of binary logistic regression analysis for determining the predictors of childbirth violence. p < 0.05 was considered significant. Confounding factors were controlled for each variable.
We have followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Guidelines when preparing this article.
Results
Sociodemographic characteristics
A total of 307 postnatal women participated in this study for a response rate of 100%. Over half (57.7%) of the respondents’ age ranged 21 to 29 years, with the mean ± SD age 26 ± 6.379 years. The majority (85.7%) of them were recruited from public health facilities. Over half (53.1%) of them reside in urban areas and the majority (84.4%) of participants were married. Half of the respondents (50.8%) had completed primary education and most (52.4%) of them were self-employed (Table 2).
Sociodemographic characteristics of study participants (N = 307).

Obstetric characteristics
A majority (60.9%) of the participants were multiparous and (91.9%) had been admitted to the facility as a self-referral from home. Majority (92.2%) of them had spontaneous vaginal deliveries and most (87.6%) waited less than 1 h for admission procedures. It was further noted that a majority (86.6%) of the participants had one to two healthcare providers present during childbirth. Of 307 study participants, (85%) were comfortable to be attended by either male or female health providers. The majority of women (92.5%) were not allowed to choose their position for giving birth and they mostly (85.7%) gave birth while lying on their back (lithotomy) (Table 3).
Obstetric characteristics of study participants (N = 307).
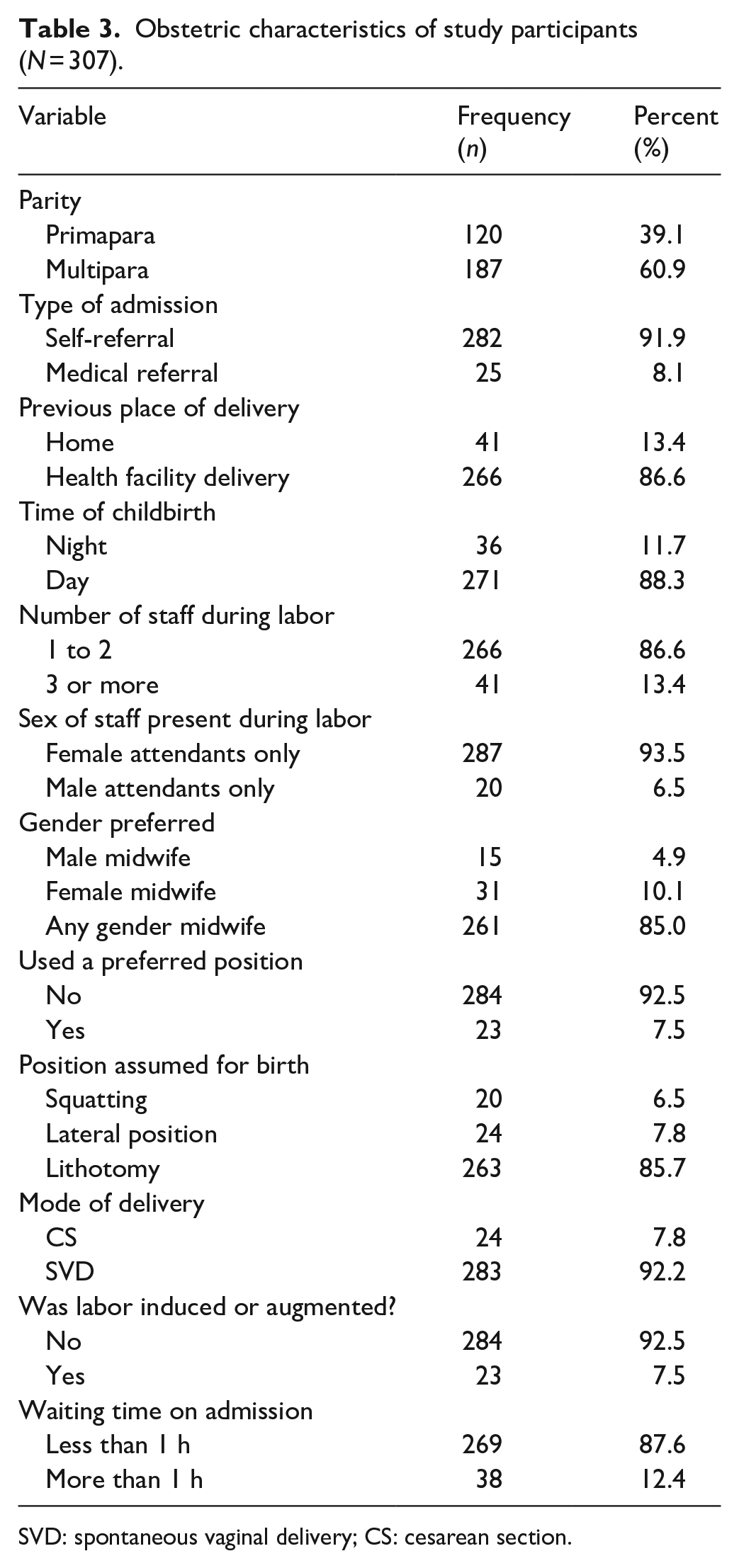
SVD: spontaneous vaginal delivery; CS: cesarean section.
Frequency distribution of items used to measure intrapartum violence
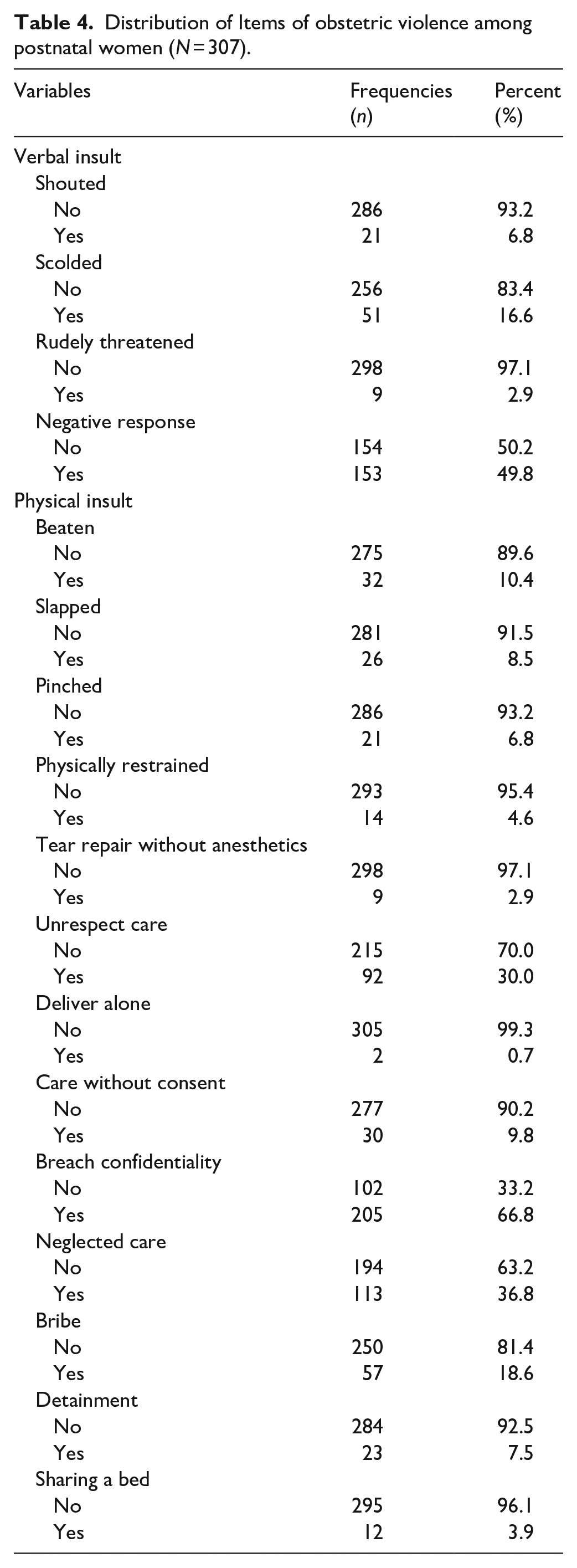
Intrapartum violence among postnatal women was assessed using 17 questions. The results showed that majority (66.8%) of participants reported non-confidential care, and about half (49.8%) of participants reported negative responses from health providers when they asked for assistance. Many (36.8%) participants had care denied or neglected care by healthcare providers (Table 4).
Distribution of Items of obstetric violence among postnatal women (N = 307).
Prevalence and types of intrapartum violence
Out of 307 postnatal women who participated in the current study, more than half (51.5%) experienced intrapartum violence. Violence among postnatal women was assessed using 7 categories of disrespect and abuse. The majority (66.8%) of participants reported to have experienced non-confidential care, more than half (58.0%) experienced verbal abuse, and (45.3%) reported to have experienced physical abuse (Figure 2).

Categories for intrapartum violence reported by study participants.
Predictors of intrapartum violence
After adjusting for all factors, postnatal women residing in urban areas were almost 3-fold more likely to report intrapartum violence compared to women residing in rural area (adjusted odds ratio [AOR] = 2.67, P = 0.026). Women whose husbands were employed were 77% less likely to experience intrapartum violence compared to women whose husband were not employed and the difference was significant (AOR = 0.233, P = 0.043). Women who had a medical referral were 3 times more likely to report intrapartum violence compared to those who had self-referral and the difference was significant (AOR = 3.7673, P = 0.030) (Table 5).
Significant predictors of obstetric violence during intrapartum (n = 307).
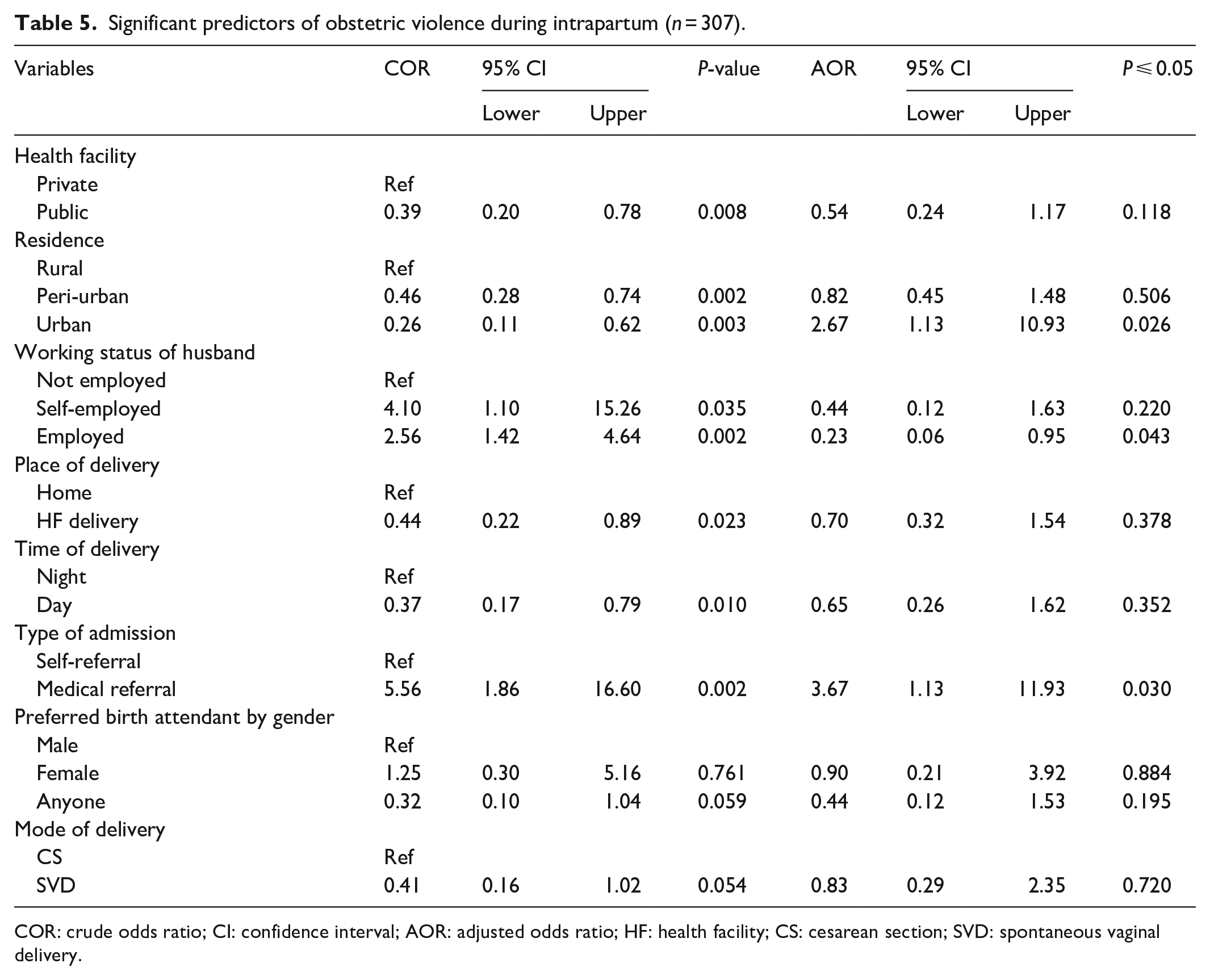
COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio; HF: health facility; CS: cesarean section; SVD: spontaneous vaginal delivery.
Frequency distribution of immediate maternal and neonatal birth outcomes
Table 6 displays findings regarding immediate maternal and neonatal birth outcomes as recorded on their RCH card. Only 24 (7.8%) of postnatal women had history of prolonged labor, 16 women (5.2 %) experienced a PPH and 70 women (22.8%) had perineal tears or episiotomy. In terms of neonatal outcomes, 10 (3.3%) of babies were stillbirth, 57 babies (18.6%) received resuscitation after birth using suction, a bag, and mask and 11 neonates (3.6%) developed caput succedaneum (Table 6).
Immediate maternal and neonatal birth outcomes post-delivery (n = 307).

PPH: postpartum hemorrhage; FSB: fresh stillbirths.
Significant association of immediate maternal and neonatal birth outcomes with intrapartum violence
Univariate results indicated that type of neonatal resuscitation (bag and mask (crude odds ratio [COR] = 6.000, P = 0.020)) and Apgar score at 5 min (< 7 (COR = 3.204, P = 0.046)) were the birth outcomes which significantly were associated with intrapartum violence. After controlling for confounders, women who reported any form of intrapartum violence were almost two times more likely to deliver a baby with a low Apgar score (AOR = 2.141, 95% CI = 1.576–7.951, P = 0.034) and four times more likely for their baby to be resuscitated with bag and mask (AOR = 4.223, 95% CI = 1.832–21.445, P = 0.025) (Table 7).
Association of maternal and neonatal birth outcome with obstetric violence (n = 307).

COR: crude odds ratio; AOR: adjusted odds ratio; CI: confidence interval; PPH: postpartum hemorrhage; FSB: fresh stillbirths.
Discussion
Disrespect and abuse during childbirth is defined as violence against women’s human rights and can be interpreted as an indicator of poor-quality care, 35 a significant barrier to increasing facility-based births, as well as a breach of rights-based approaches to care. 37 Obstetric and/or intrapartum violence can negatively affect the pregnancy outcome 36 and possibly may lead to reduced facility-based health seeking behaviors.34,35 The current study analyses intrapartum violence and its determinants among postnatal women in Tanzania.
The key findings of this study include high (51.5%) reported subjective prevalence of intrapartum violence. Such violence was associated with women who reside in peri-urban areas, husbands’ lack of formal employment, and medical referral. Another key finding included a positive association between neonatal resuscitation using bag and mask and Low Apgar score (<7) at 5 min with reported intrapartum violence.
The prevalence of intrapartum violence in the current study is consistent with that of previous studies conducted in other resource limited settings, including Nigeria (55.9%), 38 India (57%), 39 and in Kenya, Tanzania, Sudan, and South Africa (52%). 40 These similar findings may be due to the similar method of recruiting postnatal women who were interviewed face to face upon their discharge from the hospital. Also, these high magnitudes of intrapartum violence observed in these low-resource settings may be contributed by low support of health systems including inadequate working environment, lack of appropriate infrastructures for deliveries (no privacy in labor ward), shortage of staff leading to overworking, inadequate medicine, equipment, and supplies. 41 Another reason may be untrained healthcare providers for cultural engagement. 41 With all these shortcoming health providers end up into frustration. It is well known that a woman in labor need continuous support care from skilled birth attended. However, when there are many women in labor wards who need that care and there are few providers, there is no way all women can receive a skilled supportive care. As a result the women will receive pieces of care and some providers will not respond to each woman request, which correspond to the theory of Humanistic Nursing Theory “The Call” “And” and “The Response”. 8
The prevalence of intrapartum violence in this study is higher compared to studies conducted in Mexico (33.3%) 42 and in the United States (42.7%). 43 The reasons for the observed discrepancy may be due to the study approach. In the current study, we approached our respondents immediately after their birth experience, using face to face interviews and inquired about OV in the current delivery, while the study conducted in Mexico asked about OV experiences over the past five years, which may be influenced by recall bias. Another predictive reason may be the level of education, in current study the majority of participants had attained primary school, and low level of education may be associated with low awareness of the women rights during labor and delivery and women with higher levels of education maybe more likely to be aware of their rights. 32 Also, women with high level of education may have high income and knowledge about their rights.
On the other hand, the proportion of childbirth violence in the present study is lower than the reported prevalence in different studies, example, in the study conducted in South Ethiopia (79.7%), 44 Northwest Ethiopia 75.1%, 32 in Western Ethiopia (74.8%), 34 in Spain 67.4%, 45 the variation in time of interview after childbirth could be a reason for the observed difference. Also, overcrowded hospitals and shortage of staff may contribute healthcare workers to behave abusively. 32
The forms of intrapartum violence experienced by postnatal women in current study included mainly verbal abuse, breach of confidentiality, physical abuse and denial of care. Similar findings were reported by several studies conducted elsewhere in sub-Saharan Africa and outside Africa, especially Spain, Mexico and Europe.32,42,45,46 The moral lesson learned from these findings is that obstetric and/or intrapartum violence can be found everywhere regardless of the economic status of the country. Obstetric and/or intrapartum violence demoralizes the community involved in building trust in maternity care and it was found to reduce healthcare-seeking behavior.46,47
Considering sociodemographic characteristics of the postnatal women in the current study, we found that, urban residents were more likely to report any form of OV compared to postnatal women residing in the rural area. This keeps in line with the findings reported elsewhere. For example, in a study done by Mihret, 32 it was found that urban residents were almost two times more likely to report any form of OV compared to rural residents. Another study conducted in Mexico by Castro and Frías, 42 reported similar findings, that women residing in urban area are more privileged to report OV compared to women residing to the rural area. The reasons for why urban residents are more likely to report the experience of OV might be contributed by several factors; educational level of the participants, which is reported to increase the likelihood of reporting OV events during maternity care. 11 The knowledge and awareness level of the participants regarding OV and women rights might be more common to people living to urban due to several exposures.35,48 In another study conducted at Northern Nigeria, it was reported that lack of awareness on RMC because of lower level of education may contribute to their inability to differentiate between acceptable standard of care, and abusive care. 38
We also found that women whose husbands were employed were protected against any form of OV during labor and childbirth compared to their counterparts. This correlates with family income. The same evidence was also reported in a study conducted in India by Jungari et al., 39 who reported that poor and lower caste women are more vulnerable to mistreatment and abuse during childbirth. Furthermore, another study conducted in Tanzania reported that poor women coming from poor families are more likely to experience OV. 36 Women of lower socioeconomic backgrounds were also more likely to report events of OV and disrespectful care in Sri Lanka. 26 This raises concerns about class discrimination by healthcare providers. 36
Our study also found that pregnant women referred for childbirth were almost four times more likely to report events of OV during labor and childbirth compared to their counterparts. A study conducted in Spain found that pregnant women referred for urgent cesarean sections were at least three times more likely to report having experienced a form of obstetric violence. 45 In Tanzania, pregnant women can be referred from a lower level facility due to risk factors indicating the need for hospital delivery where (comprehensive emergency obstetric and neonatal care) CEmONC services can be offered. 49 The increased risk of OV among referred women might be associated with healthcare providers’ attitude toward women with a perceived delay in seeking maternity care, hence, increasing likelihood of verbal abuse and other disrespectful acts. According to anecdotal evidence from the field, majority of women get referred for expertise maternity care tend to come alone without escort from the family. Such women are at increased chance to suffer detainment for not paying hospital bills on time of which it is associated with OV.10,44,50
Limitation of the study
In this study, postnatal women were reporting experienced OV which might have introduced recall bias of either over-reporting or under-reporting depending on the person’s behavior in reporting the recent and past information. We would have interviewed healthcare providers as well to rule out their perspectives on OV and integrate the postnatal women report and healthcare providers report. Also, we would have observed the healthcare provider on the care provided which could have given the different magnitude of OV. We included government health facilities Future study will need to employ qualitative research approach to explore deeply the disrespect and abusive care during childbirth.
Conclusion
Disrespect and abuse during childbirth is highly prevalent in the study area. There is an urgent need to better understand women’s experiences and the complex factors that contribute to obstetric and/or intrapartum violence in this setting. To support the safety of women receiving reproductive health services, innovative interventions are needed at all levels of health system delivery and at the community level to drive a demand for RMC. Possible approaches include community-based education about the rights of clients seeking healthcare, including for labor and birth. A focus on strengthening health systems to respond to specific women’s needs during childbirth (include provision of supportive infrastructure for women privacy, confidentiality, informed choice, information for women on their rights, mechanisms for redress following violations, and ensuring high professional standards of clinical care (1), reinforcing policies on RMC, and improving providers training to incorporate interpersonal and cultural aspects of care in the aspect of respectful and companionate care.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231189544 – Supplemental material for Intrapartum violence during facility-based childbirth and its determinants: A cross-sectional study among postnatal women in Tanzania
Supplemental material, sj-docx-1-whe-10.1177_17455057231189544 for Intrapartum violence during facility-based childbirth and its determinants: A cross-sectional study among postnatal women in Tanzania by Neema Egid Sanga and Angelina A Joho in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057231189544 – Supplemental material for Intrapartum violence during facility-based childbirth and its determinants: A cross-sectional study among postnatal women in Tanzania
Supplemental material, sj-docx-2-whe-10.1177_17455057231189544 for Intrapartum violence during facility-based childbirth and its determinants: A cross-sectional study among postnatal women in Tanzania by Neema Egid Sanga and Angelina A Joho in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.