
Abstract
Background:
Maternal health service utilization decreases maternal morbidity and mortality. However, the existing evidence is inadequate to design effective intervention strategies in Ethiopia.
Objectives:
This study aimed to examine the utilization of maternal health service and identify its determinants among women of reproductive age in southern Ethiopia.
Design:
A community-based cross-sectional study was conducted from October 21 to November 11, 2022 on a sample of 1140 women selected randomly from the Northern Zone of the Sidama region.
Methods:
Data were collected using the Open Data Kit mobile application and exported to Stata version 15 for analysis. We used a multilevel mixed-effects modified Poisson regression with robust standard error to identify determinants of maternal health service utilization.
Results:
Utilization of antenatal care, health facility delivery, and postnatal care was 52.0% (95% confidence interval: 49.0%, 55.0%), 48.5% (95% confidence interval: 45.6%, 51.4%), and 26.0% (95% confidence interval: 23.0%, 29.0%), respectively. Antenatal care use was associated with receiving model family training (adjusted prevalence ratio: 1.19; 95% confidence interval: 1.06, 1.35), knowledge of antenatal care (adjusted prevalence ratio: 1.54; 95% confidence interval: 1.31, 1.81), perceived quality of antenatal care (adjusted prevalence ratio: 1.02; 95% confidence interval: 1.01, 1.03), and having birth preparedness plan (adjusted prevalence ratio: 1.13; 95% confidence interval: 1.02, 1.25). The identified determinants of health facility delivery use were middle wealth rank (adjusted prevalence ratio: 1.35; 95% confidence interval: 1.03, 1.77), perceived quality of health facility delivery (adjusted prevalence ratio: 1.02; 95% confidence interval: 1.01, 1.03), antenatal care (adjusted prevalence ratio: 1.76; 95% confidence interval: 1.36, 2.26), and high community-level women literacy (adjusted prevalence ratio: 1.55; 95% confidence interval: 1.10, 2.19). Postnatal care use was associated with facing health problems during postpartum period (adjusted prevalence ratio: 1.79; 95% confidence interval: 1.18, 2.72), urban residence (adjusted prevalence ratio: 3.52; 95% confidence interval: 2.15, 5.78), knowledge of postnatal care (adjusted prevalence ratio: 1.11; 95% confidence interval: 1.04, 1.19), and low community-level poverty (adjusted prevalence ratio: 0.43; 95% confidence interval: 0.25, 0.73).
Conclusion:
Maternal health service use was low in the study area and was influenced by individual- and community-level determinants. Any intervention strategies must consider multi-sectorial collaboration to address determinants at different levels. The programs should focus on the provision of model family training, the needs of women who have a poor perception, and knowledge of maternal health service at the individual level.
Keywords
Introduction
Maternal health has become a global public health priority area, as shown by the Sustainable Development Goals (SDGs). 1 Maternal health care is the care given to women during the prenatal, intrapartum, and postnatal periods and includes antenatal care (ANC), skilled attendance at birth, postnatal care (PNC), safe abortion care, and family planning.2 –4
Proper utilization of the existing maternal health service (MHS) is a cost-effective approach to decrease maternal illness and death.2,5,6 For example, ANC gives the chance for discussion between women and health care providers regarding nutrition, obstetric danger signs (ODS), and childbirth plans; 7 vital for protective care such as the supply of folic acid pills and tetanus toxoid vaccines,7,8 early detection and quick treatment of complications of pregnancy and diseases.2,7 –9
Health facility delivery (HFD) service is an important intervention approach to avert most maternal mortality during childbirth. 10 Most maternal deaths occur in the time immediately after childbirth, and 15.0% happen at the start of the childbirth. 11 Besides, any obstetric complication during childbirth can be unanticipated and unpredictable. 12 Maternal health outcomes in such occasions are significantly improved when such complications happen in the presence of intrapartum care and health facilities that are well prepared and equipped to manage such emergency complications.2,5,13 –15
PNC is another important intervention to prevent maternal death. 16 The majority of maternal mortalities happen during the postpartum period, of which 48.9% of postnatal maternal deaths occur within 24 h of childbirth. 17 Hence, high-quality and timely PNC is a fundamental approach to women’s survival and well-being. 16
Due to the above benefits, the World Health Organization (WHO) suggests that women use at least eight ANC visits—the first contact in the first trimester, two contacts in the second trimester, and five contacts in the third trimester, 18 to attend a health facility during childbirth 2 and PNC visits 16 for all mothers. The first PNC visit should be within 1 day after childbirth at a health institution or home, followed by at least three additional postpartum visits between the 2nd and 3rd, between the 7th and 14th, and on 42nd postpartum days. 16
However, the existing maternal health service use (MHSU) is very low in developing countries, particularly in sub-Saharan Africa and Southern Asia. 5 For instance, according to the mini-Demographic and Health Survey (mini-DHS) conducted in 2019 in Ethiopia, 72% of pregnant mothers had at least one ANC visit, while 48% gave birth at health facilities, and merely 34% of women received PNC. 9 These statistics were much inferior in the Sidama region, and a study reported that utilization of the ANC service was 45%, skilled birth attendance was 40.7%, and PNC was 14.3%. 19 The major determinants of low MHSU are poverty and lack of access to health care, sociodemographic factors, place of residence, distance to facilities, lack of infrastructure and information, MHS seeking behaviors, women’s knowledge of ODS and MHS, insufficient and poor quality services, organizational and health system factors, lack of transport services, and cultural beliefs and practices.3,5,9,20
Globally, several initiatives have been undertaken to increase MHSU. These measures include the safe motherhood conference in Nairobi (1987), 21 the international conference on population and development in Cairo (1994), 22 the millennium development goals conference (2000), 23 and the latest global conference of the SDGs (2016). 1 Also, the Ethiopian government has been exerting considerable efforts to increase MHSU. These measures include the formulation of a comprehensive 20-year health sector development program, 24 a national reproductive health strategy (2016–2020), 25 health extension programs, 26 and a growth and transformation plan. 27
Regardless of all the international and national measures and efforts, MHSU remains low in Ethiopia. 9 Besides, there were significant regional and urban/rural differences at the country level, 9 which implies the need to further study the landscape of utilization patterns of MHS in local settings. Furthermore, earlier studies that investigated the utilization of MHS in Ethiopia focused mainly on individual-level determinants3,28 with limited consideration of community-level and contextual determinants. Moreover, the determinants of MHSU differ from region to region in Ethiopia. The utilization of MHS was highly variable and existing evidence was limited to designing effective and efficient intervention strategies. Assessing the current utilization and determinants of MHS services is helpful to inform program managers, policymakers, and implementers in designing effective intervention strategies to improve MHSU and achieve SDG 3. Thus, we aimed to examine the utilization of MHS and identify its determinants among women of reproductive age in southern Ethiopia.
Conceptual framework
Existing literature suggests that theory-based studies are critical for predicting human behaviors, including the use of services for sexual and reproductive health. 29 This study’s conceptual or analytical framework was based on the Andersen and Newman behavioral model of health care service utilization 30 and guidance from different literatures.3,5,9,20 This conceptual framework or model assists in better comprehending the relationship between individual, societal, and health care system determinants. 30 It included multilevel hierarchical determinants affecting MHSU in the local context of the study area. This study has conceptualized that MHSU is linked to two levels of determinants, that is, individual- and community-level determinants. We used Andersen’s health-seeking behavioral framework to select a list of independent variables for each determinant. Figure 1 denotes the list of variables under each determinant.30,31 The predisposing component of individual determinants refers to the features of the person and comprises social position, attitudinal, and demographic variables. The enabling factors comprise situations that make health service utilization accessible to women (linked with logistical features of obtaining services). The third component is need factors, which are the most proximal cause of health care utilization, or “illness level,” which is most directly associated with health service utilization and comprises diagnosed illness and perceived illness. In the context of this study, “illness level” can be interpreted in relation to gestation history and the present course of the gestation.30,31 At the societal level, we have considered several factors, such as place of residence, community-level literacy of women, community-level poverty, community-level social media use, and distance from the nearest health facility (HF) (Figure 1).

Determinants of MHS utilization among women of reproductive age in North Zone of Sidama region, Ethiopia, 2023.
Methods
Study area
The study was done in the Northern Zone of Sidama region, Ethiopia. Sidama region was newly established on June 18, 2020, and is the second smallest regional state, following Harari by land size, and the fifth largest populous in the country. 32 It is located in the southern part of Ethiopia and consists of four zones, namely, the Northern, Southern, Central, and Eastern zones, and one city administration. 33 Northern zone is located 273 km south of Addis Ababa. It has eight districts and two town administrations. There are 162 Kebeles (the smallest administrative units in Ethiopia) in the zone. Based on the report from Sidama Region Health Bureau, the zone has an overall population of 1.29 million. Women of reproductive age (WRA) are estimated to constitute 23.3% of the population. The zone has 144 health posts, 36 health centers, 1 general hospital, and 4 primary hospitals. The zone’s overall potential health service coverage by public HFs is 70%. 34 Based on the Sidama Regional Health Bureau 2022 report, utilization of at least one ANC, HFD, and PNC were 90%, 80%, and 70%, respectively. 34
Study design and population
A community-based cross-sectional study was conducted from October 21 to November 11, 2022, among WRA in the Northern Zone of Sidama region, Ethiopia. We included all randomly selected WRA who gave live birth in the last 12 months and resided in the zone for at least for 6 months. Women who were ill during the data collection period were excluded from the study since their participation and consent could be affected.
Sample size determination
The sample size was computed using OpenEpi version 3. The sample size required to estimate the utilization of MHS was computed by considering the anticipated utilization of ANC (74%), HFD (48%), and PNC (34%), according to the report of a previous study, 3 a margin of error of 5%, a 95% confidence level, and a design effect of 2.0. The design effect was calculated using the formula DEFF = 1 + (n−1)*ICC], where “n” is the average cluster size and ICC is the intraclass correlation coefficient. The minimum required number of clusters was computed by multiplying the effective sample size by the ICC. However, previous studies did not report the ICC value. We took the typical value of the ICC to be 0.05 from a range of values (0.01–0.05) based on the recommendation of Donner. 35 Accordingly, the minimum needed number of clusters was 384 × 0.05 = 19.2. To maintain the adequacy of the cluster numbers and to have sufficient power, 22 clusters were included in this study. The Kebeles which are subsets of districts were considered as clusters in this study. The sample size was adjusted for the non-response rate by dividing the initial sample size by the anticipated response rate. Based on the above information, the estimated sample size was 613 based on ANC, 795 based on HFD, and 714 based on PNC. The sample size for the determinants of MHSU was computed by taking variables significantly associated with MHSU based on previous studies done in Northern Ethiopia, 36 rural Haramaya district, Eastern Ethiopia, 3 and Northwest Ethiopia. 37 Accordingly, the assumptions considered and the resulting sample sizes were summarized in Table 1 of Supplementary File 1. Hence, the sample size of 1140 obtained from the second objective was used because it was the maximum sample size determined and would be adequate to address both objectives of this study.
Sampling technique
We used a multi-stage sampling method to select eligible women. The first stage was a selection of representative districts from the Zone using a simple random sampling method. From the eight districts that are found in the Zone, four districts (Shebedino, Hawela Lida, Boricha, and Bilate Zuria) were selected randomly for this study. In the second stage, representative kebeles were selected from each district using a simple random sampling method. Accordingly, Diramo Afara 01, Morcho Negesha, Midire Genet, Morocho Shondolo, Kowoloso, and Taramesa Kebeles were selected from Shebedino district. From the Hawela Lida district, five kebeles, namely Hawela Lida 01, Murancho, Dobe Nagasha, Chafe, and Hawela Lida Rural, were randomly selected. Similarly, from the Boricha district, five kebeles (Yirba 01, Yirba Duwancho, Sadamo Dikicha, Konsore Arke, and Fulasa Aldada) were selected randomly. Finally, six kebeles, namely Balela 01, Hanja Goro, Shondolo Liwo, Sadamo Cala, Shamana Godo, and Konsore Haranja, were randomly selected from Bilate Zuria district. The third stage was a selection of the households with WRA who gave birth in the last 12 months. The households with WRA who gave birth in the last 12 months were identified by conducting the house-to-house census. The house-to-house census was conducted by community health workers who were residents of that particular Kebeles, whereas the health extension workers and Kebeles leaders were supervised during the census procedure to minimize information bias. A sampling frame was prepared based on complete household listings that contain WRA who gave birth in the last 12 months. Initially, the determined sample size was proportionally allocated to the kebeles based on their population size (WRA who gave birth in the last 12 months). A simple random sampling method was used to select eligible households in each kebeles. Finally, WRA who gave birth in the last 12 months and resided in the selected households were included in the study. When two or more mothers were eligible for the study in the selected households, one mother was selected using a lottery method. If the selected woman was absent from the household for three successive visits during the data collection period, she was considered a non-respondent.
Study variables
The outcome variables were three MHSU-related variables (ANC, HFD, and PNC). Each outcome variable has a binary response and was measured using women’s self-report. We coded each outcome variable as “1” for use and “0” for non-use of the service from skilled providers.
We categorized the independent variables into individual- and community-level variables. The individual-level variables were socioeconomic and demographic variables, such as maternal age, educational status of the women and their spouses, occupational status of the women and their spouses, household wealth index, and exposure to mass media; obstetric characteristics such as gravidity, parity, stillbirth, maternal age at marriage, the experience of ODS, and pregnancy status; women’s knowledge and attitude toward the MHS; knowledge of ODS; perceived quality of the MHS, and birth preparedness and complication readiness (BPCR) plan. The community-level variables were place of residence, community-level literacy of women, community-level poverty, community-level social media use, and distance from the nearest HF. The details of the measurement of the variables used for this study are now provided in Table 2 of Supplementary File 1.
Data collection procedures
A structured and pretested questionnaire was used to collect our data. It was adapted from other similar previous studies.3,9,28,36 –39 The tool was first prepared in English. It was translated into the Sidaamu Afoo language (the prime language spoken in the study area) and back to English to maintain its originality and consistency. The forward and backward translations were done by two independent translators who were experts in English and native speakers of Sidaamu Afoo. The principal investigator (PI) and a third person who was also fluent in both languages reviewed the translated tool. Then, any inconsistency or inaccuracy between the two versions was corrected based on the problems noticed during the review. Prior to data collection, the PI trained the data collectors and supervisors for 2 days on the significance of the study, data collection procedures, objectives, methods, and ethical issues. The questionnaire was pretested on 5% of the sample in Dale district of Sidama region and amended before the actual data collection. Data were collected using the Open Data Kit (ODK) mobile application by 17 health professionals with Bachelor’s degrees who were experienced in data collection and were fluent in Sidaamu Afoo. The KoboToolbox server was used to archive data and upload it on a daily basis. Data were collected using a structured and face-to-face interviewer-administered questionnaire at the women’s homes. To minimize the risk of reporting bias, data collectors were told during training to properly explain to the women the importance of the questions and to elicit a genuine response from the women. A consistent check for incompleteness and non-consistency of the data was made daily. The data were exported from ODK to Stata version 15. The exported data were properly cleaned, coded, and categorized before the main analyses. This article was prepared based on the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline and the STROBE checklist is delivered as supporting information (see Supplementary File 2).
Statistical analysis
Prior to doing the main analysis, all necessary variable recoding, computations, and categorizations were done. Summary measures for categorical variables were expressed in terms of absolute frequencies and percentages, whereas for numerical variables, the mean with standard deviation (SD) was used as a descriptive measure after checking for normality of the distribution. The wealth index was calculated using principal component analysis (PCA) as a combined indicator of life standards based on 42 questions related to ownership of prudently selected household assets, such as the owner of the house, materials used for house construction, the number of rooms in a house, size of agricultural land, presence of herd or farm animals and livestock, types of fuel used for cooking, and possession of improved sanitation and water facilities.9,40 The details of the wealth index calculation procedure for this study are provided in Table 3 of Supplementary File 1.
A modified Poisson regression with robust standard error was used to calculate the prevalence ratios with 95% confidence intervals (CIs) for the determinants of MHSU. It is a better option to analyze cross-sectional data with binary outcome as compared to logistic regression when the prevalence of outcomes of interest is greater than 20%41
–43 because the prevalence ratio is easier to understand and express to non-epidemiologists than the odds ratio.
42
Besides, the odds ratio can overestimate the prevalence ratio and for the two measures, adjusting for confounding is not equal.
43
We built a multilevel model to consider the hierarchical nature of our data, to decrease potential standard error underestimation using the ordinary regression model,
44
and to provide a robust standard error estimate.
45
Five models were assessed, Model 0: an empty model; Model 1: model with only individual-level predictors; Model 2: model with only community-level predictors; Model 3: model containing both individual- and community-level predictors; and Model 4: the model with a random coefficient. The random effect model was evaluated using the median prevalence ratio (MPR) and ICC value.
46
The ICC value was used to describe the proportion of variability in MHSU that is due to the clustering variable (kebele), whereas MPR is an estimate of the unexplained kebele-level heterogeneity. The MPR is described as the average value of the prevalence ratio between the area at the lowest and highest risk of MHSU when randomly selecting two areas, and it was computed using the formula MPR = ~
Before conducting a multilevel analysis, we decided whether or not the multilevel model was required by doing a random intercept model of mixed-effect multilevel logistic regression. This model offers data regarding ICC which is used to determine whether a multilevel model is required or not.50,51 If the random intercept variance is significant or the ICC value is greater than 5%, the multilevel analysis model is mandatory to consider. Variables with p-values less than 0.25 on bivariable analysis and other variables of known practical significance with relevant support from the medical literature were included in a multivariable regression model. 52 The multivariable analyses were used to control for the potential confounding variables. Effect modification was evaluated by entering interaction terms into the multivariable analysis model one at a time. Multicollinearity among the independent variables was also evaluated using a multiple linear regression model. We declared that the effect of multicollinearity would be less likely when the variance inflation factor was less than 5 for all variables. 53
The presence and strength of a statistically significant association were assessed using adjusted prevalence ratios (APRs) with 95% CIs. A statistically significant association between the variables of interest was confirmed when the 95% CI of the APRs did not contain 1. A sensitivity analysis was conducted using the APRs from multilevel mixed-effect modified Poisson and log binomial regression models. It is associated with attempts to evaluate the suitability of a certain model specification and the degree of validity of the conclusions generated from such a model. It is also vital in circumstances where a model is anticipated to be used in the course of subsequent research studies or clinical practice to establish confidence in the outcomes of the primary analysis. 54
Result
Table 1 presents a summary of the sociodemographic and economic features of the participants. From the total of 1140 study participants, 1130 study participants took part in the study making a response rate of 99.12%. The mean (±SD) of the age of women was 28.33 (±6.26) years. The majority of respondents were within the range of 25–29 years old. The largest portion of the study participants identified themselves as being from the Sidama ethnic group (92.7%) and reported following the protestant Christian faith (85.9%), being married (98.1%), and enrolled in formal education (64.6%). More than half, 577 (51.1%), of the study respondents had access to mass media through radio, television, and newspapers.
Sociodemographic and economic characteristics of the study participants in the Northern zone of Sidama region, Ethiopia, 2022 (N = 1130).

Note: There were 22 divorced/separated/widowed women in our data. However, we collected data from all women about their husband’s occupation and education status by the time they were in marital union.
Reproductive health characteristics
The mean (±SD) of the age at first marriage of the women was 18.41 (±2.33) years. Nearly one-fifth (19%) of the women had a previous history of abortion. Approximately two-thirds (63.7%) of the study respondents had given birth to two to four children. However, 11% of women had experienced a stillbirth at least once. For 68.9% of the women, the last pregnancy was planned (Table 4 of Supplementary File 1).
MHS utilization
The utilization rate for ANC (at least one visit) was 52.0% (95% CI: 49.0%, 55.0%), for HFD 48.5% (95% CI: 45.6%, 51.4%), and for PNC 26% (95% CI: 23.0%, 29.0%) (Figure 2). About 3 out of 10 mothers (28.2%) had more than four ANC visits during their most recent pregnancy as per WHO recommendation. Less than half (46.6%) of the mothers had their first ANC visit during their fourth or more months of pregnancy. Only 14.8% of women had three or more PNC visits within 6 weeks after childbirth (Table 5 of Supplementary File 1).
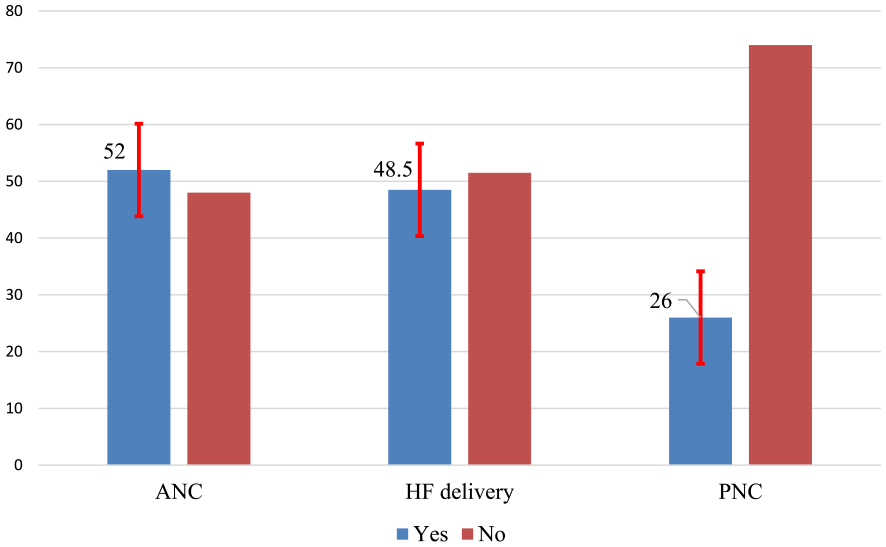
MHSU among women of reproductive age in the Northern zone of Sidama region, Ethiopia, 2022.
Descriptive reasons for not using maternal health care services
Absence of health problems during antenatal period and fast onset of labor were the main reasons mentioned by women for not utilizing ANC (45.2%, n = 245) and HFD (42.4%, n = 247), whereas absence of health problems during postnatal period was the main reason for PNC non-utilization (61.6%, n = 515). Most women (33.0%, 337) mentioned that the availability and influence of traditional healers in the villages was a common sociocultural factor that affected MHSU (Table 6 of Supplementary File 1).
Determinants of maternal health service utilization
Women who had received model family training had a 19% higher likelihood of ANC use than their counterparts (APR = 1.19; 95% CI: 1.06, 1.35). A one-unit increase in women’s knowledge score of ANC (APR = 1.54; 95% CI: 1.31, 1.81) led to a 1.54-fold increase in the prevalence of ANC utilization, whereas a one-unit increase in women’s perceived quality of ANC score (APR = 1.02; 95% CI: 1.01, 1.03) increased the likelihood of ANC utilization by 2%. Women’s BPCR plan increased the likelihood of ANC service utilization (APR = 1.13; 95% CI: 1.02, 1.25) by 13% compared to women who did not have a BPCR plan (Table 2).
Determinants of ANC use among women of reproductive age in the Northern zone of Sidama region, Ethiopia, 2022 (N = 1130).

CI: confidence interval; ©: continuous variable; CPR: crude prevalence ratio; APR: adjusted prevalence ratio; Ref: reference group; ANC: antenatal care.
Significant association (p < 0.05); **Highly significant association (p < 0.01).
Women in the middle wealth rank had 35% more HFD utilization as compared to the lowest rank (APR = 1.35; 95% CI: 1.03, 1.77). A one-unit increase in women’s perceived quality score of HFD (APR = 1.02; 95% CI: 1.03, 1.04) increased the likelihood of HFD utilization by 2%. The likelihood of HFD utilization was 76% higher among women who had ANC follow-up (APR = 1.76; 95% CI: 1.36, 2.29) than their counterparts. The women who live in communities where women literacy were high (APR = 1.55; 95% CI: 1.10, 2.19) had a higher prevalence of HFD use compared to communities where women literacy were low (Table 3).
Determinants of health facility delivery use among women of reproductive age in the Northern zone of Sidama region, Ethiopia, 2022 (N = 1130).

CI: confidence interval; HFD: health facility delivery ©: continuous variable; CPR: crude prevalence ratio; APR: adjusted prevalence ratio; Ref: reference group.
Significant association (p < 0.05); **Highly significant association (p < 0.01).
Women who had faced health problems during postpartum had a higher prevalence of PNC use than their counterparts (APR = 1.79; 95% CI: 1.18, 2.72). A one-unit increase in women’s knowledge of PNC score (APR = 1.11; 95% CI: 1.04, 1.19) led to 11% increase in the likelihood of PNC utilization. While urban residence increased the likelihood of PNC utilization (APR = 3.52; 95% CI: 2.15, 5.78) as compared to the rural residence, the likelihood of PNC use was 67% lower for those women who resided in low-poverty communities (APR = 0.43; 95% CI: 0.25, 0.73) as compared to women who resided in high-poverty communities (Table 4).
Determinants of PNC use among women of reproductive age in the Northern zone of Sidama region, Ethiopia, 2022 (N = 1130).

CI: confidence interval; ©: continuous variable; CPR: crude prevalence ratio; APR: adjusted prevalence ratio; Ref: reference group.
Significant association (p < 0.05); **Highly significant association (p < 0.01).
Random effect model of MHSU
The multilevel modified Poisson regression model fitted better than the ordinary Poisson regression model (p < 0.001). The ICC value revealed that 35.48% of the variability in using ANC, 28.01% of the variability in using HFD, and 50.76% of the variability in using PNC were related to membership in kebeles. The MPR value demonstrated that residual heterogeneity between the residential areas when randomly selecting the two individuals in different areas was related to 1.58 times the individual likelihoods of using ANC, 1.69 times the individual likelihoods of using HFD, and 2.57 times the individual likelihoods of using PNC. The final model, even after adjusting for all potential attributable factors, revealed that the heterogeneity in MHSU across residential areas continued to be statistically significant. Furthermore, the effect of the BPCR plan on ANC use showed significant variation across the kebeles (variance = 0.02; 95% CI: 0.01, 3.69). Similarly, the effect of ANC use on HFD use indicated a significant variation across the kebeles (variance = 0.11; 95% CI: 0.04, 0.33). Moreover, the effect of women’s knowledge of ODS on PNC use revealed a significant variation across the kebeles (variance = 0.09; 95% CI: 0.02, 0.48); (see Table 7 of the Supplementary File 1).
Sensitivity analysis result
We conducted the sensitivity analysis to compare the performance of multilevel mixed-effects modified Poisson regression with robust variance and log binomial regression models using AIC and BIC values. The multilevel mixed-effects modified Poisson regression with robust variance best fits the model for our data due to relatively small AIC and BIC values. Besides, for the moderate sample size and highly prevalent outcomes of interest, modified Poisson regression with robust standard error produces less-biased estimates of the APR than the log binomial regression model. 43 Thus, we used multilevel mixed-effects modified Poisson regression with robust variance based on this information (see Tables 8, 9, and 10 of the Supplementary File 1).
Discussion
The overall utilization rate was 52.0% for ANC services, 48.5% for HFD, and 26.0% for PNC. Women’s model family training, knowledge and perceived quality of ANC, and BPCR plan were determinants of ANC use. Households’ middle wealth rank, women’s perceived quality of HFD, ANC follow-up, and community-level women literacy were determinants of HFD use, whereas health problems during postpartum period, women’s knowledge of PNC, urban residence, and community-level poverty were determinants of PNC use.
Utilization of at least one ANC service was 52.0%. This result is lower than the Mini-EDHS 2019 report (74%), 9 and studies in Gedeo Zone (72.6%), 55 Holeta town (87%), 56 Hossaina town (87.6%), 57 and Kombolcha district (86.1%) of Ethiopia. 58 The difference might be due to the study period. The previous studies were conducted before the COVID-19 pandemic, while our study was conducted immediately following the control of the pandemic. It has been argued that MHSU decreased during the pandemic due to movement restrictions, limited transport access, and fear of COVID-19 infection, and that the effects of the pandemic persisted during the post-COVID-19 period and highly influenced MHSU. 59 Another explanation might be conflicts at the country level, particularly in the Sidama region over the last 3 years. Due to the conflict, some of the HFs were temporarily closed and unable to provide health services. Even the functional HFs during the conflict period were not able to provide proper services due to shortages of supplies and drugs. Moreover, our study included women from rural settings, whereas previous studies included women from only urban areas or both settings. As a result, rural women may lack autonomy in health decision-making, and there may be a lack of access to information, poor knowledge of MHS, and inadequate HFs in the study area.
This study found that HFD use was 48.5%, which is similar to the Mini-EDHS 2019 report (48.0%). 9 However, this result is lower than that of the research done in Mana district (86.4%), 28 Bench Maji Zone (78.3%), 60 and Addis Ababa (97%) 9 of Ethiopia. The probable justification for the lower proportion of HFD service in this study could be due to fewer ANC visits by women during pregnancy than in other parts of the Ethiopia. As a result, women in the study area have poor knowledge of ODS and HFD, as well as less birth and complication readiness during pregnancy. Furthermore, in the Sidama region, home delivery is a more cultural and religious practice than in other parts of Ethiopia. This argument was supported by evidence demonstrating that women in the Sidama region were discouraged from accessing and using formal MHS due to their trust in Traditional Birth Attendants (TBAs), traditional and cultural beliefs. 61
Utilization of at least one PNC was 26.0%. This result is lower than the finding from the national survey (34.0%), 9 a prior study in Sidama region (32.7%), 62 and Assela town (72.7%) 63 of Ethiopia. This could be attributed to the efforts of community health workers and Health Extension Workers (HEW) to raise women’s awareness of the benefits of PNC utilization in other settings. A previous study found that women who knew more about danger signs during the postpartum period used PNC services more than their counterparts. 64 The presence of cultural beliefs among community members who believe that movement outside of the home may expose women to evil spirits may reduce PNC use by limiting the movement of women after giving birth in the current study area. Furthermore, cultural practices and the degree of urbanization in the study settings may influence PNC utilization.
Our MHSU findings were extremely lower than the reports from Sidama Regional Health Bureau, utilization of at least one ANC, HFD, and PNC were 90%, 80%, and 70%, respectively. 34 This discrepancy might be due to the fact that routine health management information system (HMIS) data were susceptible to over-reporting MHSU indictors in Ethiopia due to competition between health facilities based on performance during the quarter review meeting, poor data recording and reporting practice, and poor data quality check mechanism. 65 Besides, there are greater mismatches or variability of HMIS report between registers, tally sheet, HMIS report, and district health information system (DHIS), which is an indication of poor data quality. Moreover, there is discrepancy between the reports at different hierarchies of health systems, such as health posts, health centers, hospitals, district health offices, zones, and regions in Ethiopia.65,66 Study conducted in the Jimma zone of Ethiopia reported consistent finding that poor agreement between ANC, HFD, and PNC estimates acquired from the survey and HMIS report. 65
This study found that the women’s model family training increased the prevalence of ANC use. A similar result was reported from a previous study in the Sidama region. 62 The possible rationale could be described as follows: women who received model family training from HEWs tend to possess good knowledge of MHS, a positive attitude, health-seeking behavior, and information on the benefits of ANC.
Women’s knowledge of ANC was significantly associated with ANC utilization. Consistent findings were reported from the studies conducted in Sunyani Municipality, Ghana 67 and Western Jamaica. 68 The reason might be that women who have good knowledge of ANC may better know the severity of problems during pregnancy and be prepared to use ANC. Furthermore, many studies proved that women who lack knowledge of the ANC are less likely to be prepared for birth and complications, and as a result, they frequently delay seeking proper MHS.67 –69
Higher score on perceived quality of ANC was significantly associated with ANC utilization. The likely justification could be that women who perceive good quality in ANC services tend to be more confident, have favorable attitudes, and engage in good health-seeking behaviors that might increase their use of ANC. Others have argued that improving women’s perception of ANC service quality could increase the sustained utilization of ANC. 70
This study showed that women’s BPCR plan was positively associated with ANC use. The reasons might be that women who are well prepared have better knowledge of ODS and good communication with HCPs. Consequently, they may have organized all the required prearrangements to use ANC services efficiently and effectively. Other researchers argued that women who have good knowledge of ODS are more likely to be birth-prepared and have complications readiness and hence often use skilled care.67 –69
The middle rank was significantly associated with HFD. Studies conducted in the Mana district of southwest Ethiopia, 28 Pakistan, 71 rural Haiti, 72 and Bangladesh 12 documented similar findings. The likely justification might be indirect and direct non-medical costs related to HFD services influencing service utilization in developing countries, including Ethiopia. Although HFD services are free in Ethiopia, women still pay out of pocket for indirect costs, such as transportation, some laboratory tests and drugs, and food during stays in towns. Studies claimed that women from communities with scarce resources had been challenged to pay for health care, and these costs constituted economic barriers to using MHS.73,74 Therefore, due to a lack of economic access, the mothers may not use HFD at all or delay receiving care.
The higher score on women’s perceived quality of HFD increased the likelihood of HFD utilization. This result agreed with the studies done in the Kaffa zone of southwest Ethiopia, 75 and Northern Ethiopia. 76 The possible explanation might be that women are not merely motivated by the verified actual quality of MHS but also by their perceived quality of MHS; this indicates that information from friends, relatives, and neighbors influences their perception. Expansion of HFs to different parts of the country merely does not assure women’s use of HF care. In rural areas, the existence of several sociocultural barriers seriously affects women’s perceptions of the quality of service and their preference for home delivery over skilled delivery care.
ANC use was significantly associated with HFD utilization, which is consistent with the study finding from the Kaffa zone, 75 Mana district, 28 and Hossaina town of Ethiopia, 57 Bangladesh, 12 Pakistan, 71 and rural Haiti. 72 This finding can be partly explained by the evidence that ANC follow-up is one of the vital linkages between women and health professionals. The women who have ANC visits would have a high probability of receiving adequate counseling and information on ODS, BPCR plan, and the importance of safe delivery at the HFs. Also, mothers who seek health care throughout their pregnancy might be more likely to seek health care during their childbirth. Moreover, the mothers who regularly visit HFs for ANC use have earlier indicated their acceptance of the health system.
This study found that high community-level women literacy increased the prevalence of HFD. Educated women tend to possess good health-seeking behavior, are more autonomous and economically independent, have better job opportunities, and have information on the benefits of ANC.62,70,77 This result agrees with previous studies done in the rural Haramaya district, 3 Holeta town, 56 Hossaina town, 57 and Kaffa zone of Ethiopia, 75 and Bangladesh. 12 Another reason might be that the literate women could have the increased community-level mass media use that might increase the dialogue about maternal health concerns in society. The WHO report showed that women who reside in high-income communities could have better exposure to mass media, which increased their awareness and knowledge of MHS.2,5 This argument is supported by the results of a study done in low-income countries. 78
Women who had encountered health problems during postpartum had an increased prevalence of PNC use compared to women who did not face any problems. This finding agrees with previous findings in Wonago district 64 and Debre Markos town 79 of Ethiopia, and Nepal. 80 The likely explanation might be that being exposed to complications increases the women’s and families’ anxiety about developing much more problems. Also, mothers who have observed serious warning signs have a high probability of negative impressions of susceptibility and the harshness of risks that directly lead to improved PNC utilization. Another reason could be women’s knowledge of ODS, which may be a significant motivator for the mother to obtain PNC as soon as complications happen.
The increased knowledge score of women about PNC leads to increased prevalence of PNC utilization. Studies conducted in northern Ethiopia 81 and rural Nepal 82 documented similar results. The possible justification could be that mothers who have good knowledge of PNC may better understand the benefits of PNC and be prepared to use PNC services. Also, many studies showed that women who had poor knowledge of MHS had a lower probability of getting ready, and as a result, they frequently delayed seeking proper MHS.67 –69
Urban residence increased the prevalence of PNC service utilization. Similar results were reported from studies in the Aysaeta District of Ethiopia, 83 Bangladesh, 12 Nigeria, 84 and Nepal. 80 The reasons would be that mothers who reside in an urban setting are more educated, have improved exposure to mass media and information, are more autonomous, have better job opportunities, are economically independent, and are nearer to health institutions. Besides, a mother’s health-seeking behavior is extremely affected by deep-rooted sociocultural traditions and negative attitudes toward the postpartum period in the rural setting of Ethiopia. Moreover, inadequate awareness, lack of transportation and road access, poor infrastructure, unavailability, and inaccessibility of service might lead to low use of PNC in rural settings.
Another key result of our study was the strong negative relationship between the use of PNC and community-level poverty. The prevalence of PNC use increased for women who resided in high-poverty communities. This finding agreed with the study finding from Ghana. 85 The probable justifications for the higher proportion of PNC utilization by poor women in the study area could be due to the fact that displaced families during the Sidama and Guji Oromo border conflicts were residing in urban areas nearer to health facilities. Furthermore, many aid organizations are providing support for the poor pregnant and lactating women through the health facilities. As a result, poor women in the study area have more likely visited a health facility to obtain aid and services compared to women from rich families. In contrast, studies from Ethiopia 86 and West Africa 87 reported a significant positive association between low-community poverty and PNC use.
Limitations of the study
The probability of recall bias may be high since we recruited women who gave birth in the last 12 months. Women might be unable to recall most of the ODS of pregnancy and postpartum periods, which may underestimate the magnitude of ODS and affect its association with ANC and PNC use. Our findings may be influenced by reporting bias because the data were collected from the women’s self-reports. There is the risk of intentionally misreporting personally related determinants such as age, education, occupation, wealth index, women’s attitude toward MHS, and perceived quality of care (social desirability bias). Therefore, the extent of these determinants might have been undervalued or overvalued, and as such, the association of these determinants with MHSU might have been underestimated or overestimated.
Conclusion
In the study area, the utilization of MHS was very low as compared with the national plan. The underutilization of MHS showed that much work remained to be done to improve women’s health outcomes. Our study identified several pertinent determinants of MHSU. The women’s model family training, knowledge and perceived quality of ANC, and the BPCR plan were determinants of ANC use. Households’ middle wealth rank, women’s perceived quality of HFD, ANC follow-up, and community-level women’s literacy were determinants of HFD use. Health problems during postpartum, women’s knowledge of PNC, urban residence, and community-level poverty were determinants of PNC use. Thus, intervention strategies should focus on promoting women’s school enrollment, creating women-focused economic reforms, strengthening model family training and BPCR plan, and developing programs to improve women’s knowledge and perception of MHS.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231218195 – Supplemental material for Individual- and community-level determinants of maternal health service utilization in southern Ethiopia: A multilevel analysis
Supplemental material, sj-docx-1-whe-10.1177_17455057231218195 for Individual- and community-level determinants of maternal health service utilization in southern Ethiopia: A multilevel analysis by Amanuel Yoseph, Wondwosen Teklesilasie, Francisco Guillen-Grima and Ayalew Astatkie in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057231218195 – Supplemental material for Individual- and community-level determinants of maternal health service utilization in southern Ethiopia: A multilevel analysis
Supplemental material, sj-docx-2-whe-10.1177_17455057231218195 for Individual- and community-level determinants of maternal health service utilization in southern Ethiopia: A multilevel analysis by Amanuel Yoseph, Wondwosen Teklesilasie, Francisco Guillen-Grima and Ayalew Astatkie in Women’s Health
Supplemental Material
sj-docx-3-whe-10.1177_17455057231218195 – Supplemental material for Individual- and community-level determinants of maternal health service utilization in southern Ethiopia: A multilevel analysis
Supplemental material, sj-docx-3-whe-10.1177_17455057231218195 for Individual- and community-level determinants of maternal health service utilization in southern Ethiopia: A multilevel analysis by Amanuel Yoseph, Wondwosen Teklesilasie, Francisco Guillen-Grima and Ayalew Astatkie in Women’s Health
Footnotes
Acknowledgements
The authors thank Hawassa University and Sidama region for their financial support. They also thank the study participants, data collectors, supervisors, and administrators at different levels in the Sidama region who directly and indirectly contributed to this study. Finally, they thank Netsanet Kibru for her big support, such as duplication of consent form and funded transportation fee.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.