
Abstract
Background:
The majority of maternal and neonatal adverse events take place during the postnatal period. However, it is the most neglected period for the provision of quality care.
Objective:
The aim of this study among mothers in the Awi Zone, Amhara region, Ethiopia, was to assess client satisfaction with existing postnatal care and associated factors.
Methods:
An institution-based cross-sectional study was conducted in Awi Zone hospitals from 1 to 30 April 2018. A total of 422 post-partum mothers were selected by systematic sampling. The data were collected using a pre-tested structured questionnaire via a face-to-face interview. Data entry and analysis were completed using EpiData version 3.1 and SPSS version 22, respectively. The data were summarized with frequency and cross-tabulation. Both binary and multiple logistic regressions were used to identify predictor variables using odds ratios and 95% confidence intervals.
Result:
The prevalence of postnatal care satisfaction was 63%. Being from urban area (AOR = 2.1, 95% CI = (1.11–3.99)), having a history of antenatal care follow up (AOR = 1.62, 95% CI = (1.23–1.64)), spontaneous vaginal birth (AOR = 3.14, 95% CI = (1.77–3.28)), and those who did not face any complications during birth (AOR = 2.90, 95% CI = (1.47–1.69)) were some of the factors associated with client satisfaction.
Conclusion:
According to the results of this study, the majority of mothers were satisfied with post-partum care services. The study findings indicate that maternal satisfaction on post-partum care is mainly affected by residency, antenatal care follow up, mode of delivery, and complications during birth. Therefore, health care providers and other concerned bodies should give special attention to those mothers who are from rural areas, who face complications during birth or who have instrumental-assisted or cesarean section birth. Also, every pregnant mother should be supported to have at least four regular antenatal care visits.
Introduction
The postnatal period is defined as the period from 1 h up to 42 days (6 weeks) after delivery of the placenta. It is both a special and a life-threatening period in the life of a woman and her newborn. 1 According to the World Health Organization (WHO), the postnatal period is the most critical and yet the most neglected phase in the lives of mothers and babies, 2 with most maternal and infant deaths occurring at this time. 3 Safe motherhood programs have recently increased the emphasis on the importance of postnatal care (PNC), recommending that all women receive a health checkup within 2 days, between 7 and 14 days, and 6 weeks after an uncomplicated birth. 3
Maternal satisfaction with respectful care during maternity service provision is one of the dimensions for the measurement of quality health care services.4,5 A postnatal visit is an ideal time to educate the mother, and it is recommended that all women receive at least three to four postnatal checkups. 6 Lack of care in this period may result in death or disability as well as missed opportunities to promote healthy behaviors for women, newborns, and children.7,8
Worldwide, more than half a million women die as a result of pregnancy, childbirth, or birth-related complications, 9 and Sub-Saharan Africa accounts for around 66% of these maternal deaths. 10 Low- and middle-income countries, where a large proportion of births take place at home, account for 99% of maternal deaths because PNC for mothers and neonates is either not available or is of poor quality.10,11 In Ethiopia, in 2011, only 17% of the women had received a PNC checkup in the first hour following birth. 12
To improve the quality of service as part of total quality management, the measurement of client satisfaction in autonomous health facilities should be carried out regularly as a basic indicator to define the strength and weaknesses of the provided services. 13 Few published studies have been conducted in Ethiopia and no study was conducted in this zone on maternal satisfaction and its contributing factors; therefore, this study is aimed to assess maternal satisfaction during PNC and associated factors.
Methods
Study design, period, and area
An institution-based cross-sectional study was conducted in the Awi Zone from 1 to 30 April 2018. The Awi Zone is located in Amhara regional state, 447 km north–west of Addis Ababa (the capital city of Ethiopia), and 118 km south of Bahir Dar (the capital city of Amhara regional state). In 2007, it had a total population of 982,941, of which 491,077 were reproductive age group women. 14 It has four public hospitals, and the study was conducted in two selected hospitals.
Study population
Participants were mothers who gave birth in selected health facilities of the Awi Zone during the study period.
Sample size determination
Epi Info version 7 software was used to estimate the sample size using a single population proportion formula with 95% confidence level and a 5% margin of error, as well as an estimated prevalence of satisfaction of 50% and non-response rate of 10%, the final sample size was 422 mothers.
Sampling procedure
Of the Awi Zone hospitals, two hospitals (one general hospital and one primary hospital) were selected using lottery methods. The samples were proportionally allocated to each hospital based on the average number of clients who received childbirth services in the respective hospitals, Changi 264 and Injbara 158. A systematic sampling technique was used to select study participants.
Data collection tools
A structured self or interviewer-administered questionnaire was prepared by reviewing relevant works of literature.4,15–19 The questionnaire was designed first in the English language and it was changed to local Amharic language by the translator and again it was changed back to English for further analysis. Three clinical nurses and two midwives (bachelor’s degree in science) were involved as data collectors and supervisors, respectively.
Data quality control
Before actual data collection, 2 days of training was given for data collectors and supervisors in questionnaire data collection in general and the questions in our questionnaire specifically. Before the actual study period, the instrument was tested on 21 (5%) mothers receiving PNC in a health center. The internal consistency of the questionnaire was checked via SPSS by reliability index measurement for satisfaction questions (Cronbach’s alpha) which was 0.86. The principal investigator and two supervising midwives supervised the performance of the data collectors daily and the data were checked for completeness and consistency. Finally, after data collection and before analysis, all collected data were checked for completeness.
Data processing and analysis
The analysis was done using SPSS version 22 software. Univariate analyses were done using frequency, percentage, tables, and charts. Associations between dependent and independent variables were assessed using logistic regression (both binary and multivariate). Odds ratios with 95% confidence intervals were calculated using logistic regression; a p-value less than 0.05 was considered statistically significant. Model fitness was checked with a Hosmer–Lemeshow test. Multi-collinearity was checked to see the linear correlation among the independent variables by using standard error. Variables with a standard error greater than 2 were dropped from the multivariate analysis.
Results
Socio-demographic characteristics of respondents
A total of 422 women participated in the study with a response rate of 100%. The mean age of the respondents was 25.62 (SD ± 5.2) years with a range of 15–51 years. A total of 348 (82.5%) respondents identified as Orthodox Christian; more than half (59.5%) of respondents were urban residents (Table 1).
Socio-demographic characteristics of respondents.
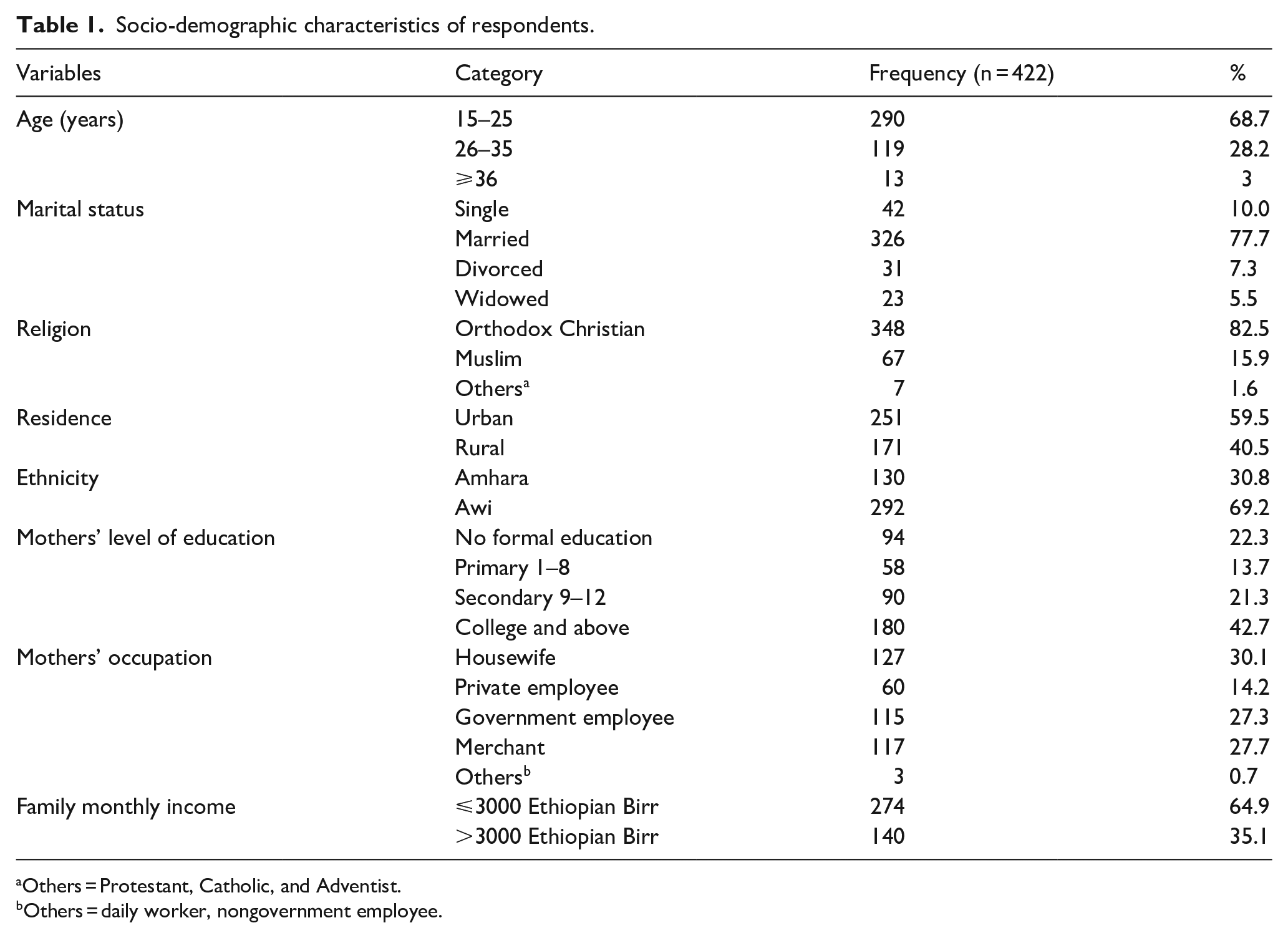
Others = Protestant, Catholic, and Adventist.
Others = daily worker, nongovernment employee.
Obstetric characteristics of respondents
In total, 379 (89.8%) respondents had a history of antenatal care (ANC) follow up; more than half (59%) of respondents were multigravida; almost all (87.9%) of the respondents had a previous history of institutional birth; 332 (78.7%) respondents had planned pregnancy; and the majority (80%) of respondents had a spontaneous vaginal birth (SVB) (Table 2).
Obstetric characteristics of respondents.

Post-partum maternal satisfaction
Almost all (83.6%) of the respondents reported that they were satisfied with the education given about postnatal exercises; more than three quarters (78.7%) of the respondents reported that they were satisfied that staff provided maternity services in a caring manner; and 293(69.4%) of respondents were satisfied with the time to discharge from the hospital. Also, 306 (72.5%) of the respondents were satisfied with decision making in post-partum family planning (Table 3). More than half (63%) of respondents were satisfied and 156 (37%) of respondents were not satisfied during PNC (Figure 1).
Category of post-partum maternal satisfaction.


Post-partum maternal satisfaction.
Factors associated with post-partum maternal satisfaction
In multivariate logistic regression residence, history of ANC follow up, mode of delivery, and those who had a history of complications during birth were significantly associated with post-partum maternal satisfaction at p-value less than 0.05.
Respondents who reside in urban areas were 2.1 times (AOR = 2.1; 95% CI = (1.11–3.99)) more likely to be satisfied than respondents from rural areas. Respondents who had a history of ANC follow up were 1.62 times (AOR = 1.62; 95% CI = (1.23–1.64)) more likely to be satisfied than their counterparts. Respondents who had an SVB were 3.14 times (AOR = 3.14; 95 % CI = (1.77–3.28)) more likely to be satisfied than those who had instrument-assisted vaginal birth/cesarean section. Respondents who did not face any complications during birth were 2.9 times (AOR = 2.90; 95% CI = (1.47–1.69)) more likely to be satisfied than their counterparts (Table 4).
Factors associated with post-partum maternal satisfaction.

OR: odds ratio; CI: confidence interval; COR: crude odds ratio; AOR: adjusted odds ratio.Discussion
The finding of this study revealed that 37% of respondents were not satisfied during PNC with 95% CI (32–42). The finding of this study is consistent with studies conducted in India (39%) and Greece (38%).4,15 This study is higher than studies conducted in Sweden, Iran, and in Alexandria in Egypt which showed that the prevalence of maternal dissatisfaction during the postnatal period was 26%, 18%, and 30%, respectively, but it is lower than a study conducted in Cairo in Egypt, which showed that 71% of the respondents were not satisfied.16–19 The difference might be due to the difference in the study area and the difference in the socio-economic and cultural aspects of care provision. Another possible explanation might be due to the gap in the health care delivery policy system, infrastructure, and knowledge of health care providers. The difference in results may also have been affected by sampling size and study period deference.
Regarding significant factors associated with satisfaction of mothers, this study found that residence, ANC follow up, mode of delivery, and any complications during birth had a statistically significant association with post-partum maternal satisfaction. Urban respondents were 2.1 times more likely to be satisfied than the rural respondents. This might be because urban residents are found near to health institutions so that they may receive all necessary information and are more likely to have an institutional delivery with fewer complications.
Respondents who had a history of ANC follow up were 1.6 times more likely to be satisfied about PNC as compared with those respondents who had no history of ANC follow up. Those who had regular ANC follow up are likely to have received better information on birth preparedness and complication readiness plan, which in turn may lead to greater satisfaction after delivery.
Respondents who had SVB were three times more likely to be satisfied with PNC than those respondents who had instrument-assisted vaginal birth or cesarean section. Respondents who did not face complications during birth were 2.9 times more likely to be satisfied than those who faced complications during birth. Respondents who face complications during birth might have greater pain and features of post-partum depression, which in turn may make them less satisfied after delivery.
Conclusion
According to the results of this study, 63% of mothers were satisfied with post-partum care services. The study findings indicate that maternal satisfaction on post-partum care is mainly affected by residency, ANC follow up, mode of delivery, and complications during birth. Therefore, special attention must be given to mothers who come from rural areas, have not attended ANC follow up, or have had instrument-assisted vaginal births or cesarean section or faced complications. If every pregnant mother is able to attend at least four regular ANC visits, this may improve maternal post-partum satisfaction, and every effort should be made to improve women’s attendance to ANC visits during pregnancy.
Footnotes
Acknowledgements
The authors would like to thank data collectors, and respondents who participated in this study.
Author contributions
Both authors contributed to the conception and design of the study to the fieldwork, and finalizing the work. They conceived the idea, approved the work and revised thoroughly, and read and approved the final manuscript. B.W. designed the study, collected and supervised the field data, undertook the analysis, and produced the draft of the manuscript. D.A. reviewed and contributed to the final draft.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and informed consent
The study protocol was ethically approved by the Ethical Review Board of Bahir Dar University and it was one of the components of master’s thesis. Awi Zone Health Bureau wrote an official letter to each hospital. Accordingly, after the objective of the study was explained, verbal informed consent was obtained from each participant above the age of 18 years. In addition to this, verbal consent was obtained from a parent on behalf of the participants below the age of 18 years. Moreover, the confidentiality of information was guaranteed by using code numbers rather than personal identifiers and by keeping the data locked