
Abstract
Background:
The quality of antenatal care (ANC) plays a crucial role in maternal and child health, yet little is known about the actual service content received by pregnant women in rural southern Ethiopia.
Objectives:
To explore the factors influencing ANC content utilization in selected rural areas of southern Ethiopia, shedding light on critical gaps in service delivery.
Design:
A mixed-methods study.
Data Sources:
Quantitative data were collected from 851 systematically selected women, and qualitative data from 20 purposefully selected participants including mothers, health extension workers, and healthcare professionals.
Methods:
Data were collected using a pre-tested structured interviewer-administered questionnaire. Quantitative data were analyzed using descriptive statistics and a generalized linear model to assess associations between variables. Qualitative data were transcribed, translated verbatim, and processed using Atlas software.
Results:
Only 5.7% of women received the full spectrum of ANC services. Weight (82.6%) and blood pressure (82%) measurements were the most commonly utilized services, while height measurement (22%) and counseling on pregnancy-related complications (31%) were significantly underutilized. Key determinants of ANC content utilization included husband support (risk ratio (RR) = 1.82, 95% CI = 1.01–2.43), perception of proximity to a health facility—short (RR = 1.38, 95% CI = 1.08–1.90) and medium (RR = 1.13, 95% CI = 1.00–1.17) distances—early initiation of ANC (RR = 1.6, 95% CI = 1.01–2.20), positive provider–patient interaction—good (RR = 1.22, 95% CI = 1.03–1.41) and medium (RR = 1.18, 95% CI = 1.00–1.27)—and a high wealth index (RR = 1.26, 95% CI = 1.16–1.37).
Conclusions:
This study underscores the critical shortfall in comprehensive ANC service utilization in rural Ethiopia. Strengthening health services in underserved areas, actively involving husbands in maternal care, empowering women, and enhancing healthcare provider training and accountability are essential to improving service delivery. A concerted effort is needed to bridge these gaps and ensure that every pregnant woman receives the full spectrum of essential ANC services.
Plain language summary
Antenatal care (ANC) is essential for ensuring the health and well-being of both mothers and their babies during pregnancy. However, in many rural areas of Ethiopia, the level of ANC services that pregnant women receive varies, and little is known about whether they receive all the recommended services. This study aimed to assess the factors that influence the use of ANC services and whether they meet the World Health Organization (WHO) guidelines. We conducted a study in selected rural areas of southern Ethiopia, using both surveys and interviews. Our findings show that only 5.7% of pregnant women received all essential ANC services. The most commonly provided services were weight and blood pressure measurements, while services like height measurement and counseling on pregnancy-related complications were less frequently offered. Several factors influenced whether a woman received complete ANC services, including support from her husband, how close she lived to a health facility, her perception of how healthcare providers treated her, her family’s wealth, and how early she started ANC visits. These results highlight the need for improved ANC services in rural Ethiopia. Efforts should focus on involving husbands in maternal healthcare, ensuring healthcare workers treat patients with respect, increasing accessibility to health facilities, and strengthening health system policies to guarantee that all pregnant women receive comprehensive ANC services.
Introduction
In 2015, complications during pregnancy and childbirth killed about 830 women every day around the world; approximately 99% of these deaths happened in the developing countries.1,2 Also, about 2.6 million stillbirths in the year 2015, most of which happened in developing countries. 3 Although pregnancy-related complications and deaths are not inevitable, most are preventable with simple and cost-effective maternity care (antenatal care (ANC)) during pregnancy.4,5 ANC remains a significant public health action for preventing maternal and neonatal mortality worldwide by enhancing the chances of accessing life-saving obstetric care. 6 Timely and appropriate antenatal practices have life-saving potential for mothers and children. Several studies have shown that ANC alone can reduce maternal mortality by 20%. 7
The World Health Organization (WHO) recommends that to make ANC services an effective preventive measure, the content and quality of care should be routinely monitored. 8 The mother should receive all components of ANC through multiple visits during pregnancy, in line with the WHO recommendation of at least eight contacts to improve maternal and fetal outcomes. These components include physical examinations (such as weight, height, blood pressure measurement, and fetal heartbeat assessment), laboratory investigations (urine and blood samples), screening for infectious diseases (such as HIV, syphilis, and hepatitis B), preventive measures (such as tetanus toxoid vaccination, iron and folic acid supplementation, and deworming), nutritional interventions, birth preparedness planning, and information and counseling on pregnancy danger signs, nutrition, breastfeeding, family planning, and newborn care, which should be provided throughout the pregnancy period. Ethiopia adopted these updated ANC services in line with WHO recommendations through its 2020 management protocol.9,10
However, very few pregnant women received the full package of ANC in line with the WHO recommendation of at least eight contacts and the national protocol. Local studies done in Addis Ababa and Debre Tabor revealed that approximately 19.6% and 10.1% of women, respectively, received ANC services that met the recommended content and frequency throughout pregnancy. 11 To attain national goals or meet international standards, ANC services should be sufficient and comply with the recommendations of national protocols or WHO guidelines. 12 Many crucial services that support the health of the mother and baby are overlooked, even in women who have had the recommended number of visits and started the first ANC visit within the recommended time. 13
Even though it is known that socioeconomic, demographic, and reproductive factors can affect how well maternal healthcare services are used and provided in Ethiopia, most studies on ANC focus on whether women attended ANC (coverage), the timing of the first visit, and the number of visits. Few studies have examined the actual content of care provided during these visits, particularly in rural settings.14,15 This gap in evidence limits efforts to ensure that ANC services contribute fully to achieving the Sustainable Development Goal targets of reducing maternal and neonatal mortality by 2030. Thus, this study aims to address this gap by assessing the factors associated with ANC service content utilizations in compliance with WHO recommendations. A full package of ANC services that includes all necessary evidence-based interventions is essential to realize the life-saving potential that ANC promises for mothers and babies
Methods
Study design and setting
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement for cross-sectional studies. 16 The reporting of the qualitative component of this study conforms to the Consolidated Criteria for Reporting Qualitative Research (COREQ) statement. 17 A mixed-methods study was conducted from October 15 to December 10, 2021, in the rural areas of the Wolaita and Dawro zones. Wolaita Sodo is the administrative capital of the Wolaita zone, located 380 km south of Addis Ababa, whereas Tercha, the capital of the Dawro zone, is located 500 km away. The Wolaita and Dawro zones have 22 and 12 districts, respectively. These zones are characterized by a high rural population, with 88.3% and 92.9% of Wolaita and Dawro residents being rural dwellers, respectively. The female population accounts for approximately 49% of the total population in both zones. 18 The Wolaita and Dawro rural zones were selected for this study because of their predominantly rural populations and the known challenges these areas face in accessing and utilizing maternal health services. These zones are characterized by geographic barriers, limited health infrastructure, and socioeconomic constraints, which are common issues in rural Ethiopia that can affect the uptake of comprehensive ANC services.
Population
The participants of the study were women of childbearing age who had given birth in the 1–2 years before the survey, no matter how the birth went, and who had at least one ANC follow-up for the pregnancy of their most recent child. Women who have lived in the study area for over 6 months and delivered their most recent baby after 28 weeks of gestation were included. Women who were very sick or had mental problems when the information was being collected were not included in the study. For the qualitative study, healthcare professionals (midwives), women development armies (WDAs), health extension workers (HEWs), and mothers who did participate in the quantitative study were all included.
Measurement variables and definitions
Outcome variables
The outcome variable of this study was ANC service content utilization throughout the pregnancy of the most recent birth. Information on each of the 12 recommended contents of ANC components was received from the participants by asking questions like “As part of antenatal care during the pregnancy of late birth, have you received any of the following at least once? Such as have you been weighed? Have you been counseled on pregnancy-related complications?” Responses were recorded as 1 for “yes” and 0 for “no.” Based on their responses, we created a compound index of the ANC component as our outcome variable which comprised a simple count of the number of elements of the ANC received. The variable had a minimum value of 0 and a maximum value of 12 indicating that the women received all elements. A similar type of content index was used in other studies. 12
Predictor variables
The predictor variables were conceptualized based on the Anderson–Newman Behavioral Model of healthcare utilization and then grouped into three sets of factors: predisposing, enabling, and need factors.16,17
Predisposing factors
These reflect individuals’ inclination to use maternal health services. These include maternal education, marital status, maternal employment status, age, partner education, mass media exposure, previous use of ANC, having best friends who use maternal care, and the number of live births.
Enabling factors
These are resources/factors that might facilitate access to health services. These are husband/partner support, wealth index, involvement in decision-making, and type of health facility.
Need factors
These factors increase/decrease the potential need for maternal health service use. These include maternal knowledge about pregnancy-related complications, reasons for ANC follow-up, maternal perception of the provider–patient approach, pregnancy intention, and previous history of a risky pregnancy.
Women development armies
WDAs are networks of community volunteers who mobilize, educate, and support maternal and child health initiatives at the grassroots level, while HEWs are government-employed frontline health workers responsible for delivering basic health services, including maternal and child healthcare, at the community level.
Sample size determination and sampling procedure
To determine sample size, a single population proportion formula was used with the following assumptions: 20.2% 9 proportion of women receiving adequate ANC service content, a 95% confidence interval, a 4% margin of error, and a design effect of 2. For possible non-responses, 10% was added, and the final sample size was 851. A three-stage sampling procedure was used to select study participants. In the first stage, six districts were chosen by lottery: four from the Wolaita zone (Sodo Zuria, Kindo Koysha, Damot Sore, and Boloso Bombe) and two from the Dawro zone (Loma and Mareka). In the second stage, two kebeles (the smallest administrative unit in Ethiopia, with approximately 5000 people) were randomly selected from each chosen district. Finally, households were selected using systematic random sampling from each kebele after eligible women—those who had given birth within the last 2 years—were identified with the support of HEWs using the health management information system registration log sheet. Both women who delivered at health facilities and those who gave birth at home were included in the study.
For the qualitative part, 20 in-depth interviews were conducted with mothers who did not participate in the quantitative questionnaire (8), WDAs leaders (4), HEWs (4), and healthcare professionals (4) in the study catchment areas. The sample size for in-depth interviews was guided by data saturation.
Data collection tools and methods
The inclusion of variables was guided by the Andersen and Newman Behavioral Model of Health Service Utilization,16,17 a well-established framework that explains health service use through the interplay of predisposing factors (such as demographic and social characteristics), enabling factors (including resources and access), and need factors (both perceived and evaluated health needs). This model was instrumental in structuring the selection and categorization of independent variables to comprehensively assess their association with ANC service content utilization in the study population. For the quantitative component, a structured questionnaire was developed based on this framework and a thorough review of relevant literature. The questionnaire encompassed multiple sections, including sociodemographic details (age, education, marital status), obstetric history (parity, previous pregnancy outcomes), healthcare accessibility (distance to facilities, transportation), and specific measures of ANC service utilization and satisfaction. The original questionnaire was composed in English, translated into the local language by bilingual experts, and then back-translated into English by independent translators to verify semantic accuracy and conceptual equivalence, ensuring the tool’s cultural appropriateness and clarity. To complement quantitative data, a semi-structured interview guide was crafted for the qualitative component to capture in-depth insights into participants’ perceptions, experiences, and barriers related to ANC services. This guide contained open-ended questions exploring themes such as physical accessibility of services, perceived quality and respectfulness of care, cultural beliefs influencing health-seeking behaviors, and health system challenges. It was reviewed by subject matter experts for content validity and piloted in a comparable community to identify and address any ambiguities or culturally sensitive items. Data collection was performed through face-to-face interviews and focus group discussions conducted in private, comfortable settings to foster candid dialog. Each interview lasted between 30 and 60 min. The data collection team consisted of 12 HEWs and two nurses with MSc degrees, all experienced in both qualitative and quantitative data collection methods. Prior to data collection, the team underwent intensive training on the study objectives, ethical standards including informed consent and confidentiality, proper use of the data collection tools, and strategies to minimize interviewer bias. Throughout the data collection period, supervisors conducted routine field visits and spot-checks to monitor adherence to protocols, ensure data completeness and accuracy, and provide ongoing support to the field team, thereby maintaining the overall quality and consistency of data gathered across both study components (Supplemental Material).
Open-ended questions were used for qualitative interviews. In-depth interviews were conducted by the lead researcher alongside an assistant who tape-recorded the interviews. Informed consent was obtained from all participants prior to data collection. This included consent for participation in the study as well as for audio recording of interviews where applicable.
In the study setting, the expected content of ANC services follows national and WHO guidelines. These services include blood pressure measurement, urine and blood tests (including hemoglobin estimation and HIV screening), tetanus toxoid vaccination, iron and folic acid supplementation, deworming, health education on nutrition and birth preparedness, and counseling on danger signs. Priority is generally given to essential components such as blood pressure monitoring, screening tests, and tetanus immunization, as these are critical for early detection and prevention of maternal and fetal complications.
Data quality control
The study tool was pre-tested on 43 women living in the Damot Gale district. All required revisions were made to the study tool based on the pre-test. Twelve data collectors and supervisors (two MSc nurses) with the required experience in data collection and supervision were recruited. A 2-day training about the aim of the study and the sampling procedure was provided to the data collectors. To ensure the correct inclusion of the participants, we made a random selection of the districts, kebelles, and interviewees. Audio recording was used. To reduce recall bias, we used a recall period of up to 2 years, similar to the United Nations Children’s Fund-supported Multiple Indicator Cluster Surveys, 19 which is far shorter than that for Demographic and Health Surveys (up to 5 years). The supervisors cross-checked the completed questionnaires by repeating the interviews with 10% of the respondents to check for correct completion. The principal investigator double-checked for any inconsistencies and gave feedback to the interviewers daily. Before commencing data analysis, appropriate transformations were made to the variables. An in-depth interview guide and field notes were used to not miss any relevant information.
The data collection instruments were adapted from standardized and previously validated questionnaires used in similar studies. To ensure reliability and clarity, the tools were pretested on a sample from a population similar to the study participants but not included in the main analysis. Based on the pretest findings, necessary modifications were made to improve the comprehensibility and relevance of the questions. Internal consistency was checked, and data collectors received training on the study protocol and the use of the tools to enhance data quality and minimize bias.
Data management and statistical analysis
The data were entered into Epi-data version 3.1.1 and then moved to STATA software version 15 (StataCorp LLC, College Station, Texas, USA) so that it could be analyzed. Descriptive statistics were used to characterize the sample. In bivariate analysis, the mean for the count variable (number of ANC items received during visits) was obtained for each category of the selected explanatory variables to examine the unadjusted statistically significant relationship between dependent variables and selected independent variables. The statistical significance was tested by analysis of variance (ANOVA). The ANOVA statistical approach was applied to identify the role of each factor in by comparing the means across the main factors. Variables with a p-value of ⩽0.2 were retained for further consideration with a generalized linear model to explore the association by controlling confounders. Negative binomial regression was used for estimating the regression coefficients. Finally, the risk ratios (RRs) and the corresponding 95% confidence interval were calculated. A p-value of less than 0.05 was used to determine the cut-off points for statistical significance. Multicollinearity was assessed using variance inflation factors (VIF). A VIF value above 4 indicates the presence of multicollinearity.20–23 In this study, the maximum VIF was 2.68, confirming that multicollinearity was not a concern.
The qualitative data were analyzed using thematic content analysis to explore participants’ perceptions of the barriers and facilitators influencing the utilization of ANC service content. First, all audio-recorded interviews were transcribed verbatim into Amharic, the local language, and then translated carefully into English to preserve meaning and context. The English transcripts were imported into ATLAS.ti software to facilitate systematic data management and analysis (ATLAS.ti Scientific Software Development GmbH, Berlin, Germany). Using an inductive approach, initial open coding was conducted to identify meaningful segments and ideas related to ANC service utilization. Data saturation was discussed during the data collection process and was considered achieved when no new themes or insights emerged from subsequent interviews. Similar codes were then grouped into categories, which were further refined and synthesized into broader themes representing key factors affecting ANC service content use.
Trustworthiness and reflexibility
Trustworthiness was ensured through several techniques applied during the qualitative part of the study. We conducted prolonged engagement in the study areas to build rapport and gain deeper understanding of the context. Data source triangulation was employed by including different participants—mothers, WDA leaders, HEWs, and healthcare professionals—to obtain diverse perspectives on ANC service utilization. Member checking was done during interviews by summarizing key points back to participants for confirmation or clarification. Informed consent for audio recording was obtained from the study participants. An audit trail was maintained throughout the study process, including detailed field notes, reflexive memos, and documentation of coding and analysis decisions. Peer debriefing was undertaken during analysis, with regular discussions among the research team to review emerging themes and challenge interpretations.
Ethical statements
Ethical approval for this study was obtained from the Academic Research Directorate of Wolaita Sodo University (CHSM/ERC/06/15). Written informed consent was obtained from all participants prior to data collection. Participants were fully informed about the purpose of the study, their rights, and the voluntary nature of their participation. Confidentiality and privacy were strictly maintained throughout the research process, and no personal identifiers were recorded. Participants were free to withdraw from the study at any time without any consequences.
Results
Sociodemographic characteristics of study participants
From a total of 851 study participants, 845 have participated, which makes the response rate 99.3%. The mean age ± standard deviation (SD) of participants was 24.4 ± 5 years. The majority of mothers have not attended any formal education (515 (60.9%)), were unemployed (744 (88.0%)), were married (810 (95.9%)), had a husband who attended at least primary education (509 (62.8%)), and had no exposure to mass media (722 (85.4%)). The majority of the women did not have a best friend who uses maternal care (575 (68.0%)) and claimed that this did not involve them in the decision-making of about their maternal health (524 (62%)), while 338 (40.0%) of the mothers belonged to a high wealth index group (Table 1).
Sociodemographic characteristics of study participants in rural areas of Wolaita and Dawro Zones, Southern Ethiopia, 2021.
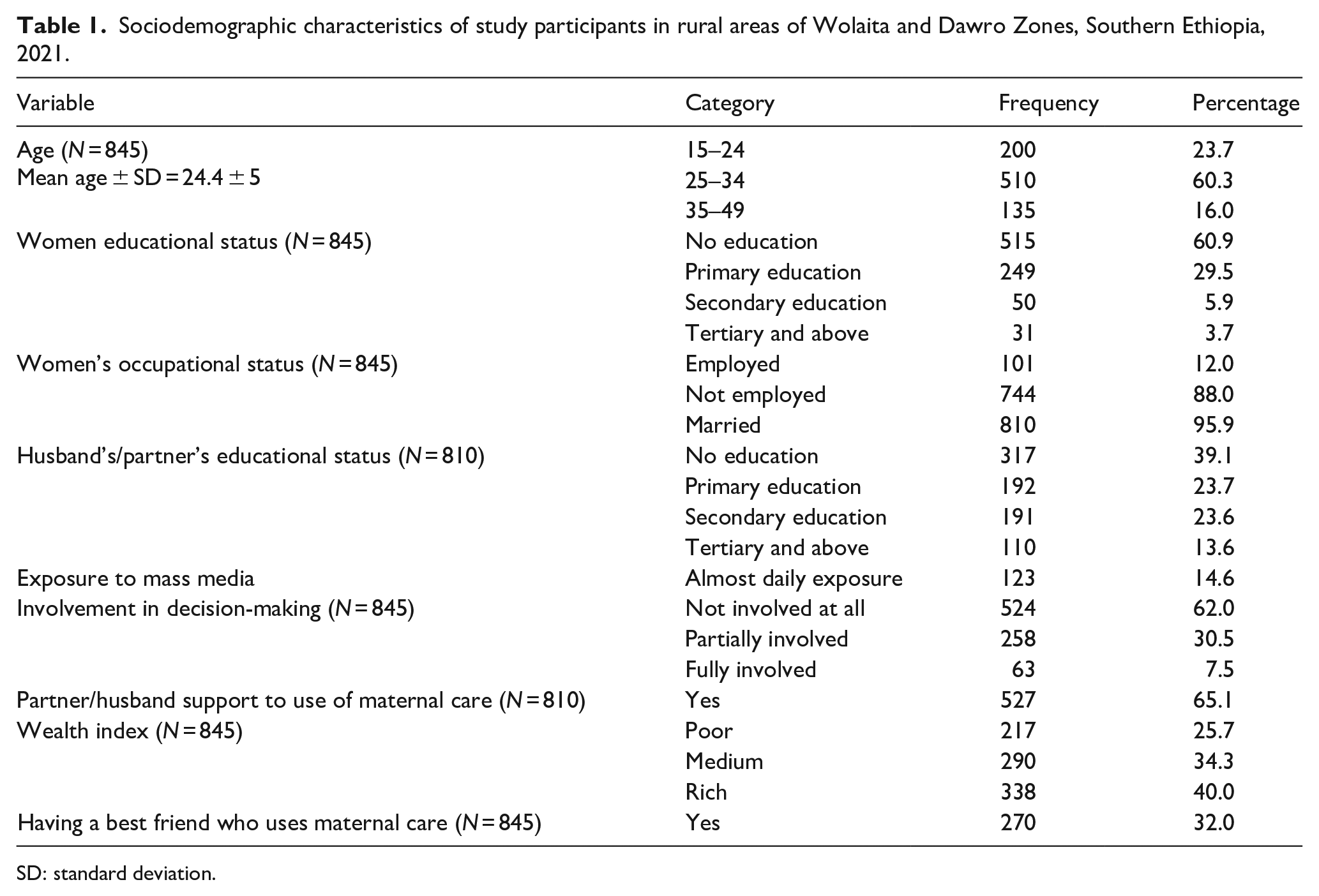
SD: standard deviation.
Reproductive history, knowledge, and perception-related characteristics of participants
About 527 (62.4%) and 506 (59.9%) of women had >3 children in their lifetimes, and their pregnancy for new birth was unintended, respectively. The majority of women had a previous history of ANC follow-up 671 (79.4%) and had no history of a risky pregnancy 518 (61.3%). The major source of ANC-related information for about 584 (69.1%) participants was health professionals. The majority of mothers had poor knowledge of pregnancy-related complications (634 (75.0%)) and reasons for ANC follow-up (587 (69.5%)). About 807 (95.5%) of participants received ANC from public health facilities, and 477 (56.1%) perceived that the proximity of the health facility where they received ANC was medium. Only 29.7% and 39.5% of the mothers perceived the waiting time to receive ANC was as short timescale and the provider approach was good, respectively. About 28.6% and 48.3% of women started the first visit within the first 12 weeks of pregnancy and had four or more ANC visits, respectively (Table 2).
Reproductive history, knowledge, and perception-related characteristics of participants in rural areas of Wolaita and Dawro Zones, Southern Ethiopia, 2021.

Antenatal care service utilization
Figure 1 shows the distribution of participants according to ANC service content utilization. The current analysis showed that the number of contents received by participants ranged from 4 to 12 out of a total of 12 contents, with a mean ± SD of 7.96 ± 0.085. Only 48 (5.7%) mothers received all recommended 12 ANC service contents at least once during the pregnancy of the newest birth. The higher percentage of women 149 (17.6%) received 8 out of 12 components, followed by those who received 7 and 9 out of 12 with the same proportion of 13.8%. About 11.9% and 12% of mothers received 6 and 10 service contents, respectively. Additionally, 9.2% of mothers received 11 service items, and this is equivalent to those who received 5 out of 12 items. The remaining 6.8% of mothers received four out of the total recommended content, and this was the lowest range of content received by the participants (Figure 1).

Percentage distribution of number of antenatal care service contents received by women in rural areas of Wolaita and Dawro Zones, Southern Ethiopia, 2021.
Regarding individual service content utilization, weight measurement was the most common item received by 703 (82.6%) of mothers, closely followed by blood pressure measurement, which was received by 693 (82.0%) of participants. The majority of mothers were reported to have had urine exam tests (60.1%) and fetal heart rate measurement (61.5%). More than half of mothers also reported having symphysis-fundal height measurement 494 (58.0%) and blood type tests 451 (53.3%), while less than half of participants reported having tetanus toxoid vaccine 357 (42.2%), anemia tests 349 (41.3%), and syphilis tests 340 (40.2%). The least received ANC service content reported by the participants was height measurement at 189 (22.2%), followed by counseling about pregnancy-related complications at 264 (31.2%; Figure 2).
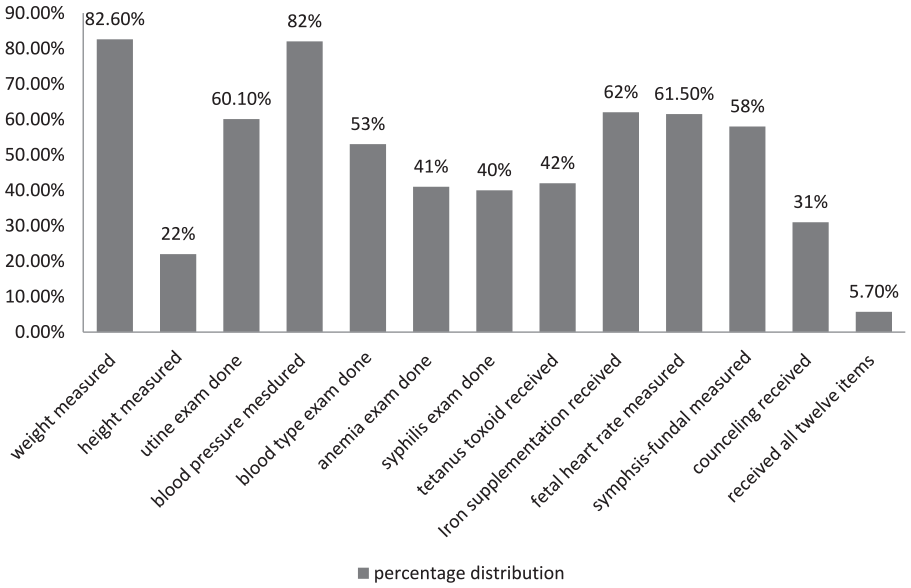
Percentage distribution of each recommended ANC content among mothers in rural areas of Wolaita and Dawro Zones, Southern Ethiopia, 2021.
Factors associated with receiving sufficient ANC service contents
During bivariate analysis, women’s employment status, her husband’s educational status, pregnancy intention, husband support, having experience of a risky pregnancy, knowledge about pregnancy-related complications, knowledge about reasons for ANC follow-up, the site of the health facility where ANC was received ANC, the perception of proximity to nearby health facilities, the perception of the provider–patient approach, the timing of the first visit, the frequency of visits, and the wealth index were associated with receiving sufficient numbers of service items with a p-value of ⩽0.05 (Table 3).
Bivariate association of ANC service utilization with some selected variables.

ANC: antenatal care.
Using a multivariable generalized linear model to control for possible confounding factors, only husband support, perception of closeness to health facilities, perception of provider–patient approach, timing of the first visit, and the wealth index were found to be significant factors in receiving adequate ANC service items.
In our analysis, enabling factors such as husband support and wealth index showed a significant association with the number of ANC service elements received by the mother. Women whose husbands supported them to follow ANC service were 1.62 times more likely to receive a sufficient number of ANC items than those who did not gain support from their husbands (RR: 1.82, 95% CI: 1.011–2.433). Women who belonged to the high wealth index group were 1.26 times more likely to receive a high number of ANC service items than those who belonged to the low wealth index group (RR: 1.26, 95% CI: 1.161–1.369).
Perception of proximity to a nearby health facility and perception of the provider–patient approach were important need factors significantly associated with ANC service content utilization. Women who perceived proximity to the nearby health facilities as short were nearly 1.38 times more likely to receive a sufficient number of ANC items than those who perceived long (RR: 1.38, 95% CI: 1.079–1.896). Women who perceived proximity to the nearby health facility as medium were 1.13 times more likely to receive high ANC service content than those who perceived long (RR: 1.13, 95% CI: 1.039–1.236).
In this study, women who perceived the health provider–patient approach at health institutions as good and medium were 1.22 and 1.18 times more likely to receive a high number of ANC service items than their counterparts (RR: 1.22, 95% CI: 1.029–1.411, RR: 1.18, 95% CI: 1.004–1.267). Furthermore, women who started the first ANC visit within the first 12 weeks of pregnancy were 1.6 times more likely to receive a high number of ANC service items than those who had fewer than four ANC visits (RR: 1.6, 95% CI: 1.013–2.322; Table 4).
Results of generalized linear model analysis with a negative binomial log link to identify determinants of ANC service content utilization.
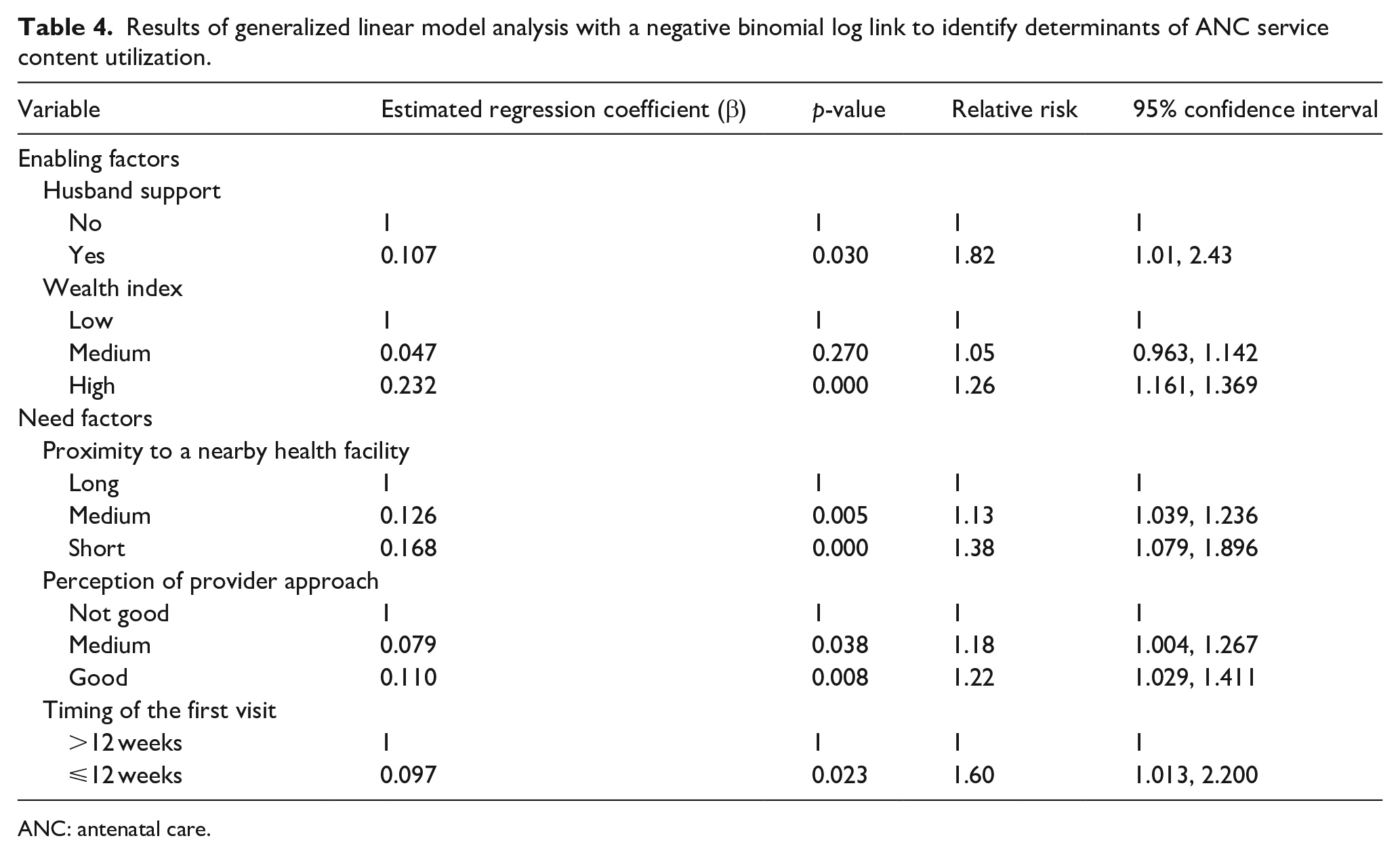
ANC: antenatal care.
Findings of the qualitative study
Barriers to the provision and reception of adequate ANC content
Our quantitative results showed that quite a few women received an adequate number of ANC contents. The qualitative findings exposed some themes that could explain some of the barriers and facilitators to the adequacy of the content and why fewer women in our study areas had sufficient service content throughout the pregnancy.
Husband support
Husband support was raised as a theme in the qualitative study. It has a positive influence on the women’s intent to receive adequate care. It was reported that the more women being supported by their husbands/partners they become more adherent to the services, and they become likely to navigate what quality ANC should include. It was revealed that in the rural areas of Ethiopia where women has been less likely to be educated and more likely to be culturally dominated by men, husbands are found to be the ones who put a decision in a family and women have less courage to do what they think is right unless approved by their partner/husband. More important than none, women were found to be more emotionally dependent on their husbands’ ideas and perspectives.
For example, a 32-year-old mother of four children explained that: “. . .during my first pregnancy my husband would have been there for me in any manner, even if that meant going with me while I went to seek antenatal care. His company would help assist me in speaking with the professionals confidently and gathering information from a variety of sources. Then, as he get used to the view that pregnancy is not a disease and there is no need to constantly attend the health care system, his support diminished with the succeeding pregnancies. I also became careless about the services I got, unlike my first child.”
Another 30-year-old midwifery who has 8 years of work experience explained: “. . .Most mothers who are not being supported to utilize the service by their husband barely come to the health service, and they are unlikely to start ANC follow-up and to have an adequate number of visits. Most importantly, they spend way less time, which is enough to provide the services in the facility, out of fear of their husbands’ acknowledgment of their attendance. So they missed out on most of the contents.”
Maternal involvement in family decision-making
Most participants in the qualitative raised a notion that mother has much less right to say the last “yes” or “no” even if the issue is about her maternal health in rural areas. Most things have been decided by the husband, as he is more likely to be the head of the household. In the households where women have no or little involvement in decision-making, it is also emphasized in the interview that they ended up with inadequate service content.
A 33-year-old diploma midwifery with a 5 years of work experience explained as the following: “. . .if the mother has the right to express her ideas and thoughts regarding what is best for her child and her health, she can persuade her husband and can freely use the services with better quality.”
Additionally, a 43-year-old WDA also shared similar information as the following: “. . .in families where the mother has the final word in matters affecting the health of the mother, she probably acquires and shares in8formation in our discussions about antenatal care follow-up and the services it entails.”
Proximity to a nearby health facility
It had been discussed in the in-depth interviews that in most rural areas of Ethiopia, women started the ANC visit at their nearest health posts, then after, they have transferred to the health centers after the third visit for they have needed better treatment and laboratory tests. The areas where these health centers are built are not near most of the clients and need extra cost for transportation. It is also repeatedly mentioned in the interview that the farther away the health facility, the more clients miss out on the essential services they should have received during pregnancy.
A HEW who has 4 years of experience explained: “We advised them to come back during their attendance at the health center since their third-time follow-up, but they were unable to do so due to the distance and the cost of transportation, thus they missed certain treatments.”
A health provider who was 40-year-old also explained how mothers and HEWs felt about the distance as the following: “Because these facilities were far from where the women resided and deserved additional travel costs, health extension workers who provided treatment in hard-to-reach areas occasionally held back on referring needy mothers to other health centers that offered tests, especially if they thought the mother was healthy and not in that serious need of some services.”
Provider–patient approach
It was discussed during the in-depth interview that having a good client–provider approach is the right of clients and an important part of ensuring that the care is high quality and acceptable. While there is a respectful approach, providers deliver the service with friendly and helpful counseling to their patients, and mothers will openly express their opinions, which in turn enhances the quality of the services offered. However, in many settings where the majority of professionals have higher dissatisfaction with the restrictions of working in a rural area and mothers instead opted to arrive late at the health institution and refuse to stay there as long as was necessary to provide sufficient care. So, this all drives disrespectful behavior and contributes to women’s poor experiences with the care.
A multipara woman explained that: “Mothers even regret visiting the medical institution because of the way staff members scold the patient. Most of the time professionals (working in health centers) do not see people from rural areas as human beings who deserve even some respect. This happened to me 4 years ago while I was pregnant with my 4th child. The nurse made a look at me while I entered the clinic and I felt like I am not in the right place, I hurriedly went back to my home to pull myself together without receiving the care I should receive. When I opened up about my experience to my friends, they told me even worst” (Table 5).
Sociodemographic characteristics of in-depth interview participants.

Discussion
Identifying the factors that determine the utilization of adequate ANC services is a matter of great policy concern for the government and other stakeholders. To the best of our knowledge, there are limited studies that specifically assess the level of ANC service utilization and its associated factors in Ethiopia, let alone in the study area. Therefore, this study aimed to identify the predisposing, enabling, and need factors influencing ANC service utilization in selected rural areas of Southern Ethiopia.
In this study, 48 (5.7%) of women received all 12 of the basic antenatal services recommended by WHO at least once. This finding was lower than previous studies conducted in Ethiopia.9,11 The existing difference in these studies might be because of the difference in the study population and settings; unlike previously mentioned studies the current study takes place in rural areas of the country where there is a lack of awareness about essential ANC service contents and a lack of adjacent health facilities rendering the service.
The level of sufficient service item utilization in this study was also much lower than in studies conducted in Bangladesh and Uganda.24,25 The shown difference could be due to differences in population, where there are clear differences in sociocultural background and poor community attitude toward the utilization of ANC that would probably have led to less people using ANC service content. Also, how different these studies are depends a lot on how committed health professionals are to providing ANC services. 26
Support from the husband was what made it more likely for women to use ANC service contents. Consistent with these studies,27,28 the current study also revealed that women whose husbands supported them to receive ANC services were 1.8 times more likely to receive a high number of ANC service contents than their counterparts. This might be because most women in developing countries need their husband’s consent to seek health services, including ANC; the husband should have a supportive attitude toward health services, thereby letting his wife attend the services.
Also, studies from the past have shown how important socioeconomic status is when it comes to how ANC content is used.29–33 Women who belonged to the high wealth index, compared to those who belonged to the low wealth index, were more likely to use the ANC content. In line with these studies, 34 the current study showed that mothers who belonged to a high wealth index were 1.26 times more likely to receive a high number of ANC items as compared to their counterparts. This can be explained by evidence showing that economic factors influence women’s health-seeking behavior in multiple ways. Limited financial resources can restrict a woman’s ability to afford direct costs (such as consultation fees, laboratory tests, and medications) as well as indirect costs (such as transportation and childcare). 35 In addition, low socioeconomic status is often linked with reduced decision-making autonomy, which can further delay or prevent timely care-seeking. 36 Studies have also shown that poverty increases vulnerability to social and structural barriers, including distance to health facilities, poor awareness of available services, and low levels of trust in the health system. 37 Together, these factors reduce the likelihood of utilizing ANC and other essential maternal health services.
Women who perceived proximity to an adjacent health facility that provides ANC service as short and medium were nearly 1.38 and 1.13 times more likely to increase the number of ANC contents received, respectively than those who perceived long. This result was the same as what a study done in Nigeria found, which was that a high score of ANC attributes was linked to easy access to health facilities. 38
The provider–patient interaction/approach has a pertinent influence on the utilization of ANC service contents. Women who perceived the provider’s approach with the patient in the health facilities as good and medium were nearly 1.22 and 1.18 times more likely to receive a higher number of ANC items, respectively than those who perceived the provider’s approach was not good/immoral. This might be because good provider–patient interaction enhances knowledge about the service in charge and the health-seeking behavior of individuals, which in turn increases maternal adherence to the treatment.
Furthermore, the current study revealed that women who started their first ANC visit within the first trimester/within 12 weeks of pregnancy were 1.6 times more likely to receive high odds of ANC service items than their counterparts. This study was supported by previous studies which stated that early initiation of ANC allows clients to have an adequate number of visits and sufficient service contents.39,40
Limitations of the study
To minimize recall bias, the study included only pregnancies that occurred within 2 years prior to the survey, thereby limiting the timeframe in which participants needed to recall their experiences. This approach helps improve the accuracy of the data, as longer recall periods are often associated with increased errors in reporting. Service content was evaluated by asking respondents to describe the ANC services they received during their most recent pregnancy. Despite these efforts to enhance recall accuracy, there remains a possibility that some women may not have fully remembered all the specific procedures, examinations, and laboratory tests conducted during their visits, which could lead to underreporting or misreporting of services received. Furthermore, although data collectors received training to effectively communicate the purpose of the study and encourage honest responses, the results may still be influenced by social desirability bias, where participants respond in ways they believe are expected or favorable rather than providing entirely candid answers.
Conclusion and recommendation
The study found that only a very small proportion of women received the full range of ANC services. While some services like weight and blood pressure measurement were commonly provided, important components such as height measurement and counseling on pregnancy-related complications were much less utilized. Factors influencing the use of ANC services included husband’s support, women’s perception of how close health facilities were, early start of ANC visits, the quality of interaction between providers and patients, and household wealth. To improve maternal health outcomes, interventions should focus on encouraging husband involvement, empowering women through community efforts, improving the quality of ANC services, and increasing access by decentralizing health facilities, particularly in rural areas.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251375220 – Supplemental material for Factors associated with antenatal care service content utilization in selected rural areas of Southern Ethiopia: Assessing the extent of compliance with World Health Organization recommendations—A mixed-methods study
Supplemental material, sj-docx-1-whe-10.1177_17455057251375220 for Factors associated with antenatal care service content utilization in selected rural areas of Southern Ethiopia: Assessing the extent of compliance with World Health Organization recommendations—A mixed-methods study by Lielt Gebreselassie Gebrekirstos, Meron Hadis Gebremedhin, Hayelom Berhe and Tsiyon Birhanu Wube in Women's Health
Footnotes
Acknowledgements
Not applicable.
Ethical considerations
Ethical clearance was obtained from the IRB of Wolaita Sodo University, College of Health Science (CHSM/ERC/06/15). Official permission letters were issued to each selected kebele within both zones.
Consent to participate
Written informed consent was obtained from all study participants and from the parents or guardians of participants under the age of 16 prior to interviewing. For participants who were illiterate, the consent statement was read aloud, and consent was provided by signing from their parents, guardians, or a person of their choice who was independent of the research team. No personal identifying details were recorded or included in any documentation related to the study, and participant privacy was strictly maintained. Participation was entirely voluntary, and no one was compelled to take part unless they agreed.
Consent for publication
Not applicable.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.