
Abstract
Background:
Women experiencing substance use disorders face barriers to treatment, including childcare, stigma and lack of gender/trauma-informed programming. Several non-government organizations in New South Wales run women-only treatment services to address these needs.
Objectives:
We aim to assess characteristics of women entering treatment in these services.
Design:
Data on client characteristics from six women-only non-government organization substance use disorder treatment services in New South Wales between 2014 and 2018 were extracted from a database containing demographics, drug use and treatment characteristics and psychological distress (Kessler-10 scale) of women entering the services. Logistic regression models were used to estimate unadjusted odds ratio and adjusted odds ratio for treatment completion and different drugs on entry.
Results:
Data were available for 1357 women. Most (91%) episodes were for residential treatment. Women’s mean age was 35.4 years (standard deviation = 9.8; range = 17–67). Residential clients tended to be younger than non-residential clients (35.1 vs 38.5 years, p < 0.001). Methamphetamine (43%) and alcohol (32%) were the most reported principal drug of concern. Women (89%) reported high levels of psychological distress (median Kessler-10 scale score = 27.5, range = 10–50), highest for women reporting alcohol as their principal drug. Overall, 43% of episodes resulted in treatment completion, most commonly for women entering residential treatment (45% vs 22%, p < 0.001) and for alcohol treatment (adjusted odds ratio = 1.42; confidence interval = 1.07–1.90; p < 0.001). Women with Kessler-10 scale scores indicating anxiety or depression at treatment entry were less likely to complete treatment than those with lower scores (adjusted odds ratio = 0.56; confidence interval = 0.38–0.80; p < 0.001).
Conclusion:
Women entering women-only residential treatment tend to be younger and report methamphetamine as principal drug of concern. Women enter treatment with high degrees of psychological distress. Women’s services need to ensure their programmes can respond to diverse needs of younger women presenting with methamphetamine use disorder and older women with alcohol use disorder experiencing high levels of psychological distress.
Introduction
Women experience significant harms due to substance use disorders (SUDs). In Australia, more men experience SUDs, 1 but recent research suggests that prevalence of substance use in men and women is converging, especially in younger age groups. 2 Furthermore, alcohol-related harms increase as women age, with alcohol-related deaths in people aged 50 years and older, higher in women. 3
Women experiencing SUDs have gender-specific presentations and treatment needs. These include differences from men in aetiology of substance use, disease progression, comorbidities and treatment access. Women are more likely to experience mental health comorbidities and significant psychological distress, and more commonly report experiencing abuse and/or trauma, all of which impact treatment and recovery.2,4,5
Women may also experience additional barriers to SUD treatment. 6 For example, as women are much more likely to be a sole or primary caregiver with childcare a significant barrier, women may also experience stigma 7 as women who use alcohol attract greater scrutiny of their parenting than male parents.4,8 Likewise, while concern for their children’s welfare can be a key motivator for SUD treatment entry, 9 fear of losing custody if their SUD is identified, can present a substantial barrier to treatment for many women.7,10–12 Other institutional-level barriers include lack of gender- and trauma-informed programming, and geographical and transportation barriers that make visitation difficult and programmes without child-minding services which limits women’s access to and ability to continue in treatment. 12
Gender-specific treatment services have been established to address the treatment needs specific to women. Women-only services may address barriers for those who are primary carers of children, or women with a history of abuse or trauma. In New South Wales (NSW) Australia, non-governmental organizations (NGOs) run several women-only services. These organizations utilize different treatment models and philosophies and offer a range of diverse services. 13
The current evidence for women-only services is generally favourable; 14 however, the strength of evidence is variable, with some studies unable to show greater efficacy for women’s only services. 15 Most literature suggests that some women may attain better treatment outcomes in women-only compared to mixed-gender services.16–19 This could be due to such services’ ability to better meet some women’s distinct psychosocial needs.6,12,18,20,21 They may, for example, provide a safe environment and facilitate gender-relevant topics of discussion. 14 Some research suggests that group gender composition can affect members’ self-perception, communication and overall group atmosphere. 15 Importantly, women-only services may be the option for a woman to remain with her children while receiving residential treatment. 22 Not all women will want or benefit from women-only services, as highlighted in a 2018 UK study of 19 women, 23 and conceptualizing women as one homogeneous group should be avoided. 2
There is currently little known about the characteristics of women entering women-only SUD services in Australia, the last research was conducted more than two decades ago. 24 However, understanding these characteristics is important as it will assist identification of women’s treatment needs and improve service targeting. Therefore, we aimed to describe the characteristics of women who entered women-only SUD treatment services in NSW between 2014 and 2018. Specifically, we examine clients’ demographic and treatment characteristics, including principal substance of concern, referral source, their level of psychological distress and treatment type, length and completion at treatment entry.
Methods
Measures and participants
Data from six women-only NGO drug and alcohol treatment services in NSW, Australia, was extracted from the Network of Alcohol and other Drugs Agencies 25 for 2014–2018, which contains routinely collected data including the National and NSW Minimum Data Sets (NMDS). The NMDS is collected upon treatment commencement and includes information on client characteristics. Women who completed assessment measures upon treatment entry between April 2014 and December 2018 were included.
All residential treatment services provided care for 6 weeks to 6 months. Some services provided withdrawal management and residential rehabilitation; others only provided rehabilitation (i.e. they completed withdrawal management elsewhere). None of the services provided only withdrawal management, with all providing some counselling, group sessions and living support.
Variables
Age in years at treatment entry and length of treatment were analysed as continuous variables. Treatment services were categorized as either residential (withdrawal management and rehabilitation) or non-residential (counselling, assessment only and other). Other baseline characteristics were categorical variables: country of birth (Australia vs other), income (temporary benefit or pension, student allowance or no income, full- or part-time employment, not stated), usual accommodation (privately owned or rented house, other, not stated) living arrangement (alone, spouse/partner/child, alone with children, other, not stated), self-referral, method of use (injects vs other) and principal drug of concern. Principal drug of concern (herein principal drug) was grouped into five categories: amphetamine/methamphetamine (herein methamphetamine), alcohol, heroin/opioids, cannabinoids and all others (‘other’). ‘Other’ drug category will not be interpreted as it involves diverse drugs. 25
The Kessler-10 scale (K10) was used to measure psychological distress 26 at treatment entry. The K10 comprises 10 items, each rated on a 5-point scale, assessing symptoms associated with anxiety and depression over the past 4 weeks. Higher scores indicate higher psychological distress. 24 We used the Australian Bureau of Statistics’ ‘Plain English’ classification of K10 scores to categorize K10 scores into three categories for analysis: may not be experiencing psychological distress (10–15), may be experiencing moderate symptoms of depression and/or anxiety (16–30) and may be experiencing some form of depression and/or anxiety (31–50). 27
Statistical analysis
Following transfer of the data for cleaning and storage, R statistical software (version 4.1.3) and Stata (version17.0) were used for analysis of clients’ characteristics. Categorical data were described using frequencies with percentages and mean values with standard deviations (SDs) for continuous data. Medians and corresponding ranges were used where data were not normally distributed. Independent t-tests were performed to compare mean values for normally distributed data. The chi-square (χ2) statistic was used to analyse categorical variables and corresponding confidence intervals (CIs). Stepwise ordinal logistic regression 28 was used to analyse K10 scores and baseline characteristics. The Brant test was performed to test the proportional odds/parallel lines assumption of the ordered logit model, which held. Generalized linear model (GLM) logistic regression was used to model treatment completion as expected. We used backward stepwise regression to select the best performing model that predicted treatment completion as expected using baseline characteristics. Statistical significance was set at p < 0.05.
Results
Treatment entry records containing national minimum data were available for 1500 clinical episodes (1357 women) between April 2014 and December 2018. Most women (n = 1229) had one episode (mean episodes per woman was 1.1). Twelve women had three episodes (mean age = 35.0, all for residential treatment) and 119 women had two episodes (mean age = 35.9, 116 residential treatment and 3 non-residential treatment). Where there were multiple treatment entries, only the first episode of treatment was analysed (second and third episodes were deleted). The final study sample consisted of 1357 women. Most (n = 1235) episodes were for residential services, and 122 episodes were for non-residential services (Table 1).
Characteristics of participants entering treatment.

Includes boarding house, hostel, supported accommodation services, homeless, prison, detention centre and other.
Includes parent(s), friend(s), other relative(s) and other.
Demographics and sample characteristics
Of total, 90% of clients reported being born in Australia, and 95% reported English as their preferred language. All clients identified as female (n = 1356), except one for whom data were missing. Data on clients’ sexuality were largely incomplete. Of 292 episodes recorded, most identified as ‘straight’ or ‘heterosexual’ (n = 255).
The most reported source of income was temporary government benefit/pension (89%). Two-thirds of the clients (68%) lived in privately owned/rented accommodations at time of treatment entry. Of the 994 women who reported living without children, 38% lived with others (parents, partners, friends or relatives) and 25% lived alone. Of the 363 women who reported living with children, 44% lived alone with their children, while 56% lived with a spouse/partner and child (Table 1).
Age
Median reported age at treatment entry was 33.9 years (range = 17–67). Residential clients tended to be significantly younger (median = 33.6, range = 17–67) than non-residential clients (median = 37.0, range = 20–66; p < 0.001). Linear regression showed that as age increased women were less likely to enter residential treatment compared to non-residential treatment. For every year increase in age, the odds of entering residential treatment decreased by 3% (odds ratio (OR) = 0.97; 95% CI = 0.95–0.98; p < 0.001). Of the 18 women aged older than 61.5 years, most (94%) were in residential treatment (Figure 1) and their principal drug was methamphetamine (n = 10), heroin/opioids (n = 5) and cannabis (n = 3; Figure 2).

Distribution plot of age by treatment type.

Distribution plot of age by principal drug of concern.
The median age of clients was 31 years for those who reported methamphetamine as their principal drug and 41 years for those who reported alcohol (Table 2). There was no significant difference in age for women who self-referred (35 years) compared to those referred by another source (33 years). Similarly, there was no significant difference in mean age between those who reported injecting drug use (33 years, interquartile range = 29–30) and those who did not (34 years, interquartile range = 28–43).
Characteristics of clients by principal drug of concern.

Substance use and injection
The most common principal drug was methamphetamine (43%) and then alcohol (32%; Figure 3). Most clients (71%) did not have data on whether they injected drugs, of those who did one-third reported injection in the past 12 months and 43% reported no injecting (Table 1). Over the 5-year period, methamphetamine remained the most reported principal drug, followed by alcohol (Figure 3).

Principal drug of concern by year.
Treatment
There was a significant difference between principal drug of concern reported and treatment type received (χ2 = 19.099; p < 0.001). Methamphetamine was more commonly reported as principal drug in residential settings (44%); alcohol was the most reported principal drug for non-residential treatment (38%; Table 3). Women with methamphetamine as their principal drug were 1.92 times more likely to enter residential treatment than non-residential, compared to alcohol (95% CI = 1.21–3.02; p = 0.01); but after controlling for demographics (age, country of birth, usual accommodation, income and living conditions), there was no difference (adjusted odds ratio (AOR) = 1.35; 95% CI = 0.78–2.31; p = 0.28).
Characteristics of clients by treatment type.

The main treatments sought were rehabilitation 67% (n = 936), withdrawal management 21% (n = 291) and counselling 9% (n = 119). Approximately half the episodes arose from self-referral (45%), which was the highest for those seeking alcohol treatment (55%) and the lowest for methamphetamine treatment (38%; Table 2).
Psychological distress
K10 data were available for 1357 women at intake. The median K10 score was 27.5 (range = 10–50), indicating high levels of psychological distress. Of total, 11% of women presenting for treatment had a K10 score below 15 indicating that they may not be experiencing psychological distress, almost 50% had K10 scores indicative of moderate psychological distress and 40% had a score above 31 indicating depression and/or anxiety (Table 4). Women entering residential services (n = 1235) had a higher median K10 score (28) than those entering non-residential services (26.5). K10 scores were the highest for women presenting with alcohol as their principal drug (median = 29, range = 10–50), with the lowest K10 scores for women where methamphetamine was the principal drug (median = 26, range = 10–50; Table 2).
Baseline characteristics associated with levels of psychological distress.
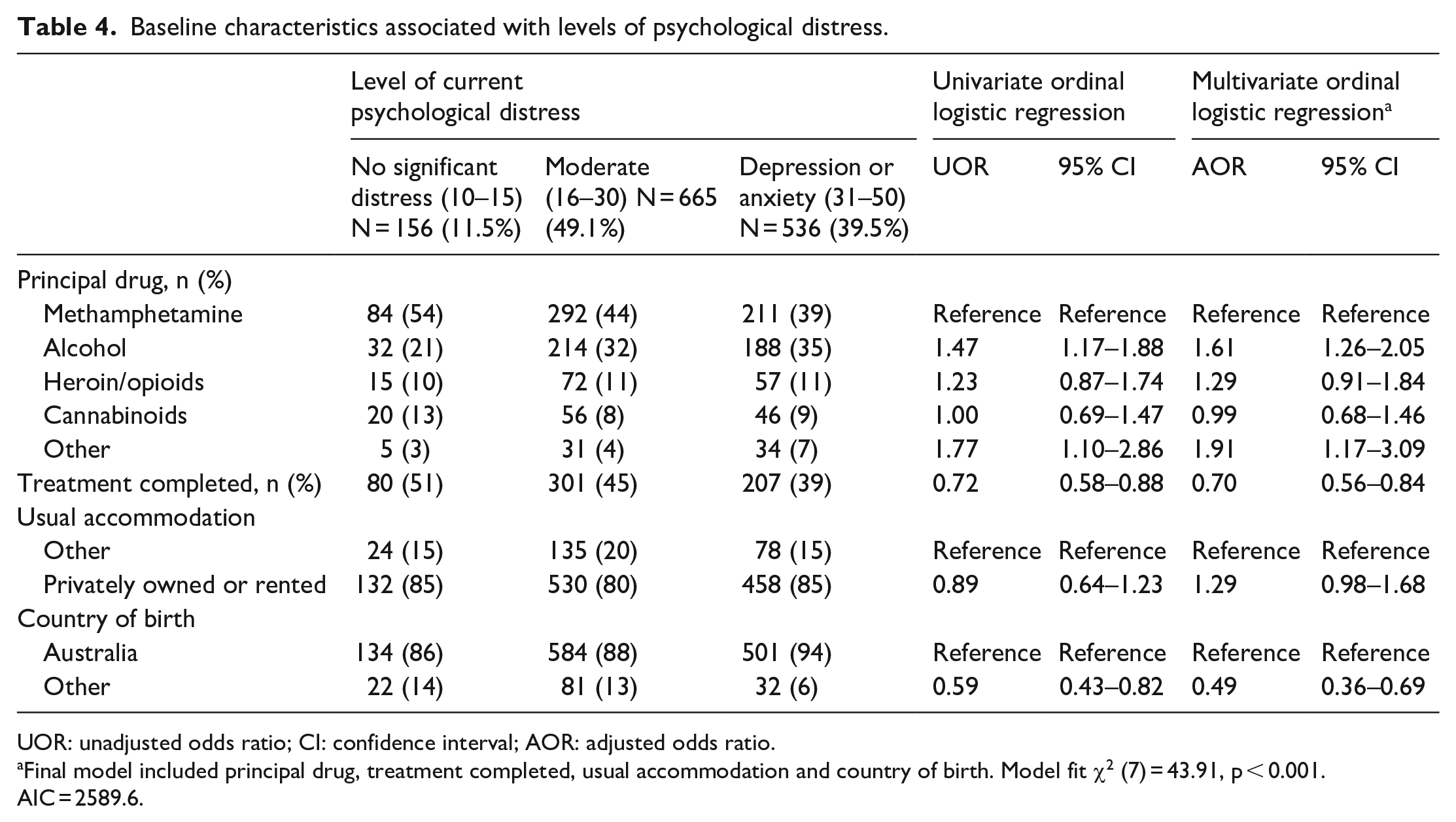
UOR: unadjusted odds ratio; CI: confidence interval; AOR: adjusted odds ratio.
Final model included principal drug, treatment completed, usual accommodation and country of birth. Model fit χ2 (7) = 43.91, p < 0.001. AIC = 2589.6.
To determine factors associated with high levels of psychological distress, baseline characteristics (age, principal drug, living arrangement, usual accommodation, income, country of birth and treatment completed) were entered into an ordinal regression model. Ordinal multiple logistic regression showed that, women presenting for alcohol treatment were associated with higher level of distress (AOR = 1.61; 95% CI = 1.26–2.05; p < 0.001), while women who were born outside Australia were 49% less likely to experience higher levels of distress (AOR = 0.49; 95% CI = 0.36–0.96; p < 0.001). For women who completed treatment, the likelihood of having moderate-to-severe distress was 30% lower than for those who did not (AOR = 0.70; 95% CI = 0.56–0.84; p < 0.001; Table 4).
Treatment length and completion
Mean treatment length was longer for non-residential clients (94.2 days) by 34.5 days compared to residential clients (59.7 days; 95% CI = 18.9–50.1; p < 0.0001). Of total, 44% of episodes resulted in treatment cessation against advice, while 43% completed treatment. Of total, 45% of residential clients and 22% of non-residential clients completed treatment as expected. However, a similar proportion of both residential and non-residential clients left treatment against advice (44% and 40%, respectively; Table 3).
The relationship between baseline characteristics and treatment completion revealed that age, usual accommodation, country of birth, living arrangement, self-referral, treatment type, K10 categories and principal drug were associated with treatment completion. Multivariate logistic regression showed that women presenting for alcohol treatment, compared to methamphetamine treatment, were significantly more likely to complete treatment as expected (AOR = 1.42; 95% CI = 1.07–1.90; p = 0.02). Women in residential treatment were 3.41 times more likely to complete treatment as expected (AOR = 3.41; 95% CI = 2.14–5.44; p < 0.001) compared to women in non-residential treatment. And women presenting with depression or anxiety were 56% less likely to complete treatment (AOR = 0.56; 95% CI = 0.38–0.80; p < 0.001; Table 5).
Unadjusted and adjusted analysis of factors associated with treatment completed as expected.

Includes boarding house, hostel, supported accommodation services, homeless, prison and detention centre.
Includes parent(s), friend(s), other relative(s) and other.
Reference group as those presenting for methamphetamine treatment were the least likely to complete treatment as expected (UOR = 0.71; 95% CI = 0.57–0.88; p < 0.001).
Final model included age, treatment type, self-referral, usual accommodation, K10 categories and principal drug. Model Fit χ2 (10) = 65.76, p = 0.00. AIC = 1813.23 and BIC = 1870.57.
Discussion
To our knowledge, this is one of the few recent studies to examine characteristics of women entering women-only SUD treatment services in Australia. We found that women entering women-only NGO treatment services in NSW, Australia, between 2014 and 2018 were most commonly presenting for methamphetamine use and alcohol. Women in the methamphetamine group were younger and less likely to complete treatment. Women presenting for alcohol treatment were older, more likely to self-refer, enter non-residential treatment and have the highest level of psychological distress. Women in residential treatment and accessing alcohol treatment were more likely to complete treatment as expected.
Methamphetamine was the most reported substance of concern, followed by alcohol. This is distinct from similar work conducted in the 1990s when, to the best of our knowledge, was the last time similar work was last conducted in Australia. The research, by Swift and colleagues published in 1996 found heroin, followed by alcohol to be the primary drugs of concern for women entering women-only substance use treatment. 24 While the prevalence of methamphetamine in our findings is consistent with a well-documented overall increase in methamphetamine use in Australia in recent years,2,29,30 it is notable that alcohol remains a significant problem for women seeking this type of treatment more than a quarter of a century since the last investigation. Nationally, in mix gender treatment services, alcohol was the most reported principal drug of concern in 2015–2016 31 and 2017–2018. 32 Between 2011–2012 and 2015–2016, the number of treatment episodes with amphetamines as the principal drug of concern increased by 175%, and cannabis treatment episodes increased by 40%, heroin and alcohol treatment episodes fell by 15% and 6%, respectively. 31
Clients reporting methamphetamine as their primary substance were also younger (median 31 years) compared to those who reported alcohol (median age 41 years). These results are in line with data from a recent study 2 of women attending specialist non-government substance use treatment services in NSW (mean age = 31 and 39 years, respectively). One potential explanation is an increase in younger people seeking methamphetamine treatment due to recent increased use of imported smokable crystalline methamphetamine.2,30,31,33 International studies34,35 suggest that methamphetamine users are likely to have experienced child or adolescence negative life events, homelessness, unstable housing or foster care increasing the risk of substances use disorders. Early initiation of amphetamine is associated with higher dependence and increased risk of mental health and psychosocial problems. 35 Therefore, our findings emphasize the need for targeted interventions at younger women. More analysis is necessary to understand the factors that may account for this age difference, but the legal status may be a contributing factor. Methamphetamine was also the most reported principal drug in the residential setting, and women who reported methamphetamine as their principal drug were approximately twice as likely to enter residential treatment than non-residential. Furthermore, methamphetamine use is associated with poor health and socioeconomic outcomes, 36 and its treatment is often associated with distinct barriers. These include clients’ lack of confidence in existing treatment options and the absence of pharmacotherapy compared to those available for other substances, as well as service providers’ lack of understanding of effective treatments.36–38 Given increased methamphetamine use across Australia, future research should examine the effectiveness of residential women-only services for such clients.
Since Swift et al. 24 last reported in 1996, the median age of women attending SUD services has increased (33.9 years cf 31 years). However, our finding (mean age = 35.4 years) is consistent with Rodriguez et al.’s 2 more recent study (mean = 35.24 years). Our data are unable to examine prior treatment engagement, but the women in the study are likely to have had multiple prior treatment episodes, as the mean age of initiation to illicit drug use in Australia is approximately 19.9 years, 33 indicating significant lag between first use and first treatment.29,39 Swift et al. 24 found, in 1996, that the ‘time-lag’ from women first becoming aware of their SUD to first seeking treatment was a median of 24 months. While we are unable examine a change in this trajectory, it is possible that women tend to seek women’s specific services after having attempted other treatment episodes.
The psychological health of women presenting for treatment has implications for the type of treatment provided, treatment retention and relapse. 12 This study found a median K10 score of 27 overall compared to a median K10 score of 12 for the general Australian population, 26 indicating high levels of psychological distress. Of total, 90% of women in the study had moderate (50%) to severe distress (40%). This is unsurprising as women with SUDs have been found to be significantly more likely to experience high levels of psychological distress and chronic alcohol or drug use may enhance vulnerability to depression or anxiety disorder.21,40 It is therefore important that these services are equipped and resourced to manage these complex conditions. This challenge is compounded when the disparate needs of older women with alcohol use disorder are also considered. The women’s-only services in NSW are almost exclusively small NGO ‘boutique’ services and must be agile in their response to both individual needs and changing population trends.
Clients were predominantly of English-speaking background. Moreover, women seeking treatment, born outside Australia, were less likely to present with higher levels of psychological distress. This raises important questions as to whether women from non-English-speaking backgrounds less frequently developed SUDs requiring treatment or whether they were less likely to seek treatment. This is important to ascertain in future research, as gender-specific services may be preferable for some members of culturally and linguistically diverse groups. The national alcohol treatment guidelines 41 recommend that alcohol treatment services take language and cultural considerations into account, recognizing that clients may sometimes prefer to see a male or female worker. 42 Women-only services are often the only providers that enable women to remain with their young children during treatment, 22 and recent clinical guidelines for management of alcohol use disorders recommend that clinicians consider childcare responsibilities when planning treatment. 42 Although some of these services provide options for children to remain onsite, there are limited data on the outcomes for the children or the type of care, including clinical care, provided. Further research is warranted to assess the importance of women-only residential services in addressing childcare needs of women seeking SUD treatment in NSW.
Limitations
Data were limited to the geographic specificity of the sample, which may limit the external validity of our findings. Data were available from April 2014 to December 2018 and incorporate the period where methamphetamine use increased; 43 however, it does not include data from the COVID-19 periods where changes to drugs markets are still being discerned. The treatment models included across the six sites are diverse and were not adjusted for. In NSW, opioid agonist treatment (OAT) is the main treatment for opioid disorders and this treatment is delivered via primary health care service and outpatient tertiary care clinics. 10 Some NGO services provide ancillary support (e.g. counselling) for these women, but do not provide the OAT, and therefore, these services may be used less frequently by women with opioid use disorder. We were interested in the characteristics of women entering treatment and treatment outcomes were beyond the scope of the data.
All data were drawn from routine collection, and therefore, some variables were blunt, including those around referral, with limited information on whether the women were referred from services such as the criminal-legal system or children protection services. We were unable to examine variables such as primary carer status and history of physical or sexual abuse, including domestic abuse as our data were derived from standardized record collection. Despite being a routinely collected data item, data on sexuality were largely missing. Sexuality diverse populations are known to experience higher rates of SUDs compared to the general population. 31 Methamphetamine use among people who identified as being homosexual or bisexual was 5.8 times as high as heterosexual people. 1 It is therefore important to obtain more data about service delivery for this community, including their preference for gender-specific services. As such, understanding the barriers to collecting this information warrants attention.
Conclusion
While limited by the above, this is one of the few recent Australian studies to examine characteristics of women entering women-only SUD treatment services. We have identified that methamphetamine is the principal drug of concern most commonly seen by these services, followed by alcohol, but importantly, these two groups have disparate presentations, highlighting the challenges women’s services face in when developing and delivering programmes to women with diverse and distinct needs. These results can guide future studies in this area, which together may assist the assessment of whether women-only services are adequately fulfilling the needs of women seeking SUD treatment in NSW, Australia, and that they are supported to do so.