
Abstract
Background:
Adverse childhood experiences (ACEs) are traumatic events that occur during childhood. Previous evidence suggests that pregnancy loss may be associated with ACEs and mental health disorders; however, to our knowledge, no studies have considered these associations in women with concurrent reproductive trauma (CRT), defined as pregnancy loss during infertility.
Purpose:
To compare ACEs, stress, anxiety, depression, and post-traumatic stress disorder (PTSD) symptoms among women with CRT and women with infertility only.
Methods:
A descriptive cross-sectional study design was used to recruit 99 U.S. women with infertility through convenience and snowball sampling on Facebook, Instagram, and at fertility clinics. A REDCap survey included demographics, ACEs questionnaire, infertility-related stress (COMPI-FPSS), perceived stress (PSS-4), anxiety (GAD-7), depression (PHQ-8), and PTSD (PC-PTSD-5). Statistical analysis using SPSS 28 included descriptive statistics, independent t-tests, and chi-square test for independence.
Results:
Women with CRT were more likely to experience 2+ ACEs than women with infertility-only (p = 0.001), with four ACEs occurring more often. Infertility-only group with 2+ ACEs had significantly higher levels of stress, PTSD, anxiety, and depression, with clinically significant higher depression and PTSD symptoms. CRT group with 2+ ACEs had significantly higher anxiety and depression, with clinically significant higher moderate or severe depression.
Discussion:
Although women with CRT and infertility experienced similar levels of psychological distress, having an ACE history worsened their mental health symptoms. ACE history may be associated with reproductive traumas, though further studies are needed. Trauma-informed care should be implemented for women with ACEs, infertility, and CRT.
Keywords
Introduction
Reproductive traumas, such as infertility and pregnancy loss, are traumatic reproductive events that cause significant psychological distress. 1 In the United States, one in five women, or individuals assigned female sex at birth, experience infertility, characterized by the inability to conceive or sustain a pregnancy after 12 months of unprotected sexual intercourse. 2 The experience of infertility is coupled with infertility-related stress, 3 depression, post-traumatic stress disorder (PTSD) symptoms, 4 and lower quality of life. 5 Fertility treatments, such as medications to induce ovulation or more advanced treatments like in vitro fertilization, are used to help women achieve pregnancy but can be an additional source of stress for women. 6 Women who undergo treatment in the United States often express concerns related to financial and occupational-related stress, which may be due to the out-of-pocket expenses to pay for fertility treatments and missed work time due to treatments that require specific interventions during the menstrual cycle. 3
In addition, pregnancy loss during fertility treatments, also called concurrent reproductive trauma (CRT), can increase infertility-related stress, decrease quality of life, 7 and cause significant anxiety and depression in women with infertility who later become pregnant after fertility treatments. 8 Pregnancy loss most often occurs prior to 13 weeks of gestation, with estimates around 13.5% of all clinically recognized pregnancies; 9 however, the incidence of pregnancy loss during fertility treatments is unknown. Pregnancy loss is associated with psychological distress, including anxiety, stress, and depressive symptoms, 10 and an increased risk of suicide in women. 11 Brigance et al. 12 reported that women who experienced infertility or pregnancy loss had significantly more trauma symptoms than those who did not experience reproductive traumas. Thus, the concurrent experience of pregnancy loss during infertility may exacerbate the psychological distress and trauma symptoms of women who are already experiencing significant stress from being unable to conceive.
Furthermore, previous traumatic experiences, whether actual or threatened, are associated with mental health disorders.13,14 In particular, childhood traumatic experiences are associated with later adult mental health disorders, 15 including psychiatric disorders and depressive symptoms. 16 Adverse childhood experiences (ACEs) are traumatic events that occur during childhood, including forms of physical, emotional, or sexual abuse; physical or emotional neglect; divorce; parental death; parental incarceration; witnessing violence or death; and experiences with substance use or mental illness in the home. 17 ACEs have also been found to have a dose-response effect, where each additional ACE worsens mental health outcomes. Daníelsdóttir et al. 16 conducted a cohort study of over 25,000 individuals and found that each additional ACE experienced was associated with 52% greater odds of a psychiatric disorder diagnosis.
Not only do ACEs affect later adult mental health, but ACEs are also associated with adult chronic diseases, including coronary artery disease, heart attack, stroke, diabetes, cancer, chronic bronchitis, emphysema, substance use, and depression.18,19 However, there is limited evidence of associations between ACEs and later adult reproductive diseases and reproductive traumas. Previous evidence suggests that pregnancy loss may be associated with ACEs, 20 and each additional ACE experienced increased the risk of pregnancy loss by 12%. 21 Kerkar et al. 22 found that women had between 1.7- and 1.9-fold higher odds of pregnancy loss if they had experienced at least four ACEs compared with women with no ACEs. To our knowledge, no studies have considered associations between ACEs and pregnancy loss in the context of women with infertility or have considered relationships between ACEs and mental health disorders in women with reproductive traumas. Therefore, the purpose of this study was to compare ACEs and psychological distress (infertility-related stress, perceived stress, anxiety, depression, and PTSD scores) among women with CRT and women with infertility alone.
Materials and Methods
Study design
This study is a secondary analysis of a parent study using a descriptive cross-sectional study design to explore ACEs, chronic stress biomarkers, and psychological distress among United States (U.S.) women with infertility and U.S. mothers. This study was approved by the University Medical Institutional Review Board at East Carolina University. Informed consent was obtained from participants prior to the start of the online survey by participants selecting “agree” to participate in the study.
Participant sample/setting
Participants were recruited between November 2023 and May 2024 through convenience sampling. Administrators from infertility-related support groups on Facebook and Instagram influencers were asked to share the study information and a survey link with their followers. Participants were also recruited through snowball sampling when Facebook users or Instagram users shared the study information or survey link with other social media users. In addition, participants were also recruited through a posted flyer at three health care and fertility clinics in Florida and North Carolina. Inclusion criteria for participants included those who were biologically female sex, had an infertility diagnosis and were undergoing fertility treatments at the time of the study, resided in the U.S., were between the ages of 18 and 49, and were able to read English or Spanish. Exclusion criteria included biologically male sex, living outside of the U.S., being younger than 18 years or older than 49 years, and being unable to read English or Spanish. A power analysis was conducted to determine the sample size. Using a power of 0.80, α = 0.05, and a moderate effect size, the estimated sample size is n = 40 for each group.
Data collection
Survey data were collected on REDCap, a Health Insurance Portability and Accountability Act (HIPAA) approved software application to develop and store online survey data. 23 Administrators from infertility-related Facebook groups and Instagram influencers/pages were contacted through the direct message on each of the social media platforms and were asked to share the survey link and study information or permission for a research team member to post the link and information in the group. Facebook and Instagram users could also share the study link and information with other social media users. Administrators from health care and fertility clinics in Florida and North Carolina were also contacted and asked to post a study flyer that contained study information and a Quick-Response (QR) code that would link to the survey. The survey was available in both English and Spanish and included an electronic consent, screening questions, infertility-related stress, perceived stress scale, anxiety, depression, PTSD, quality of life, ACE scores, reproductive history, and demographic information.
Measures
Copenhagen Multi-Center Psychosocial Infertility Fertility Problem Scale Score
The Copenhagen Multi-Center Psychosocial Infertility Fertility Problem Scale Score (COMPI-FPSS) is a nine-item scale to measure personal (three items), social (three items), and marital (three items) infertility-related stress. The scale includes two items on a five-point Likert scale ranging from strongly disagree (1) to strongly agree (5), and seven items on a four-point Likert scale ranging from not at all (1) to a great deal (4). Higher scores indicate higher infertility-related stress in each of the subscales.24,25 Internal consistency for coefficient alphas for the subscales in this study was 0.49 for personal stress, 0.64 for marital stress, and 0.76 for social stress.
Perceived Stress Scale
The Perceived Stress Scale (PSS-4) is a four-item, five-point Likert scale measuring stress within the past 2 weeks. The scale ranges from never (0) to very often (4). Higher scores indicate higher stress. 26 The coefficient alpha for this study was 0.73.
Generalized Anxiety Disorder Scale
The Generalized Anxiety Disorder Scale (GAD-7) is a seven-item, four-point Likert scale, ranging from not at all (0) to nearly every day (3). The scale measures anxiety symptoms over the past 2 weeks. Higher scores indicate more anxiety-related symptoms 27 with scores higher than 10 indicating clinical anxiety. Cronbach’s alpha for internal consistency was 0.88 in our study.
Patient Health Questionnaire
The Patient Health Questionnaire (PHQ-8) is an eight-item, four-point Likert scale questionnaire measuring depression symptoms over the past two weeks. The questionnaire ranges from not at all (0) to nearly every day (3). Higher scores indicate more depression-related symptoms, 28 with scores higher than 10 indicating clinical depression. In our study, the coefficient alpha was 0.88.
Primary Care PTSD Screen for DSM-5
The Primary Care PTSD Screen for DSM-5 (PC-PTSD-5) is a five-item screening tool measuring PTSD symptoms over the past 2 weeks. The screening includes a yes or no answer choice for all five questions. A higher number of yes responses indicates more PTSD-related symptoms, 29 with a score of 3 or more indicating probable PTSD symptoms. The coefficient alpha was 0.73 in our study.
Adverse childhood experience
The ACEs Questionnaire is a 10-item questionnaire of ACEs experienced prior to one’s 18th birthday. The questionnaire includes a yes or no response choice for all 10 ACE items, with a yes response indicating the participant experienced that ACE prior to their 18th birthday, and a no response indicating the participant did not experience that ACE item. A higher number of yes responses indicates more ACEs experienced during childhood. 30
Data analysis
Statistical analysis was conducted using SPSS 28. Descriptive statistics were used to describe demographic and reproductive characteristics. Chi-square tests for independence and independent t-tests were used to examine differences in infertility-related stress, perceived stress, anxiety, depression, PTSD, and ACE scores among women with CRT and women with infertility alone.
Results
Of the 99 participants in this study, 59 (60%) experienced CRT, and 40 (40%) had infertility-only. Most participants in both the CRT and infertility-only groups were non-Hispanic or Latino, Caucasian/White, and had an education level equal to or above a baccalaureate degree. Most of the participants were employed full-time, and the household yearly income was about evenly distributed between $51,000–$100,00, $101,000–$150,000, and >$150,000. Participants tended to live in an urban area compared with a rural or suburban area. Most participants had primary infertility and had partial or no fertility insurance coverage (Table 1).
Demographic Characteristics of Study Participants (N = 99)
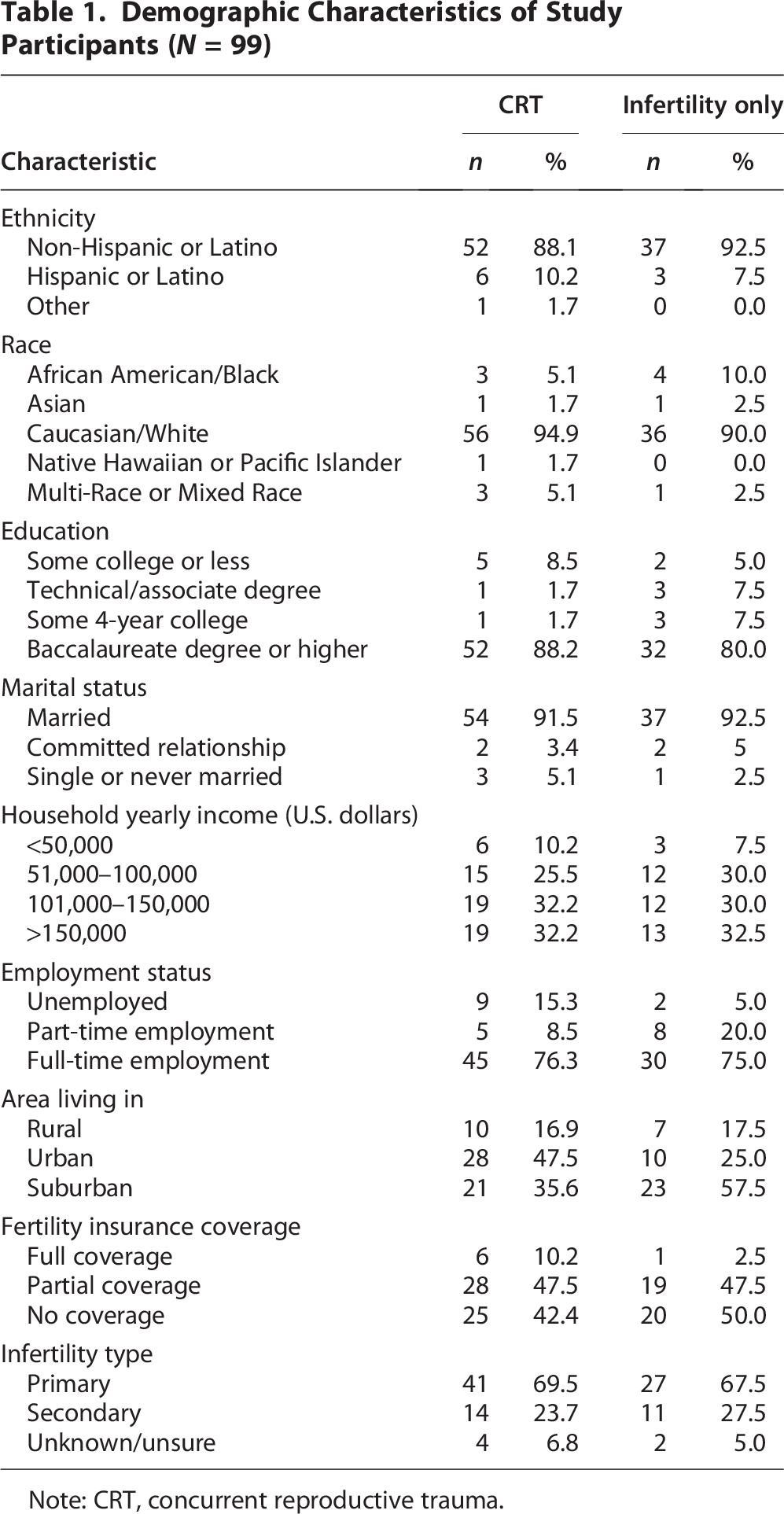
Note: CRT, concurrent reproductive trauma.
We compared the frequency of responses of each ACE item between the CRT group and infertility-only group using the Chi-square test for independence (Table 2). Compared with the infertility-only group, the CRT group reported higher ACEs on each item except ACE item 10, which asked participants if they had experienced sexual abuse as a child. Four of the 10 ACE items were selected significantly more in the CRT group, which included ACE item 1 (neglected, underfed, unprotected), ACE item 4 (substance use in the household), ACE item 6 (household member incarcerated), and ACE item 7 (verbal abuse).
Adverse Childhood Experience Scale Item Differences Between Concurrent Reproductive Trauma (n = 59) and Infertility Only (n = 40) Groups

Note: ACE, adverse childhood experience; CRT, concurrent reproductive trauma.
Table 3 presents the mean psychological distress scores between the CRT group and the infertility-only group. Mean psychological distress scores were higher in the CRT group compared with the infertility-only group, except for the PHQ8 score; however, they were not statistically significant.
Mental Health Analysis of Total Participants (n = 99), Concurrent Reproductive Trauma (n = 59), and Infertility Only (n = 40) Groups

Note: CRT, concurrent reproductive trauma; FPSS, Fertility Problem Scale Score; GAD, Generalized Anxiety Disorder Scale; PHQ8, Patient Health Questionnaire; PTSD, post-traumatic stress disorder.
We used independent t-tests to compare psychological distress scores between 0–1 ACEs and 2+ ACEs among CRT and infertility-only groups (Table 4). Of the 59 participants who experienced CRT, 40 (68%) had 2 or more ACEs, whereas 14 (35%) of the 40 participants with infertility-only had 2 or more ACEs (χ2 = 10.34, p = 0.001). The CRT group had higher means in each of the mental health scales when experiencing 2+ ACEs, compared with mental health scores among those with CRT experiencing 0–1 ACEs, with statistically significant differences between the GAD-7 and PHQ-8 mean scores. In the infertility-only group, participants who experienced 2+ ACEs had higher mental health scale means compared with 0–1 ACEs, except in the FPSS-Marital Stress subscale. Perceived Stress (PSS-4), PC-PTSD-5, GAD-7, and PHQ-8 were all significantly higher among those who experienced 2+ ACEs overall.
Mental Health Variables and Adverse Childhood Experiences with Concurrent Reproductive Trauma (n = 59) and Infertility Only (n = 40) Groups

Note: CRT, concurrent reproductive trauma; FPSS, Fertility Problem Scale Score; GAD, Generalized Anxiety Disorder Scale; PHQ8, Patient Health Questionnaire; PTSD, post-traumatic stress disorder.
In Table 5, we compared clinically significant anxiety, depression, and PTSD scores between women who had a history of 0–1 ACEs and 2+ ACEs in each group (CRT vs infertility-only). The CRT group participants who experienced 2+ ACEs had clinically significant moderate/severe depressive symptoms compared with those who experienced 0–1 ACEs. Within the infertility-only group, the participants who experienced 2+ ACEs had clinically significant moderate/severe depressive and PTSD symptoms compared with those who experienced 0–1 ACEs.
Mental Health Scale Clinical Significance Between Adverse Childhood Experiences among Concurrent Reproductive Trauma (n = 59) and Infertility Only (n = 40) Groups
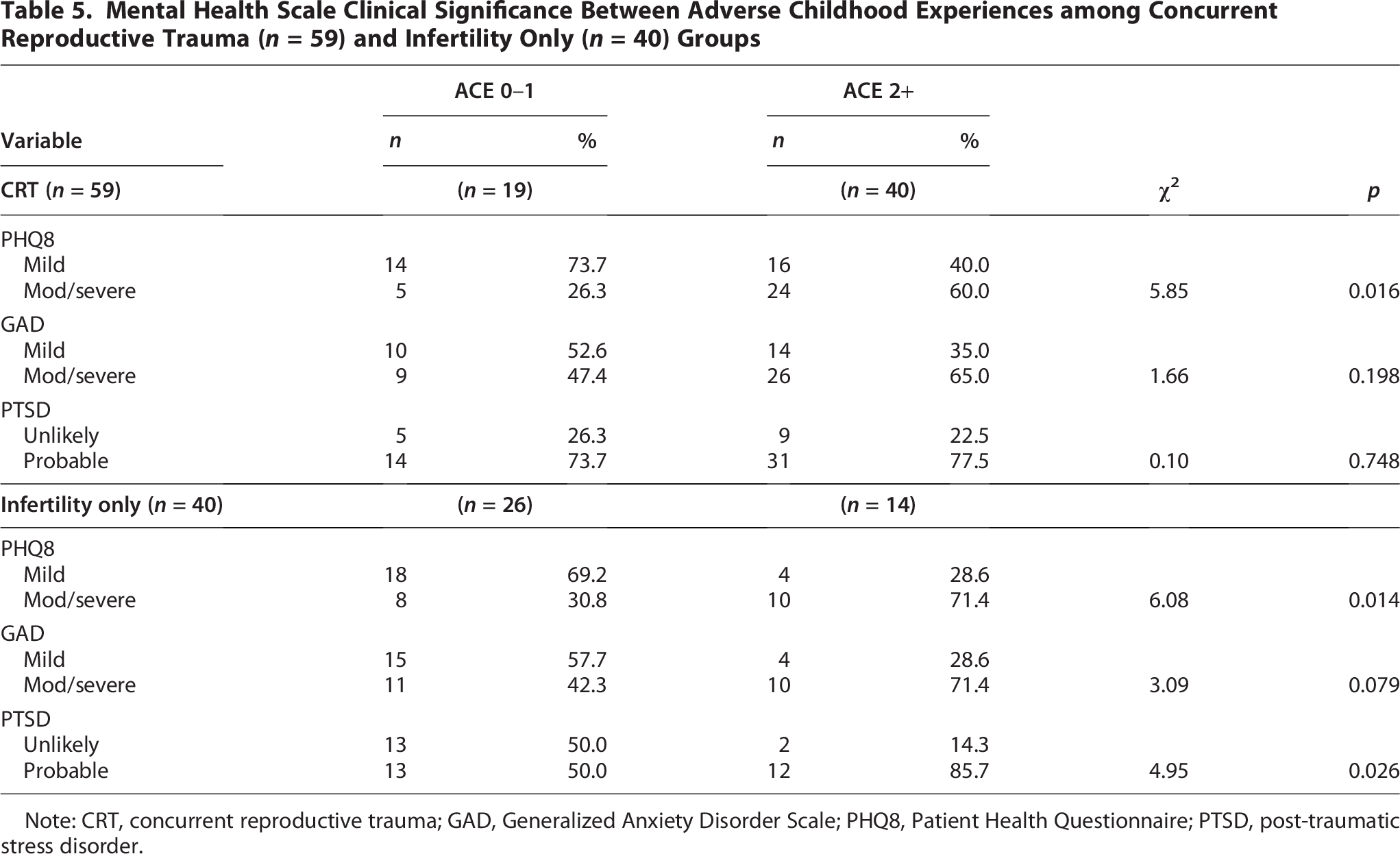
Note: CRT, concurrent reproductive trauma; GAD, Generalized Anxiety Disorder Scale; PHQ8, Patient Health Questionnaire; PTSD, post-traumatic stress disorder.
Discussion
This study aimed to explore the significance of ACEs in the context of reproductive traumas of infertility and pregnancy loss, which, to our knowledge, had not been previously studied. Our study found that women with CRT (pregnancy loss during infertility) had increased associations with having a history of experiencing specific ACEs, including neglect, substance use in the household, a household member incarcerated, and verbal abuse, when compared with women with infertility-only. We also found that while there were no significant psychological distress symptom differences between women with CRT and women with infertility-only, we found that there were differences between the two groups when we considered ACEs. Specifically, we found that women in both groups who had a history of 2+ ACEs reported worse mental health scores than women who did not experience any ACE or only 1 ACE. Our findings underscore the significant effect that ACEs have on the long-term mental health of women with infertility and how their compounding trauma experiences affect mental health outcomes.
Previous evidence suggests that women with a history of 3+ ACEs were almost two times more likely to have a miscarriage and nearly three times more likely to experience multiple miscarriages. 31 In other studies, researchers found a dose-response relationship, signifying that each additional ACE increased the association to pregnancy loss.21,22,32,33 Mersky and Lee 21 also found that 5± ACEs was associated with pregnancy loss in a study sample of 1,848 low-income mothers from Wisconsin. We found that women with infertility who had a history of 2+ ACEs were more likely to experience a miscarriage than those with 0–1 ACE. This may indicate that compounding traumas, such as childhood trauma and experiencing the trauma of infertility, could increase the risk of miscarriage. We also found that women with CRT reported a higher frequency of several ACEs compared with the infertility-only group, with significant associations involving neglect, substance use in the household, incarceration, and verbal abuse. This is consistent with other studies that found neglect and emotional abuse,34,35 substance use, and legal adversities in the household 33 were associated with pregnancy loss. Demakakos et al. 31 found an association between physical and sexual abuse and pregnancy loss; however, our study did not find that physical or sexual abuse was related to pregnancy loss among women with infertility. This could indicate that trauma experiences during childhood may affect women with infertility differently than women who do not experience reproductive diseases, although more studies are needed to investigate this further.
Although mental health scores were worse among the CRT group compared with the infertility-only group, it was not significantly different. This is a surprising finding, given that previous evidence suggested women who experience pregnancy loss also have worsening mental health symptoms such as depression, anxiety, and PTSD, 36 and that infertility-related stress is worse among women experiencing CRT. 22 The mental health outcomes of women with a history of ACEs who experience pregnancy loss are underreported in the literature. Stanhope et al. 37 found that women who experienced ACEs and pregnancy loss were less likely to report the pregnancy loss as their most stressful life event when compared with women with pregnancy loss who did not experience ACEs. Shorter et al. 38 found that ACEs were associated with depression and stress after miscarriage, but after controlling for race, the associations were not significant. These findings suggest that while women may appraise ACEs as more stressful than pregnancy loss, ACEs may not affect the development of depressive symptoms after pregnancy loss. In our study, the addition of ACEs in both groups of women with CRT and infertility-only affected the psychological distress outcomes, especially with depressive and anxiety symptoms, but they were worse among women with infertility-only. This suggests that the experience of ACEs may have a larger negative consequence on the psychological health of women with infertility and that women with CRT may have found additional support systems, such as social support, or other coping strategies that may have helped mitigate moderate to severe mental health disorders.
It is well known that mental health disorders increase in those who have a history of ACEs, 39 and cumulative trauma exposure substantially increases the risk of poor mental health and physical health outcomes. 40 Whitaker et al. 41 reported that women were more likely to experience anxiety and depressive disorders with each ACE exposure, and a meta-analysis of 15 studies that included 7,788 women also found that women with a history of ACEs were more likely to experience depressive and anxiety symptoms during pregnancy and the postpartum period. 39 Strathearn et al. 42 found that women who experienced emotional abuse and neglect as children were more likely to have anxiety, depression, and PTSD at 21 years of age. These previous studies indicate that ACE experiences in women are associated with mental health disorders; however, these studies did not report mental health scores of participants or use the same measurements, thus we are unable to compare if mental health scores from our study of women with infertility differ from women in these other studies. Recurrent reproductive traumas, such as infertility and pregnancy loss, and the anticipation of continued infertility or future loss may contribute to cumulative psychological trauma. 12 Cumulative trauma and chronic stress have been associated with neuroendocrine dysfunction, immune system dysregulation, systemic inflammation, and cardiovascular disease, 43 which may partly explain the associations between ACEs and pregnancy loss, although further studies are needed.
Clinical implications
Among the general population, almost 42% of women experience 2+ ACEs. 44 Over half of the women in our study (55%) reported experiencing 2+ ACEs, reflecting the prevalence of childhood trauma in women with infertility and warrants future consideration. These women may be particularly susceptible to mental health complications, including moderate to severe anxiety, depression, and PTSD symptoms. Health care providers, including reproductive endocrinologists, OB-GYN physicians, nurse midwives, and nurse practitioners who care for women with infertility, could integrate ACE screening in their fertility treatment plans. This would allow providers to identify women who may be at higher risk for pregnancy loss and mental health complications, thereby facilitating individualized care plans that incorporate psychological support services. Olsen et al. 45 reported that women were open to ACE screenings, and they found it helpful when providers explained the screening, had a calm and caring approach when screening, had support services available after the screening for emotional triggers, and provided education on the relevance of the screening to their health and well-being. Targeted interventions can be included in fertility care plans to decrease anxiety, depression, and stress among women with a history of ACEs facing reproductive difficulties. By recognizing the impact of ACEs on women with reproductive trauma, health care providers can better address the mental health needs of these women and improve their quality of care and psychological outcomes.
In addition, it is important to consider ACE history, as women may be retraumatized during fertility treatments or procedures. Feferkorn et al. 46 found that women with a history of sexual abuse were triggered by some experiences during fertility treatments, such as securing hands or legs, transvaginal ultrasounds, or lying down on a procedure table. Patients can demonstrate trauma in other ways, such as anxiety, lack of eye contact, or distrust in providers and plans of care. 47 Health care providers may implement trauma-informed approaches when caring for women with infertility and CRT, and especially for those with a history of ACEs. Trauma-informed care is a precautionary method of acknowledging patients with trauma and allowing providers to proactively build mutual trust and rapport with patients to reduce traumatization during health care visits. Trauma-informed care approaches include remaining at eye level, asking permission and providing clear explanations before making physical contact, and jointly creating a plan of care with patients. 47 Including trauma-informed care practices may help improve patient satisfaction and mitigate the psychological distress of women with infertility, CRT, and a history of ACEs during health care visits for fertility treatments or procedures.
Limitations
The cross-sectional design of this study limits causation among the variables. Furthermore, this study had a small sample size, and the participants were homogeneous with similar socioeconomic and demographic characteristics, which may limit the generalizability of findings. Future studies with larger, more diverse samples and longitudinal designs are recommended to validate associations between ACEs and CRT and to examine the enduring effects of ACEs and reproductive trauma on long-term mental health outcomes. This study relied on self-reported data, which may result in response bias by under- or overreporting their experiences based on their memory recall and social stigmas. We also did not ask participants about coping resources or strategies, which could have led to a deeper understanding of our findings.
Conclusion
Our study found that women with CRT and infertility-only who experience two or more ACEs are at an increased risk for psychological distress. Women with CRT were also more likely to experience neglect, a substance-use household, a household member incarcerated, and verbal abuse at home than women with infertility-only. These findings indicate that ACEs are a potential risk factor for CRT and are associated with mental health disorders in women with infertility and CRT, though further studies are needed. Incorporating ACE screening and trauma-informed approaches within reproductive health care may help provide appropriate plans of care for women with infertility and CRT. Future research is needed to further understand the long-term implications of ACEs on reproductive diseases and trauma.
Authorship Contribution
A.Swift.: Conceptualization, methodology, investigation, formal analysis, supervision, and funding acquisition. Writing—original draft. A.Schroeder.: Conceptualization, investigation, and writing—original draft. M.S.: Methodology, formal analysis, data curation, and writing—review and editing. M.F.-P.: Methodology, investigation, validation, and writing—review and editing.
Footnotes
Author Disclosure Statement
The authors report no disclosures or conflicts of interest.
Funding Information
This study was supported by the Sponsored Activities and Research Catalyst (SPARC) Award through Research, Economic Development, and Engagement at East Carolina University.