
Abstract
Background:
During neoadjuvant therapy (NAT), patients with locally advanced breast cancer (LABC) experience psychological distress (PD) and adopt appropriate coping strategies.
Objective:
This systematic review aimed to examine the prevalence and changes in PD and coping strategies in patients with LABC during NAT and to evaluate effective interventions to reduce their PD.
Design:
Quantitative (cross-sectional, longitudinal, and interventional) and qualitative studies reporting PD and coping strategies related to NAT during LABC were included.
Data sources and methods:
PubMed, Cochrane Library, Scopus, ScienceDirect, Wiley Online Library, and Web of Science databases were consulted to gather relevant literature from the first publications until July 25, 2023. Selection was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Results:
A total of 41 articles were included, of which four were qualitative. The main results showed that the prevalence of depression before NAT ranged from 0% to 46% and that of anxiety from 5.5% to 54%. After NAT, the prevalence of depression ranged from 40% to 78.5% and anxiety accounted for 27%. Additionally, PD decreased during NAT. The main determinants of PD were perceived social support, living in joint families, being affected by COVID-19 infection, delays in diagnosis, and starting neoadjuvant treatment. For coping strategies, after NAT, “resigned coping” decreased, whereas “social support” increased, and active coping strategies were correlated with better PD. Some interventions found a reduction in PD, such as a mobile health application, fasting-mimicking diet, relaxation training, and guided imaging.
Conclusion:
These findings highlight the importance of considering PD and coping strategies in patients with LABC from diagnosis to the end of NAT. The results suggest that effective psychological interventions should be implemented.
Keywords
Introduction
Breast cancer (BC) is the most common cancer in women worldwide, and its prevalence continues to increase annually. As indicated by the International Agency for Research on Cancer, the incidence of BC increased by 24.3% between 2012 and 2020. 1 Locally advanced breast cancer (LABC) is a group of breast tumors characterized by advanced progression without distant metastases. It includes tumors surpassing 5 cm in size with regional lymph node involvement, as well as tumors of any size with invasion of the skin or chest wall, regardless of the lymph node regional involvement. 2
Neoadjuvant therapy (NAT) is commonly used for the treatment of LABC. Neoadjuvant chemotherapy (NACT) was originally administered to increase the rate of conservative surgery in patients with LABC who were initial candidates for mastectomy. 3 Subsequent research has revealed a correlation between obtaining a pathological complete response and good long-term clinical outcomes.4,5 NACT has the most significant benefits in patients with human epidermal growth factor receptor 2 (HER2)-positive and triple-negative BC.6 –8 However, there is a growing trend in the use of neoadjuvant endocrine therapy (NET) for estrogen receptor positive tumors. 3
Diagnosis and treatment of cancers such as NET in LABC can become a high and chronic stressor and thus contribute to persistent psychological distress (PD). 9 Owing to the seriousness of the disease, a significant number of women experience psychological disturbances during or after treatment. The most common symptoms include fatigue, depression, psychological stress, anxiety, and fear. 10 PD levels tend to be the highest at the time of diagnosis when patients are confronted with the initial shock and the consequences of their condition. Thereafter, these levels tend to decrease progressively as the patients begin treatment. 11 According to a meta-analysis, 32% of women with BC experienced depression. 12 In another study, 13 among women who underwent chemotherapy, the level of anxiety was highest before the first infusion session. 13 Women with BC develop PD for various reasons. These include treatment uncertainty; physical symptoms; fear of progression, recurrence, and death; body image; changes in female identity; sexual problems; difficulties in daily activities; family problems; and lack of emotional support. 14
Several publications15 –18 have shown that PD is a concept that covers different alterations, such as depression (hopelessness, sadness, lost interest), anxiety (feeling tense, restlessness), fear, the inability to cope positively with stress, and emotional disorders. The choice of the term “PD” to the detriment of other concepts takes its strength from the National Comprehensive Cancer Network (NCCN) Guideline, 17 which considers it less stigmatizing and more acceptable. Commonly, psycho-oncology researchers have turned to the NCCN guidelines to define PD as “a multifactorial unpleasant experience of a psychological (cognitive, behavioral, emotional), social, spiritual, and/or physical nature that may interfere with one’s ability to cope effectively with cancer, its physical symptoms, and its treatment.” 17 The concept of PD can also be extended to dimensions encompassing the quality of life (QoL) in patients with BC. Among these dimensions, emotional functioning (EF)19 –21 and emotional well-being (EWB)21,22 are examples that have been sufficiently mentioned in the literature.
Furthermore, women adopt coping strategies as a result of LABC. Indeed, women with this diagnosis must cope with the alterations in PD, deal with the side effects of treatment and surgery, and adapt to new life circumstances.23,24 In a systematic review 25 of 20 articles aiming to investigate coping responses following a diagnosis of different stages of BC, the most common coping strategies that patients used were seeking social support, positive reframing, reappraisal behaviors, religion/spirituality, emotional expression, avoidance, and distraction.
To the best of our knowledge, no systematic review has specifically examined PD and coping strategies or their determinants during NAT in patients with LABC. However, a recent publication focusing on QoL 26 attempted to present some results without covering all aspects of PD. 26 With the increased use of NACT in LABC, research has focused on understanding PD and coping strategies to provide more effective care for patients from diagnosis to survival. Therefore, we are convinced that an in-depth systematic review of PD and coping strategies in LABC patients receiving NAT should be carried out. A protocol for this systematic review 27 has already been published. Consequently, the main objectives were (a) to present the prevalence of PD and its different forms during NAT and its evolution, to describe the coping strategies adopted, (b) to examine the determinants of PD and coping strategies during NAT, and (c) to evaluate the interventions carried out to reduce PD.
Methods
This systematic review was designed according to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines (Appendix A in the Supplemental Material). This review presented an objective procedure for extracting the maximum information from studies on PD and coping strategies for patients undergoing NAT. The protocol was registered at International Prospective Register of Systematic Reviews (PROSPERO) under the registration number CRD42021230300. We worked to ensure the integrity of this systematic review from 2022 to the end of 2023.
Inclusion and exclusion criteria
We based our inclusion and exclusion criteria on PICOS (population, intervention, comparison, outcome, and study type). A summary of the PICOS elements constituting the systematic review is presented in Table 1. The following databases were searched to identify relevant articles: PubMed, Cochrane Library, Scopus, ScienceDirect, Wiley Online Library, and Web of Science. The search strategy used Boolean operators for the medical subject heading (MeSH) terms (Table 2). We also created alerts in the databases corresponding to our search equation to identify articles suitable for our review. We extended the bibliographic research to other sources, specific journals, and manual searches of articles using Google. As this is the first systematic review of the variables in question, we conducted a comprehensive search of studies spanning more than 20 years until July 25, 2023.
Summary of the PICOS elements that make up the systematic review.
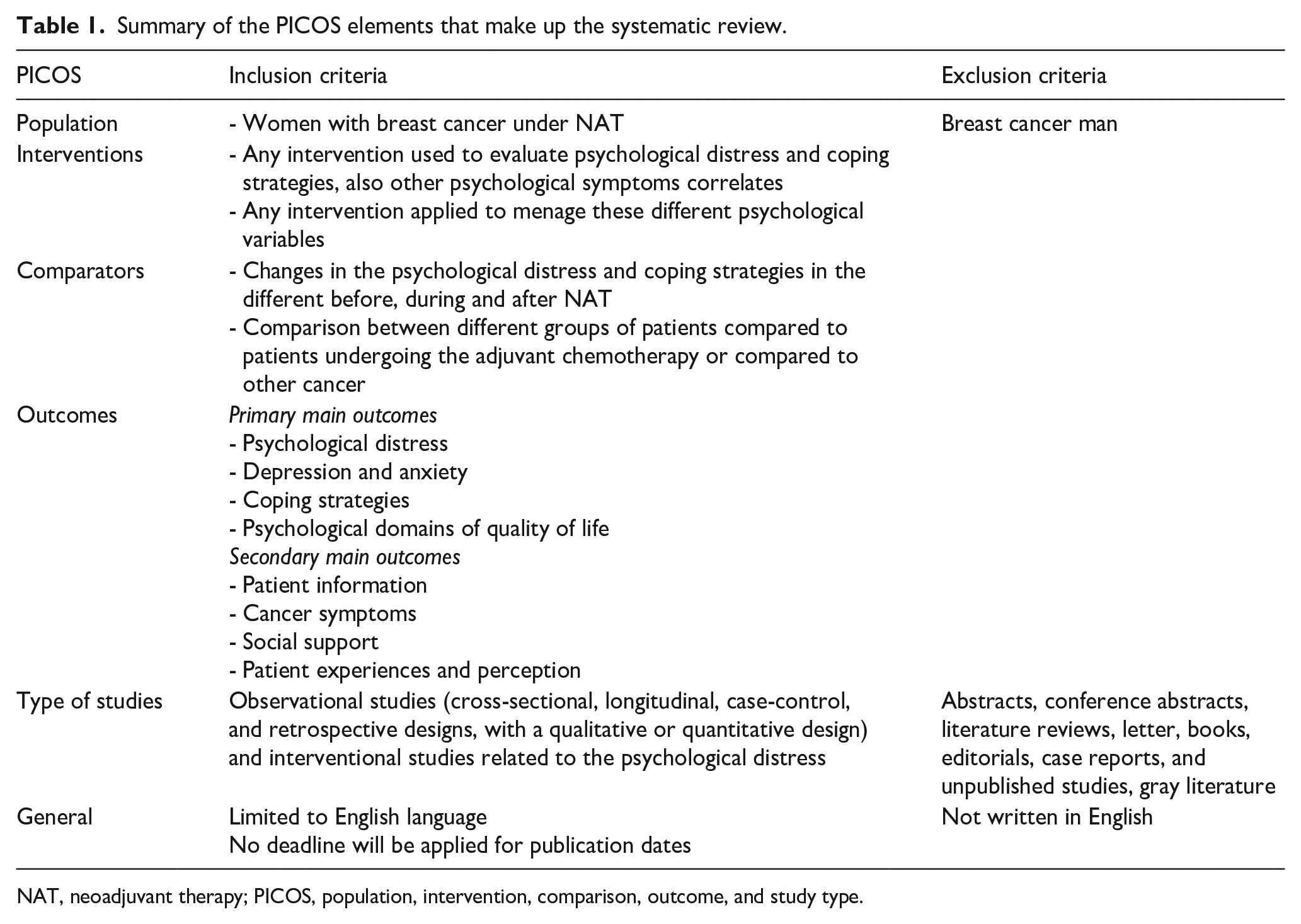
NAT, neoadjuvant therapy; PICOS, population, intervention, comparison, outcome, and study type.
Search strategy until July 25, 2023.

Data extraction
Two authors independently reviewed the inclusion and exclusion criteria of each study. All articles were collected using the Zotero reference management software, which allowed them to organize and read their titles and abstracts. Among the data extracted from each quantitative study were the first author’s name; year of study; sitting; study design; mean age; sample size; variables of interest and instrument; prevalence and mean of variables before, after, and during the NAT cycle; and the main significant changes and associates. For the qualitative studies, two reviewers listed the main findings for each theme.
Quality assessment
Two reviewers assessed the quality of the included studies using the QualSyst tool, which is generally preferred for both quantitative and qualitative studies. The QualSyst tool enables the evaluation of quantitative studies using 14 items, whereas 10 items are used for qualitative studies. 28 We noted each item was scored 2 for “Yes,” 1 for “Partial,” and 0 for “No”; items not suitable for the specified study design were labeled “NA” and eliminated while calculating the final score. Quality assessment for each quantitative study was performed by dividing the total possible score by the aggregate score, which was calculated by adding the relevant items. We calculated the scores of the qualitative studies using the same method. 28
Results
Description of included studies
A total of 2554 articles were found in the initial pool of articles. A total of 41 studies were included in this review. Figure 1 shows the selection procedure used in this study. In our systematic review, 4268 participants were included, resulting in original studies published between 1999 and 2023. Figure 1 presents a flow diagram of the process of this systematic review search, in accordance with the PRISMA guidelines. Tables 3 and 4 show the characteristics of the observational and interventional quantitative studies included in this systematic review, respectively, and Table 5 shows the qualitative studies.
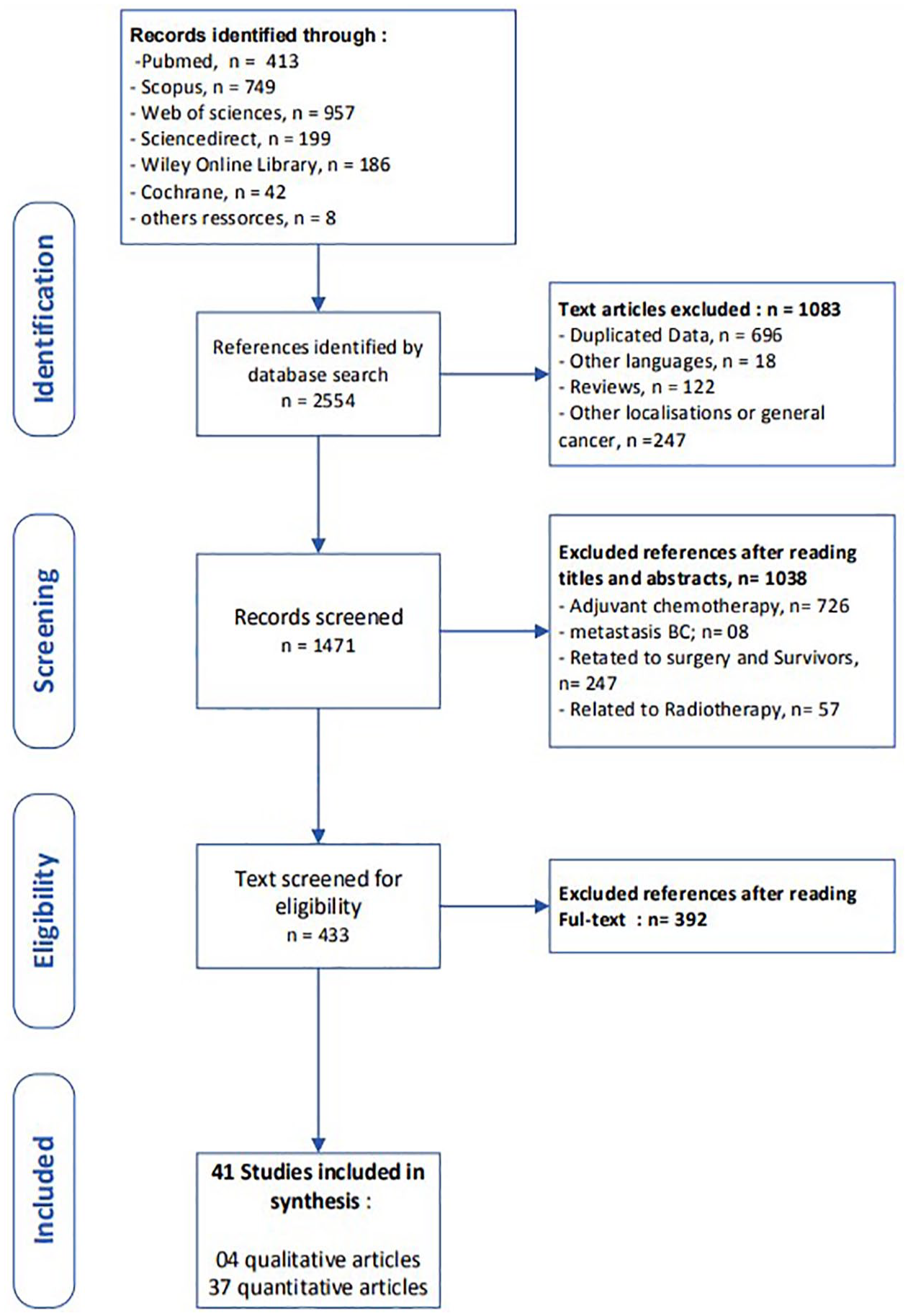
Flow diagram of the process of systematic literature search in accordance with PRISM guidelines.
Characteristics of included observational studies.

CD-RISC, Connor–Davidson Resilience Scale; FACT-B, Functional Assessment of Cancer Therapy-Breast; PR, prevalence; M, mean; EF, emotional functioning; t − 1, at baseline; t − 2, at end of NACT; NACT, neoadjuvant chemotherapy; HADS, Hospital Anxiety and Depression Scale; HADS-D, HADS-depression; HADS-A, HADS-anxiety; POMS-D, Profile of Mood State-Depression; NR, not reported; BSI, Brief Symptom Inventory; BC, breast cancer; UC, uterine cervix cancer; LET, Letrozole; BDI, Beck Depression Inventory; HAMD, Hamilton Depression Rating Scale; HAMA, Hamilton Anxiety Rating Scale; HER2, human epidermal growth factor receptor 2; ESAS-A, Edmonton Symptom Assessment Scale-Anxiety; CPC, Canadian Problem Checklist; PSSCAN-R, Psychosocial Screen for Cancer; HCG, healthy control group; PG, patient group; BAI, Beck Anxiety Inventory; BDI, Beck Depression Inventory; SDS, self-rating depression scale; SAS, self-rating anxiety scale; DT, Distress Thermometer; DA, decision aid; PSS, perceived social support; CRS, chemotherapy-related symptoms; PCG, patient cancer group; MDASI, M.D. Anderson Symptom Inventory; PSQI, Pittsburgh Sleep Quality Index; RSES, Rosenberg Self-Esteem scale; FEC 100, 5Fluorouracile-Epirubicine-Cyclophosphamide.
Characteristics of included interventional studies.

EACS, Emotional Approach Coping Scale; EF, emotional functioning; NACT, neoadjuvant chemotherapy; RCT, randomized controlled trial; STAI, State-Trait Anxiety Inventory; FCRI-SF, Fear of Cancer Recurrence Inventory—Short Form; FoP-Q-SF, Fear of Cancer Progression Questionnaire—Short Form; HADS, Hospital Anxiety and Depression Scale; HADS-D, HADS-Depression; HADS-A, HADS-Anxiety; CECS, Courtauld Emotional Control Scale; MSAS, Memorial Symptom Assessment Scale; FEC 100, 5Fluorouracile-Epirubicine-Cyclophosphamide; MOS SF-36, Medical Outcomes Study Short Form-36; FMD, fasting mimicking diet; RD, regular diet; EORTC-QLQ-C30, Cognitive Function Scale of the European Organization for Research and Treatment of Cancer (EORTC) Quality-of-life Questionnaire C30; NR, not reported; BSI, Brief Symptom Inventory; PSQI, Pittsburgh Sleep Quality Index.
Characteristics of included qualitative studies.

Several designs were considered for the articles included in this systematic review. Hence, there were 20 prospective studies,29 –33,35,36,39,40 –42,46,47,49-51,57,58,63,68 5 cross-sectional studies,34,37,52 –54 11 randomized controlled trial (RCT) studies,38,43,44,48,55,56,59–62,64 a retrospective and longitudinal study, 66 and 4 qualitative studies.65,45,67,69
Notably, China was the country with the maximum number (six) of publications,34,47,49,50,51,63 followed by Korea with five publications.32,36,40–42
Study quality assessment
The quality assessment scores for the studies included in the quantitative synthesis ranged from 64% to 95%. For quantitative studies, two cross sectional studies52,53 and two longitudinal studies30,31 had a rate of less than 80%, whereas other studies with the same design had a rate of more than 80%. For the randomized trials, a total of 12 articles had a rate of 71%–93%, and only 3 articles61,62,64 reported blinding of patients (Tables 3–5).
Quality assessment scores for the qualitative studies ranged from 80% to 85%. All the studies had clearly defined objectives with an appropriate design involving the use of clear and systematic methods. Nevertheless, qualitative studies had some limitations related to sampling and procedures for establishing the credibility of data, such as triangulation or member checking.
Sample characteristics
LABC filled most of the articles,29 –32,34,36 –43,45,47,49,51 –53,55 –60,63 –69 but some particular types were included, such as non-metastatic HER2-negative BC in46,54,61,62 and triple negative breast cancer (TNBC). 44 Additionally, postmenopausal BC patients with HR-positivity and their clinical stage, including T1c-T2, N0, and M0, were included in the study by Taira et al. 33 in patients with LABC, whereas LeVasseur et al. 35 included patients at stage I and stage IIa.
Commonly used NACT protocols were based on a combination of anthracycline and taxane29,32,36,40,51,54 or, alternatively, Cyclophosphamide, Adriamycin, and Fluorouracil regimens.30,31 Additionally, one study 41 focused exclusively on the AC regimen, whereas another study 42 was based on two protocols: doxorubicin/cyclophosphamide (AC) or docetaxel/doxorubicin (TA). Furthermore, in the study by LeVasseur et al., 35 some patients received NACT, whereas others received neoadjuvant endocrine therapy, without specifying their protocols. However, one study 33 was limited to neoadjuvant endocrine therapy based on letrozole. Regarding the comparison of subgroups, Chellappan et al. 53 presented protocols based on paclitaxel and doxorubicin administered every 3 days or every week. Barakat et al. 64 investigated the safety and tolerability of adding Metformin to NACT, and a study conducted by Rezapour et al. 57 assessed QoL in BC patients receiving AC-based therapy compared with those receiving Paclitaxel and Gemcitabine based regimens. Furthermore, some articles34,47,49,59,61,62,63 described the utilization of various therapy regimens, whereas other studies37,39,52,55,56,66,67 failed to specify the administered protocol.
Quantitative studies
In this section, we present the results related to PD and its different forms, namely, depression, anxiety, emotional, and/or psychological domains of QoL, and psychological symptoms. We then present the results related to coping strategies.
PD forms
Psychological distress
Six studies introduced PD through psychometric scales such as the Distress Thermometer,55,56,61,66 total Hospital Anxiety and Depression Scale (HADS) score, 33 and Brief Symptom Inventory.29,48 In terms of the prevalence of PD, one study 33 showed that it was significantly reduced after the initiation of NET, with a rate of 42% at baseline and 31% after NET, whereas two studies showed changes in PD. Indeed, a recent retrospective and longitudinal study 66 found that the level of distress peaked a month before treatment onset and fell steadily during NACT, and that the distress level of individuals receiving NACT was lower than that of individuals who received other treatment. 66 In the second study, 29 results showed that patients had significantly elevated levels of PD at baseline compared to the end of NACT.
Depression
Six instruments were featured in the included studies to measure depression. Fourteen studies employed the HADS,29,30,32,33,36 –39,40 –43,58,63 three utilized34,47,51 the Self-Rating Depression Scale, two used31,54 the Beck Depression Inventory, and two50,53 involved the Hamilton Depression Rating Scale (HAMD). Additionally, one study used the Profile of Mood State-Depression and another 63 applied the Patient Health Questionnaire-9.
Ten studies30 –32,36 –38,40 –42,51, evaluated the prevalence of depression at baseline, ranging from 0% to 46%. After NACT, four studies30,31,40,63 reported the prevalence of depression, with estimates ranging from 40% to 78.5%. Regarding the change in depression during NACT, only one study 29 reported that depression scores decreased significantly.
Regarding depression correlates, patients living in joint families 30 and those with children 54 tended to experience lower rates of depression. By contrast, patients with low perceived social support (PSS) expressed a high level of depression. 32 Moreover, increased depression levels have been linked to delays in diagnosis and initiation of neoadjuvant treatment. 54
Clinically, women who report higher levels of depression also demonstrate greater cognitive difficulties. 37 However, in a study conducted by Hermelink et al., 58 there was no significant correlation between cognitive test results and depression before NACT, whereas at the end of NACT, depression was associated with self-reported cognitive complaints. 58 Furthermore, certain side effects such as sadness, worry, nausea, and vertigo had a significant impact on the development of depression. 63 Additionally, an increase in the pain symptoms by one point resulted in a 1.123 times higher risk of depressive mood. 63 It should also be noted that patients with depression at baseline, compared to non-depressed patients, had a significantly high nutritional risk 51 and low BMI and potassium, total cholesterol, sodium, total protein, and fasting glucose levels during NACT. 51
Anxiety
Seven instruments were used to measure anxiety in the 19 included articles. HADS was used in 11 articles.29,32,33,36,38,39,40 –43,70 The self-rating anxiety scale was used in three articles.34,47,48 Two studies used the Spielberger State-Trait Anxiety Inventory,55,56 and the Beck Anxiety Inventory was used in only one study. 54 LeVasseur et al. 35 identified patients with anxiety using three instruments: the Edmonton Symptom Assessment Scale-Anxiety, the Canadian Problem Checklist, and the Psychosocial Screen for Cancer Revised.
At baseline, anxiety ranged from 5.5% to 54%.32,35 –38,41–42 However, after NACT and before surgery, only one prospective study 40 revealed an anxiety rate of 27%. When comparing anxiety means, four studies found that anxiety significantly decreased between the beginning and end of NACT29,47,49,50 and declined during neoadjuvant letrozole (LET) (NET). 33
Regarding sociodemographic correlates of anxiety, there was no significant association, 54 whereas the study of Kemer et al. 54 found that increased anxiety levels were associated with delays in diagnosis or the beginning of neoadjuvant treatment.
Clinically, anxiety remained significantly related to persistent chemotherapy-induced peripheral neuropathy 36 and the late chronotype 41 during NACT. Women who experienced a high level of anxiety also reported more difficulties with cognitive function. In contrast, one study 40 found that anxiety was moderately correlated with QoL during NACT.
PD as a domain of QoL
The study of PD can also be extracted from the dimensions encompassing the QoL scales used in patients with BC. Our results found the use of domains of the following QoL scales: EWB of the Functional Assessment of Cancer Therapy-Breast (FACT-B),33,52,54 EF of the European Organization for Research and Treatment of Cancer-Quality-of-life Questionnaire-C30 (EORTC-QLQ-C30),57,59,62,64 and mental health and role emotional (MH and RE) of the Medical Outcomes Study Short Form-36 (MOS SF-36). 60 Below, we present the correlations between these psychological dimensions. Thus, the EWB can improve or deteriorate depending on the nature of the NAT. Thus, EWB showed a significant improvement from baseline and during treatment based on NET, 33 whereas, in another study, 53 patients receiving weekly NACT had significantly better EWB than those receiving NACT every 3 weeks. Moreover, women who received social support from family or friends reported an improvement in EWB. 54 Regarding the coronavirus pandemic, patients who underwent NACT and acquired COVID-19 infection had a lower EWB (p = 0.03). In terms of the EF sub-scale of EORTC-QLQ-C30, the patients who received Paclitaxel and Gemcitabine at the end of NACT had a significantly higher mean EF than those who received Doxorubicin and Cyclophosphamide. 57
Psychological symptoms
The results in this section are based on multi-symptom patient-reported outcome questionnaires that involve psychological symptoms. The M.D. Anderson Symptom Inventory (MDASI) was used in two studies,32,63 whereas Fjell et al. 59 employed the Memorial Symptom Assessment Scale (MSAS) and Endocrine Symptom subscales added to the FACT-B. 33 Quality of sleep was also assessed with the Pittsburgh Sleep Quality Index (PSQI).
In a prospective study 32 using the MDASI, certain psychological symptoms, such as sadness, distress, memory loss, and insomnia, showed a significant decrease during NAT. Moreover, patients who experienced moderate-to-high levels of PSS presented significantly lower scores for distress, insomnia, and memory loss during NACT, 32 whereas another study 63 found that after NACT, 90.4% of patients suffered from sadness. Further, PSS from the friends group stated a significant decrease in distress, insomnia, sadness, and memory loss; and PSS from the significant others group reported a decrease in sadness and insomnia. 63 Taira et al. 33 presented the prevalence of psychological symptoms at baseline. It was noted that 42% of the patients had problems with interest in sex, 5.7% had irritability, and 5.5% presented with mood swings.
Sleep quality was assessed using the PSQI before NACT in three Korean studies.36,41,42 In fact, two studies found that 16.2% 36 and 16.4% 42 of the patients experienced poor sleep quality. Furthermore, 18.2% of patients had poor sleep quality in the third study. 41 In another study, 46 a significant increase in sleep duration was reported from baseline to the end of FEC 100 and from baseline to the end of all sessions of NACT.
Coping strategies
This section outlines the various scales used to assess coping strategies. We discuss the key findings of each study in relation to the coping strategies.
Our results showed that five articles29,38,40,52,68 involved coping strategies during the NACT. The instruments used in these studies included the Ulm Coping Manual, 29 Connor–Davidson Resilience Scale, 40 Courtauld Emotional Control Scale (CECS) in Walker’s RCT study, 38 the subscale “satisfaction with treatment and coping with disease management” in the QOL-Questionnaire for Cancer Patients Treated with Anti-Cancer Drugs-the Breast (QOL-ACD-B), 68 and the Rosenberg Self Esteem Scale. 52
Regarding the key findings of coping strategies, a longitudinal study by Tschuschke et al. 29 reported that before NACT, “fighting spirit coping” as an effective strategy was positively correlated with “social support coping,” and higher levels of “cognitive restructuring” were associated with lower psychological stress. During NACT, “resigned coping” decreased, whereas “social support coping” increased significantly. After the NACT, “active coping strategies” (“complying” with treatment,” “cognitive restructuring, “social support coping,” and “fighting spirit”) were correlated with better psychological adaptation, whereas “resigned coping” was associated with poorer psychological adjustment. 29 Overall, a higher score of “fighting spirit” was associated with better adaptation to treatment. 29
Resilience as an adaptive strategy, was mentioned in the study by Lee et al., 40 which found that before NACT, resilience was negatively correlated with depression and anxiety at each time point during NACT. In a study by Aprilianto et al., 52 self-esteem, an essential resource for coping with and adapting to cancer, reached a high level in 28.6% of patients, a moderate level in 48.2%, and a low level in 23.2% during NACT. Moreover, patients with a higher level of self-esteem reported better social support from their families. As a domain of the QOL-ACD-B scale, “satisfaction with treatment and coping with disease” did not change significantly between the two groups, those with high or low QoL, either before or after NACT. 68
Interventional studies
De Groot et al. 61 showed that patients receiving the fasting mimicking diet (FMD) program developed a 90%–100% response to the NACT, but PD levels did not significantly decrease under this intervention. In the study of Lugtenberg et al. 62 that included HER2-negative BC patients receiving NACT showed that those receiving the FMD had better scores of EF than those with a regular diet during NACT. In another RCT based on a decision aid program, 55 the authors showed that the mean baseline PD scores in patients undergoing NACT were not different from those in patients undergoing adjuvant chemotherapy. However, the same authors in another article 56 showed that PD, anxiety, and fear gradually decreased significantly after the dispensation of the Decision Aid program in patients undergoing NACT. In the RCT study by Walker et al. 38 based on a relaxation training and guided imaging program, depression in patients under the NACT increased significantly until cycle 5 and then declined until the end of NACT. The intervention decreased emotional suppression as a coping strategy, as measured by the CECS. Furthermore, women who practiced daily or more had lower levels of CECS unhappiness and the total score of CECS than control women. for CECS unhappiness and total score of CECS. 38 It should be remembered that the CECS is a questionnaire segregated into three subscales for the suppression or expression of anger, anxiety, and unhappiness mood.
One study found that an intervention group using a mobile health app experienced lower EF than the control group after completing the NACT. 59 Additionally, the intervention group had a lower prevalence of feeling sad and a better score on the MSAS-Psych subscale than the control group. 59 However, Barakat et al. found that the addition of Metformin to NACT did not improve EF scores from baseline to the last cycle of the NACT. 64
In summary, we can infer those programs such as the fasting-mimicking diet, the decision aid program, relaxation training and guided imagery, or the mobile health app can have a positive effect on the indicators of PD in patients with BC undergoing NACT.
Qualitative studies
The synthesis of the four qualitative articles included in this systematic review allowed us to design three themes related to patients’ experiences during NACT: (a) patient challenges and needs during the NACT; (b) information and decision-making regarding the NACT; and (c) interventions and strategies reassuring patients during the NACT.
PD during NACT
During diagnosis, it was difficult for patients to assimilate what happened when the first symptoms of BC were discovered, and they did not attempt to perform a self-examination or engage in any form of care. 45 They experienced a high level of distress and anxiety, 45 and had a sense of fear and panic. 45 Receiving the NACT regimen was expected to be a challenging and traumatic experience. 67 It was difficult for them to know that cancer remained in the body during NACT and that severe side effects may occur. 67 Thus, they transitioned from fit and healthy to ill. 67 Additionally, the patients expressed concerns about their families. In particular, they worried about their children and husbands’ reactions to the worrisome information they received about the disease. 67 Regarding care, patients noted that the lack of continuity in care was reported as a result of meeting too many nurses and physicians in each appointment, 65 and that accessibility issues were caused by lack of time, and nurses were frustrated. The findings also indicated that few women said that they had benefited from psychological support, 67 and others preferred to receive support from patients who had undergone the NACT. 67 Furthermore, surgical decision-making raised prognostic concerns among participants who mobilized anxious preoccupation as a coping strategy. 45
Information and decision-making about NACT
Receiving information can be considered a source of frustration and anxiety. 67 Indeed, patients would have difficulty retaining the information received at the time of diagnosis, and receiving all the information was perceived as stressful. 67 They also reported experiencing anxiety when searching for information on the Internet. 67 Patients participating in the study of Fjell et al. 65 reported insufficient information in certain areas of care, whether others felt there was too much information. In some cases, the patients felt that information regarding the reasons for NACT was withheld. 65 Therefore, they expressed the need to obtain more information using other resources. 65 Women viewed the decision-making process as a burden rather than an opportunity. 69 They struggled to accept the preferential nature of NACT, particularly because the survival benefits were comparable to those of the initial surgery. 69 Additionally, some women perceived that they had no other treatment options 69 and that their doctors influenced their decisions, stating that it was the best option. 69 Thus, they did not play an active role in choosing NACT. 69
Among the reasons involved in decision-making was the need for urgent action to avoid deterioration in their health condition, which led women to feel that a quick decision was necessary. 69 For most women, decision-making occurred either during or shortly after their first oncology consultation. 69 They considered key reasons for admitting NACT, such as breast-conserving therapy rather than mastectomy, personal circumstances, or what they considered psychological acceptable. 69
Interventions and coping strategies reassuring patients during NACT
Patients considered family relationships as a motivating factor to pursue treatment after diagnosis, and it was associated with high rates of fighting spirit. 45 Regarding informational coping, patients sought to use additional information about NACT decisions by receiving written information or a decision-aid program, 69 which helped them understand their doctors. 69 Furthermore, the patients expressed their satisfaction with written and verbal information 65 and viewed that online forums could be reassuring. 67
Regarding NACT and care, several women reported that they appreciated their doctor’s suggestions regarding a treatment plan and their offer to adjust the treatment protocol at any moment. 69 Patients also reported that discussing topics related to the NACT was important for their sense of involvement 65 and that receiving the treatment plan simplified their daily organization. 65 Furthermore, 65 access to nurses was viewed as a beneficial and warm atmosphere in oncology clinics that allowed patients to have reassuring relationships.
For using health mobile applications in the study by Fjell et al., 65 the patients described them as an easy and accessible source of information, especially on how to manage their symptoms. 65 They confirmed that in the event of severe concern, they were able to reach the contact nurse directly. 65 This application allowed patients to report their health conditions to nurses. Patients felt seen, listened to, and monitored positively. 65 The main elements of the results section are illustrated in Figure 2.

Conceptual map of psychological distress and coping strategies attributes, determinants, and effective intervention approaches.
Discussion
This systematic review analyzed 41 articles about PD and coping strategies in patients with BC during the receipt of NAT to examine their prevalence and changes, the different associated determinants, and different interventions reducing the level of PD.
Through our review, we identified 13 forms of PD: depression, anxiety, emotional domains related to QoL, stress, fear, sleep disturbances, self-esteem, problems with interest in sex, irritability, mood swings, insomnia, memory loss, and sadness. The included articles reported multiple coping strategies such as fighting spirit, social support, cognitive restructuring, compliance with treatment, resilience, emotional suppression, CECS unhappiness, satisfaction with treatment, coping with disease, and informational coping.
Prevalence and change of PD
Before the start of the NACT, only one study 29 estimated PD using the DT scale, with a prevalence of 42%, whereas the results showed that the prevalence of depression ranged from 0% to 46% and anxiety ranged from 5.5% to 54%. Regarding other psychological symptoms in patients receiving NET, 33 42% of patients had problems with interest in sex, 5.7% had irritability, and 5.5% presented mood swings. An analysis of the qualitative studies included in this review concluded that during the diagnosis phase, distress, anxiety, fear, and panic were the main disturbances reported by patients. 45
We considered these prevalence (PR) rates to be heterogeneous and difficult to compare with the results of similar studies. However, the use of different measurement scales, especially to assess depression and anxiety, as well as the sensitivity of the answers to the questionnaires, contributed to producing different PR rates, while we cannot underestimate the psychological shock of diagnosis and treatment for patients. 11
Conversely our findings before and after NAT showed that depression rates ranged from 40% to 78.5%, although only one prospective study reported an anxiety rate of 27% after NACT. 58 In addition, one study 63 found that 90.4% of patients experienced sadness. The articles that presented the PR of different forms of PD after NAT and before surgery were relatively limited. This could have led to an underestimation of the magnitude of PD during this phase. Indeed, this period is marked by the management of adverse effects of NACT as well as preparation for surgery. However, the included articles did not cover the PR of PD for each NACT cycle. Consequently, it is difficult to follow its evolution correctly. However, some of these articles examined variations in the mean scores of psychological variables, comparing them before and after receiving NACT, and only one article explored these changes in each NACT cycle. 66 Two studies measured it at mid-treatment and at the end.33,46
Our results showed that at the start of NACT, the levels of PD, depression, anxiety, sadness, insomnia, and memory loss were high but gradually decreased until the end of treatment; hence, the level of EWB showed improvement. In comparison with the findings of a recent prospective study related to adjuvant chemotherapy in early-stage BC, the percentage of patients presenting with anxiety decreased from the beginning to the end of complete treatment. Similarly, the mean anxiety scale scores reduced and EWB improved during this journey. 71
Despite this variability, the findings highlighted a problem that must be considered. 72 It is essential to assess PD in patients with cancer as soon as the diagnosis is announced, until the start of chemotherapy, at each NAT cycle, and in the period from the end of NAT to the time of surgery. Therefore, providing adequate attention and appropriate interventions for these psychological problems during these periods is crucial.72,73
Determinants associated with distress
The results of this systematic review highlighted the various determinants of PD. Thus, high PSS was correlated with lower levels of insomnia, distress, and memory loss during NAT 32 and when PSS arose from family and friends, EWB (FACT-B) 54 and self-esteem 52 improved. Additionally, lower levels of depression were associated with patients who had sons and daughters, 54 lived in joint families, 30 and had low PSS. 32 Moreover, insomnia and sadness decreased when the level of “PSS stems from the significant person” was high. 32
Regarding clinical determinants, adverse symptoms of NACT such as worry, sadness, vertigo, nausea, and pain had an impact on developing depression. 63 Patients with higher levels of depression or anxiety reported experiencing more cognitive difficulties before NACT and self-reported more cognitive complaints after NACT.37,58 Compared to non-depressed patients, patients with depression at baseline had a significantly higher nutritional risk and lower BMI, potassium, total cholesterol, sodium, total protein, and fasting glucose levels during NACT. 51 This review led us to propose further research exploring psychological clusters in patients with LABC from diagnosis to the time of surgery. In addition, Kemer et al. 54 found that delays in the diagnosis or commencement of NAT were related to higher levels of depression and anxiety. In this context, researchers have concluded that any delay of more than 3 months between the first medical consultation, and the start of cancer treatment is associated with a more advanced stage of the disease and reduced survival.74 –78 We suggest strengthening “patient navigation” programs for patients with BC, to overcome the obstacles that mainly cause delays in therapeutic management. Such projects would also help reduce PD in these patients. 79 Regarding COVID-19 infection, there was poor EWB (FACT-B) in patients undergoing NACT who were diagnosed with COVID-19. These results are consistent with those of previous studies on COVID-19 and cancer. 80 Therefore, they emphasize the need to offer support to patients during difficult periods, including future pandemics.81 –83 Qualitative studies identified several determinants that contribute to PD. These included the side effects of NAT, living with the perception of being “sick,” as well as concerns about family members, the nature and sources of information received, and the decision-making process.45,67 Other determinants were also revealed, 65 such as the lack of continuity of care, meeting different nurses and doctors, and the consequences of the surgery that they had to undergo after NACT.
Coping strategies
Regarding coping strategies, two articles29,40 included in this review found that before NACT, higher levels of “cognitive restructuring” were associated with lower psychological stress 29 and that resilience was negatively correlated with depression, anxiety, and QoL during NACT. 40 Cognitive restructuring, considered an adaptive coping strategy, involves identifying unhelpful thoughts that lead to feelings such as anxiety and depression and analyzing them for their truth, accuracy, and validity while developing more helpful ones. 84 Given the significance of this strategy, the development of clinical interventions that rely on cognitive restructuring is of utmost importance in patient care. Our results also showed that during NACT, “resigned coping” decreased, whereas “social support coping” increased significantly. 29 After NACT, 29 “active coping strategies” were correlated with better psychological adjustment, whereas “resigned coping” was associated with poorer psychological adaptation. 29 Resignation occurs when an individual struggles to achieve unattainable goals, resulting in PD and reduced well-being. 85 Concerning informational coping, qualitative studies reported that patients searched for information on the Internet, but it was seen as terrifying and anxious 67 and they expressed their need for empathy, support, and advice to cope with the effects of the diagnosis.65,67 They sought additional information on NACT decisions by receiving written information or a decision-support program. 69 Our results are consistent with those of several studies, demonstrating that adopting active positive coping strategies during diagnosis and seeking social support are associated with better psychological adjustment.86 –90 Moreover, negative strategies such as anxious preoccupation, feelings of lack of control, avoidance, and denial are associated with deteriorating MH in patients with cancer.81,83,91,92
Intervention to reduce psychological distress
Among the interventions that demonstrated efficacy in this systematic review, the AD program,55,56, mobile health application, 59 FMD program, 62 and relaxation training and guided imaging program 38 were found to be beneficial in reducing the extent of PD during NACT.
Per the present systematic review, the DA program55,56 was characterized by a decrease in fear of progression, anxiety, and distress from baseline until the end of the NAT. The results also indicated that using a mobile health application showed an improvement in EF (EORTC-QLQ-C30), a lower prevalence of feeling sad, and better MSAS-Psych scores after NAT. 59 Regarding the qualitative study results, the patients described the use of this mobile application as an easy and accessible source of information, particularly on how to manage their symptoms, and as a safe space for interaction with nurses. 65 Self-management programs based on mobile technology are increasingly providing various types of care, including psychological interventions. 93 These studies support the feasibility and efficacy of digital psychosocial interventions,94,95 which may decrease anxiety, depression,96,97 and distress. 94
Furthermore, in this review, patients receiving an FMD program showed an improvement in EF (EORTC-QLQ-C30) during NACT. 62 In another RCT study 38 based on a relaxation training and guided imaging program, depression increased until sequence 5, and then increased until the end of NACT. Moreover, the intervention reduced emotional suppression and unhappiness. 38
By referring to recent guidelines on the management of distress, depression, and anxiety,17,98,99 we identified other interventions for patients with BC. These include psychoeducation, cognitive-behavioral therapy, supportive therapy or counseling, relaxation training or mindfulness-based therapy, supportive expressive therapy, problem-solving therapy, and other interventions.
Limitations
The findings of this systematic review cannot be generalized owing to several limitations. Although most publications were limited to depression and anxiety, we attempted to introduce other concepts attributed to PD by referring to the definitions mentioned in the NCCN guideline. 17 This approach did not, however, provide sufficient clarity on PD, since a total of 13 attributes were involved. Consequently, our ability to draw a definitive conclusion remains limited, and we were unable to accurately compare the different levels and attributes of PD because of the varied measurement tools used in the included articles. However, owing to the limited number of articles involved in the study, we were unable to obtain a clear picture of coping strategies before and at each cycle of NET; specifically, we were unable to identify the most mobilized strategies. Furthermore, most of the included quantitative studies presented only prevalence values without other statistics, such as confidence intervals. Therefore, the conclusions of this analysis are not suitable for a meta-analysis and should be interpreted with caution.
Conclusion
This systematic review identified the main conclusions drawn from an analysis of the included articles. Thus, the rates of PD and its attributes in patients who were followed up sometimes exceeded 50%. Additionally, various factors associated with PD were identified, and their identification remains crucial for predicting distress and guiding future research. However, results concerning coping strategies are limited, highlighting the need for further research on these strategies. These findings highlight the importance of addressing PD and assessing coping strategies in patients with LABC at crucial points from diagnosis to the end of NAT, and immediately before surgery.
This systematic review, alongside an examination of key psycho-oncology guidelines, highlights the main interventions that can help reduce PD and facilitate the adoption of effective coping strategies. Implementing these strategies would improve the preparation and support for patients throughout their care pathway, not only during NAC, but also at later stages, such as radiotherapy, hormone therapy, and plastic surgery.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241276232 – Supplemental material for Psychological distress and coping strategies in breast cancer patients under neoadjuvant therapy: A systematic review
Supplemental material, sj-docx-1-whe-10.1177_17455057241276232 for Psychological distress and coping strategies in breast cancer patients under neoadjuvant therapy: A systematic review by Majid Omari, Lamiae Amaadour, Achraf El Asri, Zineb Benbrahim, Nawfel Mellas, Karima El Rhazi, Mohammed El Amine Ragala, Jaouad El Hilaly, Karima Halim and Btissame Zarrouq in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.