
Abstract
Objective
To investigate the relationship between health-promotion behaviour and psychological distress and whether menopausal symptoms and social support mediate these relationships in patients with breast cancer receiving endocrine therapy.
Study design
This was a cross-sectional study involving convenience sampling that involved 226 patients with breast cancer.
Main outcome measures
Participants were investigated by self-reporting questionnaires that included demographic and clinical information, the Kessler psychological distress scale, the Health-Promoting Lifestyle Profile Ⅱ, the Menopause Rating Scale, and the Perceived Social Support Survey to measure psychological distress, health-promoting behaviour, menopausal symptoms, and social support, respectively. Mediation analyses were conducted with the bootstrapping method to test for mediating factors.
Results
In total, 78.7% patients reported that they were suffering from psychological distress. Their health-promoting behaviours were directly and negatively associated with psychological distress. In addition, health-promoting behaviour had a significant indirect effect on psychological distress through menopausal symptoms and social support. Mediating effects accounted for 34.8% and 27.6% of the total effect, respectively.
Conclusions
There was a high prevalence of psychological distress in patients with breast cancer receiving endocrine therapy. Menopausal symptoms and social support mediated the association between health-promoting behaviour and psychological distress. Health professionals should evaluate menopausal symptoms and health lifestyles, and provide professional interventions to increase health-promoting behaviours and manage unpleasant somatic symptoms for patients and their caregivers; these actions may improve their psychological distress.
Keywords
Introduction
Breast cancer is the most common cancer in women worldwide. 1 Owing to improvements in breast cancer treatment, long-term survival is now common after treatment, with a 5-year survival rate of almost 90%.1,2 Of the different forms of breast cancer, approximately 70% of patients present as hormone receptor-positive and need to receive at least 5 years of endocrine therapy; in some cases, therapy may last as long as 10 years.2,3 Adjuvant endocrine therapy (AET) is one of a crucial form of component therapy, following primary treatment including surgery and chemotherapy, to reduce the mortality and recurrence of breast cancer. 3 However, patients with AET suffer from physical and psychological distress, including depression, hot flushes, arthralgia, and fatigue.4,5
Psychological distress (PD) is a prevalent problem among breast cancer patients across different periods of illness. 6 PD is defined as an unpleasant emotional experience that leads to the inability to cope with negative events, manifesting with non-specific symptoms of mental problems, such as anxiety and depression. 7 Previous studies showed that the incidence of PD ranged from 30% to 75%.6,8 Evidence also showed that PD was strongly associated with somatic symptoms, low well-being, and caused negative impacts on a patient’s quality-of-life and physical functionality. 9 Moreover, PD is known to increase poor treatment adherence, and increase the risk of cancer recurrence and mortality.6,10 Therefore, we need to pay more attention to PD in patients with breast cancer receiving AET.
Previous researchers have reported that PD is related to several factors, including socio-demographic and clinical characteristics. 11 More specifically, the results of previous studies revealed significant differences in the level of PD among breast cancer patients of different ages, educational level, marital status, stage of cancer, and the time of treatment. 7 However, some researchers have reported conflicting data; it is believed that these discrepancies relate to the diversity of measurement tools and geographical regions. 7 Perceived social support, regarded as a protective factor, is also known to exert impact on PD.7,11,12
Health-promotion is the process of adopting health-promoting behaviours for individuals to maintain physical and mental health. 13 With the guidance of the action plan provided by the Healthy China 2030 initiative, significant emphasis has been placed on health promotion lifestyles in breast cancer patients. 14 Evidence suggests that health promotion behaviours, including engaging in healthy diet and physical activities, have a positive effect on enhancing the level of well-being, improving the quality-of-life and reducing mortality.15,16 Nevertheless, there is limited evidence relating to the relationship between health promotion behaviour and PD in breast cancer patients with AET.
Menopausal symptoms, as clinical manifestations of estrogen deficiency, are one of the most common symptom clusters in patients with AET, including hot flushes, night sweats, vaginal dryness, and muscular/joint pain. 17 The incidence of menopausal symptoms ranges from 37% to 95%; these are higher than for women without breast cancer. 5 These symptoms contribute to emotional distress and affected patients are more likely to become depressed. 18 However, the specific role of menopausal symptoms on PD in breast cancer patients with AET remains uncertain.
This study was designed to investigate the relationship between social support, health-promotion behaviour, menopausal symptoms and PD, and to investigate the role of social support and menopausal symptoms in the relationship between health-promotion behaviour and PD in breast cancer patients with AET.
Methods
Participants
This was a cross-sectional study and involved the convenience sampling of 226 patients. Eligible participants were included if they (a) were over 18 years of age, (b) had a pathological diagnosis of breast cancer, (c) were currently taking, or had received endocrine therapy, and (d) had the ability to read and communicate in Chinese. Patients were excluded if they had other types of cancer or cognitive impairment.
Procedure
Patients were recruited from breast oncology clinics in one oncology hospital between March 2020 and February 2021. Researchers screened eligible patients and introduced the purpose of the study and the procedures involved. All patients were willing to participate in the study and provided signed and informed consent. A paper-based self-reporting questionnaire was used to collect the data and was completed by each participant independently. Subsequently, researchers examined each questionnaire for missing data and returned it back to the participant if additional data were required.
Measures
Demographic and clinical information
A range of sociodemographic data were collected in this study, including patient age, educational level, marital status, employment status, average monthly family income, and menopause status. Disease data included cancer stage, the history of chemotherapy, and the time on current endocrine therapy.
Psychological distress
The Kessler psychological distress scale (Kessler 10), developed by Kessler et al., 19 was used to assess non-specific psychological distress over the previous 4 weeks. 19 This scale features a total of 10 items and each item was rated using a 5-point Likert scale from 1 (none of the time) to 5 (all the time), ranging from 10 to 50. Higher scores indicated more severe mental distress. A total score exceeding 15 points was considered psychological distress. 20 The Cronbach’s α coefficient in this study was 0.936.
Health-promoting behaviours
The Health-Promoting Lifestyle Profile Ⅱ (HPLP-Ⅱ), developed by Walker et al. 21 and the Chinese version revised by Cao, 22 were used to measure the health-promoting lifestyle behaviours of individuals. This is a 40-item scale with six dimensions, including health responsibility, exercise, nutrition, spiritual growth, interpersonal relationships, and stress management. Each item was scored on a 4-point Likert scale. Higher scores indicated better health-promoting lifestyles. 22 In the present study, the Cronbach’s α of this scale was 0.947.
Menopause symptoms
The Menopause Rating Scale (MRS) was originally developed to measure the severity of menopausal symptoms in women 23 and consists of 11 items with response options on a 5-point Likert scale from 0 (no symptoms) to 4 (very severe). The scale is further divided into three subscales (somatic, psychological, and urogenital) with higher scores representing greater severity. 23 In the present study, the Cronbach’s α of this scale was 0.808.
Social support
The Perceived Social Support Survey (PSSS) was compiled by Zimet 24 and translated into Chinese by Jiang. 25 We used the PSSS survey to evaluate an individual’s social support. The PSSS is a 12-item scale with three subscales, including support from family, friends, and significant others. Each item is rated by a 7-point Likert scale from 1 (very strongly disagree) to 7 (very strongly agree). 25 In the present study, the Cronbach’s α of this scale was 0.950.
Statistical analysis
All statistical analyses were performed in SPSS version 23 and PROCESS version 4.0. Demographic data and key variables were subject to preliminary descriptive statistics. Categorical variables are presented as frequencies and percentages. All continuous variables were first tested using Kolmogorov–Smirnov method to confirm that they were distributed normally. Variables that were distributed normally are presented as mean (with standard deviation; SD). Otherwise, non-normally distributed variables are shown as median (interquartile, IQR); these variables included some of the main variables (psychological distress, health-promoting behaviours, menopause symptom, and social support).
Univariate analysis was used to compare key variables with regards to different characteristics; we used the Mann Whitney U test for comparisons between two groups and the Kruskal Wallis test for comparisons between three or more groups. Spearman’s correlation was conducted to investigate the association between the main variables. A multivariate linear regression model was used to test the relationships between the four variables; in thus analysis, demographic variables that were significantly associated with the key variables in the bivariate analysis were included as covariates to control their effects.
To test the proposed hypotheses, multiple mediation analysis was performed by the regression bootstrapping method using The PROCESS macro in SPSS developed by Hayes. 26 Specifically, two sets of mediation analyses were conducted by examining the mediating effect of menopause symptom (M1) and social support (M2) on the relationships of health-promoting behaviours (X) with PD (Y). In each equation model, a, b, and c were presented as coefficients between two variables. a*b was calculated to represent the mediating effect. Bootstrapping samples were set to 5000 samples with a 95% confidence interval (CI). p values <0.05 were regarded as statistically significant.
Results
Participant characteristics
The status of psychological distress, health-promoting behaviour, and menopausal symptoms and social support by different characteristics (n = 226).
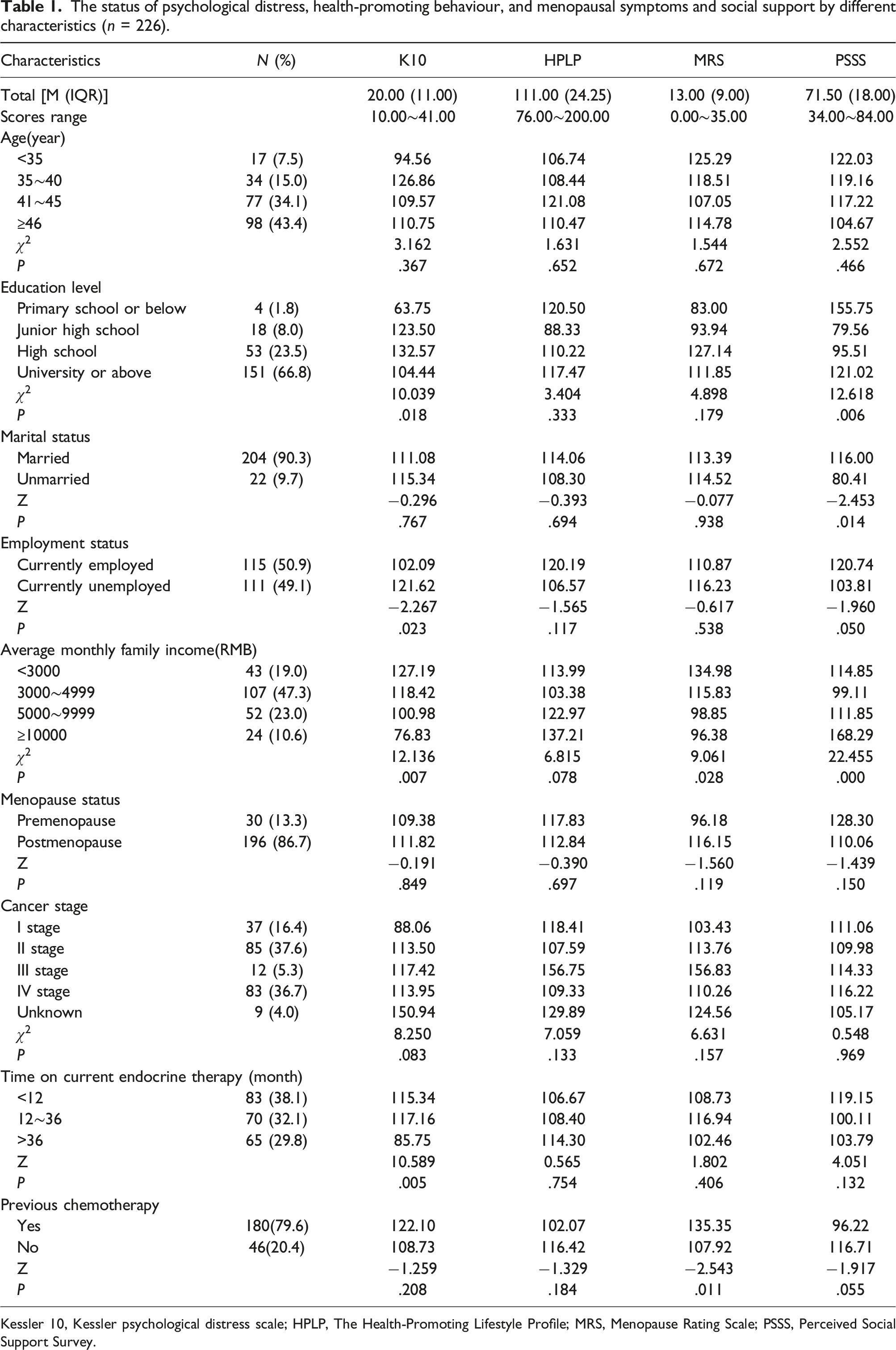
Kessler 10, Kessler psychological distress scale; HPLP, The Health-Promoting Lifestyle Profile; MRS, Menopause Rating Scale; PSSS, Perceived Social Support Survey.
The scores for PD, health-promoting behaviour, menopausal symptoms, and social support were 20.00 (IQR: 11.00), 111.00 (IQR:24.25), 13.00 (IQR: 9.00), and 71.50 (IQR: 18.00), respectively. Of the 226 breast cancer patients with AET, 178 (78.7%) patients reported suffering from PD. Further participant characteristics and the status of PD, health-promoting behaviour, menopause symptoms, and social support by different characteristics are presented in Table 1.
The associations between psychological distress, health-promoting behaviour, menopausal symptoms, and social support
Correlation among the main variables of interest (n = 226).
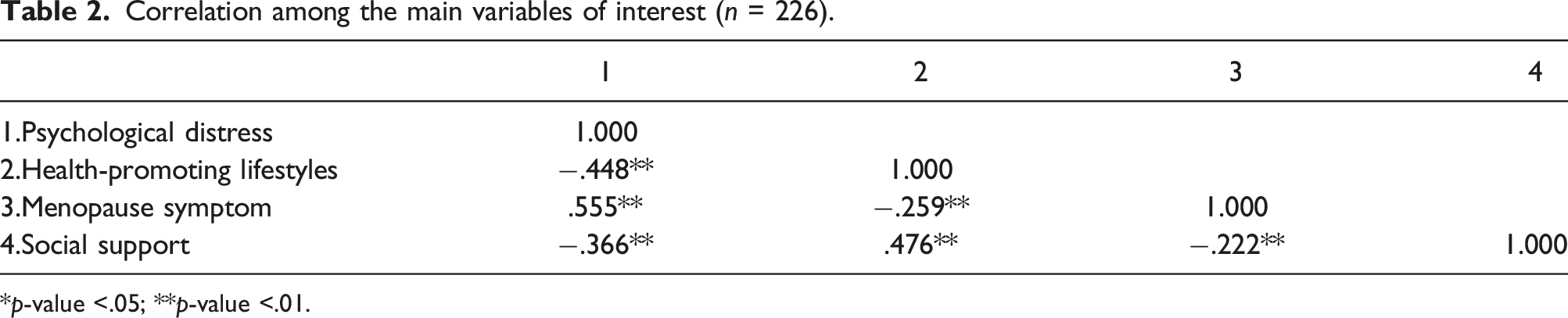
*p-value <.05; **p-value <.01.
Multivariate linear regression analysis of association among psychological distress, health-promoting behaviour, menopausal symptoms, and social support.
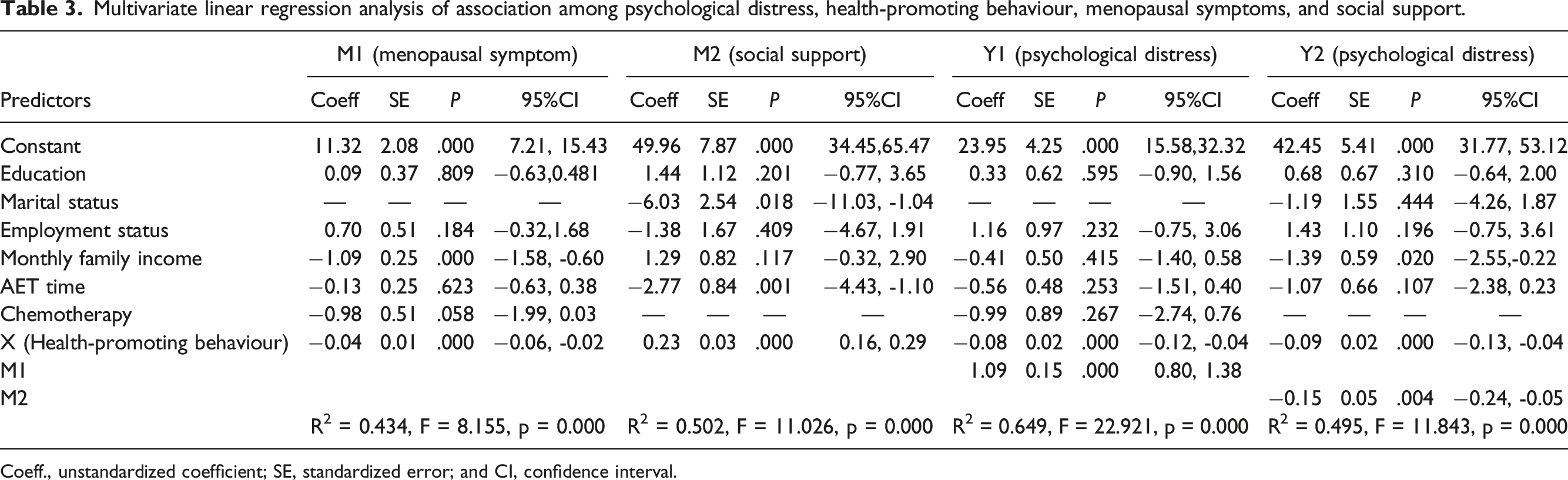
Coeff., unstandardized coefficient; SE, standardized error; and CI, confidence interval.
Mediation model analysis
Mediation analysis was conducted using the PROCESS macro in SPSS. In equation path 1, the indirect effect of menopausal symptoms in the association between health-promoting behaviour and PD was -0.041, with a 95% confidence interval (CI) from -0.069 to -0.022. The mediated effect accounted for 34.8% of the total effect (Z = −3.242, p = .001, Figure 1). In equation path 2, the indirect effect of social support on the association between health-promoting behaviour and PD was -0.033, with a 95% CI from -0.056 to -0.010. The mediated effect accounted for 27.6% of the total effect (Z = −2.661, p = .008, Figure 1). Mediating effect of menopausal symptoms and social support on the relationship of health-promoting behaviours with psychological distress.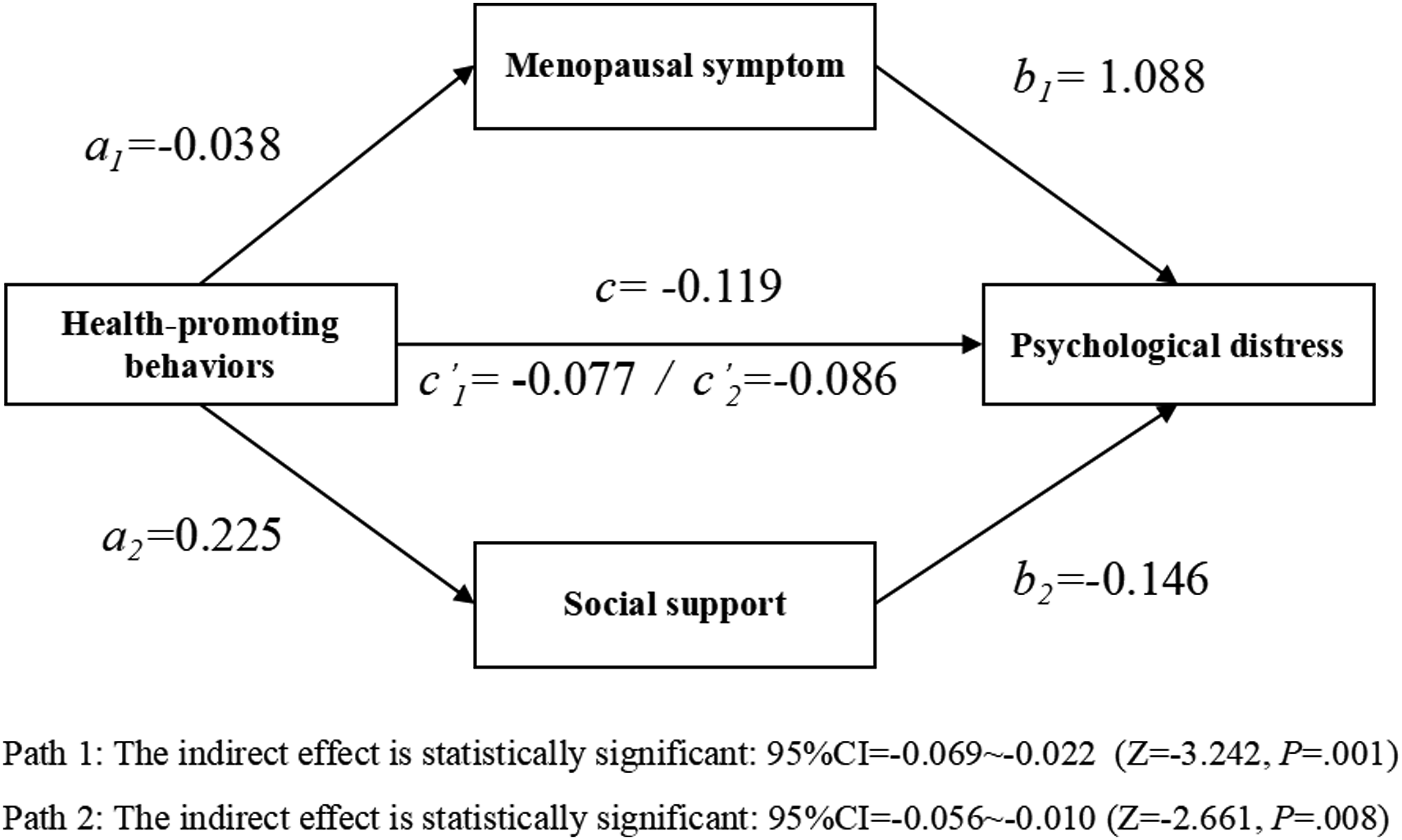
Discussion
To our knowledge, this is the first study to investigate the association between health-promoting behaviour and PD in patients with breast cancer receiving AET and examine the mediating roles of menopausal symptoms and social support. Our analysis showed that health-promoting behaviour had positive impact on the mental health of patients and that menopausal symptoms and social support mediate the association between health-promoting behaviour and PD in Chinese women with breast cancer receiving AET. These findings will assist researchers and clinicians to better understand the mechanism between the study variables, and will contribute to the development of related interventions and clinical practices.
In the current study, the median score of PD was 20.00 (11.00) and 78.7% of all patients had reported experiencing PD. This result is inconsistent with previous research and somewhat higher than the outcome reported in earlier research, which indicated that 42% of patients suffer from PD. 27 Of the 226 patients in our study, 56.6% were younger than 46, 86.7% were postmenopausal and 79.6% had a history of chemotherapy. It is possible that younger women who have received chemotherapy also suffer from premature ovarian insufficiency, which increases psychological sequelae. Compared with women younger than 46, older women with breast cancer, who experience menopausal symptoms may experience less distress in view of the more congruent social and cultural experience, being closer to the average age of menopause. Furthermore, the reported prevalence of PD varies in accordance with study design and assessment tools. 28
According to univariate analysis, patients with a lower education level, with a lower average monthly family income, those who were unemployed, and those with a shorter duration of AET, all experienced more severe PD; however, only average monthly family income acted as an influencing factor based on multiple regression analysis. We found that patients with a poor financial situation had a clear risk of PD. One possible explanation for this is that patients with economic burden experience more stress with regards to maintaining their previous normal life, have limited access to medical resources, and have little energy to manage their health status; therefore, they would be more likely to experience depression and anxiety symptoms. 29 Similarly, several previous studies have found that patients experienced more PD if they were unmarried, less educated, taking AET within the first 2 years, lived in rural areas, or had a greater burden of symptoms.7,11
Our analyses also indicated that health-promoting behaviour was a protective factor for PD in patients with breast cancer receiving AET; this is consistent with previous literature.18,30 Health-promoting behaviours have a direct effect on PD, which is evaluated across six sections: health responsibility, physical activities, nutrition, interpersonal support, stress management, and spiritual growth. As the health promotion model demonstrated, individuals engage in positive behaviours to promote healthy lifestyles that reduce the risk factors of diseases, thus effectively reducing PD. 30
The current analysis showed that menopausal symptoms were significantly negatively related to health-promoting behaviour, and positively related to PD; this is in line with previous research.18,31 Moreover, we found that menopausal symptoms played a partial mediating role in the relationship between health-promoting behaviour and PD, accounting for 34.8% of the mediating effect. Patients with AET reported almost (but not limited to) 16 symptoms and commonly reported five particular symptoms, including muscle/joint pain, hot flushes, low sexual desire, and muscle/joint stiffness. 32 The incidence of menopausal symptoms, which was as high as 85%, has varied across different studies and depend on many factors such as endocrine medications and measurement tools. 32 Research has demonstrated that a high menopausal symptom burden can cause negative emotions and a poor quality-of-life related to health.18,33 Adopting a healthier lifestyle involves symptom management on the basis of nutrition, physical activity, and stress management; these strategies can help patients to cope with symptom burden, thus reducing negative emotions. 34
In our study, social support also played a partial mediating role in the relationship between health-promoting behaviour and PD, accounting for 27.6% of the mediating effect. Previous studies suggested that perceived social support had a profound effect on physical and mental well-being. 35 A majority of breast cancer patients undertake AET at their own home; this stops them from seeking professional support; therefore, supportive care needs are not met in a timely manner. Information support, emotional support and tangible support play significant roles in health management for this population. 36 Previous studies have demonstrated that high levels of social support from family, friends, and medical providers can be beneficial in increasing healthy behaviours and regulating negative emotions.35,36
Study limitations
There are several limitations that must be considered when interpreting the results from this study. First, participants were recruited from one city of China; therefore, the study population only provides a limited representation of patients with breast cancer. Larger samples across different regions and cultural backgrounds now need to be investigated. Second, the measurement tools used in this study were self-reporting questionnaires; this strategy may have led to subjective information; thus information bias was inevitable. Third, the relationships among the study variables and the mediating factors were identified based on statistical methods and cross‐sectional study design. Therefore, the causal relationships cannot be supported. Moreover, although health-promoting behaviours may help to improve PD via the improvement of menopause symptoms, it is possible that those with more severe menopausal symptoms are not as able to engage in health-promoting behaviours due to their symptom load, thus may have influenced the correlations we identified. Future studies should examine the roles and dimensions of study variables more comprehensively and investigate the effects of other potential confounding factors on PD. A longitudinal study could establish a theoretical model for the development of comprehensive interventions.
Clinical implications
In this study, we detected a high prevalence of PD in patients with breast cancer receiving AET; we also investigated the effect of social support, menopausal symptoms, and health-promoting behaviour on PD. To prevent negative illness-related consequences, patients who suffer from PD should be assessed as soon as possible so that we can identify menopausal symptoms and provide potential interventions. Non-pharmacological interventions are normally used to manage the menopausal symptoms of breast cancer patients. Anderson et al. recommended a multimodal lifestyle program that effectively reduced menopausal symptoms and improved the quality-of-life. 37 Several organizations, such as the American Cancer Society (ACS) and the Chinese Cancer Quality Control Center, have published guidelines on health-promoting lifestyle behaviours for breast cancer patients, including physical activity, diet, weight, and the management of side effects.38,39 In addition, health professionals should make full use of mobile health technology and integrate into health care services to increase health literacy, facilitate healthy lifestyles, and thereby ameliorate negative emotion-related issues. 40
Conclusions
Overall, our analyses identified that health-promoting behaviour had a direct negative influence on PD in patients with breast cancer receiving AET. We also found that menopausal symptoms and social support mediated the relationship between health-promoting behaviour and PD. These findings indicate that PD can be improved in breast cancer patients receiving AET by evaluating patients carefully and by providing interventions to alleviate menopausal symptoms and increase the perceived social support when undergoing health-promoting strategies.
Footnotes
Acknowledgements
We would like to acknowledge the participants who took part in this study for their time.
Contributorship
T-TW, XL contributed to design of the study. T-TW and YZ designed the measurement tool. YZ, H-LR, X-YL collected research data. T-TW, X-YL conducted statistical analysis of the data and interpretation. The first draft of the manuscript was written by XL. T-TWrevised the manuscript. All authors approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research is funded by Tianjin Research Project on Deepening the Reform of the Medical and Health System (2022YG12), Tianjin nursing society Research Project (tjhlky2023QN03), Tianjin Key Medical Discipline (Specialty) Construction Project (TJYXZDXK-011A), Nursing Department Research Project of Tianjin Medical University Cancer Institute and Hospital (TJMUCH-H-2022-04).
Ethics approval
This research was approved by Research Ethics Committee (# Project no. bc2022105).
Guarantor
T-T W.