
Abstract
Background:
Extant research suggests that disparities in healthcare utilization and experiences of mental health disorders such as depression exist across sociodemographic groups. One understudied pathway that may have significant implications for these disparities is the role of family functioning. How families interact, communicate, and adapt may vary, but these relationships remain integral for vulnerable subsets of the population due to their seemingly protective properties. Yet, few studies have examined the relationship between family functioning and health.
Objective:
The aim of this study was to explore family functioning as a predictor for healthcare utilization and depression among young mothers and as a moderator of disparities for each of these outcomes.
Design/methods:
This analysis uses data from a prospective cohort study which was conducted with 296 pregnant young women recruited from obstetrics clinics in Connecticut between July 2007 and February 2011 and followed 1-year postpartum. Logistic regression models were used to assess family functioning, race/ethnicity, and immigrant status as predictors of healthcare utilization and depression. Family functioning was evaluated as a moderator for both outcomes.
Results:
Black and Latina mothers had decreased odds of using physical healthcare services (odds ratioBlack = 0.13, p < 0.001; odds ratioLatina = 0.31, p = 0.02). Family functioning was associated with decreased odds of using mental healthcare services (odds ratio = 0.97, p = 0.04) and had a protective effect against depression (odds ratio = 0.96, p = 0.003). Family functioning significantly moderated the relationship between immigrant status and physical healthcare utilization, Black race/ethnicity and physical healthcare utilization, and Other race/ethnicity and depression.
Conclusion:
Family functioning is a significant factor associated with both healthcare utilization and depression among young mothers. It should be a strongly considered component within healthcare settings to mitigate risks among vulnerable populations.
Introduction
Health disparities research has established that differences in the utilization of healthcare services and experiences of mental health conditions like depression exist across multiple sociodemographic dimensions.1-6 For example, research suggests that women are more likely to utilize healthcare services than men.7,8 However, women experience specific barriers to healthcare that may lead them to forego care, including cost, transportation, lack of time due to work and/or caretaking responsibilitites, and limited access to childcare. 9 Additionally, women are more likely to develop depression during their lifetime compared to men.10-12 While causes for gender differences in depression remain unclear, some research suggests that exposure to adversity and stress, structural gender inequities, and specific psychological traits are some reasons why women experience depression at higher rates than men.10,12
To further understand these findings, behaviors and outcomes should be explored among specific subsets of women. For example, young mothers are an interesting group to consider as there may be unique ways that they navigate healthcare and mental health outcomes, especially after birth. Compounded changes spurred by shifting life stages and experiences such as birth suggest that young mothers are more vulnerable to physical, social, and mental health challenges. 13 It is critical that researchers examine trends in healthcare utilization and depression among young mothers to develop appropriate interventions to combat adverse effects.
Disproportionality in healthcare utilization and depression are also widely noted among racial/ethnic minorities. Black, Hispanic/Latinx, and American Indian and Alaska native individuals, for instance, report lower levels of healthcare utilization compared to non-Hispanic white people 2 for an array of reasons including medical mistrust, 14 poor doctor-patient communication, 15 and being uninsured.2,16 Regarding depression, research suggests that while minoritized populations are less likely to experience acute major depressive episodes compared to white people they are more likely to experience chronic episodes of depression in ways that have severe implications for their daily functioning. 4 Additional studies also highlight that non-Hispanic Asian individuals have the lowest prevalenceof depression compared to other racial/ethnic groups. 17
Continuously, research on healthcare utilization among immigrant populations highlights significant differences between foreign-born and US-born groups with immigrants having lower rates of healthcare utilization compared to native populations.3,18 Moreover, while immigrants on the whole are less likely to experience mental health disorders like depression compared to U.S natives, specific subgroups of immigrant populations (e.g. refugees, immigrants who arrived as children, etc.) have equally high levels of risk or higher risk for experiencing depressive symptoms compared to their US-born counterparts.19-21 The long-standing healthy immigrant paradox, which was first studied among a cohort of Hispanic immigrants from Mexico in 1986, 22 suggests that less-acculturated immigrants outperform native-born populations in domains of health. 23 However, disparities in health outcomes across immigrant populations are still present and require immediate attention especially given current social and political discourse. It is imperative that scholars expand their research to incorporate social concepts that might explain prominent health disparities across sociodemographic dimensions, such as gender, race/ethnicity, and immigrant status.
Thinking critically about racial/ethnic minorities, immigrants, and specific subsets of young women, there are unique social spaces that have not been thoroughly studied within a public health framework. One understudied pathway is the role of family. In operationalizing the concept of family, researchers have used family functioning to measure and evaluate how families interact and communicate. 24 Family functioning refers to the social and structural properties of the family environment, including interactions and relationships within a family, quality of communication, organization, and adaptability.24 –26 Families with healthy family functioning report clear communication, high levels of adaptability, clearly defined roles, and excellent cohesion while families with poor functioning report high levels of conflict, disorganization, and poor affective and behavioral control. Given this, family functioning may have significant implications for mental health and healthcare utilization as families are often considered an embedded social unit that influences how individuals interact with health on an interpersonal, intrapersonal, and structural level. Yet, there remains a dearth of research exploring how family functioning impacts healthcare utilization and mental health disorders, especially within the aforementioned populations.
Understanding the role of family functioning in health could inform research efforts, programming, and policy toward increasing healthcare utilization and improving mental health outcomes especially for vulnerable subpopulations. Therefore, in this paper we use data from a cohort of young mothers to investigate whether race/ethnicity, immigrant status, and family functioning are predictors for healthcare utilization and depression and whether family functioning is a moderator for disparities in these outcomes.
Materials and methods
For our secondary data analysis, we used data from the Parenting and Relationship Transition and Risk Study (PARTNRS).27,28 PARTNRS was a prospective cohort study that took place between July 2007 and February 2011 in Connecticut. The study evaluated the effects of relationships on sexual health, mental health, and pregnancy outcomes at the prenatal period (baseline), 6-month (T2), and 1-year postpartum follow-up (T3). Couples for this study were recruited from obstetrics and gynecology clinics and an ultrasound clinic in four university-affiliated hospitals across the state. All procedures were approved by the Yale Human Investigation Committee and by the Institutional Review Boards of each study clinic (Ethical approval no. 0412027305).
Eligibility to participate in the original prospective cohort study required that women had to be between 14 and 21 years of age, in their second or third trimester of pregnancy at the time of enrollment, and able to speak English or Spanish. It also required that both male and female partners were in a relationship, both members of the couple reported being the biological parents of the unborn baby, and that both parties agreed to participate in the study. Participants were deemed ineligible or excluded from the study if (1) they did not meet the study criteria presented above, (2) they could not be contacted after the initial screening and before their estimated due date, and (3) either member in the relationship was preparing to end the relationship or move from Connecticut. At baseline, consent forms were read to participants and signed in person and then stored in a filing cabinet with participants receiving their own written copy for their records. All individuals, regardless of age, signed informed consent. As is consistent with Connecticut General Statutes 19a-216, 19a-582, 19a-600-602, and 19a-285 which permits adolescents to seek reproductive care (e.g. prenatal care, sexually transmitted disease (STD) screenings, etc.) for themselves and their children without parental consent, the emerging parents were able to provide informed consent to participate in the study. Of 413 eligible couples, 296 were enrolled in the study. 28 More information on the design of and data collection methods used in the prospective cohort study can be found elsewhere. 28
As mentioned above, this secondary analysis is part of a larger study. The power analysis from the larger study was determined on the basis of the primary data analysis strategy (multilevel modeling). Power was assessed on the ability to detect the effect of a single predictor controlling for covariates, on a single outcome. A goal of 80% power was chosen. Preliminary research found effect sizes for key study variables of d = 0.3–0.5. Therefore, using the lower limit of that effect to be conservative, and with power at 0.80 and alpha set to 0.05, the research team needed 240 couples to detect a small/medium effect size of d = 0.3. Assuming a 20% loss to follow-up, 300 couples were needed to attain a final sample size of 240. The original study sample size estimate was calculated using Optimal Design for Multilevel and Longitudinal Research Version 0.23.
Furthermore, in this secondary data analysis, we did not evaluate both partners in the romantic dyad but instead only evaluated the female subset. Thus, our final analytic sample consisted of 296 women. We used data from all time points listed (baseline, 6 months, and 1-year postpartum).
Demographic variables
Demographic information for young women included age, education, income, and relationship status. Age was divided into two groups: < 18 and 18–21 years. Education was categorized into three groups: < 12th grade, high school graduate, and any college. Household income was considered to indicate the 125% federal poverty level in Connecticut (< US$15,000 and ⩾ US$15,000). 29 Relationship status was categorized into two groups: single and formerly married/not single. The formerly married/not-single category included individuals who were married, divorced, or widowed at the time of enrollment.
Independent/predictor variables
Our two primary predictors included race/ethnicity and immigrant status which were taken at baseline. Participants were asked to choose their racial/ethnic group from a provided list which included Black, Latina/o, White, Alaskan, Native American, Asian, Pacific Islander, and Other. Individuals who identified themselves as Asian, Alaskan, Native American, Pacific Islander, and Other made up less than 5% of the sample and as such were grouped together in the Other category. Thus, our final sample of participants was categorized into four groups: non-Hispanic white, non-Hispanic Black, Latina, and Other race/ethnicity. For immigrant status, data on nativity were used to identify those who were immigrants (foreign-born) and those who were non-immigrants (US-born).
Dependent variables
Outcomes included healthcare utilization and depression. Both outcomes were assessed at 1-year postpartum or time 3. General healthcare utilization was assessed by self-report with a 26-item scale created by the study team. This scale measured types of healthcare services used and frequency of visits in the past 3 months. Three different types of healthcare visits were assessed: physical healthcare services (whether participants saw a family practitioner), mental healthcare services (whether participants saw a social worker or mental health professional), and emergency healthcare services (whether participants went to an emergency room or had an overnight stay in the hospital).
Data on depressive symptoms were obtained using the Center for Epidemiologic Studies Depression Scale (CES-D). 30 For each symptom of depression, participants indicated how often they felt or behaved in the specified way with options ranging from “less than 1 day a week” to “most of the time (5–7 days a week).” Following clinical guidelines, individuals reporting a score of 16 or greater were categorized as experiencing moderate depressive symptoms. While other scales, such as the Edinburgh Postnatal Depression Scale, 31 have been intentionally created to assess postpartum depression, the study team decided to use the CES-D because the original prospective cohort study included both men and women and aimed to assess changes in depression during both the prenatal and postnatal period. The CES-D has been used in multiple studies assessing depression in pre- and postpartum women.32,33
Moderator
We evaluated family functioning as a predictor and moderator of healthcare utilization and depression. Family functioning was assessed at 6 months postpartum and was captured using a 12-item shortened scale adapted from the 40-item family functioning scale (FFS). 34 The FFS measures five general dimensions of family functioning: positive family affect, family communication, family conflicts, family worries, and family rituals/supports. Individuals were asked to indicate how accurately statements concerning the five general dimensions described their family on a seven-point Likert-type scale ranging from never [1] to always [7]. Higher scores indicated higher family functioning. The minimum score for the shortened FFS tool is 12 and the maximum score is 84.
Statistical analysis
Data were analyzed using SAS 9.4 software. In analysis, all dependent variables were analyzed using bivariate and multivariate logistic regression. All demographic variables were evaluated as possible covariates at a significance level of α = 0.05. Multivariate models included age, education, income, and relationship status along with primary predictors. For moderation analysis, interaction terms were used to determine significant effects between race/ethnicity and family functioning, and interactions between immigrant status with family functioning. Simple slopes were then calculated to obtain stratum-specific estimates for significant interactions.
Results
Descriptive statistics
Demographic characteristics can be found in Table 1. The majority of the sample was between 18 and 21 years of age (75%), 43.6% did not graduate from high school, approximately 32.1% reported an annual income below US$15,000, and 38.9% were not in a relationship. For race/ethnicity, 39.5% identified as non-Hispanic Black, 39.5% as Latina, 16.9% as non-Hispanic white, and 4.1% as Other. About 11% of the sample were foreign-born/immigrants.
Demographic characteristics of the sample of young mothers (N = 296).

Total may not sum to entire sample due to missing data.
Bivariate analyses
For bivariate analyses (Table 2), both Black (ORBlack = 0.177, 95% CI: 0.073, 0.428, p = 0.0001) and Latina (ORLatina = 0.341, 95% CI: 0.150, 0.778, p = 0.0105) mothers showed significantly decreased odds of using physical healthcare services in the last 3 months at 1-year postpartum compared to non-Hispanic white mothers. Black mothers also reported lower odds of using mental healthcare services in the previous 3 months (ORBlack = 0.211, 95% CI: 0.083, 0.537, p = 0.0011). Young mothers of Other races showed significantly higher odds of using emergency healthcare (OROther_Race = 4.364, 95% CI: 1.080, 17.631, p = 0.0386) compared to non-Hispanic white mothers. For depression, young mothers of Other races reported almost 11 times the odds of experiencing depressive symptoms compared to non-Hispanic white mothers at 1-year postpartum (OROther_Race = 10.665, 95% CI: 2.074, 54.830, p = 0.0046). Higher family functioning was associated with decreased odds of using mental healthcare services (OR = 0.962, 95% CI: 0.937, 0.987, p = 0.0032) and reduced odds of reporting depressive symptoms (OR = 0.961, 95% CI: 0.938, 0.984, p = 0.0012).
Unadjusted associations between healthcare utilization and depression and race/ethnicity, immigrant status, and family functioning. a

Bolded values indicate statistical significance (p < 0.05).
Multivariate analyses
Healthcare utilization
In multivariate analyses (Table 3), healthcare utilization varied by race/ethnicity. Black (ORBlack = 0.128, 95% CI: 0.042, 0.387, p = 0.0003) and Latina (ORLatina = 0.312, 95% CI: 0.117, 0.836, p = 0.0205) mothers reported decreased odds of physical healthcare use. Young Black mothers also reported significant decreased odds for mental healthcare utilization (ORBlack = 0.271, 95% CI: 0.087, 0.839, p = 0.0235). Higher family functioning was significantly associated with decreased odds in mental healthcare utilization (OR = 0.971, 95% CI: 0.944, 0.999, p = 0.0411). Immigrant status was not significantly associated with any healthcare utilization outcomes.
Adjusted main effect models between healthcare utilization and depression, and race/ethnicity, immigrant status, and family functioning. a

All models were adjusted for covariates of age, education, household income, and relationship status. Bolded values indicate statistical significance (p < 0.05).
Depression
In our model including all predictors, higher family functioning was associated with reduced odds of experiencing depressive symptoms (OR = 0.960, 95% CI: 0.935, 0.986, p = 0.0028), showcasing a protective effect among our sample of young mothers. Race/ethnicity and immigrant status were not significant in our main effects for experiencing depressive symptoms.
Moderation analyses
Moderation analysis resulted in three significant interactions. We also calculated stratum-specific estimates using simple effects for each significant interaction (Figure 1(a)–(c)). The first significant effect was between Black race/ethnicity and family functioning for physical healthcare utilization (p = 0.0203), where our simple effects showed that young Black mothers were more likely to use physical healthcare services with increased family functioning.
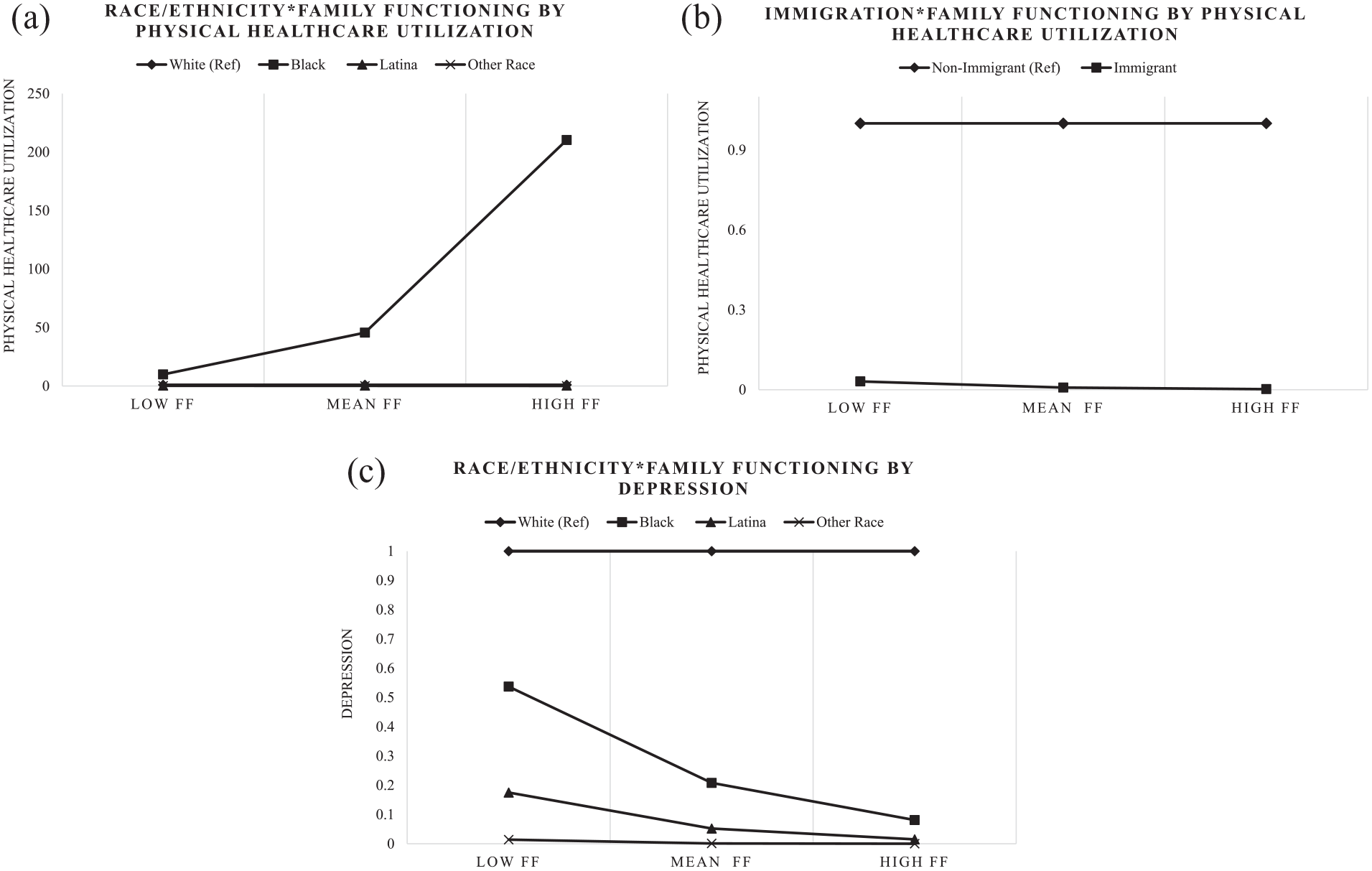
(a) Interaction plot with race/ethnicity × family functioning by physical healthcare utilization. (b) Interaction plot with immigrant identity × family functioning by physical healthcare utilization. (c) Interaction plot with race/ethnicity × family functioning by depression.
In addition, there was a significant interaction between immigrant status and family functioning for physical healthcare utilization (p = 0.0196) with immigrants being less likely to use physical healthcare services with increased family functioning. Finally, there was a significant interaction between Other race/ethnicity and family functioning for depression (p = 0.0428) suggesting that young mothers of Other races were less likely to experience depressive symptoms as family functioning increased.
Discussion
Overall, our study showed that Black and Latina mothers were less likely to use physical healthcare services compared to non-Hispanic white mothers 1-year postpartum. Young Black mothers also utilized mental healthcare services at lower rates than non-Hispanic white mothers. High family functioning showcased significant importance as a protective mechanism against experiencing depressive symptoms and also decreased the likelihood of using mental healthcare services among this cohort of young mothers during the postpartum period. Furthermore, family functioning served as a significant moderator between race/ethnicity, immigration, depression and healthcare utilization.
Our results extend previous findings regarding the limited use of healthcare services by young mothers. This body of research highlights the unique challenges and barriers that young mothers face when accessing healthcare services. For instance, a qualitative study conducted in Uganda uncovered that pregnant adolescents were less likely to use physical health services, in this case maternal health services, due to lack of financial support, difficulty in reaching or transporting to health facilities, and experiencing disrespect from healthcare workers and people in their communities. 35 These barriers and others may continue to plague young mothers even after they give birth. In fact, another study exploring access to mental health services for adolescent mothers suggested that additional barriers such as fear of lack of confidentiality, perceived stigmas around mental disorders and being an adolescent mom, as well as environmental obstacles (i.e. the dangerous location of mental health service providers) led to low levels of engagement with mental health services. 36 Furthermore, decisions to engage or not engage with healthcare may exist beyond individual choice for young mothers. In the context of family, access to care for adolescents is often shaped by how parents and caregivers perceive care.37–39 For example, if a parent has negative perceptions of healthcare systems, they may be less likely to seek care for their adolescent child.
Challenges and barriers to physical and mental healthcare for young mothers may be further exacerbated for those who identify as racial/ethnic minorities. Generally, the existing literature asserts that non-Hispanic Black and Latina populations are less likely to use healthcare services for myriad reasons including institutional and structural barriers (e.g. income inequality, racism, lack of health insurance coverage, and limited employment opportunities),16,40-42 and cultural barriers (e.g. insufficient language services and lack of culturally relevant health information)43-45 which may deter vulnerable populations from using care. Indeed, in a study assessing barriers to prenatal care for emerging young adult Latina mothers, the majority of participants noted that institutional barriers were significant factors that hindered their access to care. 46 For example, some participants indicated that the inability to schedule timely appointments with physicians was a major barrier to accessing prenatal care in the first trimester. Here, the authors suggest that many physicians choose not to accept Medicaid or other types of government assistance, making it difficult for pregnant or parenting adolescent/young adults to receive care. This decision further inundates physicians who do accept all forms of insurance, possibly increasing wait times for patients. Other participants in this study noted that a general mistrust of the healthcare system—a perspective often shared among historically marginalized groups who may experience racism and discrimination in treatment settings47-50—was another significant barrier to care. 46 For Black mothers, in particular, experiences of racial discrimination and other forms of racism in medicine are major risk factors for Black maternal mortality and morbidity which remains a significant public health issue in the United States.51,52
In our study, we also observed that young Black mothers were less likely to use mental healthcare services compared to young non-Hispanic white mothers. Extant research showcases that Black communities harbor negative attitudes and high levels of stigma toward mental health disorders, often associating them with limited intellectual ability, weakness, inferiority, embarrassment and shame.53 –55 Ultimately, these perceptions and beliefs, coupled with the effects of intergenerational trauma, experiences of systemic oppression, and racism may prevent young mothers in Black communities from seeking the care they need. These factors may become compounded for young Black mothers who are also vulnerable to the unique barriers faced by adolescent mothers, generally; some of which are noted above. In addition, studies show that Black communities may seek spiritual advice when addressing mental health problems.53,56 This treatment modality may be used by young Black mothers in place of seeking medical treatment, and can explain why they were less likely to use formal mental healthcare services in our study.
Our results emphasize the importance of family functioning as a protective mechanism against depression. Adolescent mothers experience higher rates of depression compared to their non-pregnant peers and adult mothers, both prenatally and postpartum.57,58 In general, the likelihood of experiencing postpartum depression is driven by multiple risk factors, such as past history of psychiatric disorders, stressful life events, lack of social support, and antenatal depression, anxiety, and emotional problems.59,60 For young mothers, mental health concerns such as depression—during and after pregnancy—may be a result of navigating the ups and downs of adolescence and emerging adulthood and the forthcoming demands of being a parent all within a context of economic strain and social disadvantage. 57 This strain and disadvantage may be particularly salient for historically marginalized young mothers since experiences of and exposure to racism and discrimination in childhood and beyond, 61 as well as limited access to resources, 62 may be higher for these vulnerable communities in ways that increase the likelihood of experiencing depression. From our findings, we theorize that family functioning is a major pathway of social support throughout pregnancy and afterward, and thus reduces experiences of depressive episodes. Generally, some studies have found that high family support and cohesion often act as a buffer to emotional distress and depression.21,63 –65 In the context of young motherhood, families may be able to provide practical support such as running errands and going to the grocery store. They may also provide emotional support, without judgment, for new mothers who struggle after birth. This support may reduce stress for young mothers and in turn decrease the likelihood of experiencing depression and other mental health disorders. Given the adverse effects of postpartum depression on both the mother and their infant’s development,66,67 techniques and programs that aim to boost healthy family dynamics should be assessed as a way to reduce adverse effects.
Continuously, family functioning was also shown to reduce the use of mental healthcare services among our sample of young mothers. Seeking help for mental health problems such as depression is dependent on social influence and individual action. 68 While social influence is dictated by an individual’s vast social network, with research focusing extensively on the role of friends and peers, family remains a constant structure, for some, that may dictate the use of healthcare services. In some instances when family support and cohesion is high, family may serve as an alternative resource or proxy to formal mental healthcare support 69 therefore reducing the likelihood of an individual engaging in mental healthcare services. In cases where family functioning or support is low or rife with conflict, however, family may adversely affect help-seeking behavior through influence on the individual. 70 Here, families may exacerbate feelings of shame regarding help-seeking thus increasing negative stigma around mental disorders, or fail to mention formal mental healthcare services as a treatment option at all. Therefore, integrating tools to increase family functioning within healthcare settings should be strongly considered to increase patient/provider connectivity and utilization.
We further identify family functioning as a significant moderator. As family functioning increases, young Black mothers are more likely to use physical healthcare services. We believe this finding extends previous research on the role of family networks in help-seeking among Black populations. In one study, respondents with large family networks were more likely to use both informal and formal sources of care which suggests that families provide informal support while also increasing access to and use of professional services. 69 Influential family members may also serve as enablers, recommending health services to individuals especially if they have used those services previously and reported positive experiences.70,71 Moreover, our moderation analyses uncovered that higher family functioning was associated with decreased use of physical healthcare services among those who identified as foreign-born or immigrant. As family functioning literature is limited in scope, we can only assume that the notable strong family dynamics presented within immigrant families acts as a substitute for formal care, looking to the concept of alternative care mentioned above. Furthermore, even if immigrant populations want to use physical healthcare services, they may underuse care because of legal or political considerations, such as fear of deportation and being uninsured due to lack of documentation. More research is needed to capture nuances among specific immigrant populations. First-generation, refugees and undocumented immigrants may present different reasons for using or not using services.
Our last interaction suggests that as family functioning increases, young mothers of Other races are less likely to experience depressive symptoms. In general, this finding extends the existing literature on family functioning and depression, discussed above, which asserts that individuals in frequent contact with families with high cohesion and support are less likely to experience depressive episodes. While the association between family functioning and depression is made evident by the existing literature, the explanation for why young mothers of Other races showed significance in this context is opaque. Since our analysis combined multiple racial categories (Asian, Pacific Islander, Native American, Alaskan, and Other) as Other race, the collection of differences across groups could be the reason behind this association. For example, there is a limited body of literature on adolescent mothering within Asian populations with the existing literature highlighting that Asians report some of the lowest percentages of teen pregnancies compared to other racial/ethnic groups. 72 Furthermore, literature assessing cultural beliefs and mental health preferences of ethnically diverse individuals suggests that Asian individuals, when compared to non-Hispanic whites, are less likely to seek mental healthcare services, often preferring to discuss their mental health with family and friends or deal with it on their own. 56 The use of family as a proxy for mental healthcare may decrease the reporting of depressive symptoms among young Asian mothers. Therefore, more research is needed to explicate differences within Asian and other populations. In addition, the small sample size of Other race/ethnicity (N = 12) should be noted when interpreting this result.
Despite the strengths of our study, there are several limitations to consider. First, generalizability is a concern since our sample only includes young women who are pregnant/postpartum, so our results cannot be applied to broader populations of young women throughout various life stages. This also suggests that our analysis of depression and healthcare utilization could be compounded by additional stressors, such as recent pregnancy. Second, all of our measures are self-reported which may increase recall bias that can lead to misestimation of associations. Next, although we did not find significant associations between immigrant status and our outcomes, it is possible that we could not capture explicit distinctions from our data. This analysis does not imply that immigrant status is not an important predictor for utilization or depression, but rather calls for more extensive research to be done within specific populations, such as young mothers who may be foreign-born. Finally, we also want to note that our focus on sociodemographic dimensions, such as race/ethnicity, gender, and immigrant status, while in concert with existing public health literature, is meant to explore the impacts of these socially constructed categories rather than reify them. Through this exploration, we can begin to understand and dismantle rather than reconstitute systems of patriarchy, racism, and heteronormativity.
Conclusion
As the health disparity gap continues to plague marginalized communities, one substantial, yet understudied pathway to consider is the role of family functioning. Our results highlight that race/ethnicity, immigrant status, and family functioning should be considered when examining health outcomes and health decision-making. The future direction of this work should aim to integrate and leverage family functioning into healthcare sectors to improve patient/provider relationships and to mitigate adverse physical and mental health outcomes. Indeed, family interventions have been used in clinical settings to improve communication, coping skills, and health management within families.73 –75 Some of these programs have even been developed and implemented to assess family involvement in adolescent pregnancies and after birth.76,77 These same methods can and should be applied to improve family functioning for young mothers during pregnancy and after. Physicians can work with family therapists to make sure that parents/caregivers, and pregnant and postpartum young mothers are able to work through conflict and set boundaries in a healthy and effective way, especially after birth. In tandem with family counseling, physicians should also connect families and young mothers to social workers who may help facilitate peer groups, access to employment and educational activities, and other tools to increase autonomy and independence. 78 To do so, however, requires more culturally competent and intersectional tools to assess family functioning to fully understand the complex nuances and experiences of specific subsets of the population, including but not limited to immigrant communities of color.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231199039 – Supplemental material for Disparities in healthcare utilization and depression among young mothers: The role of family functioning
Supplemental material, sj-docx-1-whe-10.1177_17455057231199039 for Disparities in healthcare utilization and depression among young mothers: The role of family functioning by Shannon Whittaker, Isabel Martinez and Trace Kershaw in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.