
Abstract
Background:
Lifestyle interventions are effective in reducing cardiovascular disease (CVD) risk, but few target mothers of toddlers and preschool-aged children. Cardiovascular risk factors may emerge or worsen during this life stage due to high child-rearing demands, with the potential to persist long-term. We scoped the literature to synthesize findings and highlight future research opportunities regarding CVD prevention interventions among mothers of young children.
Methods:
We searched PubMed, Scopus, Web of Science, CINAHL, Embase, and APA PsycINFO for 2010–2024 peer-reviewed, English-language articles about CVD risk reduction lifestyle interventions for mothers with young children aged 1–5 years. Due to limited initial results, we broadened this demographic criterion to include mothers with children either <1–5 years (infants to young children) or 1–12 years (young to school-age children).
Results:
Six of 424 studies were eligible for review. Only one study exclusively enrolled mothers with children aged 1–5 years. Three enrolled mothers with children between <1 and 5 years; two enrolled mothers with children between 1 and 12 years. Four interventions were conducted in-person and two via digital formats. All interventions targeted ≥1 cardiovascular health component as defined by Life’s Essential 8, including weight (n = 4), diet (n = 4), physical activity (n = 3), blood pressure (n = 3), blood glucose (n = 2), and blood lipids (n = 2). None addressed nicotine exposure nor sleep. Five studies reported statistically significant results for at least one of their outcomes.
Conclusion:
Very few studies discuss lifestyle interventions for CVD prevention among mothers of young children, highlighting a salient gap and opportunities for additional research in this population.

Introduction
Cardiovascular disease (CVD) is the leading cause of death globally and among women in the United States. 1,2 The prevalence of cardiovascular risk factors, such as diabetes and obesity, is high and rising among non-pregnant reproductive-age women. 3 Diabetes prevalence among reproductive-age women increased from 3.0% in 2009–2010 to 4.1% in 2017–2020, 4 and obesity prevalence increased from 24.6% in 2011 to 27.6% in 2017, with higher prevalence among Black and Hispanic women, thus conferring a higher lifetime risk of CVD and its adverse sequelae. 5 Healthy lifestyle behaviors, as defined by the American Heart Association’s Life’s Essential 8 (formerly Life’s Simple 7), are foundational in maintaining high cardiovascular health throughout the life course and preventing CVD in later life. 6 –8 However, women in their reproductive years, especially those who are mothers, may face unique challenges in maintaining healthy cardiovascular behaviors.
Mothers of young children, particularly mothers of toddlers and preschool-aged children, often face high-intensity, hands-on caregiving. 9 –12 This life stage of caring for young children has been associated with decreased physical activity and lower quality diet for mothers. 13 –15 In addition, some financial support systems for postpartum women, such as Medicaid coverage for those of low socioeconomic status, end at 1-year postpartum, adding financial stressors to an already demanding child-rearing period. 16 Women in this life stage may also have limited awareness of their CVD risk, which clinicians may underrecognize as well, further compounding barriers to optimizing their cardiovascular health. 17,18
Lifestyle interventions have been shown to effectively reduce CVD risk, including among pregnant women and women up to 1-year postpartum. 19 –22 However, CVD risk remains high well past the 1-year postpartum time point. One study showed that mothers with early postpartum weight retention had greater cardiovascular risk factors at 3 and 5 years after delivery than mothers without postpartum weight retention. 23 Additionally, women with adverse pregnancy outcomes have higher long-term CVD risk than those who do not experience adverse pregnancy outcomes. 24 Yet, in a preliminary literature review, we noted a significant paucity of research on lifestyle interventions aimed at reducing CVD risk for mothers beyond the 1-year postpartum period. Compared with mothers of school-aged or older children, mothers of toddlers and preschool-aged children likely face greater demands in caregiving effort and stress, 25 due to the high needs of young children and limited sharing of caregiving responsibilities with schools at this stage, 26 and thus greater strain on their lifestyle behaviors. Given the unique challenges this population faces in maintaining cardiovascular health and the scarcity of targeted research, we conducted a scoping review to systematically synthesize the available literature on lifestyle interventions for CVD risk reduction among mothers with young children. In doing so, we also aimed to highlight knowledge and evidence gaps that may guide future research in this population.
Methods
Search strategy and eligibility criteria
This scoping review was registered in the Open Science Framework, 27 and it was guided by Arksey and O’Malley’s conceptual framework for conducting scoping reviews. 28 We presented these methods in detail in the Supplementary Data. In brief, we searched six electronic databases, PubMed, Scopus, Web of Science, CINAHL, Embase, and APA PsycINFO to identify eligible articles (Supplementary Table S1).
Articles were included in the scoping review if they were peer-reviewed, in English, reported behavioral and lifestyle interventions (randomized controlled trials and nonrandomized interventions), and enrolled mothers of young children, which we conceptualized as 1–5 years old (past the infancy stage but before school-age). When we applied this strict age criterion, however, our initial screening only yielded one article. Hence, we expanded our eligibility criteria to include studies that enrolled mothers with children across a wider age range, provided they still included 1–5-year-old “young” children. Our updated eligibility criteria included studies that enrolled mothers of infants to young children (age <1–5 years) and studies that enrolled mothers of young to school-age children (age 1–12 years). 29 We excluded studies that only enrolled pregnant mothers or mothers of infants (children up to 1 year), as well as studies that only enrolled mothers of school-age and older children (children >5 years). We excluded protocol studies, abstracts, case studies or case reports, and editorials, as they represent works in progress, low level of evidence, or opinion. 30 The time frame for article eligibility was January 1, 2010, to November 25, 2024. We did not predefine the term “mother” and relied on each publication’s definition of mother. Behavioral and lifestyle interventions were defined as those not testing medical or device therapy (Supplementary Table S2).
Data screening and extraction
We screened articles with the updated eligibility criteria using Covidence software in two stages: (1) title and abstract review and (2) full-text review. Two study team members conducted independent screening at both stages of review, with disagreements related to eligibility of articles resolved by a third study team member or by consensus. We extracted data via standardized criteria, which included study population, recruitment methods, intervention type, follow-up period, and results. The screening process followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses—Scoping Review (PRISMA-ScR) guidelines. 31 Because the scoping review examined already published data, the Institutional Review Board did not require human subjects review.
Results
Identification of relevant studies
Our database search identified 424 studies. Of these, 57 were duplicates and were removed. We conducted title and abstract screening of 367 studies, of which 19 were retrieved for full text-screening. Five studies met the inclusion criteria for this scoping review through the database searches. During article preparation, one additional eligible study was identified through supplementary searching and included in the scoping review. The reasons for ineligibility are reported in the PRISMA-ScR flowchart (Fig. 1).
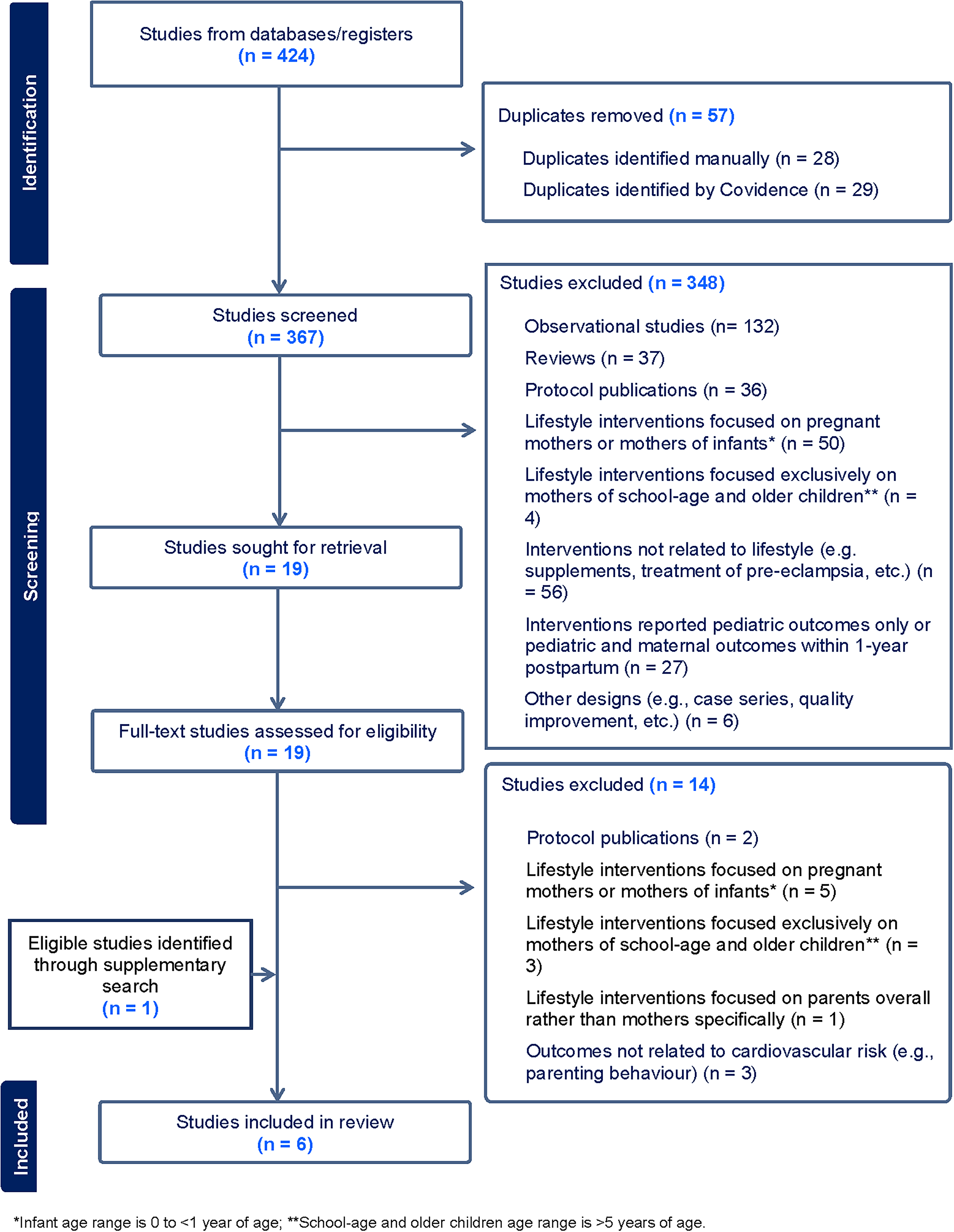
PRISMA-ScR Flowchart. PRISMA-ScR, Preferred Reporting Items for Systematic Reviews and Meta-Analyses—Scoping Review.
Overview of included studies
Of the six studies, two studies were conducted in the United States, two in Australia, one in China, and one in Nepal. Five were randomized controlled trials, of which two were cluster randomized controlled trials and one was a pilot feasibility study. Only one study met our original eligibility criteria of exclusively enrolling mothers of young children aged 1–5 years. Of the remaining studies, three studies enrolled mothers of infants and young children (<1–5 years), and two studies enrolled mothers of young and school-age children (1–12 years). All studies included components of Life’s Essential 8 as cardiovascular risk factor outcomes, including weight, diet, physical activity, blood pressure, blood glucose, or blood lipids (Table 1).
Study Characteristics and Results

RCT, randomized controlled trial.
Recruitment methods
Out of the six studies, three studies described the duration of recruitment, which ranged from 6 months to 21 months. Four of the six studies described their methods for recruiting participants, either within the study itself or through previously published work. 34,37 –39 Of the four studies that described recruitment methods, three studies used multimodal recruitment methods, which included printed materials, radio announcements, in-person announcements and information sessions, letters, telephone calls, and digital advertising (social media or webpage). Only one out of four studies relied on one recruitment method, which was digital advertising (Table 2).
Studies Categorized by Recruitment Methods
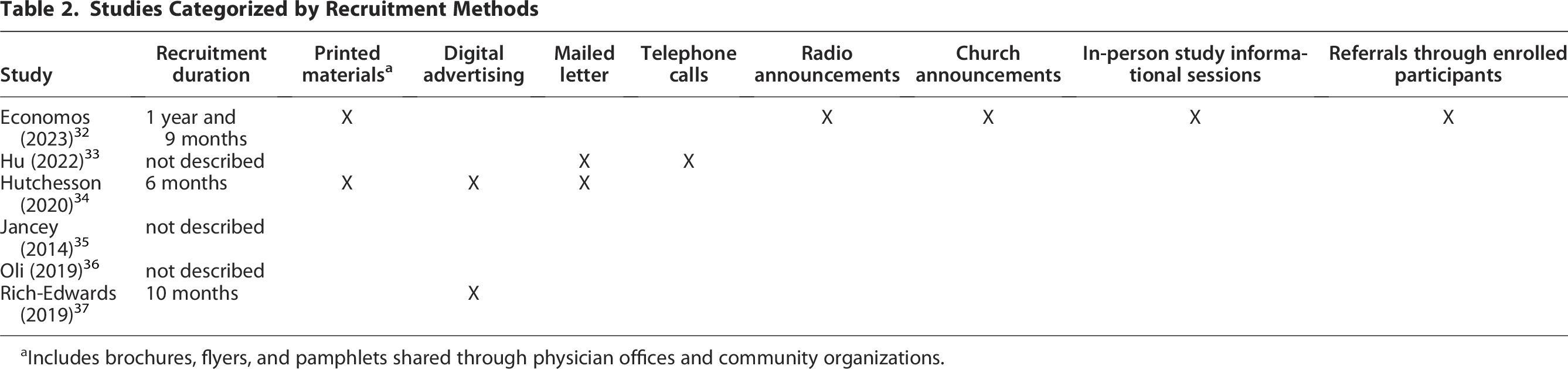
Includes brochures, flyers, and pamphlets shared through physician offices and community organizations.
Design of lifestyle interventions
Four of the six interventions delivered cardiovascular health education in-person, and the other two interventions provided cardiovascular health education primarily through websites. In the Economos et al. study, program coordinators delivered 12 in-person education sessions about cardiovascular health behaviors, as well as conducted five phone calls with each participant to support goal setting and progress tracking, over the course of 1 year. 32 Additionally, a subset of participants in this study was offered six in-person sessions about social and policy issues related to obesity over the course of a second year. Over nine months, dieticians in the Hu et al. study provided five in-person education sessions about diet and physical activity, as well as two telephone calls, to support mothers’ diet and physical activity progress. 33 This was the only study that had a pre-post study design, as well as the only study that conducted follow-up assessments beyond the duration of the intervention. In Jancey et al.’s intervention, university students conducted five in-person group education sessions about diet, in addition to supporting participants in goal setting and progress monitoring, over six months. 35 Oli et al. recruited and trained peer mothers, who then educated participating mothers about cardiovascular health components in group sessions over 3 months, though the frequency of sessions was not specified. 36 Hutchensson et al. and Rich-Edwards et al. both primarily used interactive websites as the intervention modality, which included educational materials about cardiovascular health components, as well as goal-setting and progress-tracking tools. Hutchensson et al. also included a weekly email newsletter about cardiovascular health recommendations and prompts to use the website. 34 Rich-Edwards et al. additionally provided personalized coaching with dieticians through six telephone calls and three emails, as well as an online community support forum for participants. 37 All six interventions included education about diet, and five interventions addressed physical activity. Two interventions included weight education, and one covered stress education. In addition, five interventions provided support in goal setting and progress tracking (Table 3).
Mode of Intervention Delivery and Intervention Topics That Studies Used

Cardiovascular risk factor outcomes
Four studies assessed weight-related outcomes (weight, body mass index [BMI], waist circumference, or body fat percentage), four examined diet, three assessed physical activity, three examined blood pressure, two measured blood glucose, and two measured blood lipids. None of the studies examined avoidance of nicotine nor sleep as outcomes. However, sleep was added to Life’s Essential 8, the updated guidance on cardiovascular health components, in 2022, which was after the intervention periods for the included studies. Three studies investigated additional outcomes, including use of glucose-lowering medications, CVD risk prediction (Framingham 30-year risk score), psychosocial well-being (composite score for depression, anxiety, and stress), self-efficacy with regard to diet and physical activity, feeling informed about CVD risk, and feeling a sense of control over CVD risk (Table 4).
Studies Categorized by Cardiovascular Risk Factor Outcome, with + Indicating a Statistically Significant Result for the Outcome and-Indicating no Statistically Significant Result for the Outcome
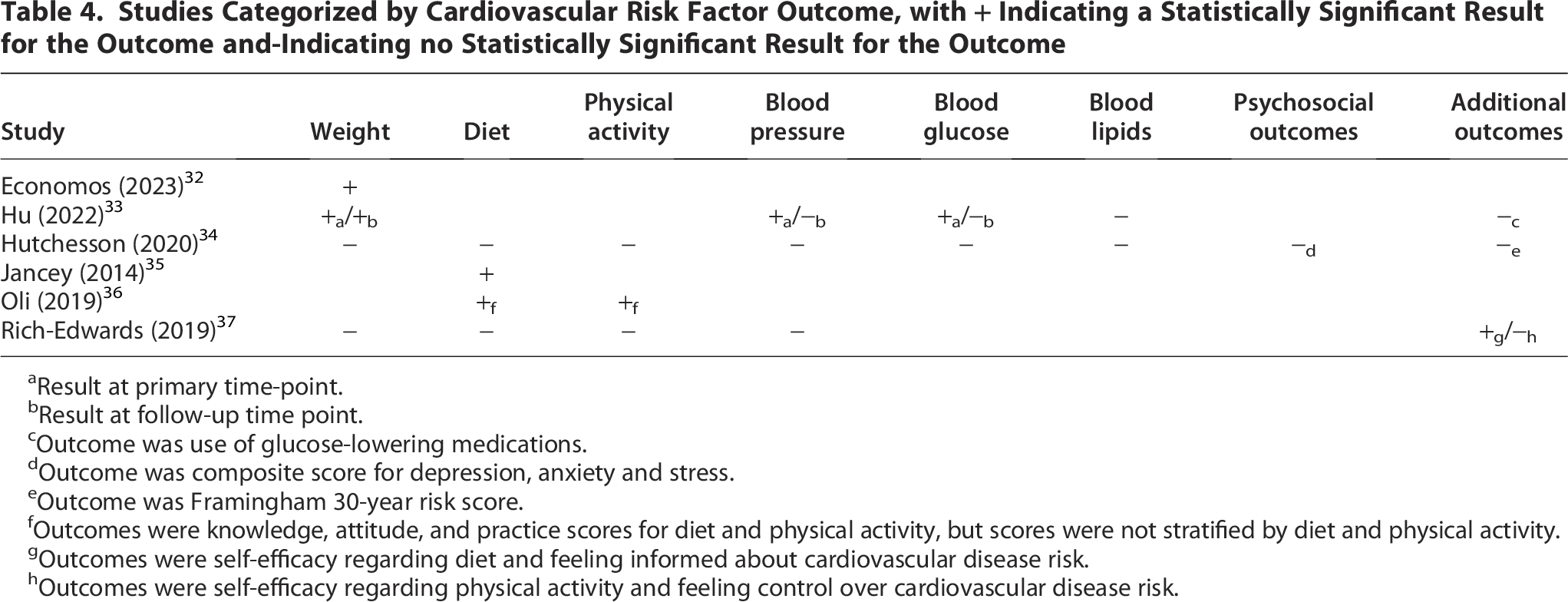
Result at primary time-point.
Result at follow-up time point.
Outcome was use of glucose-lowering medications.
Outcome was composite score for depression, anxiety and stress.
Outcome was Framingham 30-year risk score.
Outcomes were knowledge, attitude, and practice scores for diet and physical activity, but scores were not stratified by diet and physical activity.
Outcomes were self-efficacy regarding diet and feeling informed about cardiovascular disease risk.
Outcomes were self-efficacy regarding physical activity and feeling control over cardiovascular disease risk.
Five out of six studies reported statistically significant results for at least some of their outcomes. Primary time points were at the end of the interventions, which varied between 3 and 24 months. One study followed participants past the primary time point, up to 9 years post-intervention.
Two studies had statistically significant outcomes for BMI, with Economos et al. reporting a reduction in BMI for participants that had full completion of the education sessions compared with those that had partial or no completion (−1.76 kg/m2, 95% CI [−3.14, −0.37]), 32 and Hu et al. describing a reduction in BMI post-intervention compared with pre-intervention (−1.12 kg/m2 ± 1.48, p < 0.001) that was sustained at the follow-up time point. 33 Diastolic blood pressure (−3.49 mmHg ± 9.93, p = 0.009) and fasting blood glucose (−0.98 mmol/L ± 1.80, p < 0.001) were also decreased post-intervention in the Hu et al. study, though not at the follow-up time point. 33
Improved outcomes related to diet were described in three studies. In the Jancey et al. study, the intervention group had higher Fat and Fiber Barometer scores (mean difference 0.12, 95% CI [0.07, 0.16]), which corresponded to healthier habits, as well as increased daily serving intake of fruits (mean difference 0.16, 95% CI [0.01, 0.31]) and vegetables (mean difference 0.35, 95% CI [0.13, 0.56]), compared with the control group. 35 The intervention group in the Oli et al. study had greater increases in scores for diet and physical activity-related knowledge (difference-in-differences estimate 5.8, 95% CI [4.6, 7.0]), attitude (difference-in-differences estimate 6.9, 95% CI [4.5, 9.3]), and practice (difference-in-differences estimate 6.0, 95% CI [5.6, 6.3]) from baseline to post-intervention relative to the control group, though results were not stratified by diet and physical activity. 36 The intervention group in the Rich-Edwards et al. study experienced a greater increase in scores for self-efficacy related to diet from baseline to post-intervention relative to the control group (difference-in-differences estimate 0.2, corrected p-value 0.03, standardized mean difference 0.5). 37 Additional results are presented in Tables 1 and 4.
Discussion
To our knowledge, this is the first review of lifestyle interventions for cardiovascular risk reduction among mothers of young children. Even with a comprehensive search process, we only identified six relevant studies, and only one of these studies enrolled mothers with children strictly between the ages of 1–5 years old. In contrast, our screening process identified 55 lifestyle intervention studies focused on women in the antepartum or 1-year postpartum period. The reasons for the paucity of data focused on mothers with children 1–5 years old are unclear and underexplored. However, some reasons could be less frequent routine health care system engagement after 1-year postpartum, 40 the ending of a variety of social support programs at that time point (e.g., pregnancy-related Medicaid coverage and the Special Supplemental Nutrition Program for Women, Infants, and Children Program), 16,41 or competing time demands. Regardless of the rationale, this dearth of data underscores a missed opportunity for cardiovascular prevention among women in this life stage. In our search process, we identified one protocol publication for a randomized controlled in-person lifestyle intervention for Hispanic mothers with 3–5-year-old children. 42 However, the results of this intervention have not yet been published and therefore did not meet our inclusion criteria. The existence of this registered randomized controlled trial, in addition to the studies we found, highlights the possibility for cardiovascular risk reduction among mothers of young children to be a topic of growing focus among researchers.
Recruitment may present a challenge to engaging mothers of young children in interventions, as they may not be aware of their cardiovascular risks and have competing priorities. 17,18 The studies we found used diverse and multimodal strategies to recruit mothers, collectively and within individual studies. Multimodal recruitment strategies are effective for expanding reach, 43,44 but they are also likely to be costly, time-intensive, and resource-intensive. 45,46 Data on which recruitment strategies are most effective for mothers of young children are sparse. Yet, these data are necessary to identify optimal ways to engage this population and thus promote improved cardiovascular health. Future intervention studies should consider reporting details about their recruitment methods, costs, and effectiveness.
In-person and digital interventions each have their benefits and drawbacks in this population. Mothers with young children may have a high degree of digital literacy, 47,48 and digital interventions can minimize barriers related to time, childcare, and transportation that in-person interventions may present. 49,50 On the other hand, mothers of young children may desire in-person engagement and support, which could also potentially positively impact their cardiovascular health behaviors and risk factors. 51 Previous data on the effectiveness of in-person versus digital interventions in patients with cardiovascular risk factors have been mixed. 52,53 Given the limited number of studies we found in our scoping review, it is difficult to assess the effectiveness of in-person versus digital interventions among mothers of young children. Nonetheless, these existing studies, as well as the potential benefits and drawbacks discussed, may inform the design of future lifestyle interventions among mothers of young children.
Almost all interventions focused on diet and physical activity education, which aligned with their most common outcomes of diet, physical activity, and weight. The lack of interventions and outcomes focused on nicotine may reflect the decreased global prevalence of tobacco use over time, as well as the lower rates of tobacco use among women compared with men. 54 However, electronic cigarettes and vaping have risen in popularity, especially among younger populations. 55 The prevalence of electronic cigarette use and vaping among different population subgroups, as well as their effects on CVD, remain an area of active research. 55,56 Sleep, as an integral component of cardiovascular health, was included in Life’s Essential 8 in 2022, an update from Life’s Simple 7. 6 Given that these interventions took place prior in 2022, it is not unexpected that sleep was not addressed in the intervention education nor assessed in the study outcomes. However, increasing evidence demonstrates that poor sleep, which mothers with young children may be at risk of, 57 is linked to adverse cardiovascular health. 58,59 Only one study examined psychosocial well-being as an outcome, which is recognized as a foundational factor for cardiovascular health in Life’s Essential 8. 6 Future lifestyle interventions may consider incorporating avoidance of nicotine, sleep, and psychosocial health as education targets, as well as evaluating these as cardiovascular risk factor outcomes.
Strengths and limitations
Our scoping review focuses on an understudied population—mothers with young children—whose health behaviors and CVD risks have received limited attention. We conducted the scoping review using a comprehensive search strategy. However, this review also has limitations to consider. Given that scoping reviews do not include quality appraisal, we did not assess study quality in this review. Additionally, it is important to acknowledge that there is broader literature showing that lifestyle interventions can reduce cardiovascular risk factors such as BMI and blood pressure in women, including those of reproductive age. 60 Some of these studies could have included mothers of young children, though their results may not reflect the challenges and barriers faced by mothers of young children specifically, but these studies may not have been captured in our search and scoping review if they did not use terms such as “mothers” in its text or indexing. Furthermore, there are several factors that make it difficult to draw robust conclusions about the effectiveness of lifestyle interventions for CVD risk prevention in our scoping review’s population. There was heterogeneity in study design and outcome reporting, such as the reporting of difference-in-differences estimates vs. mean differences between groups. Few studies reported effect sizes alongside statistical significance, limiting comparability across studies and assessment of clinical significance. Only one study reported outcomes beyond the primary time point, making it difficult to assess the durability of lifestyle intervention effects over time. Lastly, outcomes were limited to cardiovascular risk factors, with no data on long-term CVD or acute cardiovascular events.
Conclusion
Our scoping review of lifestyle interventions for cardiovascular risk prevention among mothers with young children revealed a small number of studies. Existing interventions and outcomes have primarily focused on diet, physical activity, and weight. Further studies are needed to understand which recruitment strategies and lifestyle intervention modalities are most effective for engaging this population. Furthermore, future lifestyle interventions should address a greater range of cardiovascular risk factors to support the cardiovascular health of mothers of young children.
Authors’ Contributions
O.C.L.: Conceptualization, data curation, writing—original draft, writing—review and editing. B.N.: Data curation and writing—review and editing. J.Z.: Writing—review and editing. T.M.S.: Writing—review and editing. M.A.: Conceptualization, data curation, writing—original draft, writing—review and editing, supervision.
Ethical Considerations
There are no human participants in this article, and informed consent is not required.
Footnotes
Acknowledgment
The authors thank Sinia Sareen for her support in this project.
Author Disclosure Statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
M.A.’s salary is partially supported by a NYU CTSA grant [KL2 TR001446] from the National Center for Advancing Translational Sciences, National Institutes of Health.