
Abstract
Objectives:
Moderate-to-vigorous physical activity provides multiple benefits to women after childbirth. To achieve these benefits, the recommendation that adults obtain, 150 min of moderate-to-vigorous physical activity per week and reduce sedentary behaviors, also applies to women in the post-partum phase of the life span. However, research examining the moderate-to-vigorous physical activity and sedentary behaviors of women with young children (0–2 years) is limited. A greater understanding of these behaviors from a nationally representative sample is needed. Therefore, the primary objective of this study was to determine the levels of moderate-to-vigorous physical activity and sedentary behaviors of a nationally representative sample of women with young children within the United States. A secondary objective was to examine the influence of body mass index and sociodemographic factors on these behaviors.
Methods:
Cross-sectional data from four cycles of the National Health and Nutrition Examination Survey (2007–2008, 2009–2010, 2011–2012, and 2013–2014) were used for analysis. Descriptive statistics were calculated and a generalized linear model was used to investigate associations between mean minutes of moderate-to-vigorous physical activity, sedentary activity, body mass index, and sociodemographic variables.
Discussion:
Women with young children (n = 477) obtained 634 min in moderate-to-vigorous physical activity per week and this was positively associated with having a higher income (p < 0.001) and the number of children in the home (p < 0.001). In total, 62% of women were meeting the World Health Organization guidelines for aerobic activity. Lower odds of achieving guidelines was associated with being Black (p = 0.004), Mexican American (p = 0.009), or married (p = 0.042) compared with being White or not married. Finally, women accumulated ~5 h of sedentary activity per day, with higher levels associated with race (p = 0.005), education (p = 0.022), and number of children within the home (p < 0.001). Research efforts should continue to focus on strategies to help non-adhering women with young children achieve the physical activity recommendations and reduce time spent in sedentary behaviors.
Introduction
Physical activity provides multiple benefits to women with young children (0–2 years). Specifically, physical activity in the postpartum period has been associated with physical benefits including a quicker return to pre-pregnancy weight, improved cardiovascular fitness, and reduced lactation-induced bone loss.1–5 Furthermore, physical activity is related to aspects of psychosocial well-being such as lowering levels of anxiety and depression.2,6 This is crucial as about 10% of women experience postpartum depression with ~25% of women continuing to need treatment after 1 year. 6 In addition, as women are often the primary caregivers for young children, their influence on a child’s health behaviors such as physical activity is paramount. 7 Several studies have found that mothers’ physical activity levels are positively related to their child’s physical activity levels.8 –10 Given the increasing prevalence of obesity in the United States, primarily in children, improving the physical activity levels of mothers may be an effective strategy for improving the health of women and children.
Due to the negative impact of sedentary behavior and the high benefits of moderate-to-vigorous physical activity (MVPA), the World Health Organization (WHO) 11 recommends adults obtain at least 150 min of moderate-intensity aerobic activity (e.g. brisk walking, mowing lawn) or 75 min of vigorous-intensity aerobic activity (e.g. jogging, shoveling) or an equivalent combination of MVPA weekly to reduce the risk of chronic diseases. Determining the amount of MVPA and sedentary time women with young children accumulate has been challenging. The limited research that has occurred was conducted in specific geographic areas, utilized different assessment tools, and included light intensity activity when reporting physical activity guidelines making it difficult to compare MVPA outcomes across interventions and across countries.12 –17 As MVPA contributes additional health benefits when compared with light physical activity 6 and there is a lack of consistently reported data, there is a need to assess a nationally representative sample of women with young children to understand their MVPA and sedentary behaviors. Furthermore, a majority of the research in this area has focused on the postpartum period (⩽1 year after birth). Due to the potential impact maternal MVPA and sedentary behavior can have during a critical period of physical development and establishment of behaviors for children during the first 2 years of life, expanding the age range of assessment in women with children 0–2 years of age could better assist clinicians, researchers, and health practitioners in improving the health of women and young children.
In addition, minimal investigation has been done regarding how MVPA and sedentary behaviors may be associated with body mass index (BMI) and sociodemographic factors in women with young children. Previous research in postpartum women has been conflicting. For example, one study suggests factors such as gestational weight gain, race, age, education, and intent to work are significantly associated with more time spent in sedentary behaviors. 14 Conversely, another study found weight was not associated with physical activity during the post-partum period. 17 These studies were also limited to women with children less than 1 year of age. Additional research regarding BMI and other sociodemographic factors that have been found to be associated with MVPA in the general adult population such as marital status are needed. This information from a nationally representative sample can help guide clinicians, researchers, and health practitioners in efforts to effectively promote MVPA and reduce sedentary behavior in this population. Therefore, the primary objective of this study was to determine the levels of MVPA and sedentary behaviors of a nationally representative sample of women with young children within the United States. A secondary objective was to examine BMI and sociodemographic factors that influence these behaviors.
Methods
Study sample
This cross-sectional study utilized data from the National Health and Nutrition Examination Survey (NHANES). NHANES is a national longitudinal survey developed to assess the health of children and adults in the United States. NHANES consists of both an interview-administered survey along with physical examinations and testing in a mobile examination unit to obtain biometric health information. Using a complex, multistage, probability sampling design, NHANES selects 7000 US residents to represent the civilian, noninstitutionalized US population each year. Efforts are made to oversample certain subgroups (e.g. African Americans, Mexican Americans, low income White American) to ensure adequate representation of the US population. As a part of the NHANES data collection process, participants sign a written consent form assuring their responses are completely confidential and identifiable data will not be released without their consent. 18 The NHANES de-identified data set is publicly available. 19 Researchers in this study did not obtain the data through interaction with individuals, and no identifying information is provided, thus this study did not constitute human subjects research and ethical approval was not required (Protection of Human Subjects 46.102.e). 20
For this analysis, four cycles of NHANES (2007–2008, 2009–2010, 2011–2012, and 2013–2014) with independent samples were used to accumulate an appropriate sample size. Additional cycles were unable to be used due to changes in the wording of questions related to physical activity data. Specifically, questions from the demographic, early childhood, physical activity, and weight history questionnaires were utilized as well as physical exam data. We included adult women, 19 years of age and older, with at least one child 0–24 months old. Participants were excluded if they were currently pregnant.
Measures
Physical activity and sedentary behavior were self-reported during the NHANES interview component using the Global Physical Activity Questionnaire (GPAQ). The GPAQ was developed by the WHO to subjectively assess MVPA and sedentary behavior.11,21 The 16-item GPAQ captures MVPA in three domains: activity at work (six questions), travel to and from places (three questions), and recreational activities (sports, fitness, leisure activities; six questions). For example, within the recreational activities domain, “Do you do any vigorous-intensity sports, fitness or recreational (leisure) activities that cause large increases in breathing or heart rate like running for at least 10 minutes continuously?” is asked. If respondents answers yes they complete questions regarding the number of days in a typical week they participate in these activities and the number of hours or minutes they participate in these activities on a typical day. The GPAQ also includes one question regarding sedentary behavior which asks “How much time do you usually spend sitting or reclining on a typical day?”
MVPA behavior was examined by calculating: (1) the mean number of minutes of total MVPA per week as measured by combining the total of moderate-intensity activity and vigorous-intensity activity and (2) proportion of women with adherence to WHO physical activity aerobic recommendations (referred to as WHO recommendations hereafter). Adherence to WHO recommendations was defined as obtaining 150 min of moderate-intensity physical activity, 75 min of vigorous-intensity physical activity, or an equivalent combination corresponding to ⩾600 min of physical activity per week (MET). 21 Sedentary behavior was examined by calculating the mean number of minutes of sedentary behavior (e.g. sitting, traveling, watching television).
BMI and sociodemographic factors
Covariates included race (non-Hispanic White; non-Hispanic Black; Mexican American; other Hispanic; other); education (<9th grade, 9–11th grade, high school, some college, college graduate (or degree)); marital status (married, not married which included widowed, divorced, separated, never married, and living with a partner), age, household size, number of children ⩽5 years of age in household, number of children 6–17 years of age in household, and income-to-poverty ratio. In accordance with other investigations, age (⩾29 years) and income-to-poverty ratio were dichotomized at the median value. 22 BMI was also included and categorized as underweight (BMI < 18.5), normal (BMI 18.5–24.9), overweight (BMI 25–29.9), obese class I (BMI 30–34.9), obese class II (BMI 35–39.9), and obese class III (BMI 40 or greater). 23
Statistical analysis
For each of the four NHANES cycles, the demographics, BMI, MVPA, and sedentary data were merged by respondent sequence number. The resulting merged files were combined. Sampling weights were adjusted to account for multiple cycles. Either mobile examination center or dietary sampling weights were used, dependent upon variables being analyzed. Statistical analyses were performed in R 3.4.2 using the SURVEY package to account for the weighted nature of the data.24,25 Demographics of the sample were reported as frequencies for categorical variables and as mean values with standard error of the mean for continuous variables.
Descriptive statistics of MVPA and sedentary behavior were reported as mean (standard error (SE)), median (interquartile range (IQR)), and frequencies. Mean minutes of MVPA and sedentary activity were compared among the covariates listed above, by fitting a generalized linear model and using the Rao–Scott test to test whether all coefficients of a particular group were zero. Mean (SE) number of minutes of MVPA per week were reported for all subgroups and a p-value was calculated to compare the mean values. In addition, the variable of proportion, which met WHO recommendations was compared among the above-mentioned covariates. Frequencies and p-values are reported, with p-values being calculated for the χ2 test with Rao and Scott adjustment. Using statistically significant and borderline significant (i.e.a-level ≤0.1) predictors from the univariate analysis, a multiple variable logistic regression model was constructed “with meeting WHO recommendations” as the dependent outcome. In total, 95% percent confidence intervals were based on inverting the Rao–Scott likelihood ratio test and p-values calculated using the t-distribution.
Results
A total of 477 women met the inclusion criteria for the study. Women’s average age was 29 years. With regards to ethnicity, the majority of the women were White (57%), followed by Mexican American (14%), and Black (12%). Approximately two-thirds of the sample had a BMI categorized as overweight (31%) or obese (36%). The median income-to-poverty ratio was 1.88 indicating an income 188% above the poverty threshold. Additional demographic details can be found in Table 1.
Sample characteristics (n = 477).

HH: household.
Descriptive statistics were calculated using the weighted sample.
Cycles 2011–2012 and 2013–2014 only, question not included in other cycles.
Indicates that these mothers had a child within the last 0–24 months but the child is not living in the household.
n =447.
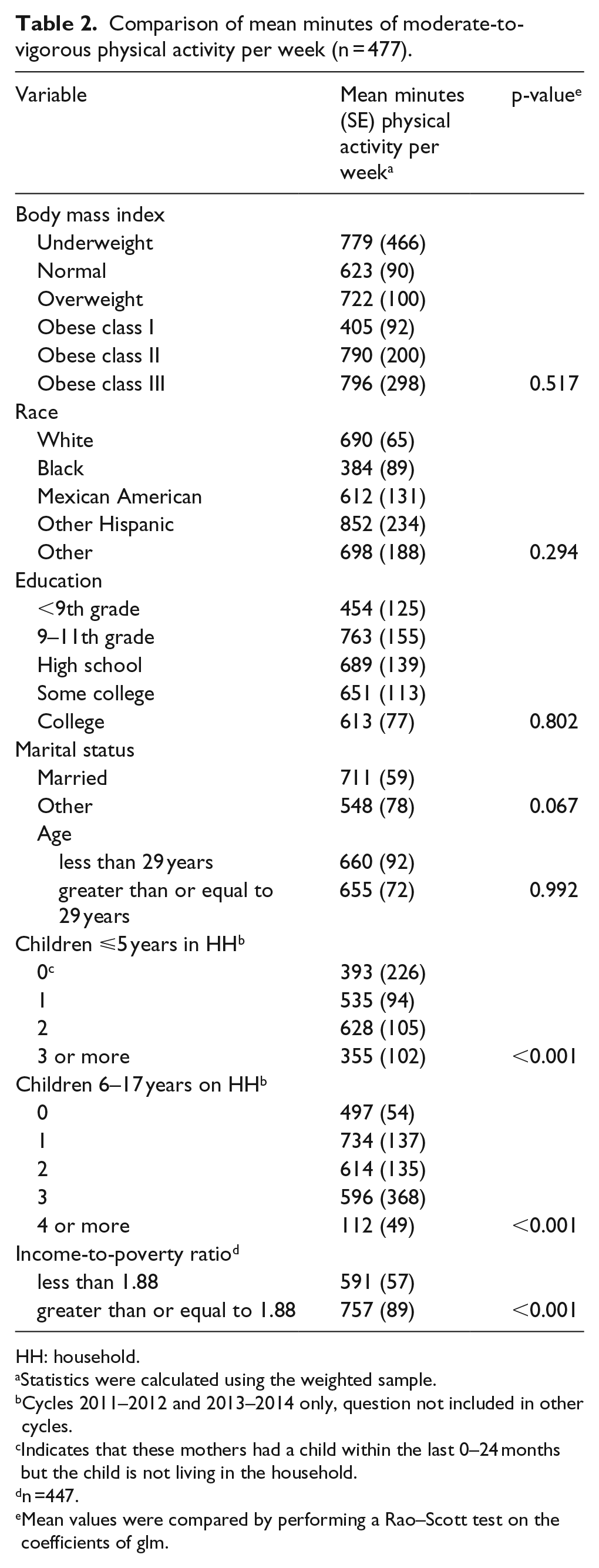
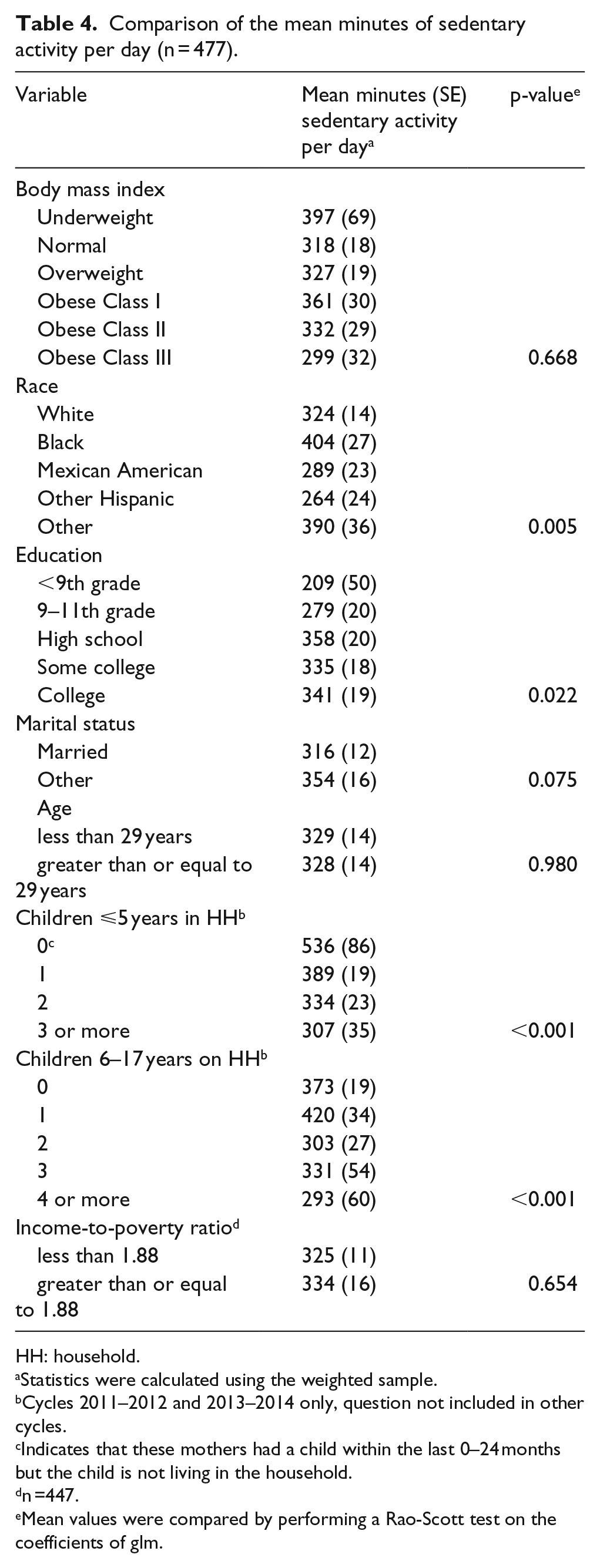
Women reported a mean of 634 min of MVPA per week (Table 2; raw minutes), with a mean of 91 min per day. Approximately 62% of women reported meeting the WHO guidelines for MVPA as defined as obtaining 150 min of moderate-intensity physical activity, 75 min of vigorous-intensity physical activity or an equivalent combination corresponding to ⩾ 600 MET. Women also reported being sedentary for a mean of 328 min per day (raw minutes).
Comparison of mean minutes of moderate-to-vigorous physical activity per week (n = 477).
HH: household.
Statistics were calculated using the weighted sample.
Cycles 2011–2012 and 2013–2014 only, question not included in other cycles.
Indicates that these mothers had a child within the last 0–24 months but the child is not living in the household.
n =447.
Mean values were compared by performing a Rao–Scott test on the coefficients of glm.
When examining if differences existed between the mean number of minutes of MVPA attained per week and BMI, no significant differences were found (Table 2). However, significant differences did exist between mean minutes of MVPA and several sociodemographic variables. Specifically, the amount of MVPA per week was significantly associated with the number of children ⩽5 years in the household (p < 0.001) and the number of children 6–17 years in the household (p < 0.001). In addition, women with a higher income, as measured by the poverty-to-income ratio, reported higher levels of MVPA (p < 0.001).
Similar to the findings regarding MVPA, no significant differences were found between those meeting the WHO guidelines and BMI (Table 3). When examining differences for meeting WHO guidelines and other sociodemographic variables, significant differences were shown for race (p = 0.001). For marital status, a significantly higher proportion of married women (67%) were meeting WHO recommendations in comparison to all other relationship statuses (p = 0.005). Finally, a higher proportion of women above the poverty ratio were found to meet physical activity guidelines (p = 0.071).
Comparison of the percentage of women meeting WHO guidelines for aerobic physical activity (n = 477).

HH: household; WHO: World Health Organization.
Statistics were calculated using the weighted sample.
Cycles 2011–2012 and 2013–2014 only, question not included in other cycles.
Indicates that these mothers had a child within the last 0–24 months but the child is not living in the household.
n =447.
Counts were compared using Chi-square test with Rao and Scott adjustment.
Concerning differences in the number of mean minutes of sedentary activity per day, significant differences were also found based on sociodemographic variables. Again we found significant differences based on race (Table 4, p = 0.005). Education was also significantly positively associated with sedentary minutes (p = 0.022).
Comparison of the mean minutes of sedentary activity per day (n = 477).
HH: household.
Statistics were calculated using the weighted sample.
Cycles 2011–2012 and 2013–2014 only, question not included in other cycles.
Indicates that these mothers had a child within the last 0–24 months but the child is not living in the household.
n =447.
Mean values were compared by performing a Rao-Scott test on the coefficients of glm.
Finally, an additional analysis examined the odds of meeting the WHO recommendations based on the variables that were found to be associated with meeting guidelines (race, marital status, income; Table 5). In regard to race, Black women and Mexican American women had significantly lower odds (p = 0.004 and 0.009, respectively) of meeting guidelines in comparison to White women. In regard to marital status, married women had significantly higher odds of meeting guidelines (p = 0.042) in comparison to not being married. No significant association was found between meeting guidelines and income (p = 0.653).
Factors associated with meeting WHO guidelines by multivariable logistic regression. a

WHO: World Health Organization; CI: confidence interval.
Estimates and inferences are from a weighted sample.
Discussion
This study found women with young children (0–2 years) in the United States reported obtaining 634 min of MVPA per week and variables associated with higher amounts of MVPA included a higher income and having two children, ⩽5 years of age, and/or one child, 6–17 years of age, in the home. In total, 62% of women were meeting the WHO recommendations and variables associated with meeting guidelines included race, marital status, and income. Furthermore, women who were Black or Mexican American and not married had lower odds of achieving the physical activity recommendations. Finally, women accumulated ~5 h of sedentary activity per day; variables associated with increased sedentary behavior included race (Black), education (high school and above), and number of children within the home (fewer).
The mean minutes per week in MVPA (634 min/week) and the proportion of women (62%) meeting the physical activity guidelines was relatively high. This is contrary to other research within the United States. Evenson et al. 16 found that at 3- and 12-months postpartum, women reported ~3 h (180 min) of perceived MVPA each week. However, a study in Australia found a similar percentage (63%) of women 3–4 months postpartum were meeting physical activity guidelines. 26 The proportion of women of childbearing age within the United States who meet the WHO recommendations through recreational aerobic activity ranges from 48.2%–50.6%. 27 Our study may indicate that through an expanded definition of postpartum (0–2 years compared with 0–1 years) and inclusion of additional forms of MVPA, more women within this life stage may be achieving higher amounts of MVPA. It is also important to note that 67% of the sample was overweight or obese. However, while reflective of the US population, this may be misleading since women were within the postpartum period and may not have been at their typical pre-pregnancy weight. 28 Importantly physical activity is known to reduce weight gain and has a plethora of other benefits (e.g. health, mood, quality of life) therefore it is promising that these women are currently active. 6 Future analysis of NHANES data could analyze minutes of activity by type of activity (work vs active transport vs recreational activity) to gain a better understanding of where women are obtaining their MVPA from and/or collect more contextual data to better understand how women are achieving their activity (e.g. playing with children or jogging).
Interestingly, in the Evenson et al. 16 study, objective measurement of physical activity through accelerometers found women at 3- and 12-months postpartum only achieved an average of 119–126 min of MVPA per week indicating a disconnect between women’s perceived levels of activity and actual achieved activity levels of ~60 min. To obtain more accurate levels of MVPA, more objective measures of physical activity are needed. However, subjective assessments should not be discounted as these represent women’s perceived levels of physical activity and their belief in the amount of physical activity they participate in. Thus, if they perceive they are meeting physical activity recommendations, they will be less likely to be interested in physical activity programs and not receive the numerous benefits that physical activity of higher intensities can provide.29,30 Future studies may need to alter recruitment strategies to enroll women who believe they are meeting guidelines. Further, utilizing both types of measures in future interventions could allow researchers and health promotion professionals to better improve the MVPA and sedentary behaviors of women with young children.
Similarly, in regard to sedentary behavior, women in this study were less sedentary than studies from the general population and other studies with women of young children.15,31 Evenson et al. 15 found even higher amounts of sedentary behavior in their population of women 3- and 12-months postpartum at over 9 h of sedentary time per day. Our study indicates that women may be less likely to be sedentary during this extended postpartum time period potentially due to additional caregiving duties associated with small children such as diapering, food preparation, and parent-directed play. However, more research is needed to determine when sedentary time begins to increase and if this is associated with the age of children to identify key time periods for intervention. 32
Interestingly, education was also significantly positively associated with sedentary minutes with women with increasing levels of education reporting higher mean minutes of sedentary activity per day. This aligns with findings by Durham et al. 14 who found in a population of overweight and obese women, women with more education were less active. These results may indicate higher education in women leads to employment in “white-collar professions,” potentially working in an office or other administrative setting that requires more sitting time. 14
Contrary to previous research—which found that being married had a weak negative association with physical activity participation for adults in general or no relationship at all—this study found being married was associated with meeting the WHO recommendations for physical activity.32,33 In support of this finding, a qualitative study with working mothers and fathers found support through the availability of a spouse who could watch the children was a facilitator of physical activity. 34 Thus, future research efforts could explore how to help married women with young children who are not meeting WHO recommendations discuss the need for support with their spouses as well as identify alternative avenues of support for unmarried women with young children.
Other research has found that mothers with a child <6 years of age obtained fewer minutes of MVPA compared to adults without children. 35 Our study found that the amount of MVPA per week was associated with the number of children ⩽5 years in the household, specifically mothers with two children ⩽5 years achieving the highest amount of MVPA and mothers with 3 or more children ⩽5 years achieving the least amount of sedentary time. Thus, the number of children ⩽5 should be taken into consideration when developing future interventions as some mothers may be in more need of physical activity promotion efforts from clinicians, researchers, and health practitioners. Future research should also explore the potential impact of more specific age categories and number of children to determine how to best support mothers’ physical activity.
Several other sociodemographic factors were associated with MVPA in our study, with Black or Mexican American and lower income women at risk for less MVPA. 14 Other research has suggested factors such as age and education to influence postpartum physical activity; however, these factors were not significant in this study. As mentioned above, previous research has suggested that women who work are less active. 14 While this was a variable of interest to the current study, we were not able to include the number of hours worked (which would have been used to determine the influence of work on physical activity) in our analysis since this question had only a 20% response rate. Future research should continue to look at the influence of work on sedentary time and MVPA as well as how it interacts with other health behaviors that are negatively influenced by working, such as breastfeeding.36,37
This study had several limitations. First, the WHO physical activity recommendations also include two or more days of muscle-strengthening activities. 11 The GPAQ does not ask specific questions regarding muscle-strengthening activities and thus the high levels of women meeting the physical activity guidelines is only reflective of those meeting the WHO aerobic recommendations. Second, the analysis used a subjective questionnaire. Previous research has found that subjective assessments tend to over-report physical activity levels potentially due to social desirability. GPAQ has been previously validated but may overestimate activity levels in comparison to accelerometers. 38 However, understanding women’s perceptions of their MVPA and sedentary behaviors is critical in determining how to help them achieve optimal levels of health behaviors. Third, the combination of multiple cycles of NHANES data may have produced weaknesses in generalizing the data. Policy changes such as the gestational weight gain recommendations that were altered in 2009 could have had an influence on women’s behaviors. 39 Finally, although NHANES is designed to obtain a representative sample of the US population, in our cohort the mean income-to-poverty ratio was 2.2. When the family income-to-poverty ratio is greater than 1, the income is higher than the poverty level. Therefore, these results may not be generalizable to all socioeconomic status levels. The major strength of this study was that it was one of the first to examine the MVPA and sedentary behaviors of women with young children in a nationally representative sample in the United States.
Conclusion
Our results indicate over half of women with young children reported meeting WHO recommendations; however, the variables of race, marital status, and income influenced the amount of MVPA obtained. Furthermore, women reported less total time spent in sedentary activities than previous research has shown; however, this also varied significantly by income and education level. These findings suggest the disparities in MVPA and sedentary behavior among women based on sociodemographic variables is a cause for concern. All women must feel they have support and access to engage in physical activity. Future research should continue to determine how clinicians, researchers, and health practitioners can best support women with young children, with particular concern for Black, Mexican American, and low-income populations in their desire and ability to engage in MVPA and reduce sedentary activity to reduce the burden of chronic disease.
Footnotes
Authors’ contributions
D.D. contributed to the design of the study and writing all sections of the text. K.S. and C.H. contributed to the design of the study and assisted in writing sections of the manuscript. N.H. and L.S. contributed to the design and conducted all analyses. M.S., S.M., and P.F. contributed to the design of the study, interpretation of findings, and assistance with the writing. All authors read and approved the final manuscript.
Availability of data and materials
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.