
Abstract
Background:
Postpartum contraceptive use reduces unintended pregnancies and results in better health outcomes for children and women. However, there is a dearth of knowledge on postpartum contraceptive use in Ghana, particularly among women in low-income urban settings. To shed light on strategies that might enhance access to postpartum family planning services in low-income urban settings, we examined contraceptive use among postpartum women in Accra, Ghana, at 1, 3, 6, and 12 months following the birth and the methods used. The predictors of modern contraceptive use in the 12-month postpartum period were also examined.
Methods:
Data come from a cross-sectional survey conducted in 2018 among 624 women aged 16–44 years who reported giving birth in the past 13–31 months prior to the interview. We generated descriptive statistics to examine the prevalence of contraceptive use among postpartum women at 1, 3, 6, and 12 months after birth. We further estimated a binary logistic regression to examine the predictors of modern contraceptive use at 12 months postpartum.
Results:
Forty percent of postpartum women never used any contraceptive method during 1 year after birth and of those who used a method, 40% relied on traditional methods. Moreover, 29% of women started using a method the immediate 1 month post-birth. Results further show that postpartum modern contraceptive uptake was positively associated with higher education, having more live births, and being currently in a union.
Conclusions:
Findings highlight that there may be opportunities to improve the quality of counseling during antenatal and postnatal care visits by clients to ensure fully informed choices regarding postpartum contraception. Community outreach by health providers/promoters or similar models should be promoted in low-income population settings to educate postpartum women on modern contraceptive use. Women who plan to use traditional methods should be provided with information on the consistent and correct use of these methods.
Introduction
The benefits associated with the use of contraceptives are enormous and transcend health to economic and social empowerment of women and households. 1 According to the World Health Organization (WHO), 2 postpartum women have the highest unmet need for contraception. Studies show that about 70% of postpartum women who desire to prevent pregnancy for the next 2 years are not using any contraceptive method.2,3 Contraception uptake within the first 12 months of postpartum can significantly reduce unintended pregnancies and is particularly important because women and children under-five years simultaneously achieve best health outcomes when pregnancy intervals are long.4–9 A minimum of 24 months following live birth is recommended before the next pregnancy, whereas a 6-month period is recommended for the next pregnancy after miscarriage or abortion.6,8 Women who delay the next pregnancy after birth, miscarriage, or abortion have a lower risk of maternal and child mortality, low birth weight, and preterm birth. 8
Certain fertility behaviors potentially increase or reduce the risk of pregnancy during 12 months postpartum period, and these include the use of contraceptives, resumption of sexual activity, breastfeeding, and return of menstruation.4,6 Women who exclusively breastfeed for the first 6 months after birth and are amenorrhoeic are unlikely to become pregnant within the first 6 months postpartum period. 4 However, after 6 months, their risk of becoming pregnant increases with time. 4 Postpartum women who use contraceptives in addition to practicing exclusive breastfeeding without the return of menstruation have extra protection against unintended pregnancy.6,10
In most low- and middle-income countries (LMICs), the use of contraceptives, especially modern methods after birth are generally low. 5 A systematic review of the literature between 1997 and 2018 shows that the overall postpartum modern contraceptive prevalence rate (mCPR) in LMICs is about 41%, with West Africa having the lowest mCPR (36%), whereas South Asia/South East Asia has the highest rate (42%). 5 Likewise, in Ghana, postpartum modern contraceptive uptake is low. Studies in the country reported postpartum modern contraceptive use among women varying between 25% and 26.5% based on the health facility studied and the location of the facility.5,11,12 For instance, the reported postpartum modern contraceptive use for Tema General Hospital and Tema Polyclinic, Accra, in 2018 was 26.3%, whereas 26.5% was reported for a well-baby clinic of Komfo Anokye Teaching Hospital, Kumasi, in 2011.11,12 Some of the factors influencing the use of modern contraceptives by women in Ghana during the postpartum period include prior use of contraceptives before pregnancy, return of menstruation, resumption of sexual activity, and having received maternal health services such as family planning (FP) counseling during antenatal care (ANC). 11
All health facilities, from the basic to the highest level of health service provision, under the Ghana Health Service (GHS) are required to provide comprehensive counseling during antenatal and postnatal visits, including counseling on postpartum contraception and providing women with options of methods to choose from. Other private health facilities are required to provide similar services in Ghana. Though a few postpartum contraceptive use studies have been carried out in Ghana, largely these studies are facility-based.6,11,12 Moreover, Atiglo and Biney 13 who used population-based data (Ghana Demographic and Health Survey) to assess postpartum contraceptive use among unmarried young women in Ghana did not give the context of the low-income urban population. Unlike other urban settings, urban poor women are predisposed to the effects of urbanization such as floods, congestion, and other health hazards, and often have inequitable access to health services.14,15 To shed light on strategies that might enhance access to postpartum services and reduce unintended pregnancies in low-income settings of urban populations in Ghana, we pursued two aims in this study. First, we examined the prevalence of immediate, 1, 3, 6, and 12 months postpartum contraceptive use among women who have had a live birth in Accra and the methods they used. Second, we identified and analyzed the predictors of modern contraceptive use in the 12-month postpartum. The study hypothesizes that socio-economic attributes of women and their use of antenatal and postnatal care (PNC) services affect their modern contraceptive uptake within the 12-month postpartum period.
Methods and materials
Study setting
This article used data from a larger community representative cross-sectional assessment as part of a larger pre-post quasi-experimental study conducted in low-income urban settings of Accra, Ghana. 16 The larger study, referred to as Willows Impact Evaluation (WIE), surveyed women living in two poor neighborhoods of Accra, Ghana.16–18 The first neighborhood, which is in the coastal part of Accra was selected for planned interventions and consisted of La, Teshie, and Nungua communities. These three communities are part of a broader area called OLALE, an acronym for Osu-Klottey, La Dede Kotopon, and Ledzokuku-Krowor areas in the Greater Accra region. The population of OLALE area was estimated to be 533,183 in 2010, with a population density of about 5262 per square kilometer. 19 OLALE mainly consists of indigenous populations (Ga-Dangbe) with a mix of ethnic groups from other parts of the country. The main economic activities of the indigenous ethnic groups are fishing, fish mongering, and petty trading.
The second neighborhood is inland and consisted of Madina, Abogba, and Old Ashongman communities. These three communities are part of the La-Nkwantanang Madina Municipal in the Greater Accra region. The population of the municipal area was estimated to be 111,926 in 2010 with a population density of 3604 per square kilometer. 19 The main economic activities in the La-Nkwantanang Madina area are petty trading and fish mongering. These two low-income neighborhoods (OLALE and La-Nkwantanang Madina) were purposively selected based on similar socioeconomic, demographic and ethnic mix attributes.16–18 Unlike the formal settings of urban cities, the study area is relatively poor and often predisposed to the effects of urbanization such as floods, pollution, congestion, sanitation problems, and outbreak of diseases.14,15 Furthermore, most parts of the study area have temporal structures as dwellings, and as such, the population is fluid. 16 Figure 1 shows the map of the study sites (coastal and inland communities) in Greater Accra, Ghana. The blue is Ghana map, while the red is a map for the Greater Accra region. The yellow circles are the study areas.

A map of Greater Accra, Ghana, with study areas shown in yellow circles.
Sampling procedure
This study is based on the data from a larger project that aimed to assess the impact of the Willows intervention on mCPR in the intervention areas compared to the comparison area. The project was designed to be able to detect an effect size of an increase of 5 percentage points in mCPR in the intervention area when compared to the matched women in the comparison area. The study was powered to test for a statistically significant effect at 0.05 critical value with 90% probability of exceeding the critical value if the actual effect size in the treatment area is at least a 5 percentage point rise in mCPR. This implies a required sample size of 1497 women in each of the two areas. This number was rounded up to a sample of 2000 women in each of the intervention and comparison areas to account for nonresponse.
To obtain a representative sample, the WIE study employed a three-level cluster sampling technique (Figure 2). A cluster in this study refers to a subdivision of an enumeration area that has several structures, houses, and households (defined as a group of persons with common living arrangements and a defined head) in it. At the first level, 200 clusters (100 each for the coastal and inland communities) were randomly sampled from equally divided enumeration area maps of the study communities obtained from the Ghana Statistical Service (GSS). All women in their reproductive ages 16–44 years within the sampled clusters were subsequently listed. A total of 5651 households with women aged 16–44 years were listed from the sampled clusters. At the second level of the sampling, an average of 25 households were randomly sampled from each cluster. The inclusion criterion for the sampled households was for each to have at least one woman within the age range of 16–44 years. At the third level, one eligible woman was randomly sampled and interviewed in the case where the sampled household had more than one eligible woman. A total of 4180 women out of 4323 contacted consented to be part of the WIE and had completed interviews. However, this article used data for 624 women who reported in the contraceptive calendar section of the questionnaire to have given birth in the past 13–31 months prior to the interview.
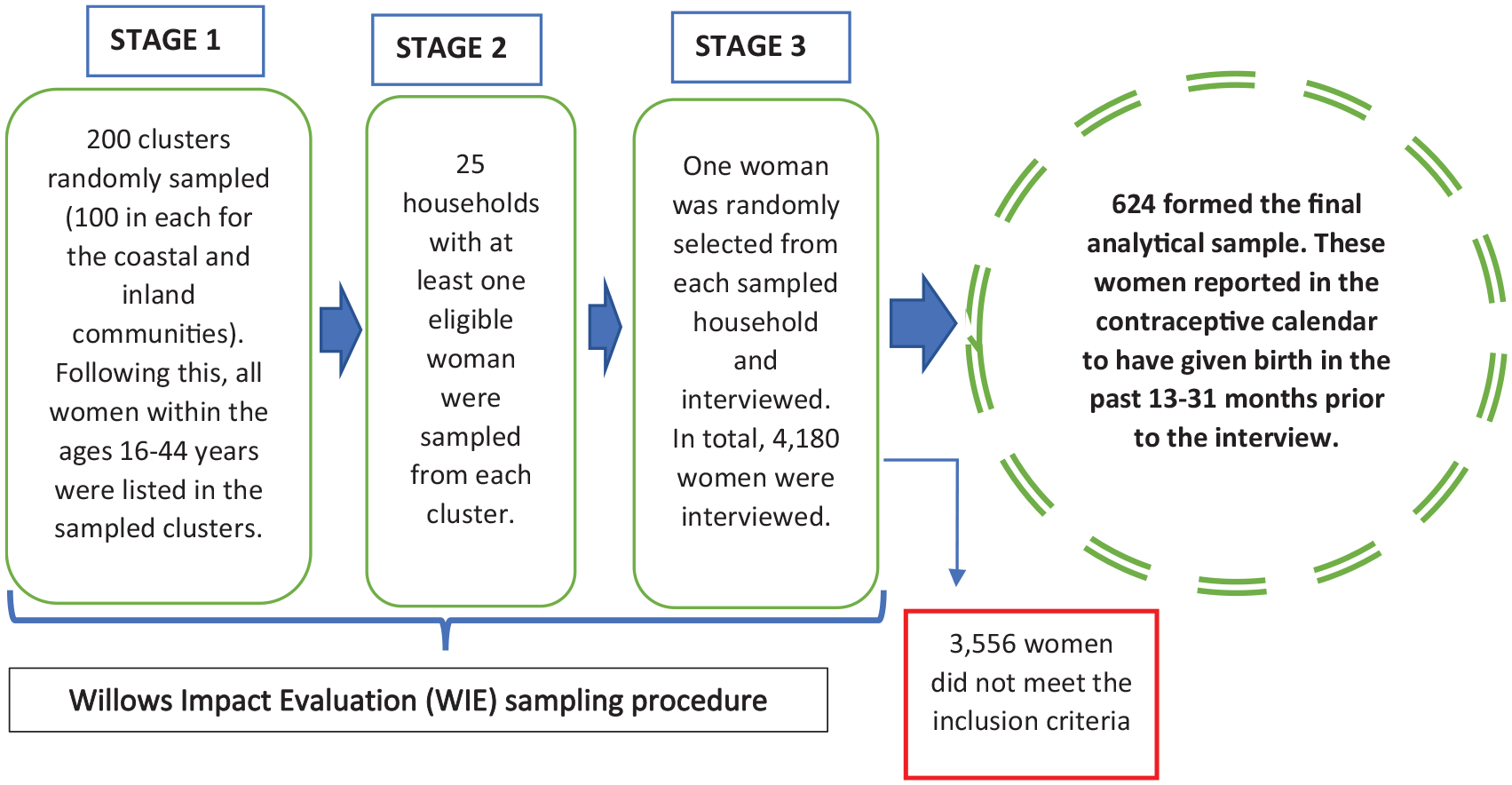
Sampling procedure for obtaining the sample used for analysis.
Data collection
The questionnaire for the larger study was based, for the most part, on Ghana Demographic and Health Survey (GDHS). It was pretested and finalized. Data were collected with the use of electronic devices (tablets) which were programmed with the questionnaire using CommCare software application. 20 Data collection spanned from January to July 2018. Prior to data collection, field enumerators and supervisors were extensively trained for 2 weeks. The data collected include background characteristics and health information of women, including questions on their reproductive health such as contraceptive use, pregnancies, and abortions. All interviews were conducted through a face-to-face interaction between enumerators and participating women in either English or local language.
Measures
The WIE study used a contraceptive calendar like that used in the GDHS to record retrospective information of women regarding their use of contraceptives, discontinuation, reasons for switching and as well as births, pregnancies, and terminations. For this article, data for women who reported in the contraceptive calendar to have had given birth between 13 and 31 months prior to the interview were included for analysis. The postpartum period in this study refers to the 12-month period after birth. Contraceptive methods were broadly categorized into no method, traditional methods, and modern methods. Traditional methods include withdrawal and rhythm. Methods considered modern include sterilization, intrauterine device (IUD), implants, injectables, oral contraceptive pills (OCP), condom, emergency contraceptive (EC) pill, and lactational amenorrhea method (LAM).
Based on the review of other studies on postpartum contraceptive use in sub-Saharan Africa,4,6,11,12 several predictors were selected. Measurement for the selected predictors of postpartum modern contraceptive uptake is as follows: age of woman (16–24, 25–34, and 35 years and above); marital status (never in union, currently in union, and formerly in union); educational level (no formal education, completed primary, completed middle/junior high school, completed secondary and tertiary/higher education); religion (Pentecostal, Catholic, Anglican/Methodist/Presbyterian, other Christians, Muslim, and no religion/other); number of live births (one live birth, two live births, and three live births/more); received FP counseling during ANC (yes and no); ANC provider (nurse and physician); attended PNC after birth (yes and no), and received FP counseling during PNC (yes and no). Having received ANC was dropped from the analysis because of collinearity with counseling during ANC.
Analysis
STATA version 17.0 was used for the analysis. 21 The prevalence of postpartum contraceptive use among women was estimated at 1, 3, 6, and 12 months following birth. A binary logistic regression model was also fitted to examine the predictors of postpartum modern contraceptive use. The binary logistic model was employed to examine associations with the use of a modern method in the 12-month postpartum period: used a modern method in one or more months in the postpartum period versus never using a modern method in the postpartum period. Explanatory variables for the regression with p-values less than 5% were considered statistically significant for the analysis and discussed.
Results
Background characteristics of women
Table 1 shows that the majority (55%) of women are within the age band 25–34 years and more than 79% reported being in a union with a partner at the time of the interview. Except for some (14%), most women had a form of formal education with over a third reporting to have completed secondary education or higher. Furthermore, the majority of women are from the Akan (34%) and Ga/Dangme (33%) ethnic groups and a higher proportion also fall in the poorer (20%) and average (39%) wealth scales. Two-thirds (71%) of postpartum women had reported having two or more live births.
Sociodemographic characteristics of women who delivered between 13 and 31 months before the survey.

The 5-category wealth index was created similar to the DHS approach, using principal components analysis methods on household assets with an urban sample in Ghana.
Maternal health services women received and source of services
Table 2 shows the services women received before and after birth, as well as the providers of the services. Ninety-nine percent of women had reported having had at least one ANC visit before their last birth and of these, about 85% received ANC services at least four times. Eighty percent of women had obtained their recent ANC service from a public hospital/clinic and the providers (96%) were mostly nurses/midwives. Only a few (4%) had received their recent ANC service from a physician. Slightly over three-quarters (77%) of the women had ever received FP counseling during ANC services. Apart from a few (3%) women who delivered at home, the majority (94%) had delivered in either a public (78%) or private (15%) hospital/clinic. Unlike ANC (99%), a relatively lesser percentage of women (93%) had attended PNC after delivery. Further, the majority (87%) of women had received FP counseling during PNC.
Maternal health services women received for the last pregnancy and source of services.

ANC: Antenatal care; FP: Family planning; PNC: postnatal care.
Thirty-seven women had missing information on both ANC and PNC.
Contraceptive methods women used at months 1, 3, and 12 after birth
Table 3 shows the postpartum contraceptive methods women used at months 1, 3, 6, and 12 after birth. About 40% of postpartum women never used any contraceptive method during 12 months after birth. Of the 375 women who had used a traditional or modern contraceptive method during the 12 months postpartum period, 59% had used a modern method with 15% of the methods being long-acting (specifically, implants (10%), IUD (3%) and sterilization (2%)) and 44% being short-acting (specifically, injectables (16%), male condom (11%), LAM (8%), OCP (5%), EC (3%), and other (0.3%). Twenty-nine percent of women used a method in the immediate 1 month after birth. Of these methods users (81 + 97 = 178), 54% used a modern method with 14% of the methods being long-acting and 40% being short-acting contraceptives. Again, of the modern method users (97 women) in month one post-birth, 23% were using LAM. Results further show that the uptake of contraceptives in general increased among all women during the 12-month postpartum period from 29% in the immediate one month to 60% in the 12th month following birth (Figure 3).
Postpartum contraceptive methods used at months 1, 3, 6, and 12 post-birth. a

Methods at the various months are reported methods and do not necessarily reflect their effectiveness for that period.

Percent of women using no method, a traditional method or a modern method, by month since birth.
Factors associated with the uptake of modern contraceptives in postpartum period
Table 4 shows results for both adjusted and unadjusted logistic regression models fitted for the predictors of modern contraception uptake in the 12-month period post-birth. For the unadjusted model, postpartum modern contraceptive use is significantly associated with the number of live births, educational level and postnatal counseling. For instance, postpartum women with a record of only one live birth were less likely to use a modern method compared with those with three or more live births (odds ratio (OR) = 0.6, p < 0.05). Also, women who reported that they had not received FP counseling during the postpartum period had lower odds of using a modern method relative to their counterparts who had received FP counseling (OR = 0.6, p < 0.05). Postpartum women with tertiary education or higher were 2.3 times as likely to use modern contraceptives compared with those with no formal education. Even after adjusting for other factors, women with tertiary education or higher were 2.9 times as likely to use a modern method compared with those with no formal education. However, after accounting for other factors, postnatal FP counseling did not significantly predict postpartum modern contraceptive use. The adjusted model further shows that women formerly in a union with a partner were less likely to use a modern contraceptive during the postpartum period compared with those currently in a union (OR = 0.3, p < 0.05). Like the unadjusted, results for the adjusted model shows that postpartum women with just one live birth are less likely to use a modern contraceptive during the postpartum period. Furthermore, results from the adjusted model show that women of higher age had lower odds of using modern methods in the postpartum period. The religion of the woman, whether the woman received FP counseling during ANC or not, the type of ANC provider and whether the woman attended PNC after birth were not significantly predicting postpartum modern contraceptive uptake. Having received ANC or otherwise was dropped from the regression analysis because of collinearity. STATA, the software used for this analysis, automatically dropped ANC attendance because it was greatly correlated with receiving FP counseling during ANC.
Predictors of modern contraceptive use in postpartum period.

ANC: Antenatal care; FP: Family planning; OR: Odd ratio; PNC: Postnatal care; Ref: Reference category; UOR: Unadjusted odd ratio; .
Adjusted odd ratios: Observations = 585, LR Chi2 (18) = 43.04, Prob > Chi2 = 0.00.
NB: Having received ANC or otherwise was dropped from the model because of collinearity.
Seven women who reported had not received ANC are included.
Seven women who reported had not received PNC are included.
Discussion
Generally, the study found that two in five postpartum women were not using any form of contraceptive during the 1-year postpartum period and were at risk of unintended pregnancy and likely to be lopped off from the health benefits associated with postpartum contraception uptake. A systematic review on postpartum contraceptive use among women in low- and middle-income countries reported a similar finding of low postpartum contraception uptake among those residing in urban settings, though not specific to the poor urban communities. 5 Moreover, among the women who used any method during the 12-month postpartum period, about 40% had used a traditional method, even with high utilization of maternal and child health services such as attendance of ANC, PNC, and receiving FP counseling. Traditional methods are often associated with high failure rates,22–24 and thus, traditional method users are also at risk of unintended pregnancy though less than nonusers of any method. Studies have suggested that the reasons for the prevalent use of traditional methods and nonuse of FP methods in most LMICs, as well as in the urban poor context include incomplete counseling by health providers during FP counseling sessions, fear of side effects, myths, and misconceptions about contraception and partners’ restrictions.5,11,25,26
Furthermore, less than a third of women initiated the use of contraceptives in the immediate 1 month following birth. Studies show that about 52% of women often resume sex 5 to 6 weeks following birth and 90% would have resumed sexual activity by the third month after birth.27–29 With this, some of the remaining two-thirds of women who had not used any method in the first month after birth might get pregnant. Our findings further show that only a few of the women who used a modern method in month 1 post-birth had used a long-acting contraceptive. Though the fertility intentions of women were not ascertained in this study, the use of long-acting methods generally enables women to effectively achieve best health outcomes in the postpartum period through long pregnancy intervals. 30
On postpartum method mix, it is observed that rhythm (17%) was predominantly used by postpartum women and followed by injectables (10%). The use of rhythm/calendar method is largely based on one’s knowledge of the menstrual cycle, especially the last menstruation. 31 As such, women’s use of rhythm is an indication that their menses had probably returned. Biologically, ovulation precedes menstruation and most of the women who reported using rhythm in the first month post-birth could potentially be fertile even before the method was used. The use of injectables by nearly a third (28%) of modern method users is not surprising as this is consistent with a recent study conducted in the urban settings of Ghana. Coomson and Manu 11 studied postpartum women who visited health facilities in Tema, an urban city in Ghana and indicated that close to 30% of women who reported using modern methods had used injectables. Also, a facility-based study in Sunyani, an urban area in Ghana, showed that most women who covertly used contraceptives preferred injectables. 32 Similar to findings of Coomson and Manu, less than a tenth of postpartum method users had used LAM. Seven women had opted for sterilization. It is most likely that these women had achieved their desired number of children as further analysis (not reported here) showed that they all had three or more live births and are in their mid-30s or above. A few women (3%) using pills may possibly be attributed to side effect concerns on breast milk and for the newborn, though evidence of combined oral contraceptive pills on breastfeeding is inconsistent. 33
Regarding the predictors of postpartum modern contraception, results indicate that younger women, those with more live births, currently in union and those having a higher educational level are more inclined to have used a modern method during the postpartum period. Women with higher education are expected to have better insights into the various contraceptive methods and would opt for more effective methods. Analysis of DHS data from 43 developing countries including Ghana showed that higher education is positively related to uptake of postpartum FP methods, 34 corroborating our findings. In addition, most women with more live births are likely to have achieved or probably surpassed their fertility intentions and would, therefore, use modern methods that are effective for preventing unintended pregnancies. Findings also suggest that postpartum women currently in a union with a partner are inclined to use modern contraceptives relative to those formerly in union. Women currently in union are more likely to be sexually active and therefore exposed to the risk of pregnancy than women who were formerly in union. Further findings suggest that younger women aged 24 years or less are more likely to use modern methods during the postpartum period. Most younger women are exposed to information on contraceptive methods from various sources, including social media, and this could have contributed to their choice of modern methods. In fact, this finding is not peculiar to our study. A previous study showed that younger women are inclined to opt for long-acting modern methods, though from a high-resource setting. 35
The use of maternal health services, particularly ANC and PNC visits, was not significantly related to postpartum modern contraceptive uptake. In Ghana, ANC and PNC models in both public and private health facilities are designed to include counseling on FP. During ANC visits, pregnant women are expected to receive counseling on a broad mix of FP methods, advantages and disadvantages of each method, and how to correctly use the methods. Postpartum women are also expected to undergo a similar counseling section during one of the PNC visits, often on the first visit which is 1 week following birth. Contraception methods such as depo injection, insertion of implants and IUDs are expected to be readily available and offered to women who prefer to immediately start with any of the methods after the counseling. Our findings, however, indicate that either the content and/or the process of such counseling were weak and require improvements. Such counseling may have overlooked the importance of postpartum contraception for maternal and child health, number of contraceptive methods available, and their relative advantages and disadvantages, or the counseling may have been brief.
Though ANC and PNC were not significantly related to postpartum modern contraceptive uptake, utilization of these maternal health services was generally high. For instance, about 93% of postpartum women had visited a health facility for PNC. In recent times, poor urban communities have received a lot of attention and health interventions in Ghana, including education programs from different health stakeholders. One such intervention implemented in the study area and other parts of Accra before the WIE survey was the Reducing Maternal Morbidity and Mortality (R3M) program. 36 This may have partly contributed to the high PNC attendance in the study area.
Strengths and limitations
This study is not free of limitations. The main limitation is the potential recall bias. The study relied on a contraceptive calendar for analysis. The calendar collected retrospective information from women regarding their use of contraceptives for up to 31 months before the interview. Recalling past events for more than a month and providing accurate information may be challenging. However, our enumerators were well-trained to aid respondents in recalling their past contraceptive behavior. Major reproductive events such as pregnancies, terminations, miscarriages and births were useful in aiding women’s recall of previous contraception. Another limitation of this study is that women’s fertility intentions were unknown, limiting expanded discussion on their choice of contraceptive methods during the twelve months postpartum period. Future work in this area should consider prospective studies where women’s fertility intentions are determined.
Conclusion
In conclusion, findings indicate that 40% of postpartum women never used any contraceptive method during 1 year after birth and of those who used a method, 40% had used traditional methods. Moreover, a much smaller proportion of women started using a method in the immediate 1-month post-birth. Results further indicate that postpartum modern contraceptive use is positively associated with higher education, having more live births and being currently in a union. The outcomes of the study suggest that most postpartum women in low-income urban settings are at risk of unintended pregnancy and likely to be lopped off from the health benefits associated with optimal birth spacing. Community outreach by health providers/promoters or similar models should be promoted in low-income population settings to educate postpartum women on modern contraceptive use.
Supplemental Material
sj-docx-1-whe-10.1177_17455057221141290 – Supplemental material for Postpartum contraceptive initiation and use: Evidence from Accra, Ghana
Supplemental material, sj-docx-1-whe-10.1177_17455057221141290 for Postpartum contraceptive initiation and use: Evidence from Accra, Ghana by Caesar Agula, Elizabeth G Henry, Patrick O Asuming, Akua Obeng-Dwamena, Theophilus Toprah, Martin Wiredu Agyekum, Iqbal Shah and Ayaga A Bawah in Women’s Health
Footnotes
Acknowledgements
We acknowledge the administrative support from the Regional Institute for Population Studies, University of Ghana and Department of Global Health and Population, Harvard T.H. Chan School of Public Health. We also acknowledge the contributions of all field workers.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.