
Abstract
The objective of this article is to review clinical differences between men and women with bipolar disorder. The secondary objective is to analyze the differences in adherence to medication between genders. Men usually present with manic episodes and have comorbid drug abuse, while women usually present with major depressive episode, the onset is often later, comorbidity of physical pathology is common and adherence to medication is greater than in men. In women who have an earlier onset of the illness and are single, the risk of nonadherence is higher than in other groups of women. There are two time periods that are very important in women: pregnancy and postpartum. Both are critical periods and a relapse or recurrence of symptoms at either stage can have serious consequences for the woman and/or her baby. In addition, the effect of medication on the fetus is unclear. In conclusion, there is a clear need for more studies on gender differences in bipolar disorder and how to improve adherence to treatment. Moreover, a better understanding of how to treat women with bipolar disorder during pregnancy and lactation will undoubtedly lead to improved outcomes for both the mother and her child.
 Medscape: Continuing Medical Education Online
Medscape: Continuing Medical Education Online
This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of Medscape, LLC and Future Medicine Ltd. Medscape, LLC is accredited by the ACCME to provide continuing medical education for physicians.
Medscape, LLC designates this Journal-based CME activity for a maximum of
All other clinicians completing this activity will be issued a certificate of participation. To participate in this journal CME activity: (1) review the learning objectives and author disclosures; (2) study the education content; (3) take the post-test with a 70% minimum passing score and complete the evaluation at www.medscape.org/journal/wh; (4) view/print certificate.
Learning objectives
Upon completion of this activity, participants should be able to:
Evaluate the epidemiology of bipolar disorder among women
Compare the characteristics of bipolar disorder between women and men
Assess the safety of drugs for bipolar disorder during pregnancy
Analyze the use of drugs for bipolar disorder during breastfeeding
Charles P Vega, Associate Professor; Residency Director, Department of Family Medicine, University of California, Irvine, USA.
Disclosure: Charles P Vega has disclosed no relevant financial relationships.
Authors and Disclosures
What is bipolar disorder?
Bipolar disorder is a serious mental disorder that causes extreme changes in mood, energy and functioning. It affects approximately 1.3% of the population, and men and women are equally likely to develop the illness. Bipolar disorder usually appears in adolescence or early adulthood, but can emerge in childhood or onset later in adulthood. Life with bipolar disorder is problematic because it affects family and social relationships, employment and the general quality of life of the affected person.
The clinical course of bipolar disorder is characterized by the occurrence of one or more manic or mixed episodes. Often individuals also have recurrent episodes of major depression. Manic episodes are periods of abnormally and persistently elevated, irritable or expansive mood during which the person may have the following symptoms: inflated self-esteem or grandiosity; flight of ideas or subjective experience of racing thoughts; decreased need for sleep; feels more talkative than usual or feels pressure to keep talking; distractibility; psychomotor agitation; or excessive involvement in pleasurable activities that can be the cause of painful consequences [1]. The most important symptoms associated with major depressive episodes are the presence of depressed mood most of the day, significant weight loss (when not dieting) or weight gain, insomnia or hypersomnia, fatigue or loss of energy, markedly diminished interest or pleasure in (almost) all activities, psychomotor agitation or retardation, feelings of worthlessness or excessive or inappropriate guilt, diminished ability to think or concentrate, or indecisiveness, and recurrent thoughts of death [1]. Usually, a person with bipolar disorder only has some of these symptoms.
There are two types of diagnosis: bipolar I disorder and bipolar II disorder. Bipolar I disorder is characterized by recurrent episodes of mania and depression, while bipolar II disorder is defined as recurrent episodes of depression and hypomania [1].
Studies have investigated many different aspects of bipolar disorder, including diagnosis, substance abuse, suicide attempts, mixed states and rapid cycling [2–5]. It is important to study prognostic factors, especially those that can be modified to improve prognosis and adherence to treatment. The objective of this article is to review clinical differences between men and women with bipolar disorder and to analyze the differences in adherence to medication between genders. We performed an electronic literature search of the PubMed® database and an OvidSP metasearch of the following specific databases: Excerpta Medica Database (EMBASE®), Ovid MEDLINE®, PubMed and PsycINFO®. We searched for articles published from the first available year to August 2011 using the following search terms: bipolar disorder AND gender differences, bipolar disorder AND pregnancy, bipolar disorder AND delivery OR postpartum OR breast feeding OR lactation.
Two independent investigators (first and second authors) screened the titles and abstracts of all publications and excluded those articles that were not relevant for the research question; for example, those that referred to a different population (patients or diagnosis) or outcome variables.
Gender differences in bipolar disorder
Bipolar I disorder has equal prevalence in men and women, whereas many studies have shown that there are more women than men with bipolar II disorder [6–8]. Traditional epidemiologic studies give prevalence rates of 0.4–1.6% for bipolar I disorder and 0.5–1.9% for bipolar II disorder [1]. Other studies indicate that the prevalence of bipolar disorder II is even higher in the general population and, when the spectrum of bipolarity is extended to bipolar disorder in general, the affected population is about 5% [9].
The clinical features, phenomena and evolution of bipolar disorder differ between men and women, especially the course of illness, perception of quality of life and psychosocial functioning of patients. Manic episodes are more common in men and depressive episodes occur more frequently in women [10]. Existing evidence suggests that men usually present with manic episodes whereas women tend to present with major depressive episodes [11,12]. Moreover, the onset of the bipolar disorder is often later in women than in men [13]. Women have a higher probability of experiencing mixed episodes compared with men [14], and are more likely to experience seasonal episodes and rapid cycling [13]. In addition, women with bipolar disorder have greater comorbidity of physical pathology, particularly thyroid diseases [13]. Comorbid drug abuse is more common in men with bipolar disorder, whereas women with bipolar disorder tend to have more comorbid eating disorders [11] and anxiety disorders [13], although these latter associations with the female sex remain to be confirmed.
Treatment of bipolar disorder
Medications for the treatment of bipolar disorder include lithium, anticonvulsants and atypical antipsychotics, which are used both for acute episodes and for long-term maintenance treatment [15]. These drugs are often combined with benzodiazepines when there are coexisting symptoms of anxiety or insomnia [16]. The most commonly used atypical antipsychotics are aripiprazole, clozapine, olanzapine, risperidone, quetiapine and ziprasidone [15,17]. Valproate, carbamazepine and lamotrigine are the most widely used mood stabilizers, and are all anticonvulsants [18,19].
The treatment of bipolar disorder is complex and must be individualized for each person. Treatment of women with bipolar disorder is complicated by the need to consider the potential for pregnancy. The drugs mentioned above all interact with oral contraceptives and increase risk of endocrine pathology (hypothyroidism) [20].
Adherence to treatment
Adherence to medications for the treatment of bipolar disorder has been a topic of interest in recent years as a potentially modifiable factor for improving patient outcomes. Good medication adherence is necessary to prevent recurrence of affective episodes, which are associated with cumulative increases in morbidity risks, treatment nonresponse, full syndromal recurrence and suicide [4,21–23]. Factors affecting the ability of a person with bipolar disorder to take their medication as prescribed or to understand other treatments include absence of insight, rapidly fluctuating moods and the long-term nature of living with mood instability [24]. Nonadherence to medication in bipolar disorder is estimated to range from 12 to 64%, and studies with longer follow-up intervals have higher rates of nonadherence [25,26]. Lithium, the gold standard treatment in bipolar disorder, has a high rate of discontinuation and short-term prescription; in a 6-year follow-up study, the median adherence time was only 76 days [27].
Numerous studies have identified specific factors associated with treatment nonadherence in bipolar disorder, including younger age at onset, male sex, a lower level of education, being single, comorbid abuse of alcohol or drugs and excess affective morbidity [28]. Although men have been described as being less adherent than women [29], there are no specific studies of bipolar disorder patients showing gender differences in adherence to treatment.
Gender differences in adherence to treatment & factors associated with nonadherence
Rates of nonadherence are high among patients with bipolar disorder. In a US study, the reported rate of major medication defaulting in the past was 32.9%, the rate of missing recent single doses was 33.8%, and there were many cases of previous and current nonadherence [24].
Factors identified as being associated with treatment nonadherence in bipolar disorder populations include comorbid abuse of alcohol and drugs, marital status, hospitalization, suicide attempts, age at disease onset, family history, health status, functional level, residual cognitive dysfunction, lower level of education and gender [29–32].
Substance abuse is associated with nonadherence and is more common in men than women [29]. Among patients with bipolar disorder, the rates of alcohol consumption and other substances are 38 and 25%, respectively [29].
Another factor related to treatment nonadherence in bipolar disorder is the subjective experience of illness [33]. Some researchers have shown that a good illness experience can be a major and effective motivator for patients to adhere to their treatment plan, whereas a poor subjective experience of illness often leads to lowered treatment adherence. Experience of illness is multifactorial and includes the level of social support, experience of positive or negative medications effects, and perceived stigma. Past research has found gender differences in these factors: women are concerned about weight gain, possible negative side effects of medication and want more social support than men [33–35]. Kriegshauser et al. did not find any differences between men and women in self-stigmatizing attitudes, perception of stigma and in perceived weight gain [33]. However, they did find that women had more concern than men about weight gain and perceived higher quality relationships than men. The data for substance abuse revealed that men with bipolar disorder are more likely than women to abuse alcohol, but there are no gender differences in the rates of drug abuse and in reports of lessened irritability and/or impulsivity due to psychiatric medications [33].
Spanish study of gender differences in adherence to treatment
In a 10-year naturalistic follow-up study in Vitoria, Spain, we analyzed the differences in adherence between men and women with bipolar disorder and identified factors associated with nonadherence using bivariate and logistic regression models. A total of 72 subjects were recruited and, at inclusion, the mean ± standard deviation age of the men and women were 44.00 ± 13.65 and 43.57 ± 16.42 years, respectively. During follow-up, 16 subjects (22.2%) were considered poorly adherent to lithium treatment: five on the basis of low serum lithium levels and 11 by both clinical assessments and assays. Some patient characteristics differed between the adherent and nonadherent men and women (
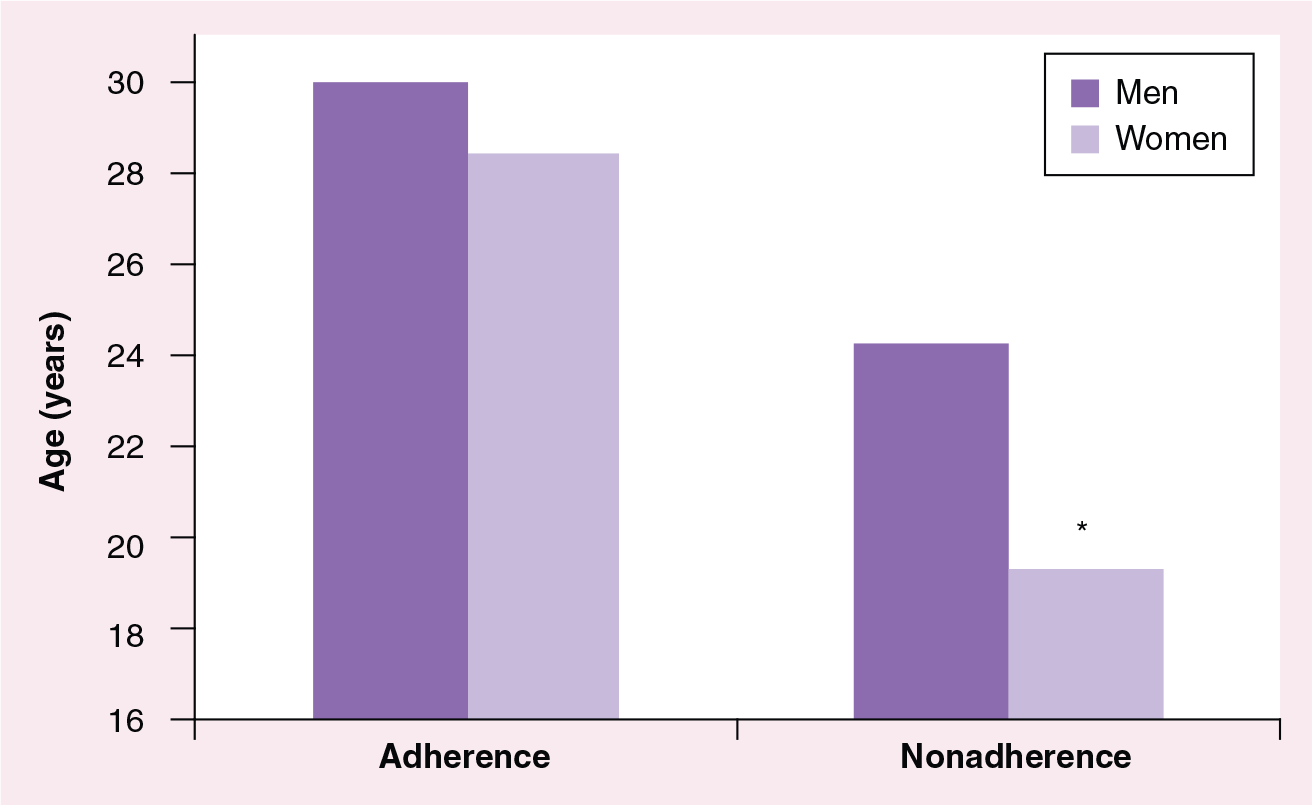
Differences in age of onset of bipolar disorder between adherent and nonadherent patients.
Adherence to treatment was higher in women than men: 93.3 versus 60.61%, respectively, were classified as adherent (
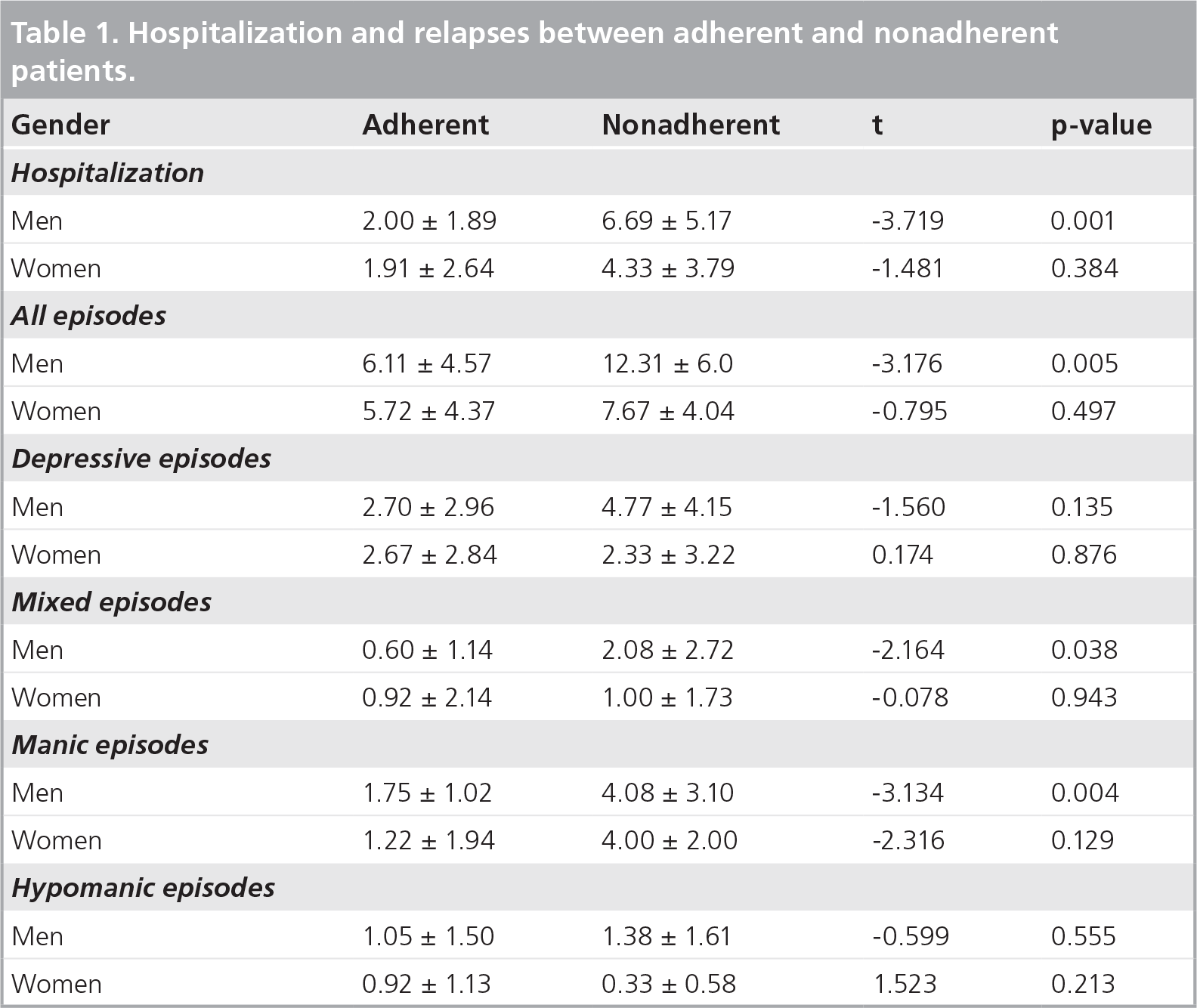
Hospitalization and relapses between adherent and nonadherent patients.
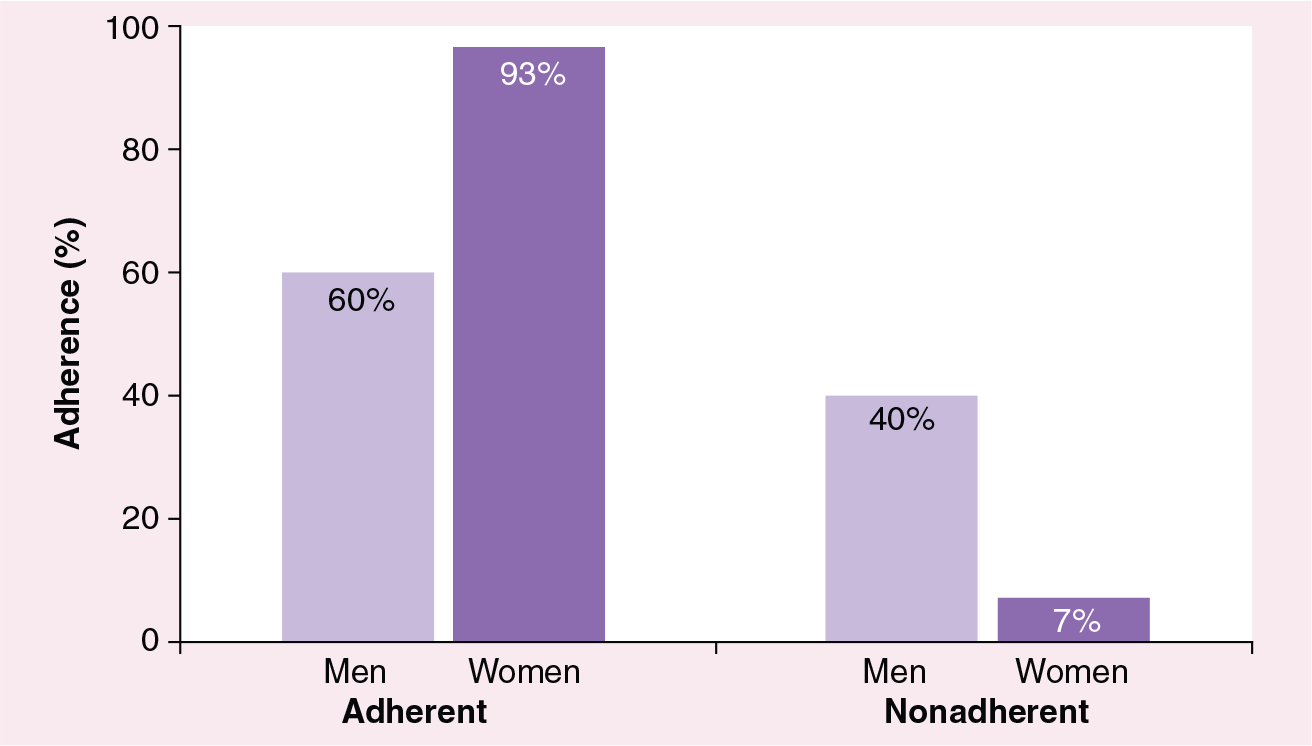
Differences in adherence between women and men.
In logistic regressions, the dependent variable was adherence to treatment in the group of men, as there were very few nonadherent women. In men, the number of hospital admissions for manic and mixed episodes were both statistically significant (manic p = 0.017, odds ratio [OR] = 2.13; mixed p = 0.028, OR = 1.64), whereas the number of manic episodes was statistically significant (p = 0.002, OR = 1.87), but the number of mixed episodes was not statistically significant (p = 0.074, OR = 1.64). These findings support existing evidence that there are important differences in adherence between men and women with bipolar disorder.
Special considerations during pregnancy & the postpartum period
The management of bipolar disorder in women during pregnancy and the postpartum period needs special consideration and is currently being investigated in many studies. However, despite the high prevalence of bipolar II disorder, there are few studies of its impact during pregnancy and the postpartum period.
Some studies have reported that between 20 and 30% women with bipolar disorder have a postpartum mood episode, mainly of the depressive type, within 1 month of delivery [36,37]. Other studies have reported that between 9 and 20% of women have hypomanic symptoms after delivery [37,38]. Hypomanic symptoms are more difficult to diagnose because they may be confused with the normal joy experienced by mothers after childbirth. There is no consensus on the prevalence of postpartum mood episodes and it has been reported that as many as 40–67% of women with bipolar disorder experience a postpartum mania or depression [39].
If bipolar disorder begins after childbirth, misdiagnosis as major depressive disorder can be a common problem. Sharma et al. explain that more than half of the outpatients seen consecutively with the referral diagnosis of postpartum depression were later diagnosed as having bipolar disorder [37,40]. Misdiagnosis of bipolar disorder as major depressive disorder during the postpartum period can lead to delays in the prescription of suitable pharmacological treatment. Moreover, inappropriate treatment with antidepressants may precipitate mania or a mixed state and, in the worst cases, psychiatric hospitalization [41].
Treatment during pregnancy
Some authors recommend suspending pharmacological treatment during the first trimester of gestation and even during the 2–3 weeks before conception, suggesting that this would avoid adverse effects of treatment on the fetus [42]. However, it is not easy for women with bipolar disorder to stop taking their medication during pregnancy as this would interfere with their activities of daily living, including taking care of a child [43], inadequate nutrition, increased alcohol or tobacco use, exposure to other medications or natural remedies (herbal, homeopathy), problems in family environment and deficits in mother–infant bonding [44].
There is a lack of information on the consequences of taking bipolar disorder medication during pregnancy; the few studies available on this subject have reported conflicting results.
It has been reported that taking lithium during pregnancy can cause birth defects, such as Ebstein's anomaly, which is a rare cardiac problem [42]. However, the association between mood stabilizer use during pregnancy and an increased risk of birth defects or other adverse outcomes is unclear [45]. Some studies report that the use of mood stabilizers (especially valproic acid) and antipsychotics during pregnancy increases the risk of congenital malformations, pregnancy complications, neonatal complications, extrapyramidal motor symptoms and longer term developmental outcomes throughout childhood [42,46–50].
The effects of poly therapy in pregnant women with bipolar disorder is a further concern. In a recent study, Holmes et al. assessed the risk of malformation among infants born to women who had taken lamotrigine or carbamazepine as part of poly therapy during the first trimester of pregnancy [51]. The authors concluded that the risk of malformation was significantly higher when lamotrigine or carbamazepine was used together with valproate, but not when either anticonvulsant was used alone. Therefore, in these situations, the doctor must choose which medications to prescribe during pregnancy on the basis of their experience, that of their colleagues, and the evidence-based information available, and always after discussing the risks and benefits of therapy with the woman and her family.
Recently, McCauley-Elsom et al. reviewed the use of antipsychotics in pregnancy [50]. Although only limited data are available, they found two single cases with normal babies before taking olanzapine in pregnancy and one case with fetal malformations with multiple anomalies, but they could not conclude it was due to medication because the rate of major malformations was no significantly different to those who were not exposed to antipsychotic medications. In a review of 36 prospective and retrospective cases, the rates for spontaneous abortion (13%), stillbirth (5%), prematurity (5%) and major malformation (0%) were similar to those for the general population [50]. Use of olanzapine or clozapine during pregnancy has been associated with a significantly heavier mean infant birth weight compared with intrauterine exposure to typical antipsychotics [52]. Olanzapine appears to be associated with a higher risk of metabolic complications in pregnant women [53], but other studies have reported that the development of the fetus, delivery and development of the child during the first 6 months were normal [54]. Yeshayahu reports the single case of a woman who took olanzapine during her pregnancy (with no other substances or complications), whose baby was born with an atrioventricular canal defect and unilateral clubfoot [55]. Such findings cannot be attributed to a teratogenic effect of olanzapine.
Clozapine is commonly used during pregnancy, and there are reports of no complications or birth defects as well as case reports of neonatal convulsions, floppy baby and gestational diabetes [50]. In one case report of a woman who took clozapine throughout her pregnancy and while breastfeeding her baby for 1 year, the baby had delayed speech acquisition [56]. However, it was not possible to conclude whether this neurodevelopmental difficulty was due to the use of clozapine or other factors. Others case reports on clozapine use during pregnancy have reported no complications or congenital anomalies [57,58].
There are few reports on the safety of risperidone treatment during pregnancy. In their review of antipsychotics, McCauley-Elsom et al. concluded that exposure to risperidone does not increase pregnancy risks compared with those in women not taking the drug [50]. Other single case reports provide support for the successful use of risperidone during pregnancy without postnatal complications [43,59–61].
The same is true for quetiapine use during pregnancy, with the majority of cases reporting no adverse outcomes, although the existing information is limited and other medications may have been taken before or during the pregnancy [50,62]. To date, there is little information on the effects of aripiprazole use in pregnant women. There is one case report of fetal tachycardia in a woman who took aripiprazole during conception and some of her pregnancy, but the baby had no neurodevelopmental impairment [63]. Other case reports did not find any association between aripiprazole use during pregnancy and fetal complications [50]. There are only two case reports of ziprasidone use during pregnancy: in one case, the baby was born with a cleft palate [64]; in the other case, the mother took ziprasidone and citalopram and had a baby without abnormalities [65].
Benzodiazepine treatment during pregnancy has been associated with cleft lip and palate, and some authors recommend these drugs should not be used during the first trimester [42]. Although bipolar disorder symptoms are often accompanied by symptoms of anxiety and insomnia, it is common practice to avoid using anxiolytic and hypnotic benzodiazepines during pregnancy, but there is no scientific consensus on this issue. It is unethical to perform randomized controlled trials of benzodiazepine use in pregnant women. However, it is also not good practice to systematically deny the use of benzodiazepines during pregnancy. Today, we know that acute maternal anxiety may have significant effects on the fetus and that, regardless of alterations in fetal behavior observed at the time of delivery, fetal exposure to high maternal anxiety has been associated with delayed mental development and an increased risk of developing behavioral and emotional problems in childhood. There is also an increased risk for postpartum depressive symptoms in the mother [66].
With regards to the teratogenicity of benzodiazepines, we know from the meta-analysis of Altshuler et al. that exposure to benzodiazepines during pregnancy can cause cleft lip/palate in the fetus, and that this risk is higher with diazepam than with alprazolam [67]. The Committee on Drugs of the American Academy of Pediatrics [68] recommends the use of short-acting agents, such as alprazolam and lorazepam, if a benzodiazepine is needed for the treatment of acute mania during pregnancy. For preventive treatment, lorazepam is preferred over alprazolam because it has no active metabolites, high potency and a low placental concentration, and is not associated with a neonatal abstinence syndrome as seen with alprazolam.
Antiparkinsonian drugs are not are not recommended during the gestation [42].
Electroconvulsive therapy (ECT) is often the treatment of choice for depression during pregnancy and has been reported to be a safe and effective option in pregnant women [69,70]. However, there are few controlled studies of the effects of ECT during pregnancy and the literature consists mostly of case reports [71–74]. ECT is recommended by the American Psychiatric Association Task Force on ECT [75]. The only complications reported after ECT during pregnancy include vaginal bleeding [72] and premature uterine contractions, although child development after delivery was normal [73]. Because ECT can promote uterine contractions, it is essential to have proper coordination with obstetric services. Anesthetics used during ECT cross the placenta and fetal blood–brain barrier but are not a serious threat due to the brevity of exposure. The use of drugs with anticholinergic effects should be kept to a minimum to reduce the risk of gastroesophageal sphincter relaxation and, thereby, the risk of suction, which is already high in the ECT [76].
Treatment in the postpartum period
In the postpartum period, women with bipolar disorder require medication because they have an increased risk for mood episodes which, if severe, rarely can lead to suicide or infanticide [74,77,78].
During lactation, treatment of women with bipolar disorder aims to minimize infant exposure and adverse effects while maintaining optimum maternal mental health. The mood stabilizers carbamazepine and valproate are considered compatible with breastfeeding, whereas lamotrigine should be used with caution and lithium use during lactation is discouraged [37,79]. There are no firm conclusions about the risks or benefits of most antipsychotic medications in breastfeeding, but clozapine and olanzapine should be considered contraindicated during breastfeeding, although further long-term data on the effects of drug exposure through breast milk are needed [80,81].
The use of relatively low doses of benzodiazepines does not seem to be a contraindication to breastfeeding. However, infants less able to metabolize benzodiazepines may have sedation and feeding difficulties even if the dose received by the mother is low [66,76].
Electroconvulsive therapy can be used safely during lactation if care is taken not to breastfeed the infant too soon after the ECT session in order to minimize the effects of anesthetics, muscle relaxants and anticholinergics on the infant [66].
During the first month after childbirth, there is an increased risk of psychiatric re admission in women with bipolar disorder; however, in the subsequent postpartum period, nonmothers with mental disorders have higher re admission rates than mothers with mental disorders [82].
Future perspective
It is evident from the above review that it is still unclear whether there are important differences between men and women in their experience of bipolar disorder. The studies conducted to date have reported differing and sometimes contradictory results.
There is a lack of specific studies conducted during pregnancy and the postpartum period in women with bipolar disorder. Both are critical periods and a relapse or recurrence of symptoms at either stage can have serious consequences for the woman and/or her baby and the relationship between them. It is important for the mother to remain in a stable mental condition during pregnancy and in the postpartum period. Many key clinical questions remain unanswered. Are women with bipolar disorder at greater risk of mood episodes during pregnancy or in the postpartum period? What medications for bipolar disorder are safe to take during pregnancy and lactation? Should medication be started or continued throughout pregnancy or taken only in certain trimesters and/or at lower doses? What are the teratogenic risks of the different medications available for treating bipolar disorder? Does exposure to medication in utero or via breastfeeding cause neurodevelopmental impairment in the child? What are the short- and long-term consequences of nonadherence with bipolar disorder medication during pregnancy and in the postpartum period? Despite these many questions, it is clear that the potential harmful effects of medication on the fetus must be balanced against the risk of worsening mood episodes in the mother and poorer treatment outcomes, including relapse, hospitalization, poor functioning, violence and suicide.
Some research suggests that medication for bipolar disorder should be stopped during pregnancy, mainly during the first few months, but the impact of this on the mother has not been well studied. If the mother has a relapse during pregnancy, what memory will she have of that pregnancy and how will it affect the relationship with her child? If a woman continues to take her medication during pregnancy we must know from studies what adverse effects may occur so we can make informed decisions about the risks involved. However, it is very difficult to carry out clinical trials in pregnant women. If we decide to use a lower dose of medication during pregnancy for fear of teratogenic risk, we must take into account the increased risk of relapse and the inherent risks of untreated disease.
Given the obvious ethical difficulties of conducting clinical trials in pregnant women, we must find other ways of collecting, collating and disseminating data on bipolar disorder in women during pregnancy and the postpartum period, while respecting the confidentiality of patients. Towards this, it would be of enormous value if systematic records were kept at routine gynecology visits on the use of psychotropic drugs. Also, it would be helpful if all psychiatrists took notes on the pregnancies of their patients and the development of the offspring.
Thyroid disorders have been associated with mood alterations and bipolar disorder, especially in women, but there is little published data on this. The association between thyroid function and bipolar disorder and its treatment are areas for further research.
In our study we found that women are more adherent to medication than men, but the major finding of the research is that women with younger onset and who are not married have a higher risk of lack of compliance with medication. These data have important consequences because these are the women with higher risk of having an unplanned pregnancy. If women stop their medication during pregnancy there is a high risk of relapse. This has been associated with inadequate nutrition, increased drug abuse, problems with other members of the family and deficits in the mother-child relationship.
Substance abuse is common in bipolar disorder and is associated with nonadherence which, in turn, is associated with relapse. Women with bipolar disorder have four-times the rate of alcohol use problems and seven-times the rate of other substance use disorders, compared with women in the general population [7]. Several risk factors are associated with comorbid substance abuse in patients with bipolar disorder: early age of onset, male gender, family history of substance use disorders and presence of mixed mania [29,83].
Currently, substance abuse is more common in men than women, but this appears to be changing: drug consumption in women is increasing and has almost reached the same level as that in men. Interventions to avoid or reduce substance abuse are important for the whole population, but even more so for people with a family history of bipolar disorder. There is some evidence that substance abuse is associated with the early onset of psychosis. Further work on the impact of substance abuse in patients with bipolar disorder is needed.
Treatment discontinuation is an important factor associated with relapse and recurrence in bipolar disorder [29,84]. Some studies have found that the female gender is associated with better medication adherence in bipolar disorder [3,21,29,85], whereas other studies have not found any association between gender and adherence [24,84]. These differences are probably due to the different ages of women in these studies. Younger and nonmarried women have higher rates of noncompliance, and should be carefully studied and treated.
Despite our improved knowledge on nonadherence to treatment in patients with bipolar disorder, differences in adherence between men and women need to be better understood. Kriegshauser et al. found no differences between men and women in perceived weight gain, but women were significantly more concerned than men about weight gain [33]. This finding probably reflects a greater influence of societal factors such as body image in women. It is important to consider these factors when prescribing medication to women as drug-induced weight gain may be a major contributor to nonadherence with medication. More research is needed on strategies for improving adherence in people with bipolar disorder. Psychoeducation can improve treatment adherence and patient understanding of the benefits and risks of medication.
Executive summary
Bipolar disorder is a serious mental disorder that causes extreme changes in mood, energy and functioning.
The clinical course of bipolar disorder is characterized by the occurrence of one or more manic or mixed episodes. Often individuals also have recurrent episodes of major depression.
Bipolar I disorder has equal prevalence in men and women.
Men usually present with manic episodes and comorbid drug abuse is common.
Women usually present with major depressive episodes and the onset is often later than in men. Comorbidity of physical pathology, including thyroid disease, eating disorders and anxiety disorders is common.
Specific factors are associated with treatment nonadherence in bipolar disorder, such as younger age at onset, male sex, a lower level of education, being single, comorbid abuse of alcohol or drugs, and excess affective morbidity.
Atypical antipsychotics include: aripiprazole, clozapine, olanzapine, risperidone, quetiapine and ziprasidone.
Mood stabilizers include: lithium and anticonvulsants (e.g., valproate, carbamazepine and lamotrigine).
Anxiety or insomnia can be treated with benzodiazepines.
Some studies report that the use of mood stabilizers (especially valproic acid) and antipsychotics during pregnancy increases the risk of congenital malformations, pregnancy and neonatal complications, extrapyramidal motor symptoms and longer term developmental outcomes throughout childhood. Other studies did not find abnormalities in children whose mother took medication during pregnancy.
Electroconvulsive therapy is often the treatment of choice for depression during pregnancy and has been reported to be a safe and effective option in pregnant women.
There are no firm conclusions about the risks or benefits of the use of most antipsychotic medications during breastfeeding, however, clozapine and olanzapine should or be used during breastfeeding, although further long-term data on the effects of drug exposure through breast milk are needed.
The mood stabilizers carbamazepine and valproate are considered to be compatible with breastfeeding, whereas lamotrigine should be used with caution and lithium use during lactation is discouraged.
Electroconvulsive therapy can be used safely during lactation if care is taken not to breastfeed the infant too soon after the electroconvulsive therapy session in order to minimize the effects of anesthetics, muscle relaxants and anticholinergics on the infant.
Female gender is associated with better medication adherence in bipolar disorder.
Substance abuse is associated with nonadherence and is more common in men than women.
Women had more concern than men about weight gain and perceived higher quality relationships than men.
Men with bipolar disorder are more likely than women to abuse alcohol, but there are no gender differences in the rates of drug abuse and in reports of lessened irritability and/or impulsivity due to psychiatric medications.
Adherence to treatment was higher in women than men.
Men tended to abuse substances more frequently than women, and nonadherent men had more substance abuse than adherent men.
Civil status was associated with adherence only in women: all adherent women were married.
Nonadherent men had significantly more episodes of bipolar disorder than adherent men.
Nonadherent men also had more hospitalizations than adherent men, whereas in women there were no differences in hospitalizations according to adherence.
Nonadherent women had more suicide attempts (F = 0.05) than woman who adhered to their treatment.
It is still unclear whether there are important differences between men and women in their experience of bipolar disorder.
It is important for the mother to remain in a stable mental condition during pregnancy and in the postpartum period.
There is a clear need for more studies on gender differences in bipolar disorder and how to improve adherence to treatment.
A better understanding of how to treat women with bipolar disorder during pregnancy and lactation will undoubtedly lead to improved outcomes for both the mother and her child.
Further work on this and improving the subjective experience of illness will help improve patient outcomes.
In conclusion, there is a clear need for more studies on gender differences in bipolar disorder and how to improve adherence to treatment. Moreover, a better understanding of how to treat women with bipolar disorder during pregnancy and lactation will undoubtedly lead to improved outcomes for both the mother and her child.
Footnotes
Acknowledgements
The authors would like to thank the mental health professionals who helped with this research.
Bipolar disorder among women
To obtain credit, you should first read the journal article. After reading the article, you should be able to answer the following, related, multiple-choice questions. To complete the questions (with a minimum 70% passing score) and earn continuing medical education (CME) credit, please go to www.medscape.org/journal/wh. Credit cannot be obtained for tests completed on paper, although you may use the worksheet below to keep a record of your answers. You must be a registered user on Medscape.org. If you are not registered on Medscape.org, please click on the New Users: Free Registration link on the left hand side of the website to register. Only one answer is correct for each question. Once you successfully answer all post-test questions you will be able to view and/or print your certificate. For questions regarding the content of this activity, contact the accredited provider,