
Abstract
Background:
Postpartum hemorrhage (PPH) is a global health concern and remains the leading cause of maternal death worldwide. Studies assessing the prevalence of PPH and related maternal risk factors in the United Arab Emirates are scarce.
Objectives:
This study aims to evaluate the prevalence of PPH and associated maternal risk factors in women in the Emirate of Abu Dhabi.
Design:
Prospective mother and child cohort study.
Methods:
This analysis was based on data from the Mutaba’ah Study. The sample composed of 2937 women who underwent normal vaginal delivery (2017–2023). Descriptive analysis was performed to compare the characteristics between patients with PPH and those without PPH. Logistic regression analysis was performed to identify maternal characteristics associated with PPH.
Results:
Overall prevalence of PPH was 4.3% (n = 125, 95% CI: 3.6%–5.1%). The median total blood loss among women with PPH was 700 mL (interquartile range (IQR): 600–1000), and 20% of affected women required blood transfusion. No observed significant difference between those with and without PPH regarding maternal education, body mass index, and comorbidities (p > 0.05). Women with PPH were younger at pregnancy (median (IQR): 28.4 (23.8, 34.3) versus 29.8 (25.4, 34.6), p = 0.022), and had higher proportions of assisted vaginal delivery (13% versus 3.7%, p < 0.001) compared to those without PPH. Women with PPH had significantly greater neonate weight compared to women without PPH (median (IQR): 3210 (2975, 3490) versus 3140 (2865, 3430), p = 0.029). In the adjusted analysis, women who underwent assisted vaginal delivery (adjusted odds ratio, aOR (95% CI): 2.82 (1.60, 4.97)), and those with increased neonate weight (aOR per 100 g: 1.06 (1.01, 1.10)) remained significantly associated with developing PPH.
Conclusion:
Findings of this study underscore the importance of early identification of women at increased risk of PPH to provide tailored obstetric care. Improved management protocols and increased awareness among healthcare providers are essential to mitigate the risk of PPH and ultimately enhance maternal outcomes.
Plain language summary
Postpartum hemorrhage (PPH), or heavy bleeding after childbirth, is the leading cause of death in mothers during or after giving birth around the world. However, there is little known about how common PPH is and what causes it in the United Arab Emirates (UAE). This study looked at data from nearly 3000 women in the Emirate of Abu Dhabi who gave birth naturally (vaginal delivery) between 2017 and 2023, as part of the Mutaba’ah Study. The goal was to find out how many women experienced PPH and what factors might make it more likely. The study found that about 4 in every 100 women (4.3%) had PPH. Women who had PPH were more likely to have had an assisted delivery (for example, using tools like forceps or vacuum), or a surgical cut called an episiotomy. They also tended to be younger and giving birth for the first time. Heavier newborns were also linked to a higher risk of PPH. These findings suggest that certain women may have a higher risk of bleeding after childbirth. Identifying these women early and providing specialized care may help prevent complications and improve the safety of mothers during delivery.
Introduction
Postpartum hemorrhage (PPH) is characterized by excessive blood loss exceeding 500 mL after vaginal delivery or over 1000 mL following a cesarean section. 1 According to the World Health Organization, approximately 14 million women globally are affected by PPH annually, making it the leading cause of maternal death worldwide. 2 It is estimated that a woman dies from PPH every 2 min, resulting in approximately 70,000 maternal deaths annually.2,3 In developed nations, effective emergency care has significantly reduced PPH-associated maternal mortality rates. 4 However, the incidence of PPH continues to rise, potentially due to unrecognized modifiable risk factors and inadequate preventive measures. 5
The risk factors contributing to PPH are multifaceted, including physiological, obstetric, and healthcare-related factors. Common causes include uterine atony, retained placental tissue, lacerations, and coagulation disorders.6,7 Preventive measures for PPH are taken only in women with certain risk factors, such as multiple gestation, polyhydramnios, and coagulopathy. 8 In these cases, uterotonic agents such as oxytocin are administered during the third stage of labor to help the uterus contract, as well as to ensure adequate iron intake and red blood cell levels during prenatal care, as a way to minimize the risk of PPH. 9 However, many cases of PPH occur in women without identifiable risk factors. 10 In addition, survivors of PPH often face severe complications, including the need for emergency surgical intervention or long-term health consequences such as fertility impairment.11 –13
The prevalence of PPH varies considerably across different populations and regions, often influenced by healthcare access, maternal health status, and socioeconomic conditions.7,14,15 In the United Arab Emirates (UAE), the prevalence of PPH and its associated risk factors remains understudied. Despite that, maternal mortality rates in the UAE are generally low compared to global averages; specific complications like PPH warrant further investigation. 16 Research has highlighted that obesity is increasingly recognized as a major risk factor for various complications during pregnancy and childbirth, including PPH. Elevated pre-pregnancy body mass index (BMI) has been linked to an increased risk of obstetric complications such as PPH. Yet, findings across different studies have been inconsistent regarding other ranges of BMI.17,18 In the UAE, the prevalence of obesity has surged, particularly among women, with studies indicating a two- to three-fold increase from 1989 to 2017. 19 Previous research in the UAE has explored the relationship between pre-pregnancy BMI and cesarean section rates but has not specifically investigated its risk of developing PPH. 20
The prevalence of PPH and its associated risk factors in the UAE has not been previously studied. This gap in knowledge poses significant public health implications, as identifying risk factors for PPH can enhance preventive measures and improve maternal health outcomes. Therefore, this study aims to evaluate the prevalence of PPH and associated maternal risk factors in women of reproductive age in the Emirate of Abu Dhabi.
Materials and Methods
This analysis was based on an ongoing prospective maternal and child cohort study—the Mutaba’ah Study—in Al Ain, the Emirate of Abu Dhabi, UAE. The Mutaba’ah Study is the largest cohort study in the UAE recruiting pregnant women from the Emirati population and following them up during antenatal, birth, and postnatal periods, and their children until the age of 18 years. Further details about the Mutaba’ah Study, including the recruitment process and data variables, are available elsewhere. 21 The study was approved by the UAE University Human Research Ethics Committee (ERH-2017-5512) and the Abu Dhabi Health Research and Technology Ethics Committee (DOH/CVDC/2022/72). Informed written consent was obtained from all participants prior to data collection. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement for cohort studies in preparing this manuscript. 22 The complete checklist is provided in the Supplemental Material.
Study sample
The study sample comprised of 2937 pregnant women who underwent normal vaginal delivery between 2017 and 2023. Only women with singleton pregnancies were included. Women who had cesarean delivery, abortion, or unspecified delivery mode were excluded from the final analysis. Women with primary PPH (⩽ 2 h after delivery) were identified using the International Classification of Diseases—10th revision (ICD-10) code (O72), and confirmed by documented blood loss of 500 mL or more. The blood loss was estimated clinically using the visual method, and the amount is routinely documented in the medical records. The ICD-10 codes have been semantically validated by cross-reference with clinical documentation for all cases.
Data collection
Data were collected using a self-administered questionnaire and extraction from the medical records. The questionnaire was administered during pregnancy by a trained research assistant. Collected data were automatically stored in the study database. The questionnaire collects data on sociodemographic characteristics (i.e., age, gender, education, and occupation), past and current pregnancy history, and medical history. In contrast, data on anthropometric measurements, laboratory results, medical and surgical interventions, and clinical details of previous pregnancies were collected from the medical records. For this study, we utilized data on participants age, education, BMI, parity, comorbidities like diabetes mellitus, hypertension, and surgical and medical interventions like episiotomy, and assisted vaginal delivery, vaginal laceration, and risk factors of uterine atony.
Multiple etiologies could be assigned for each PPH case, as applicable. The data were obtained directly from medical records, and causes were classified using a multiple-cause approach rather than a single primary cause.
Standard PPH prophylaxis in the hospital
As the standard of care, the active management of the third stage of labor as PPH prophylaxis includes administration of 100 μg of intramuscular carbetocin for every patient after delivery of the baby. Controlled traction of the umbilical cord is also used for the placenta expulsion. Uterine fundal massage after expulsion of the placenta is not routinely applied. Additionally, women with a history of three or more deliveries receive 40 IU of oxytocin in 500 mL of normal saline at a rate of 167 mL/h for a duration of 3 h as a routine prophylactic care.
Post hoc sample size estimation
The minimum required sample size for developing the multivariable model was retrospectively estimated using the approach of Riley et al., which specifies criteria to limit overfitting and ensure precise estimation of model parameters and overall risk. 23 Inputs included an anticipated model discrimination (C statistic = 0.828) and an outcome prevalence of 1.9%, derived from a large multicenter study in Hunan Province, China. 24 A global shrinkage factor of 0.90 and 10 candidate parameters were specified. This procedure yielded a recommended minimum of N = 2816 participants.
Statistical analysis
In descriptive statistics, continuous variables were summarized using median and interquartile range (IQR), while categorical variables were presented using counts and percentages. Demographic, maternal, and birth-related characteristics were compared between women with PPH and those without using the Wilcoxon rank-sum test and Pearson’s chi-squared test or Fisher’s exact test for continuous and categorical variables, respectively.
Simple and multivariable logistic regression were used to identify risk factors associated with PPH. Independent variables in the unadjusted analysis with p-values <0.25 were entered into the adjusted analysis. In the adjusted analysis, variables with missing values such as education (6.5%), delivery assisted (0.4%), parity (0.8%), previous pregnancy outcome (2.9%), baby’s gender (0.04%), and weight (0.2%) were imputed using Multivariate Imputation by Chained Equations using the package mice in R. 25 Furthermore, estimates from the five repeated complete data analyses were combined using Rubin’s rules. 26 In a sensitivity analysis, we re-examined the adjusted analysis when missing values were handled using complete case analysis. Multicollinearity among independent variables was evaluated using the generalized variance inflation factor. All predictors demonstrated acceptable values (<2.0), indicating no significant multicollinearity in the model. First-order interaction terms involving maternal age and neonatal birth weight with other predictors (e.g., parity, assisted vaginal delivery, and episiotomy) were evaluated in the multivariable model. No significant interactions were observed (all p > 0.05), and thus only main effects were retained in the final model. All statistical tests were two-sided; p-values <0.05 were considered statistically significant. All analyses were performed using R software version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria). 27
Results
A total of 2937 pregnant women with vaginal deliveries were included in the analysis with 125 experienced PPH (Figure 1). The overall prevalence of PPH in this cohort was 4.3% (95% CI: 3.6%–5.1%).

Cohort flowchart.
The median age at pregnancy and pre-pregnancy BMI of the study sample were 29.7 years (IQR: 25.4–34.6) and 26.8 (IQR: 23.5–30.6), respectively. Overall, almost one-quarter (24%) of pregnant women were older than 35 years, and two-thirds (65%) of the women were overweight or obese. Moreover, 21.4% of the pregnant women were nulliparous. Assisted vaginal delivery and episiotomy use were observed in 6.6% and 16.3%, respectively. Finally, the median neonate weight was 3140 g (IQR: 2870–3430).
Characteristics of pregnant women included in the study
There was no significant difference between the two groups (with PPH versus without PPH) regarding education, BMI, and comorbidities (p > 0.05). However, women with PPH were younger at pregnancy (median (IQR): 28.4 (23.8, 34.3) versus 29.8 (25.4, 34.6), p = 0.022), and had higher rates of assisted vaginal delivery (12.6% versus 3.7%, p < 0.001), and episiotomy (7.7%, versus 3.6%, p < 0.001) compared to those without PPH. Women with PPH also had higher birth weights compared to those without PPH (3210 (IQR: 2975–3490) versus 3140 (IQR: 2865, 3430), p = 0.029). The prevalence of PPH among women with high birth weight was twice that of women with normal birth weight; however, this difference was not statistically significant (8.6% versus 4.3%, p = 0.10). The demographic, maternal, and birth characteristics of the pregnant women examined in this study were summarized and presented in Table 1.
Baseline demographic, maternal, and birth characteristics of women with and without postpartum hemorrhage, United Arab Emirates, 2017–2023.

IQR: interquartile range; BMI: body mass index.
Wilcoxon rank-sum test; Pearson’s chi-squared test; Fisher’s exact test.
Bold significance level at p-value <0.05.
In the full study sample, the prevalence of PPH among nulliparous women was twice that of grand multipara (6.7% (4.9%–9.0%) versus 3.2% (2.2%% versus 4.7%); Supplemental Figure S1). Interestingly, women with increased age (>35 years) had a significantly lower proportion of PPH compared to younger women (<30 years) (3.4% (2.3% versus 5.2%) versus 5.0% (3.9–6.2%)). No significant difference in the prevalence of PPH was observed across the three pre-pregnancy BMI categories; however, a lower prevalence of PPH was noted in obese class II (3.0%) compared to normal (4.5%) and obese class III (5.9%), indicating a nonlinear relationship between the five BMI categories and PPH (Supplemental Table S2).
Clinical characteristics of PPH cases
The median total blood loss (in mL) in PPH patients was 700 (IQR: 600–1000, min–max: 500–4700). Of the 125 patients, 24 cases (20%) required blood transfusions. Uterine atony was the most frequently reported cause of PPH (52.8%, n = 66), followed by trauma/laceration (25.6%, n = 32), retained placenta (22.4%, n = 28), and placental problems like placenta abruption (3.2%, n = 4; Figure 2(a)). Multiparity (previous three or more deliveries) was the most documented characteristic among the PPH patients (43.2%, n = 54), followed by assisted vaginal delivery (13.6%, n = 13). High blood pressure, including preeclampsia and history of PPH, was reported in 4.8% (n = 6), whereas macrosomic children were noted in 4.0% (n = 5) of the PPH patients (Figure 2(b)).

Documented causes and clinical characteristics of 125 women with postpartum hemorrhage in the United Arab Emirates, 2017–2023. (a) Causes and (b) clinical characteristics of women with postpartum hemorrhage in the study sample. Of 125 postpartum hemorrhage cases, 37.6% (n = 47) and 9.6% (n = 12) had no defined risk factors and causes, respectively.
Factors associated with the odds of developing PPH
Simple and multivariable logistic regression models were used to identify factors associated with PPH (Table 2). In the unadjusted analysis, a year increase in age at pregnancy was associated with a 4% decrease in the odds of PPH (crude odds ratio, cOR (95% CI): 0.96 (0.93, 0.99); p = 0.017). Pregnant women with a parity of above four were less than 50% less likely to experience PPH at delivery compared to nulliparous (0.46 (0.28, 0.75); p = 0.002). Women who underwent assisted delivery had over three and a half times the odds of developing PPH (3.77 (2.31, 5.95); p < 0.001). Finally, baby birth weight (cOR per 100 g: 1.04 (1.00, 1.08); p = 0.045) became significantly associated with increased risk of PPH.
Unadjusted and adjusted logistic regression analysis of factors associated with postpartum hemorrhage in pregnant women, United Arab Emirates, 2017–2023.
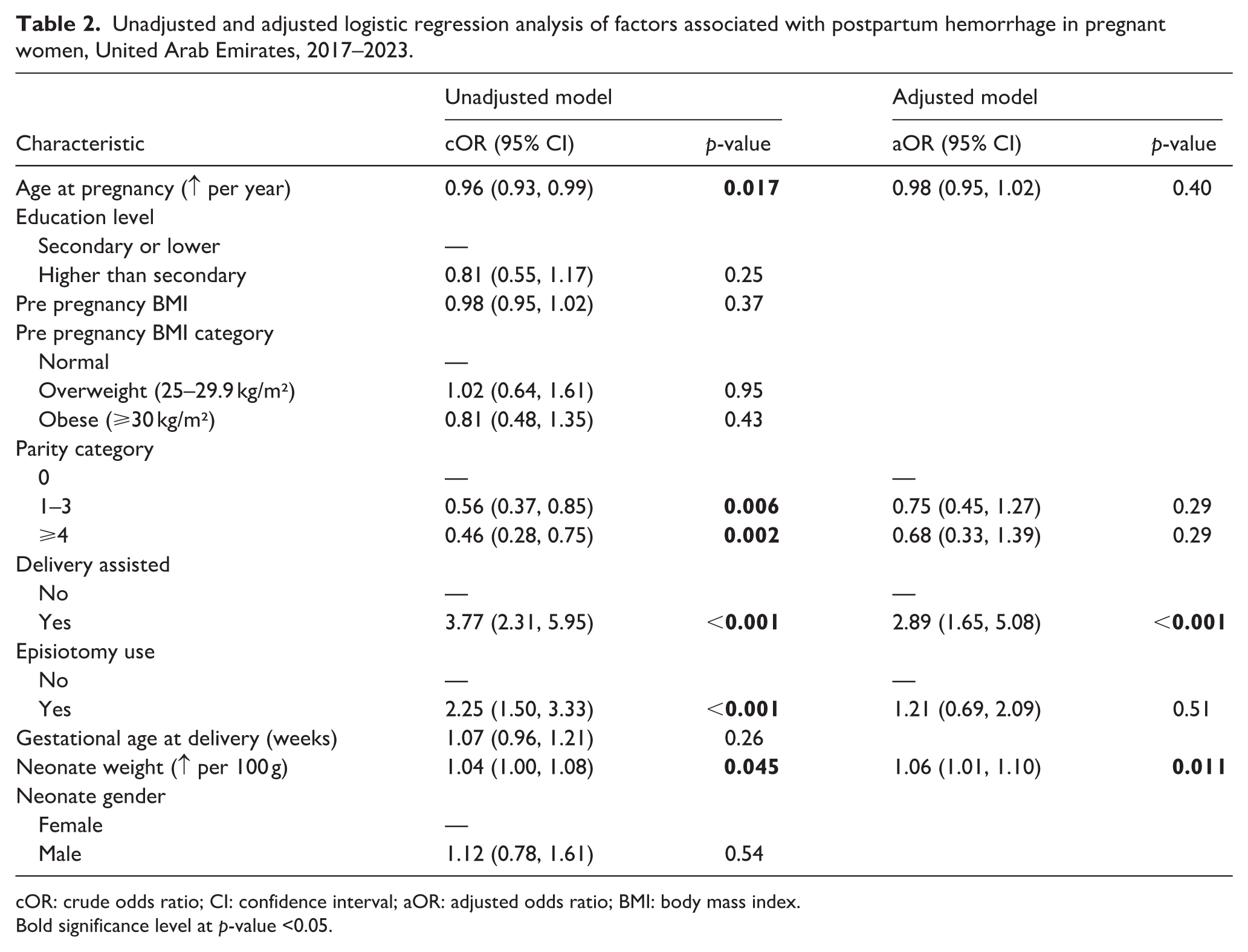
cOR: crude odds ratio; CI: confidence interval; aOR: adjusted odds ratio; BMI: body mass index.
Bold significance level at p-value <0.05.
In the adjusted logistic regression, women who underwent assisted delivery (adjusted odds ratio, aOR (95% CI): 2.89 (1.65, 5.08); p < 0.001) and neonatal birth weight (aOR per 100 g: 1.06 (1.01, 1.10); p = 0.011) remained significantly associated with developing PPH. Notably, the significant association between PPH and neonatal birth weight diminishes following categorization (Supplemental Table S3). The sensitivity analysis, which used a complete case analysis, demonstrated comparable results to our main analysis (Supplemental Table S4).
Discussion
The study identified significant risk factors associated with increased risk of PPH in a culturally specific group of women from the Emirati population characterized by multiparity and extended reproductive time. In the presented cohort of 2937 pregnant women, the overall prevalence of PPH was 4.3%, and the median total blood loss in PPH patients was 700 mL. The observed prevalence of PPH in this cohort is comparable to recent findings reported from other Middle Eastern populations; 4.0% in Oman, 2.5% in Saudi Arabia, and 3.7% in Egypt.28 –30 Almost one-quarter were older than 35 years, and two-thirds were overweight or obese. Interestingly, the frequency of PPH was higher in women who underwent assisted vaginal delivery and delivered babies with increased neonatal birth weight. Moreover, uterine atony, trauma/laceration, and retained placenta were among the most commonly reported causes of PPH development.
PPH remains one of the leading obstetric complications. In the present study, we utilized the standard definition of PPH, with a threshold of 500 mL of blood loss. A meta-analysis conducted by Can-ran Huang, which included 36 articles, found that the incidence of PPH was 17% among the group of patients whose blood loss exceeded 500 mL. 31 In contrast, the prevalence of 4.3% in our study was lower than the international findings and only 20% of women required a blood transfusion. The low percentage of hemorrhages likely resulted from the active management of the third stage of labor, which routinely included the administration of prophylactic uterotonics. 32
One of the key elements in managing PPH is prevention as well as the ability to anticipate its occurrence based on the presence of risk factors. According to the literature, the most common risk factors include prior cesarean section, a history of PPH, hypertensive disorders, multiparity or in some instances nulliparity, obesity, macrosomia, abnormal fetal position, multiple pregnancy, and placental spectrum disorders. 31 Moreover, cervical ripening, prolonged second or third stage of labor, induction or augmentation of labor, assisted delivery, genital tract trauma, and episiotomy can also increase the risk of PPH. 31 In the present study, we confirmed assisted vaginal delivery and increased neonatal birth weight as risk factors for PPH. It is worth noting that most studies were conducted many years ago, while medical management and prophylaxis have changed significantly in recent years. At the hospital where this study was conducted, standard PPH prophylaxis includes administrating 100 μg of intramuscular Carbetocin to every patient. Additionally, women with a history of three or more deliveries receive 40 IU of oxytocin in 500 mL of normal saline at a rate of 167 mL/h for 3 h. The elevated preventive doses may contribute to the relatively low prevalence of PPH (4.3%), and could also explain the absence of association between obesity and PPH in the study, notwithstanding the considerable prevalence of obesity. Nonetheless, analogous findings were observed from Denmark. 33 Conversely, the correlations between obesity and PPH identified in other research may stem from uncalibrated prophylactic doses relative to the patient’s weight (the usual dose consists of 5–10 IU of oxytocin).34,35 Another confirmed risk factor is assisted vaginal delivery, which is also associated with a higher incidence of vaginal trauma.36,37 Increased fetal weight, as a risk factor for PPH, applies not only to cases with confirmed macrosomia.36,38,39 In our study, we demonstrated that every 100-g increase in fetal birth weight raises the odds of PPH by 6%.
In the present study, we also identified additional pregnancy-related causes of PPH, and the results are consistent with global trends.31,40 The most common of those were uterine atony (52.8%), followed by trauma/lacerations (25.6%) and retained placenta (22.4%). An interesting finding is that, despite the use of potent uterotonics, uterine atony remains one of the most frequent causes of PPH in our study sample. The relatively high incidence of genital tract trauma may be related to the current trend toward spontaneous vaginal deliveries without episiotomy and the patient’s advanced age. 41 However, the current meta-analysis proved no significant difference between non-episiotomy and selective episiotomy regarding the risk of obstetric anal sphincter injuries. Still, it may significantly increase the risk of first degree perineal tears.42,43 This risk may additionally increase with the other components, like a macrosomic baby and a nulliparous patient.41,44,45
Limitations
The presented study encompasses a substantial cohort of nearly 3000 pregnant women from the Emirati population. It is the first research conducted within the culturally and ethnically distinct Middle East and North Africa region. By focusing exclusively on patients who experienced vaginal deliveries and ICD-10 reliance, the study underscores the significance of advanced PPH prophylaxis, which likely contributed to the observed low prevalence of PPH. Furthermore, the study does not corroborate several previously identified risk factors, such as obesity, advanced maternal age, and episiotomy. This finding aligns with recent research suggesting that while factors like obesity and advanced maternal age have been associated with PPH, their predictive value may be limited in different cohorts.
Although the study included a representative sample of pregnant women from the Emirati population, the data comes from only one city in the UAE (Al Ain), which may limit the generalizability of the findings to all pregnant women in the UAE. Healthcare practices, sociodemographic characteristics, and service accessibility may differ across other Emirates. Therefore, additional multicenter studies covering other regions of the UAE are warranted to confirm and extend these findings. Furthermore, the initial extraction of patient data was based on ICD-10 codes, potentially leading to the omission of patients who were not diagnosed with PPH during hospitalization. Moreover, the routine use of uterotonics as part of the active management of the third stage of labor could have contributed to underestimating the number of patients in the study group. Additionally, we included only the patients with immediate PPH, which can also narrow the group to the early cases. Another limitation of this study is the absence of data on antenatal care utilization, induction of labor, and duration of labor. These variables are known to influence both delivery outcomes and the risk of PPH. Similarly, hematologic parameters such as hemoglobin level, anemia status, and platelet count were incomplete for many participants. In a supplementary analysis limited to available data, platelet count showed a non-significant result after adjustment for obstetric variables. These findings suggest that while hematologic and intrapartum factors may influence the risk of PPH, their effects were not independently captured in this analysis. Future studies with comprehensive antenatal and laboratory data are warranted to better elucidate these pathways.
Conclusion
The study revealed a prevalence consistent with previous reports of PPH among Emirati women following vaginal delivery. However, the findings support the importance of early identification and closer monitoring of pregnant women at increased risk for PPH, such as those undergoing assisted vaginal delivery or with increased neonatal weights. Improved management protocols and increased awareness among healthcare providers are essential to mitigate the risk of PPH and ultimately enhance maternal outcomes. Moreover, available data highlights the importance of active management of the third stage of delivery as a method of PPH prophylaxis.
Supplemental Material
sj-docx-1-whe-10.1177_17455057261429219 – Supplemental material for Postpartum hemorrhage following vaginal delivery and associated risk factors in the United Arab Emirates: The Mutaba’ah study
Supplemental material, sj-docx-1-whe-10.1177_17455057261429219 for Postpartum hemorrhage following vaginal delivery and associated risk factors in the United Arab Emirates: The Mutaba’ah study by Abubaker Suliman, Amal AlZahmi, Shouq Alnuaimi, Dana B. Alshomali, Taif K. AlKaabi, Aleema Sadafa Nellikunnu Sameer, Aasiya Beevi, Mohammad Khogali, Kornelia Zaręba and Luai A. Ahmed in Women's Health
Footnotes
Acknowledgements
The authors would like to acknowledge and thank all the participants of the Mutaba’ah Study.
Ethical considerations
The Mutaba’ah Study is approved by the UAE University Human Research Ethics Committee (ERH-2017-5512) and the Abu Dhabi Health Research and Technology Ethics Committee (DOH/CVDC/2022/72).
Consent to Participate
Informed written consent was obtained from all participants prior to data collection.
Consent for publication
Not applicable.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the United Arab Emirates University Summer Undergraduate Research Experiences (SURE+) Program (G00004859). The funder had no role in the design, conduct, or dissemination of the results of the current study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All relevant data are available within the manuscript. Additional requests could be submitted to the Mutaba’ah Study after ethical approval.
Supplemental material
Supplemental material for this article is available online.
Artificial intelligence use
We acknowledge the journal’s Artificial Intelligence Policy. Generative AI tools (e.g., ChatGPT) were used to assist with language edition, grammar refinement, and formatting of the manuscript. No AI-generated data, analysis, or references were created or modified using these tools. The authors have thoroughly reviewed all content for accuracy and originality and take full responsibility for the scientific integrity of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.