
Abstract
Postpartum depression (PPD) is a common mental health challenge in resource-constrained sub-Saharan Africa (SSA). Characterizing its correlates will aid prediction, early detection, and pre-emptive interventions. This review aimed to systematically synthesize and stratify PPD correlates in sub-Saharan Africa. The review was structured as per the Preferred Reporting Item for Systematic Reviews and Meta-Analyses. We included studies that reported the correlates of PPD in SSA. We searched PubMed, Medline, CINAHL, Academic Search Complete, and PsycINFO for relevant peer-reviewed literature. The correlates of PPD constituted the primary outcome. A random effect model was fitted to estimate the pooled correlation coefficient per correlate. The clinical relevance of correlates was stratified based on strength of correlation (r) and recurrence (f). The mean age of the participants was 27.0 ± 6.0 years, and 68.6% of participants had completed at least secondary education. The correlates of PPD in SSA were intimate partner violence (IPV) ((risk weight (rw) = 2.8; r = 0.212 (confidence interval (CI): 0.11–0.31), poor social support (PSS) (rw = 1.9; r = 0.250 (0.133–0.361)), unwanted pregnancy (UP) (rw = 1.6; r = 0.279 (CI: 0.14–0.41); I2 = 95.89), and maternal age (MA) (rw = 0.96; r = 0.27 (CI: 0.154–0.37)), among others. A cumulative risk weight of ⩾0.95 was predictive of PPD and marks the critical point at which preemptive interventions should be instituted. The stratification of risk PPD factors and computation of risk stability index are useful in identifying the clinical significant risk factors. The provision of critical risk point will simplify early detection thus facilitating cost-effectiveness. Of the correlates of PPD in SSA, IPV, PSS, UP, and MA are the most important. Targeted screening and pre-emptive interventions for women with high risk weight may be a reasonable strategy both in the short and long term.
Introduction
Postpartum depression (PPD) is often misdiagnosed in women, and as a result, patients are left with no treatment options. 1 This is attributable to a lack of understanding of the diagnosis and treatment of PPD by family health practitioners. 2 At least 25% of mothers with PPD experience symptoms that extend for more than 6 months. 3 In sub-Saharan Africa (SSA) Africa, the pooled prevalence is 16.8%, although a recent and robust yet-to-be-published meta-analysis pegged the SSA African PPD rate at 21.8%. 4 PPD makes newborn care more difficult and even puts the baby at risk of injury. In extreme cases of PPD, mothers have been documented to try to harm their children. Adolescent psychiatric disorder is more common in children whose mothers have PPD. 5 PPD is most frequently diagnosed between a few weeks and about a year following delivery. 6 PPD has been observed to occur up to 4 years following delivery. 7 Early detection and treatment of PPD remain poor in SSA Africa due to a major lack of focus. 8 Fortunately, PPD is both preventable and treatable if it is detected and treated early.9,10 PPD early prevention and treatment must be guided by a thorough understanding of the risk factors, as is the case with other disease conditions.
In SSA Africa, several factors have been linked to PPD, including age, education, household income, and unplanned pregnancies.11,12 However, the strength and recurrence of these correlates are yet to be ascertained. We expect that policymakers’ attention will be called to the socioeconomic implications of PPD in pursuit of universal health coverage and the African Union Agenda 2063, therefore sparking adequate support for early detection and treatment. We conducted this systematic review to fill in gaps on the correlates of PPD in SSA Africa as part of the efforts to treat and prevent the disease. We aim to provide policymakers in SSA Africa with the most relevant PPD correlates. Hence, the review aimed to systematically characterize and stratify the correlates of PPD in SSA for prediction purposes and early intervention.
Methods
Protocol and registration
This is a systematic review of epidemiological studies aimed at synthesizing the evidence on the correlates of PPD in SSA Africa. The protocol was structured using the Preferred Reporting Item for Systematic Reviews and Meta-Analyses (PRISMA) checklist 13 (Supplementary file). The protocol was registered with the Open Science Framework Registry: https://osf.io/5xzp8.
Eligibility criteria
Studies that reported the correlates of PPD among postpartum women in SSA Africa were included in the review. Articles written and published in English were included. Observational studies that documented the correlates of PPD in SSA Africa irrespective of sample size, study design, sampling technique, test statistics, and whether a control group was employed or not. The correlates of PPD in SSA Africa were the primary outcome. If assessed at least once throughout the study, it was included. Clinical, sociodemographic, and study characteristics were all secondary outcomes.
Sources of information and search strategy
The principal reviewer (MN) developed the search strategy. A variety of combinations of terms from the medical subject headings and free terms from a selected number of key articles were used in the searches. To begin, a PubMed pilot search was carried out to establish the face sensitivity of the search strategy. Eventually, the most sensitive strategy yielded over 6000 papers: ‘Depression [All field] AND (postnatal or postpartum [All field] AND Africa [MeSH Terms]’. The terms were adapted to the other databases’ syntax and subject headings, including Medline, Academic Search Complete, CINAHL, and PsycINFO. An additional search was done in the references of the selected observational and review articles to further identify relevant studies.
Inclusion and exclusion criteria
The criteria for inclusion comprise peer-reviewed observational studies on PPD conducted in SSA Africa, studies in which PPD was diagnosed after 7 days postpartum solely through the use of a standard instrument (without medical examination/assessment), or studies in which PPD was diagnosed 7 days postpartum days through the use of a standard instrument and medical examination/assessment, and studies in which, except for hospital data, random sampling was used. We excluded studies that employed convenience/purposive sampling unless they were hospital studies, and studies in which PPD was diagnosed less than 7 days postpartum solely with the use of a questionnaire-based instrument (without medical examination/assessment). We excluded qualitative and case studies to allow for quantitative and cumulative synthesis.
Study records and data management
The results of the literature search were exported to EndNote 8 for data management and de-duplication, as well as the selection of articles for inclusion. After that, full-text copies of the articles that met the criteria were downloaded. The included studies’ eligibility criteria and screening forms were developed, piloted, and refined.
Procedures for selection and data collection
The title and abstract were simultaneously screened by two independent reviewers (OA and UP). In consultation with the primary reviewer (MN), conflicting points of view were reconciled. The primary reviewer double-checked the preliminary screening results and read the full text of selected studies for further screening using the previously established eligibility criteria. Data extraction was done non-independently by OA and UP, and verified and updated by MN and MU. Authors were not contacted for primary data and full texts were available. Details of the flow of studies during the selection process were presented using a PRISMA diagram, along with the rationale for exclusion (Figure 1).

PRISMA flow diagram of the systematic review on characterization and stratification of the correlates of PPD in SSA (2004–2020).
Data items
The following data items were collected: authors’ identities and study characteristics such as study design, region, the timing of diagnosis, sample size, method of assessment, the instrument used, and sampling technique.
Quality appraisal/risk of bias assessment
The risk of bias was assessed using a quality assessment checklist developed from Hoy et al. 14 It evaluates the suitability and adequacy of the methodology, as well as the study’s design, participant recruitment, data collection, analysis, and presentation of findings. It can be used to assess most study designs. The tool is made up of 10 items, with the tenth item being a summary score. The studies were assessed as low risk (0–3), medium or moderate risk (4–6), and high risk (7–8) on a 3-point Likert-type scale (7–9). Twelve (20%) of the included studies were independently appraised by MN and MU, with a rater agreement of 0.92. The remaining 48 (80%) were assessed by MU.
Summary measures
Participants’ ages were summarized using mean and standard deviation. Participants’ level of education was summarized in terms of the percentage that attained post-primary education. We pooled the correlation coefficient for each identified correlate.
Data synthesis and analysis
The pooled correlation coefficient was estimated consistent with Borenstein et al., 15 Wang and Liu, 16 and Lenhard and Lenhard. 17 The pooled correlation coefficient was synthesized using the random effect model. The heterogeneity measure and I2 were calculated following Higgins et al. 18 I2 values were interpreted per the Cochrane Handbook for Systematic Reviews of Interventions as follows: 0%–40% may indicate low heterogeneity, 30%–60% may indicate moderate heterogeneity, 50%–90% may indicate substantial heterogeneity, and 75%–100% may indicate considerable heterogeneity. 18 We fitted a meta-regression model to identify the sources of heterogeneity. MN and MU conducted the statistical analysis.
Stratification of correlates
Towards the stratification of the correlates, we computed risk weight (Rw) as a product of the effect size (r) and frequency/recurrence of correlates. High-risk weight signifies a more economically or clinically important correlate. We ranked correlates as level one, two or three based on their risk weight. Correlates up in the ladder were regarded as being more clinically important than those down the ladder.
Results
Study selection
A total of 6861 records were identified from PubMed (326), Medline (598), CINHAL (238), Academic Search Complete (5419), PsycINFO (273), and reference list (7). Following de-duplication and title and abstract screening, we eliminated 995 records that were deemed irrelevant, leaving 5866 articles for the title and abstract screening. Ultimately, 43 studies met the eligibility criteria (Figure 1). The 43 studies were also included in the meta-analysis (Table 1).
Study characteristics and risk of bias.
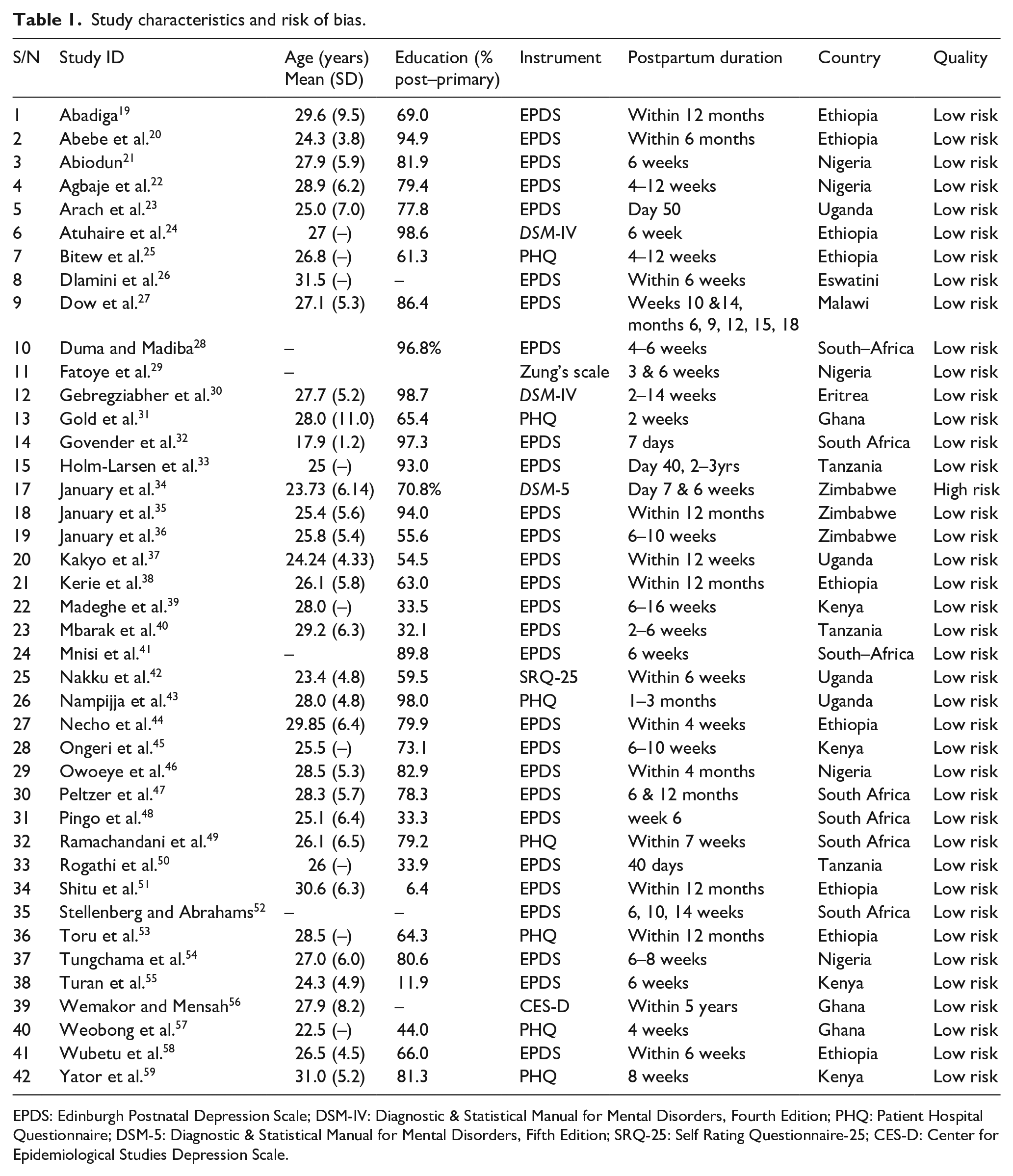
EPDS: Edinburgh Postnatal Depression Scale; DSM-IV: Diagnostic & Statistical Manual for Mental Disorders, Fourth Edition; PHQ: Patient Hospital Questionnaire; DSM-5: Diagnostic & Statistical Manual for Mental Disorders, Fifth Edition; SRQ-25: Self Rating Questionnaire-25; CES-D: Center for Epidemiological Studies Depression Scale.
Study characteristics and risk of bias
Of the 46 SSA African countries, 10 were involved in this review. About 68.6% of participants in the included studies had completed at least secondary education. Of the 43 included studies, 9 were conducted in Ethiopia, 6 in South Africa and 5 in Nigeria, and 4 each in Kenya and Uganda. The mean age of the study participants was 27.0 ± 6.0 years. Interestingly, all but one of the included studies possessed a low risk of bias (Table 1).
Correlates with PPD in SSA Africa
In this review, 17 factors emerged as the most important correlates of PPD in SSA Africa and were classified into three levels. Level-one correlates occupy the upper quartile and include intimate partner violence (rw = 2.8; r = 0.212 (confidence interval (CI): 0.11–0.31); OR = 2.2), poor social support (rw = 1.92; r = 0.250 (0.133–0.361); OR = 2.6), unplanned/unwanted pregnancy (rw = 1.62; r = 0.279 (CI: 0.14–0.41); I2 = 95.89; OR = 2.9), and maternal age (rw = 0.96; r = 0.27 (CI: 0.154–0.37); OR = 2.8). Level-two correlates occupy the interquartile range include illness in mother (rw = 0.92; r = 0.225 (CI: 0.073–0.367); OR = 2.3), being single (rw = 0.652; r = 0.181 (CI: 0.045–0.312); OR = 1.9), poor socioeconomic status (rw = 0.59; r = 0.21 (CI: 0.10–0.32); OR = 2.2), and low education (rw = 0.51; r = 0.51 (CI: 0.41–0.59); OR = 8.4). Level-three correlates occupy the lower quartile and include perinatal death (rw = 0.50; r = 0.28 (CI: 0.17–0.38); OR = 2.8), undesired infant sex (rw = 0.46; r = 0.16 (CI: 0.09–0.24); OR = 1.8), Caesarean section (rw = 0.43; r = 0.22 (CI: 0.13–0.30); OR = 2.2), substance abuse (rw = 0.37; r = 0.30 (CI: 0.091–0.478); OR = 3.1), antenatal depression (rw = 0.365; r = 0.27 (−0.03 to 0.53); OR = 2.8), poor health of new child (rw = 0.34; r = 0.12 (0.04–0.21); OR = 1.6), and primiparous ( rw = 13; r = 0.13 (−0.21 to 0.43); OR = 1.6). We observed low to substantial heterogeneity (I2 = 48.72–96.44). No publication bias was recorded (p > 0.05) (Table 2). A level-one correlate is approximately twice and thrice the risk of a level-two and a level-three correlates, respectively (Table 2).
Correlates of PPD in SSA.
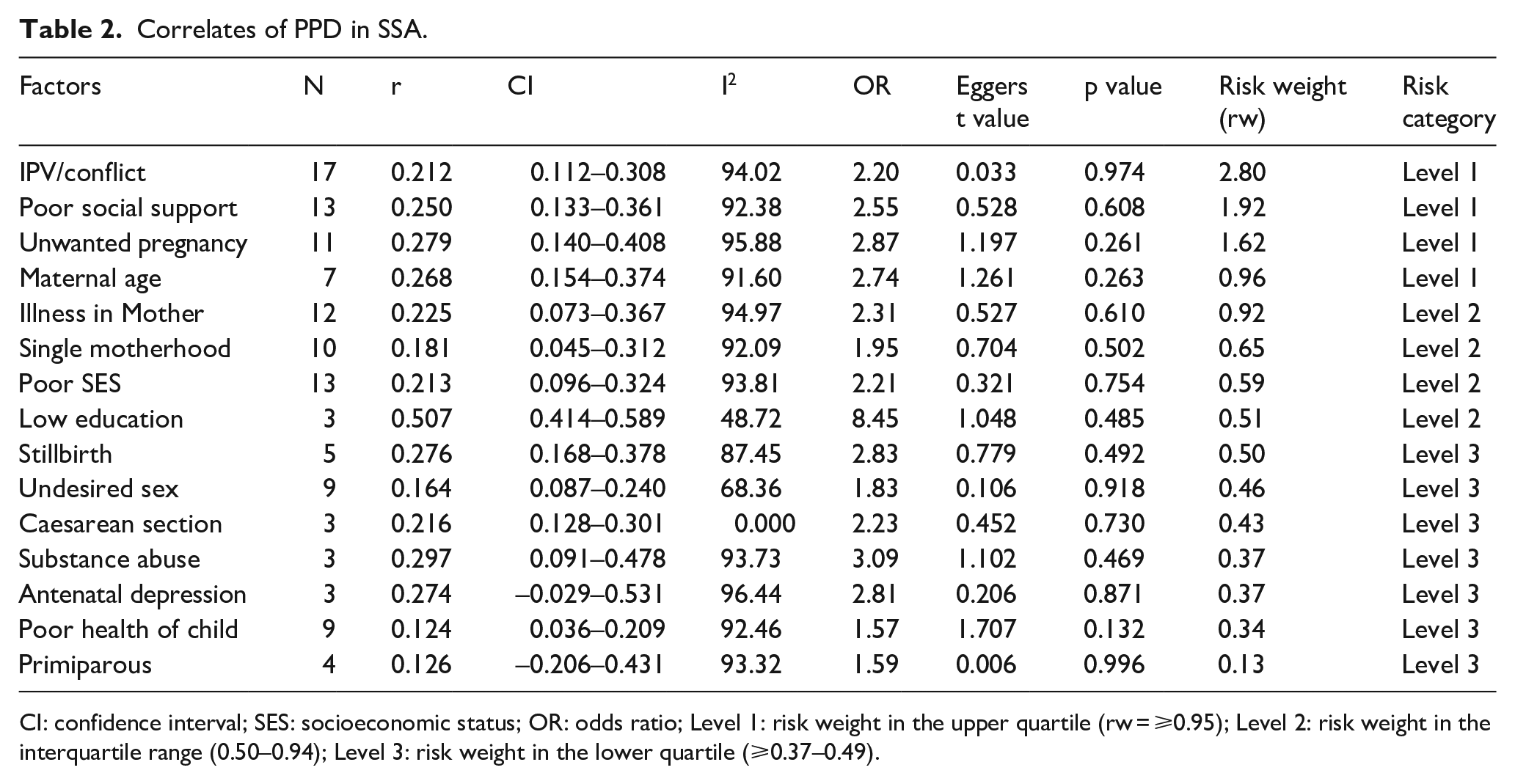
CI: confidence interval; SES: socioeconomic status; OR: odds ratio; Level 1: risk weight in the upper quartile (rw = ⩾0.95); Level 2: risk weight in the interquartile range (0.50–0.94); Level 3: risk weight in the lower quartile (⩾0.37–0.49).
Discussion
Summary of evidence
The presence of a level-one correlate namely intimate partner violence, poor social support, unplanned/unwanted pregnancy or maternal age is predictive of PPD. Hence, antenatal women with any one level-one correlate, two level-two correlates or three level-three correlates should be marked for early detection for PPD using valid and sensitive measures such as the Edinburgh postnatal depression scale (EPDS), and possible pre-emptive intervention. Based on the findings of our study, pre-emptive intervention should include conflict resolution, psychotherapy, mobilization for improved social support, and specialized child care and parenting skills. 60 Preventive measures include planned parenthood, early girl-child education, and so on. As part of the strategy to improve social supports, governments at various tiers could promulgate an affordable insurance policy to protect pregnant women, postpartum women and newborns against poor access to healthcare services. 60 Preventive measures and early interventions should be individualized and based on the underlying correlates. Ultrasound could be used to determine baby sex prior to delivery as this could aid counselling in a situation where baby sex is undesired. 61 The availability of data on risk weight of the correlates of PPD in sub-Saharan Africa may reduce cost associated with PPD. Although data on the economic burden of PPD is lacking in Africa, maternal depression cost modern societies billions of dollars per annum. 62 For example, in the United States, the cost of maternal depression was an astounding $14.2 billion – an average of $32,000 per mom. 62 This is especially in countries saddled with crises of mental health and health insurance with no pre-emptive measures. 63 Despite the lack of data on the economic burden of PPD in Africa, the cost of maternal healthcare is approximately twice those of mothers without maternal depression. 64 Hence, we advocate for preemptive intervention facilitated through early detection aided by the risk category of the emerging correlates as here discussed.
Level-one correlates
Intimate partner violence, poor social support, unplanned pregnancy, and maternal age are the most important correlates of PPD in sub-Saharan Africa. Our finding is consistent with Dadi et al. 6 in which intimate partner increased risk of PPD by approximately threefold. Marital problems such as intimate partner conflict and abusive relationships are consistent sources of stress throughout the postpartum period.48,65 Mechanisms employed by intimate partner violence include in physical and social isolation, as well as psychological injury resulting in low self-esteem and miserable living.66,67.Consistent with our study, mothers with poor social support were 2.5 times more likely than their peers to suffer from PPD. 68 Women who did not receive adequate support from close family members during birth or in the care of their newborn were shown to be less satisfied, stressed, and at a higher risk of depression. 69 Regarding the role of unplanned pregnancy in genesis of PPD, lack of preparation for childbirth and inability to cope with pregnancy, labour, and the postpartum period have been implicated. 70 Low levels of preparation may leave mothers feeling anxious, helpless, and unable (or unwilling) to cope with the changes and challenges (including financial and social stressors) that babies bring. 22 The role of maternal age in the genesis of PPD was impacted by education. In settings where early girl-child schooling is uncommon, a very young age constitute a risk of PPD due to very immature coping strategies, 54 whereas advanced maternal age is a risk for PPD in societies where early girl-child education is attainable. This could be attributed to a lack of peer support as a result of deviations from social norms surrounding maternal age, obstetrical problems, and multiple births, all of which are linked to an increased risk of complications. 71
Level-two correlates
Maternal health problem, single motherhood, and poor socioeconomic status constitute level-two correlates of PPD. By implication, the presence of any two correlates in predictive of PPD and indicates who should be candidate for early detection and pre-emptive intervention. Maternal health problems may include febrile illness, preeclampsia, HIV/AIDS, puerperal complications, and so on. Mothers with maternal health problems were 2 times more likely to develop PPD when compared with their peers. This is consistent with Dadi et al., 6 which reported a high odds of PPD along with physical illnesses especially when illness was chronic of onset. In our study, postnatal women who were single were 5 times more likely to develop PPD than those women who were married. The stigmatization that accompanies single motherhood and the socioeconomic responsibilities surrounding the care of an infant could be possible reasons. The lack of emotional support, care, guidance, material support, and assistance with chores could also be responsible for this connection.72,73 Consistent with Dadi et al., 6 our finding revealed higher postnatal depression is among mothers with lower socioeconomic status. Women with poor socioeconomic status may be disadvantaged due to a lack of financial resources and inadequate health insurance, resulting in stress. 74 Since up to 80% of the sub-Saharan African population does not have access to free medical treatment, declining socioeconomic indicators and rising healthcare costs place a heavier strain on patients and their families. 46
Level-three correlates
Stillbirth, unwanted infant sex, caesarean section, and poor health of child constitute level-three correlates. Any pregnant mother with any three of the level-three correlates should be regarded as candidate for early detection and pre-emptive interventions. Consistent with Arach et al., 23 our study shows that mothers who had experienced perinatal death were approximately 3 times as likely to develop PPD as mothers who had not experienced perinatal death. Chronic sadness characterized with spells of pervasive melancholy, sorrow, or other grief-related experiences could explain why women who experienced perinatal loss had an increased risk of postnatal depression. 75 We found C-section a relevant correlate of PPD in SSA. It is said to be initiated by surgical trauma and the financial burden of the procedure and stigmatization for surgery in Africa, particularly in Nigeria. 46 Consistent with our finding, dissatisfaction with child gender constituted a risk for PPD as reported in several studies conducted in SSA Africa.29,46,52 Some studies, however, found no link between PPD and dissatisfaction with the gender of the child.69,76 Hence, there could be cultural factors causing this discrepancy in findings, as the importance of gender changes across different cultures. Regarding the role of poor health of the new child in occurrence of PPD in SSA, the risk of PPD was 3–4 times higher in mothers with infants suffering from illness that limit the ability to breastfeed and sleep. 77 Infant sickness increases mother’s stress level while reducing her ability to sleep. 78 Mothers of babies who have problems sleeping were about four times more likely to be depressed compared with mothers with healthy newborns. 78 Hence, putative pathways that mediate PPD in these mothers may include maternal sleeplessness and exhaustion.79,80 One limitation in this study was the failure to account for the role of sub-ethnic disparity in the development of PPD. However, it is reasonable to argue that ethnic-related difference in development and occurrence of PPD may be insignificant across sub-Saharan African settings.
Implications for policy and practice
To stem the growing tide of PPD in SSA, psychotherapy, conflict resolution, and/or social support including specialized child care training should be offered to expectant mothers identified with a level-one correlate, expectant mothers with any two of the level-two correlates, and expectant mothers with any three of the level-three correlates with level one. To reduce cost and improve care efficiency, targeted PPD screening of at-risk pregnant women should be promoted. Preventive measures and early interventions should be individualized and based on the underlying correlates.
Conclusion
There are three levels of PPD correlates in SSA. Level-one correlates are the most important and include intimate partner violence, poor social support, unplanned pregnancy, maternal age, and illness in the mother. A cumulative risk weight of ⩾0.95 was predictive of PPD and marks the critical point at which preemptive interventions should be instituted. Targeted support and pre-emptive interventions for women with high risk weight may be a reasonable strategy both in the short and long term.
Supplemental Material
sj-docx-1-whe-10.1177_17455057221118773 – Supplemental material for Characterization and stratification of the correlates of postpartum depression in sub-Saharan Africa: A systematic review with meta-analysis
Supplemental material, sj-docx-1-whe-10.1177_17455057221118773 for Characterization and stratification of the correlates of postpartum depression in sub-Saharan Africa: A systematic review with meta-analysis by Martins Nweke, Maryjane Ukwuoma, Ada C. Adiuku-Brown, Princewill Ugwu and Elizabeth Nseka in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.