
Abstract
Objective
There is a paucity of data on the psychosocial issues and coping mechanisms among pregnant and postnatal women with COVID-19 infection. We, therefore, aimed to explore the psychosocial issues and coping mechanisms of pregnant and postnatal women diagnosed with COVID-19 at tertiary-level hospitals.
Methods
This was a qualitative phenomenological study conducted in 2021 with a sample size of 16 women admitted at two referral hospitals serving as COVID-19 admission facilities for pregnant and postnatal women in Lusaka, Zambia. In-depth interviews were conducted via telephone to understand what these women experienced when diagnosed with COVID-19. All the interviews were audio-recorded and transcribed verbatim. Thematic analysis was conducted using the six steps approach to develop emerging themes.
Results
Two major themes emerged: psychosocial issues and coping mechanisms. The primary psychosocial issues were worry and stigma. Women worried about infecting their unborn baby or neonate, being separated from the baby, the general safety of the baby, and the health of other family members. Women also worried about the attitude of health care providers and faced discrimination or stigma because of their infection. Thus, some coping mechanisms were developed that helped them, such as a positive attitude, keeping the disease secret, reliance on family members for support and using positive information from social media.
Conclusion
This study provides unique insights into the psychosocial experiences of pregnant and postnatal women diagnosed with COVID-19. Women were particularly concerned about the unborn baby’s well-being and discrimination.
This study suggests the need for policy and clinical practice to consider the integration of effective mental health services into the provision of maternal health and COVID-19 services.
Introduction
The coronavirus disease 2019 (COVID-19) was declared a pandemic by the World Health Organization (WHO) in March 2020. Some facts show that the disease is triggered by severe respiratory syndrome and has shown a rapid increase in cases and number of deaths since its emergence. 1 The disease has been noted to have no sex or age predilection although severe disease has been reported more in the very young, very old and those with other comorbidities. 2 Furthermore, due to the physiological changes in the respiratory system during pregnancy, studies have been done to ascertain the risk of disease in pregnant women, their foetuses and newborns. In addition, it has been shown that there is an increased risk of hospital admission among pregnant women, however, it cannot be concluded that there is an increased risk of maternal and foetal complications, as earlier studies have shown conflicting results.3,4
The first case of COVID-19 in Zambia was reported on 18 March 2020, since then, the disease has spread countrywide with reports of severe illness and associated mortalities. 5 The government through the Ministry of Health has instituted several measures to control the spread of the disease. These measures include movement restrictions, a limited number of people during social gatherings, remote work and mandatory isolation for anyone who tests positive for COVID-19. In addition, some guidelines for the provision of essential services including maternity care were changed in many ways, such as routine COVID-19 testing and the introduction of obstetric COVID-19 isolation/admission wards to reduce the spread of the virus among staff and patients.
Due to uncertainties that come with the disease, anxiety has continued to build among pregnant women with regard to vulnerabilities of contracting the disease, progression to severe illness and risk of transmission to the foetus or their newborn. 6 Experiences from previous pandemics show that women opted to abscond from antenatal and postnatal care for fear of contracting the infection hence, increased reports of fear and anxiety. 7 Social media and poor understanding of COVID-19 has also contributed to the ongoing anxiety due to the unverified information perinatal women are exposed to. 8
The virus keeps mutating and impacting all age groups including the already known vulnerable populations, such as pregnant and postpartum women. Notwithstanding, there is currently no disaggregated data to show the trends and psychosocial impact of COVID-19 on pregnant and postnatal women in Zambia. Therefore, this study aimed to explore psychosocial issues and coping mechanisms of pregnant and postnatal women who presented to the admission facilities with a positive COVID-19 test result in selected referral hospitals in Lusaka, Zambia, which were doubling as COVID-19 centres. Understanding pregnant and postnatal women’s psychosocial experiences is critical to guide practice and policy on maternal mental health needs and concerns during the COVID-19 pandemic and future pandemics.
Methods
Study Design and Setting
We conducted a qualitative study using a descriptive phenomenological approach to understand the lived experiences of pregnant and postnatal women in the admission facilities during the COVID-19 pandemic. The study was conducted in 2021 in two tertiary hospitals in the Lusaka Province of Zambia. Lusaka Province is one of Zambia’s ten provinces with the largest population. Lusaka city, within Lusaka Province is the nation’s capital and hub for both local and international travellers making it vulnerable to infection. As the virus spread in Zambia, Lusaka became the epicentre of the disease. Due to the quality of care required for COVID-19 patients, the government through the Ministry of Health initially assigned two tertiary hospitals as COVID-19 management centres, namely, Women and Newborn Hospital at the University Teaching Hospitals (WNH-UTH) and Levy Mwanawasa University Teaching Hospital (LMUTH). All pregnant and postnatal women with COVID-19 were admitted to these two health facilities.
Participants and Recruitment
Pregnant, intrapartum and postnatal women who presented or were admitted to the WNH-UTH or LMUTH between January and April 2021 with a positive rapid diagnostic test (RDT) or polymerase chain reaction (PCR) test for COVID-19 were eligible for this study. Pregnant women were recruited irrespective of the trimester while postnatal women were eligible if they had tested positive immediately after delivery up to 6 weeks post-delivery. All women presenting to the facility with abortion before testing positive for COVID-19 were excluded. Sixteen participants were included in the study through purposive sampling based on informed consent and their ability and willingness to share information about their experiences. Sampling was achieved with the help of the COVID-19 registers at each of the two selected facilities. None of the authors were involved in the recruitment process but a trained research assistant recruited participants and scheduled interviews after obtaining informed consent. This was in tandem with reducing coercion for the pregnant and postnatal mothers’ participation in this study. 9
Data collection and analysis
In keeping with national guidelines of social distancing and isolation for patients with COVID-19, interviews were done via recorded phone call, as the most convenient and equitable mode, especially for women coming from low social backgrounds with limited knowledge of the use of video conferencing platforms, such as ZOOM. Interviews were conducted at a time determined by the woman after discharge from the hospital or substantial recovery. Data were digitally recorded translated to English where applicable and transcribed verbatim by trained research assistants.
A pre-tested in-depth semi-structured questionnaire with open-ended questions and probes was used in this study. For face and content validity, the questionnaire was piloted for clarity and ease of understanding after which a few adjustments were made to ensure coherence. 10 Four participants were included in the pilot (two pregnant and two postnatal) and data from these participants were excluded from final analysis.
To gain a broad understanding of COVID-19 infection among pregnant and postnatal women, the questionnaire included four different sections that covered sociodemographic characteristics of the participant, general perspective on how women were handling the pandemic and their perception of the information obtained from the media, experiences of women before and after testing positive for COVID-19, and the perception of care received at the admission or diagnosing facility. Through the course of interviews, the research assistant remained as reflexive as possible ensuring that first a rapport was created, not asking leading questions but providing probes to avoid introducing personal biases. The study sample size was determined after reaching thematic saturation at 16 interviews. 11 The interviews lasted 25 min on average.
The interview transcripts were labelled and given unique codes to ensure anonymity that read as P [numeral] denoting participants and the numeric digit was the participant’s identification number that was given consecutively. Thematic analysis, a six-stepped method for conducting qualitative data analysis was used in this study. The iterative process includes familiarization with the data, generating initial codes, searching for themes, reviewing themes, defining and naming themes, and producing the report or manuscript. 11 The transcripts were read several times to obtain deeper meaning and understanding of the data. A codebook was independently generated by JCK and CJ inductively, and the codes were compared initially for areas of divergence to reach a consensus. Thereafter, all data were systematically coded, categorized and merged into themes. A third co-author MKL served as the gatekeeper and independently ensured that the themes that were induced were correctly representing the research findings to add rigour and credibility to our study findings. The standards for reporting qualitative research (SRQR) criteria were used in the planning, implementing and reporting of this research. 12 All authors and research assistants expressed reflexivity in all these steps.
Ethical Approval
Ethical approval was obtained from the University of Zambia Biomedical Research Ethics Committee reference number: UNZA-1187/2020. Permission was sought from the National Health Research Authority and the Senior Medical Superintendents from WNH-UTH and LMUTH, and the Director for infectious diseases from Zambia’s Ministry of Health.
Statement of human and animal rights
All procedures in this study were conducted as per the University of Zambia Biomedical Research Ethics Committee-approved protocols.
Statement of informed consent
Written informed consent was obtained from eligible study participants for both the study participation and the recording of the interviews. This was done while their identities were masked with participant numbers. Participants were assured of confidentiality.
Results
After piloting the interview guide, we contacted 22 eligible women for possible recruitment and successfully enrolled 16 participants after reaching thematic saturation. We had six refusals who cited various reasons (Figure 1). The mean age of the participants was 32 years old, 2/16 (12.5%) were single, 7/16 (43.8%) came from high density residential areas, 8/16 (50%) were employed, 10/16 (62.5%) were pregnant while 6/16 (37.5%) were postpartum, and parity ranged from 1 to 4 (Table 1). Two major themes emerged: women’s psychosocial/mental issues during the COVID-19 pandemic and coping mechanisms. Table 2 provides detail on the major themes and subthemes.

Flowchart of eligible participants for the study.
Socio-demographic characteristics.

Thematic presentation of experiences of pregnant and postnatal women diagnosed with COVID-19.
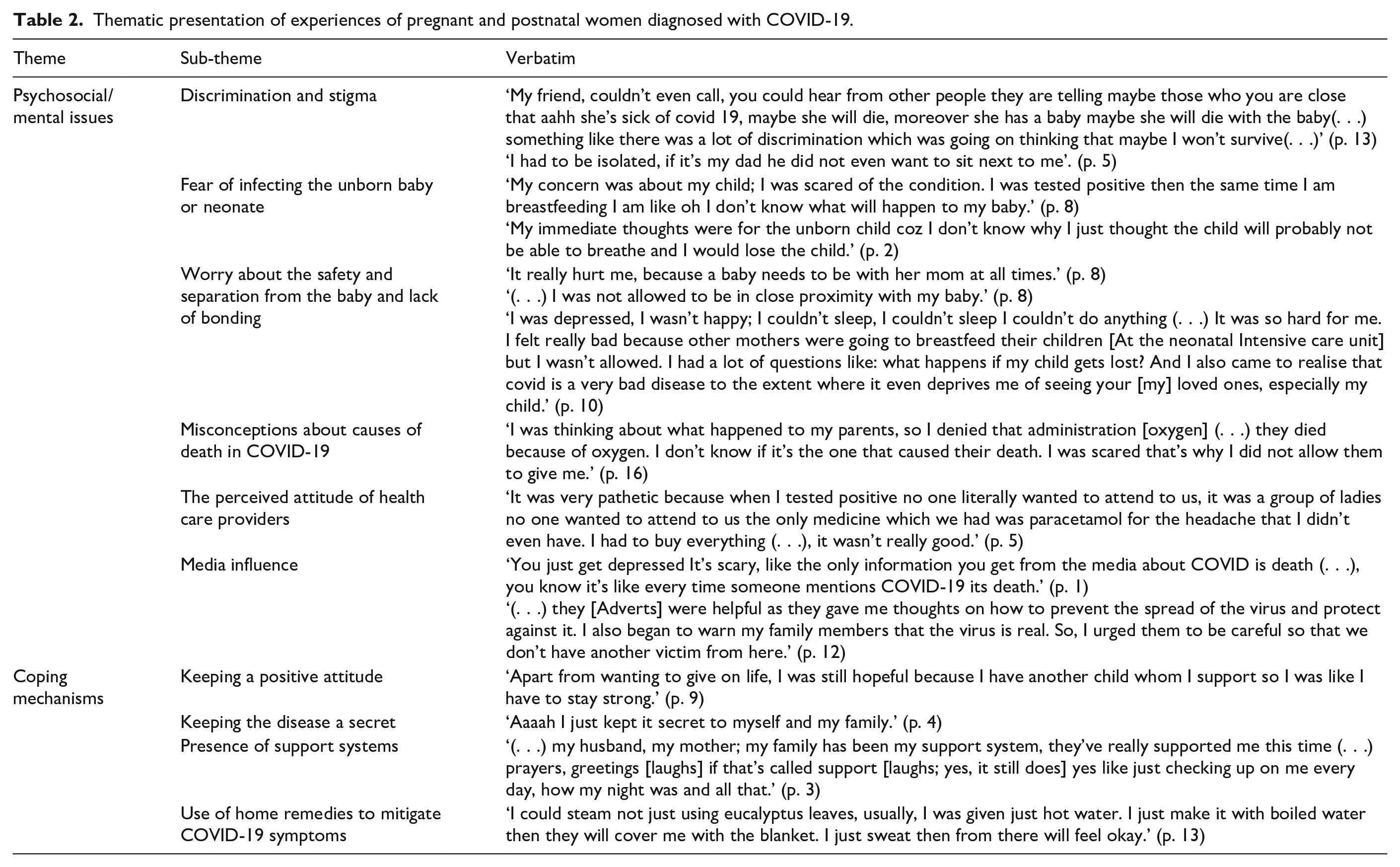
Psychosocial/mental issues
Discrimination
Since the first case of COVID-19 was reported in Zambia, stigma and discrimination have been prevalent among people who have the disease. The women in this study were not immune to this and reported discriminatory experiences with friends and family following the diagnosis.
My friend, couldn’t even call [me], you could hear from other people they are telling maybe those who you are close [to] that aahh she’s sick of COVID-19, maybe she will die, moreover she has a baby, maybe she will die with the baby something like that, there was a lot of discrimination which was going on thinking that maybe I won’t survive. (p. 13) I had to be isolated, if it’s my dad he did not even want to sit next to me. (p. 5)
One participant described feeling left out of a lot of events even after her symptoms had subsided and had a negative test result: They would just say, no don’t come near, don’t do this, don’t what. Then after you tell them I’ve been cleared, they say, no stay for a month again so that, you are sure. I missed out on a lot of things like functions, had funerals but even after I was fine, couldn’t attend. (p. 6)
Fear of infecting the unborn baby or neonate
The well-being of the unborn baby or neonate was of great concern to most of the participants. Not being sure if the disease could be transmitted during pregnancy or breastfeeding made the women scared and unsure of what to do to keep the baby safe.
My concern was about my child; I was scared of the condition. I was tested positive then the same time I am breastfeeding, I am like oh I don’t know what will happen to my baby. (p. 8) My immediate thoughts were for the unborn child cause I don’t know why I just thought the child will probably not be able to breathe and I would lose the child. (p. 2)
Worry about safety of the baby, separation from the baby and lack of bonding
Women who tested positive were required to be in isolation for 7–14 days and had uncertainties on how to care for the baby. On the other hand, some of them were completely separated from the neonates. The women expressed sadness at this as they felt it was important to be with their neonates for bonding. This was unique to postnatal women (. . .) It really hurt me, because a baby needs to be with her mom at all times. (p. 8)
When asked how long it took some mothers to see their babies, varying responses in the length of time were provided, with some indicating that it took 2 weeks, one mother had this to say, (. . .) but it took very long, about the whole two weeks. (p. 9)
The safety of the baby in the absence of the mother was of concern.
I was depressed, I wasn’t happy; I couldn’t sleep, I couldn’t do anything (. . .) It was so hard for me? I felt really bad because other mothers were going to breastfeed their children [From neonatal Intensive care unit] but I wasn’t allowed. I had a lot of questions like what happens if my child gets lost? And I also came to realise that COVID is a very bad disease to the extent where it even deprives me of seeing your [my] loved ones, especially my child. (p. 10) But then, I was worried about my daughter, who was going to be with [her] and what not. She was young. So, I was scared for my baby. (p. 5) (. . .) I was not allowed to be in close proximity with my baby. (p. 3)
Stress related to other family members contracting COVID-19
There was a lot of stress and anxiety among the women related to them as well as family members contracting COVID-19 and misconceptions about disease management and causes of death. One of the participants described their parents’ death from COVID-19 as being linked to oxygen administration.
I was thinking about what happened to my parents, so I denied that administration [oxygen] they died because of oxygen. I don’t know if it’s the one that caused their death. I was scared that’s why I did not allow them to give me. (p. 16)
While another related to being in the confinement of the bedroom for fear of infecting the relatives with the disease.
In my household, we were the two of us that came out positive. So the others learnt to take care of themselves, in the beginning, we were very cautious and all that like I need to stick to my own side, like in the bedroom without moving out or anything. (p. 11)
Perceived attitudes of health care workers and support staff
Pregnant and postnatal women shared how they perceived care during their illness and admission to the hospital. For some women, it was very comfortable while for others it was not. Some women felt that they received the best care given the circumstances. For instance, one woman who was diagnosed with COVID-19 at 38 weeks and delivered uneventfully had this to say about the care: (. . .) I think it was exceptional [health care] (. . .) I feel the doctors did a very good job, in that they were also considerate knowing that okay this is someone who is breastfeeding and needed to stay alive for the baby, so they did their best. Even with the follow-ups and check-ups, even when I was at home, they continued to check up on me, the care was perfect, I can’t complain. (p. 1)
However, other women added that the care from health personnel and support staff was not so good: It was very pathetic because when I tested positive no one literally wanted to attend to us, in fact, it was a group of ladies no one wanted to attend to us, the only medicine which we had was paracetamol for the headache that I didn’t even have. I had to buy everything (. . .), it wasn’t really good. (p. 5) (. . .) sometimes the people that used to clean would not even enter our rooms [Hospital isolation rooms]; we could not even see the person cleaning but only see the mop from the door. And the people who used to dish out food would shout to ask us if we wanted to eat knowing some were even on oxygen but they would just say [call out], and the other lady we were with was on oxygen and could not wake up (. . .) the attitude was not so good. (p. 14)
Media influence
There was a mixture of negative and positive influences from the media based on the information shared. Users of social media were spreading several misconceptions around COVID-19, a phenomenon referred to as ‘infodemic’. Some information from the media negatively influenced pregnant and postnatal women as it was perceived to largely consist of reports on death tolls Jesus Christ (. . .) there [social media] it is like a funeral parlour; you don’t go there when you have COVID-19 you just get depressed. It’s scary, like the only information you get from the media about COVID-19 is death (. . .) you know it’s like every time someone mentions COVID-19 it’s death. People really don’t know or don’t think you could get better even if you are in a very severe condition, all they think is when they tell you that you have COVID-19 the next thing you think is’oh I’m dying’ yeah so I know it’s a deadly disease but they [users] should try more on encouraging peopleor letting people know that you can still get better even after testing positive for COVID-19. (p. 1) Media is a very powerful tool; it can make or break you. (p. 3) ‘Some of the information is unnecessary, some of it is necessary (. . .) some of it just scares you off. Instead of you feeling encouraged and everything, yeah. (p. 11)
For some women, media was a form of an educational platform that helped with information on the prevention of COVID-19.
I think those things [media adverts] have really helped because when it just started, we just used to hear the word COVID-19, most of us didn’t know how to take care of ourselves, it’s not everyone who was paying attention, like wear the mask, wash your hands, do this and this until after the media spread the news. We used to hear from the TV, on social media, they [adverts] are there on Facebook, Twitter and WhatsApp. It really helped everyone, those who can read and understand. Even if you don’t know how to read, you see the posters, there are posters they have stuck all over on how to take care of yourselves. I think it really helped us to be aware of this disease and how we should take care of ourselves. (p. 13) (. . .) they [health messages] were helpful as they gave me thoughts on how to prevent the spread of the virus and protect against it. I also began to warn my family members about the virus being real. So, I urged them to be careful so that we don’t have another victim from here. (p. 12)
Coping Mechanisms
COVID-19 is a new disease that has presented the public with a lot of uncertainty. During the interviews, women expressed that they had different ways to cope with the anxiety and uncertainties that came with being found with COVID-19.
I heard things saying if they catch you with COVID-19 you are going to be isolated at the isolation centre for about 2 weeks so I was trying to be calm, telling myself I am going to be fine. (p. 5)
Positive attitude
Keeping a positive attitude and constantly reminding themselves they have children to take care of were the most common coping mechanisms that participants reported using.
Apart from wanting to give life, I was still hopeful because I have another child whom I support. So, I was like I have to stay strong. (p. 9) I used to tell myself that I’d get better since other people who had it had gotten better. I really didn’t have those negative thoughts. (p. 6)
Keeping the disease secret
Some of the women opted to keep the diagnosis secret to avoid stigma from people: I never wanted to disclose it (. . .) I just wanted to keep it to myself. (p. 8) Aaaah I just kept it secret to myself and my family. (p. 4) I didn’t tell anyone; we were just staying the two of us [with my husband]. (p. 15)
Presence of Support systems
Family is an integral part of an expecting or newly delivered mother. It was noted to be one of the strongest support systems for the participants. The support given was in different forms: emotional, spiritual and financial. This helped the women feel positive about their outcomes and that of the neonate.
My grandmother is the one who gave me support. She supported me emotionally, spiritually and financially. She encouraged me a lot, and if there was a need to buy any medications; she used to buy them. And the time we were discharged, the hospital needed someone COVID-19 free to take care of my baby as I was still positive at my time of discharge. She supported me in every way she could. (p. 10) (. . .) my husband, my mother, my family has been my support system, they’ve really supported me this time (. . .) prayers, greetings, if that’s called support yes like just checking up on me every day, how my night was and all that. (p. 3).
Others reported having very supportive spouses who had to change their daily routines and even hold off work during the entirety of the illness.
It was my husband. We were completely isolated and no one came to visit us. And he was only allowed to go back for work after I was tested negative for COVID-19. And they [work place] also told him to go with his test results after my recovery. (p. 14) One said she received support from her church: ‘when I was in quarantine people would call me, laugh with me, give me that positive vibe that is needed. Even the church sometimes they would call me’.
Use of home remedies to mitigate COVID-19 symptoms
Besides the standard treatment offered to the women on an in-patient and outpatient basis, some home remedies were perceived to have helped with recovery. These remedies included drinking herbal concoctions and steaming with water and various leaves: I could steam not just using eucalyptus leaves, usually, I was given just hot water. I just make it with boiled water then they will cover me with the blanket. I just sweat, then from there I will feel okay. (p. 13) I used to eat fresh ginger, I just used to chop it then I would eat. Sometimes, I just boil ginger and lemon, then I drink and sometimes I buy a fresh one [Ginger]. Yes, then you mix them [cinnamon, lemon and ginger], those really helped. (p. 9)
Discussion
From this study, we identified major themes around psychosocial issues and coping mechanisms that pregnant and postpartum women diagnosed with COVID-19 experienced. These findings are timely as they highlight the importance of mental health support in the continuum of care for this population to mitigate adverse consequences for the mother and offspring in the midst of a pandemic. 13
A pregnant woman is generally at risk of developing postnatal mental illness due to several factors and increased levels of depression and anxiety symptoms during this period have been associated with adverse obstetric, foetal and neonatal outcomes. 14 With the emergence of COVID-19 pandemic, the psychological and mental impact on infected people has been noticeably high.15,16 Similar to our findings, data analysed from a longitudinal study conducted in the United States among pregnant and postnatal women showed that symptoms of depression and anxiety were higher during the COVID-19 pandemic compared to pre-pandemic levels. 17 The participants in the present study reported being worried about the unborn baby or neonate and were concerned about other family members contracting COVID-19. Furthermore, there was anxiety caused by the actual diagnosis of COVID-19, the isolation and detachment from the baby. In an earlier study, the pregnant women feared serious symptoms, death and had concerns about the foetus. 18 However, in another study, in a different setting, more than 50% of the 2740 pregnant participants were more stressed about social issues, such as food running out, losing a job or household income, or loss of childcare among other stressors which is quite different from the current study’s context. 19 While in another qualitative study, women had anxiety with uncertainties over the quality of obstetric health care they would receive as well as a mistrust in health professionals. 20 Coping mechanisms towards these stresses and support systems varied among our study participants as the anxiety and stressors originated from different aspects and they had varying forms of support.
In this study, two tertiary hospitals were the main COVID-19 isolation centres where pregnant and postnatal women with infection were admitted. For efficient patient management, isolation and referral to well-equipped hospitals with specialist physicians, such as these are recommended for all pregnant women with COVID-19 infection. 21 However, being treated from a third-level hospital came with mixed positive and negative perceptions of the care that they received. COVID-19 evolution brought about uncertainties in many people and health care workers and support staff had fears about handling patients with a positive test for COVID-19. In an earlier study, the perceived change in the provision of health care was not limited to pregnant and postnatal women with COVID-19 infection, but even those who did not have the infection but were pregnant. 22 With the diminished postnatal care, several women who were sick were missed and there were mixed feelings of satisfaction with care received. 22
The findings from this study highlight that pregnant and postnatal women used natural products to allay the symptoms. However, there is a paucity of literature to indicate if these products are safe for use especially for unborn babies as well as in this population. With the pandemic ravaging the globe, there has been an upsurge in the use of natural products for the treatment of COVID-19 infection in Africa. 23 In addition, there has been rising concerns about the safety of these remedies that have not undergone clinical trials like conventional medicine. 24
In a qualitative study conducted in Brazil among 22 women infected with COVID-19 during pregnancy, there were mixed feelings concerning face-to-face relationships that were reported, such as being supported and welcomed by some relations, while others experienced the exact opposite from other relations. 18 Similarly in our study, participants were stigmatized and discriminated against by both family and friends and felt isolated even when they had recovered from the infection.
Participants described the media as the main source of information about COVID-19 which was quite overwhelming. This is similar to findings in a Swedish study where pregnant women’s experiences had many uncertainties giving a feeling of being in an information echo. However, they had strong trust in maternity services despite the limited information available. 25 The WHO and governments also face the challenge of an infodemic characterized by difficulties in finding credible and trustworthy sources amid an excess of information, magnified by and information shared quickly. 26 In the heightened digitalization, the media has been used to convey valuable information, such as emerging findings and management protocols on COVID-19 which anyone around the globally can access instantly. However, the media can also act as a barrier to achieving strides in the mitigation of COVID-19 infection due to a breadth of misinformation that several people do not fact check. 27
While this study has brought out important findings on the psychosocial experiences of pregnant and postnatal women infected with COVID-19, there are some limitations. First, being a qualitative study, the results may not be transferable and only pertain to the women at the two institutions under study. Therefore, some sub-themes may be different when conducted in other settings. The study employed an interpretivist approach that is based on the provision of in-depth explanations and meanings because reality is socially constructed without hypothesis testing and generalization. 28 While the findings may not be transferable, they are still valid in this context as the first-ever study to explore maternal psychosocial issues and coping mechanisms in Zambia, hence will help policymakers to implement measures that support those infected with COVID-19. Second, because the interviews were via telephone without video conferencing, several cues could have been missed when participants responded to the questions. Literature shows that the interviewer should get non-verbal communication from participants to validate some statements. 29 Third, this study only used one type of data collection tool and lacked triangulation from multiple sources, we did not use two or more methods which could have been essential in adding credibility to the findings in this setting. 30
Conclusion
In conclusion, this study highlights the psychosocial experiences of pregnant and postnatal women with COVID-19 infection at two tertiary hospitals in Lusaka, Zambia. The greatest concern was the mental stress due to the diagnosis of COVID-19 and anticipated or actual separation from the baby and discrimination. Therefore, health care providers and support staff should treat them holistically and provide interventions that reinforce resilience. This study suggests the need for policy and clinical practice to consider the integration of effective mental health services into the provision of maternal healthobstetric and COVID-19 services.
Supplemental Material
sj-docx-1-whe-10.1177_17455057221111326 – Supplemental material for Psychosocial issues and coping mechanisms of pregnant and postnatal women diagnosed with COVID-19: A qualitative study
Supplemental material, sj-docx-1-whe-10.1177_17455057221111326 for Psychosocial issues and coping mechanisms of pregnant and postnatal women diagnosed with COVID-19: A qualitative study by Jane Chanda Kabwe, Mwansa Ketty Lubeya, Christabel Chigwe Phiri, Mubanga Mulenga, Ntungo Siulapwa, Patrick Kaonga, Joan T. Price, Selia Ng’anjo Phiri and Choolwe Jacobs in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057221111326 – Supplemental material for Psychosocial issues and coping mechanisms of pregnant and postnatal women diagnosed with COVID-19: A qualitative study
Supplemental material, sj-docx-2-whe-10.1177_17455057221111326 for Psychosocial issues and coping mechanisms of pregnant and postnatal women diagnosed with COVID-19: A qualitative study by Jane Chanda Kabwe, Mwansa Ketty Lubeya, Christabel Chigwe Phiri, Mubanga Mulenga, Ntungo Siulapwa, Patrick Kaonga, Joan T. Price, Selia Ng’anjo Phiri and Choolwe Jacobs in Women’s Health
Footnotes
Acknowledgements
The authors would like to thank the following research assistants: Mable Ndambo, Anthony Limbumbu, Kasakula Kaunda, Theresa Shema Nzayinsenga and Caren Chizuni for their technical support during data collection period.
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study received no research funding, however, part of MKLs time is supported by TESA III-NoE project funded by EDCTP (grant number: CSA2020NoE-3104) and the UNC-UNZA-Wits Partnership for HIV and Women’s Reproductive Health (grant number: D43 TW010558). JTP is supported by the US National Institutes of Health (K01 TW010857).
Data availability statement
Transcribed de-identified verbatims and codebook are available upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.