
Abstract
Hypertensive disorders of pregnancy are one of the leading causes of poor pregnancy outcomes and are associated with increased rates of maternal mortality, preterm birth, small for gestational age newborns, stillbirth, and neonatal death. The overall and type-specific prevalence of hypertensive disorders of pregnancy and associated pregnancy outcomes are unknown in Sub-Saharan Africa. Therefore, this review aimed to identify the prevalence of hypertensive disorders of pregnancy and associated pregnancy outcomes in Sub-Saharan Africa. A systematic review and meta-analysis were conducted on observational facility-based studies irrespective of publication status, sample size, language, and follow-up duration from 19 countries between the years 2000 and 2018 in Sub-Saharan Africa. A review of studies using PubMed, EMBASE, African Index Medicus, and African Journals Online was completed with independent extraction of studies by review authors using the predefined inclusion criteria. Quality and risk of bias of individual studies were assessed using the Joanna Briggs Institute Checklist. Random effects model was used to estimate the pooled prevalence of hypertensive disorders of pregnancy and type-specific hypertensive disorders of pregnancy. A pooled adjusted odds ratio with 95% confidence interval for each study was calculated using comprehensive meta-analysis version 2 software to estimate the association of hypertensive disorders of pregnancy and its outcomes. The existence of heterogeneity was assessed using I2 and its corresponding P value. We assessed the presence of publication bias using the Egger’s test. Subgroup analysis was performed to assess the potential effect of variables, and a sensitivity analysis was conducted to assess any undue influence from studies. The analysis included 70 studies. The pooled prevalence of hypertensive disorders of pregnancy (all types combined), chronic hypertension, gestational hypertension, preeclampsia, and eclampsia were 8% (95% confidence interval = [5, 10]), 0.9% (95% confidence interval = [0.4, 1.8]), 4.1% (95% confidence interval = [2.4, 7]), 4.1% (95% confidence interval = [3.2, 5.1]), and 1.5% (95% confidence interval = [1, 2]), respectively. Compared with normotensive pregnant or postpartum women, women with hypertensive disorders of pregnancy were associated with increased risk of maternal mortality, odds ratio = 17 (95% confidence interval = [9.6, 28.8]); cesarean section, odds ratio = 3.1 (95% confidence interval = [1.7, 5.6]); perinatal mortality, odds ratio = 8.2 (95% confidence interval = [2.8, 24]); low birth weight, odds ratio = 3.2 (95% confidence interval = [2, 5]); and preterm delivery, odds ratio = 7.8 (95% confidence interval = [2.5, 25.3]) according to this analysis. The pooled prevalence of hypertensive disorders of pregnancy was high in Sub-Saharan Africa compared to those reported from other regions. Pregnant or postpartum women with hypertensive disorders of pregnancy have increased risk of maternal mortality, cesarean section, preterm delivery, perinatal mortality, and low birth weight newborn. Therefore, creating awareness of the risks of hypertensive disorders of pregnancy is essential. Pregnant women with hypertensive disorders need due attention to manage appropriately and more importantly to have favorable outcomes in this population.
Background
Globally, over the past 25 years, the maternal mortality ratio (MMR) has decreased by almost 44%, from 385 maternal deaths per 100,000 live births in 1990 to an estimated 216 maternal deaths per 100,000 live births in 2015. 1 Approximately 99% of the global maternal deaths in 2015 are from low- and middle-income countries (LMICs), with Sub-Saharan Africa (SSA) alone accounting for roughly 66%. 2 In many regions of the world, maternal mortality has declined, but it has increased in 50 countries and 27 of which are in SSA. 3 According to a recent report from the World Health Organization (WHO), in some African settings, hypertensive disorders of pregnancy (HDP) are the leading cause of maternal mortality. 4 HDP are multisystem disorders, which include gestational hypertension, chronic hypertension, superimposed preeclampsia on chronic hypertension, and preeclampsia.5,6 They contribute to 14% and 16% maternal mortality worldwide and in SSA, respectively. 7
In addition, HDP also contribute to adverse fetal outcomes. 8 HDP increase the risk of preterm birth, stillbirth, small for gestational age, and neonatal death, 9 and expose the mother to an emergency cesarean section, which increases the risk of low birth weight infants and neonatal death. 10
Globally, 2.73% of women suffer from HDP while the incidence of chronic hypertension, preeclampsia, and eclampsia are 0.29%, 2.16% and 0.28%, respectively. 11 However, in Africa, a relatively higher prevalence of HDP is reported, as it affects 1 in 10 women. 12 Furthermore, there is concern that recent reports on the global burden of HDP underrepresent SSA populations, indicating the importance of further research addressing HDP among this population. 13 The burden of hypertension has been increasing over the past few decades in SSA; however, a large percentage of the population with hypertension remains untreated, ineffectively treated, or even undiagnosed, contributing to the growing cardiovascular disorder problem in this region. 14
Little is known about the prevalence of HDP in SSA despite widespread investigation in high-income countries. 4 Hence, to the best of our awareness, we conducted the first systematic review and meta-analysis to estimate the overall and type-specific prevalence of HDP and associated pregnancy outcomes in SSA, to educate policymakers and guide strategies for early detection, prevention, and management of these disorders in the region. Therefore, the aim of this systematic review and meta-analysis was to determine the prevalence of HDP in SSA and investigate associated adverse pregnancy outcomes.
Methods
Eligibility criteria
Any observational facility-based study conducted to determine prevalence and/or adverse pregnancy outcomes of any type of HDP in SSA from 2000 to 2018 was included.
All observational studies (cohort and cross-sectional) were included regardless of publication status, sample size, language, or follow-up duration. The inclusion criteria comprised of the following: (1) facility-based studies; (2) sampling of a defined population or studies involving entire populations; (3) involving pregnant or postpartum participants; (4) reporting on the prevalence of chronic hypertension, superimposed preeclampsia, gestational hypertension, preeclampsia, and/or eclampsia and/or their pregnancy outcomes in a population of pregnant or postpartum women residing in SSA countries; and (5) defined HDP as blood pressure greater than 140/90 mm Hg 15 or urine protein and elevated blood pressure above 140/90 mm Hg. Studies that did not meet the inclusion criteria were excluded. Longitudinal studies where prevalence of HDP or pregnancy outcomes were not determined were also excluded. In addition, case-control studies from pooled prevalence of HDP were also excluded from the analysis to minimize bias.
Information sources and search
A literature search was undertaken using the databases PUBMED and EMBASE. Studies were also retrieved by searches of African Index Medicus and the African Journals Online (AJOL) using all possible key subject headings. In addition to searching databases, supplementary approaches to identifying studies such as hand-searching of journals, checking reference lists, searching websites, and contacting authors were performed. MeSH and free text terms were used to increase sensitivity to potentially appropriate studies. When MeSH terms were not used (websites), search terms were recognized, and all possible substitutes and spellings were found and used in the search strategy.
The following search terms were used: prevalence, proportion, magnitude, epidemiology, hyperten$, “chronic hypertension,” hypertension, blood pressure, “high blood pressure,” preeclampsia, preeclampsia-eclampsia, pre-eclampsia-eclampsia, pre-eclampsia, eclampsia, preeclampsia superimposed, pre-eclampsia superimposed, superimposed preeclampsia, superimposed pre-eclampsia, pregnancy induced hyperten$, hypertension, pregnancy induced, hyperten$ disorders of pregnancy, hypertensive disorders in pregnancy, gestational hyperten$, gestational hypertension, hyperten$ gestational, pregnancy outcome, outcome of pregnancy, maternal mortality, maternal death, death of mother, perinatal mortality, perinatal death, stillbirth, small for gestational age, low birth weight, cesarean section, cesarean birth, prematurity, premature birth, preterm, preterm delivery, preterm labor, preterm birth, and Sub-Saharan Africa.
The search strategy for each database is available in Tables S1 and S2. The reference list of all relevant review papers was scrutinized to identify other potential data sources. The search, which was performed and overseen by two review authors (K.S.G. and N.A.), was restricted to studies in humans published between January 2000 and November 2018. Specific search terms, inclusion and exclusion criteria, searched databases, and eventual data needed to be collected and reported were considered during searching. The review authors collaborated, and consensus was needed throughout the process, with continued discussions on steps of searching during the review.
Study selection
Eligibility assessment of selected studies was performed independently by two authors (K.S.G. and N.A.) in two phases. First, titles and abstracts of retrieved literature were reviewed to check for eligibility for the second phase, which consists of full-text screening. During this phase, the authors further screened for eligibility to include in the study. Disagreements between the two reviewers were resolved by consensus and/or resolved through discussion with the third review author (B.M.).
Data collection process
First review author (K.S.G.) extracted the data from the eligible studies, which was then kept on a data extraction sheet and checked by the second review author (N.A.). Disagreements were resolved by the discussion between the two review authors, otherwise the third review author (B.M.) decided. The studies were checked for duplication based on name of authors, sample size, outcomes, and study location. Data on year of study, country of study, study design, type of HDP, sample size, blood pressure measurement, definition(s) used for HDP, and prevalence of HDP were extracted.
All citations identified by electronic databases and manual searches were organized, duplicates deleted, and each citation assigned a unique identification number. All extracted data were stored in a Microsoft Excel file format. PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) guidelines were used for all procedures and reporting. 16
Data items
The participants were pregnant or postpartum women (population) with HDP (condition) in SSA (context). Pregnant or postpartum women (population) who are diagnosed with HDP (exposure) and normotensive pregnant or postpartum women (control) were seen for associated adverse pregnancy outcomes (outcome) in SSA.
The prevalence of HDP is the primary outcome of this study. The classification of HDP includes chronic hypertension, gestational hypertension, preeclampsia—de novo or superimposed on chronic hypertension and white coat hypertension.17–19 Hypertension in pregnancy is defined as a systolic blood pressure (SBP) of 140 mm Hg or more and/or diastolic blood pressure (DBP) of 90 mm Hg or more on two or more consecutive occasions during pregnancy. 18 Gestational hypertension is an elevation of SBP greater than or equal to 140 mm Hg and DBP greater than or equal to 90 mm Hg without proteinuria in a previously normotensive non-proteinuria pregnant woman after 20 weeks of pregnancy.18,19
Preeclampsia is defined as women who develop both hypertension and proteinuria in pregnancy after 20 weeks of gestation. 18 In this review, any forms of preeclampsia were included as preeclampsia (i.e. severe preeclampsia, mild preeclampsia, and superimposed preeclampsia). Eclampsia is the occurrence of convulsions or fit with SBP of >140 mm Hg and DBP of >90 mm Hg after 20 weeks of gestation, proteinuria of >2+, and signs and symptoms of severe preeclampsia.20,21 Chronic hypertension is defined as high blood pressure predating the pregnancy or recognized at less than 20 weeks of gestation. 22
Preeclampsia superimposed on chronic hypertension refers to a sudden increase in blood pressure and new onset of proteinuria in women with hypertension and no proteinuria in early pregnancy (less than 20 weeks of gestation). 23
The HDP definition was either reported by authors, in which case we depend on it; or we pooled data from eligible studies reporting on at least three of the four entities of HDP (i.e. chronic hypertension, gestational hypertension, preeclampsia/eclampsia, and superimposed preeclampsia/eclampsia) to acquire a rough approximation of the general prevalence of overall HDP in SSA, as limited studies reported an overall prevalence of HDP (four combined entities). 12 Specific HDP in this review was each type of HDP-like chronic hypertension, gestational hypertension, preeclampsia, or eclampsia.
The secondary outcomes of this analysis include maternal mortality, cesarean section, perinatal mortality, preterm delivery, and low birth weight. Maternal mortality is defined as the death of a pregnant woman or death within 42 days of termination of pregnancy, irrespective of site and the duration of the pregnancy, from any cause related to or intensified by the pregnancy or its management but not from unintentional or incidental causes.
24
Cesarean section/birth is the delivery of a baby through incisions made in the mother’s abdomen and uterus. 25 Perinatal mortality includes stillbirths (fetal loss after 28 weeks of gestation) and neonatal deaths (during first 7 days of life). 26 Premature delivery is when birth occurs between 20 and 37 weeks of gestation. 27 Low birth weight has been defined by the WHO as birth weight less than 2500 g 28 with infants whose weight is less than the 10th percentile for gestational age classified as small for gestational age. 29
Quality and risk of bias assessment
Quality and risk of bias of studies were assessed using the Joanna Briggs Institute assessment based on the Critical Appraisal Checklist for Studies Reporting Prevalence Data 2017. The study evaluated the quality of all included studies in accordance with the nine criteria. The criteria have a rating scale of 0, 1, and 2. 30 Depending on the score achieved (from 0 to 18), studies were categorized as being high (>14), medium (11–14), or low (<11) quality. 31 The review authors performed an assessment of the risk of bias independently and any studies which did not fulfill minimum criteria (low quality) were excluded from the meta-analysis.
Statistical analysis
The study used baseline data for cohort studies and the total number of pregnant women reported during a given period. Using studies which reported pregnancy outcomes, an unadjusted odds ratio (OR) with 95% confidence interval (CI) was calculated using comprehensive meta-analysis version 2 package. In addition to overall pooled prevalence for all forms of HDP, subgroup and sensitivity analysis was also performed. Considering the “synthesis of results,” the raw proportion was transformed into a suitable unit for meta-analysis using logit transformation. A random effects model was used to account for possible heterogeneity between studies, which defaults to the fixed effects model approach in the absence of heterogeneity to obtain an overall summary estimate of the prevalence across studies and pooled study-specific estimates. 32 The P value of less than 0.05 was considered a significant association between HDP and pregnancy outcomes. Statistical heterogeneity was evaluated with the Cochran chi-square (χ2), and I2 statistic 33 (low <25%, moderate 25%–50%, high >50%) was computed with its corresponding P value.
Risk of bias across studies
The study assessed the possibility of publication bias using Egger’s linear regression test as formal statistical test for publication bias. 34 A P value of less than 0.10 on the Egger’s test was considered indicative of statistically significant publication bias.
Additional analyses
Subgroup analysis was conducted by specific types of HDP, design, and regions of SSA. Furthermore, the degree to which the main findings of a review were affected by changes in the methods or in the data used from individual studies was explored by the sensitivity analysis. The sensitivity analysis was also done considering diagnostic criteria, high prevalence, and wide CI.
Results
Study characteristics
The literature search identified 1327 references through PubMed database and 3784 through EMBASE database (Figure 1). An additional 79 studies were found from African Index Medicus and AJOL. Following the removal of duplicates, 262 records were screened for relevance by reviewing the title and abstract. As a result, 99 full-text articles were assessed against the inclusion criteria. Consequently, 29 studies were excluded, including 9 studies which presented results differently, 6 community-based studies, 5 studies without prevalence and pregnancy outcomes of HDP, and 7 studies with no clear diagnostic criteria for HDP. Thus, 70 full-text studies remained for analysis (Table 1).
Summary of literature search for prevalence of hypertensive disorders of pregnancy in Sub-Saharan Africa.
Summary characteristics of studies on hypertensive disorders of pregnancy in Sub-Saharan Africa..
BP: blood pressure; SBP: systolic blood pressure; DBP: diastolic blood pressure; ISSHP: International Society for the Study of Hypertension in Pregnancy; HDP: hypertensive disorders of pregnancy; GH: gestational hypertension.
There were studies that used only DBP for diagnosis of HDP20,35–37 and other studies that used DBP cutoff of 80 mm Hg instead of 90 mm Hg.38,39 There were studies that included severe preeclampsia (DBP > 110 and proteinuria).37,40,41 Some studies used international organization diagnostic criteria (e.g. European Society of Hypertension and WHO standard),42–44 while eclampsia was also diagnosed based on the presence of hypertension/preeclampsia and convulsion in others.45–49 Since we retained the aforementioned studies, their effect on heterogeneity of meta-analysis was seen during subgroup and sensitivity analysis.
The characteristics of the cross-sectional,9,35,36,40,42,46–89 prospective, or retrospective cohort and longitudinal studies5,10,37–39,41,90–103 included in this review from 19 Sub-Saharan African countries are summarized in Table 1. The majority of studies were conducted in Nigeria, Ethiopia, and Tanzania, which are 21, 16, and 6, respectively. The majority of studies that included in the analysis were completed within 3 years of study period. The sample size of the studies ranged from 100 in Zanzibar 69 to 249,771 in Zambia, 38 with a total of 780,469 participants. Overall, 29,980 (3.8%) pregnant women from a total of 780,469 study participants were recorded as suffering from disorders during antepartum and/or intrapartum period.
Many studies consisted of retrospective record review with consecutive sampling of women at various stages of pregnancy till 6 weeks postpartum. The studies have reported overall HDP (Table 1), chronic hypertension, gestational hypertension, preeclampsia,41,72,84–86,94,104 and eclampsia.47,49,59,60,63,65,66,75,76,78,103,105–108
Prevalence of HDP
The pooled prevalence of HDP (all types combined) was 8% (95% CI = [6, 10]; Figure 2). The most common forms of specific HDP were preeclampsia and gestational hypertension with a prevalence of 4.1% (95% CI = [3.2, 5.1]; Figure 3) and 4.1% (95% CI = [2.4, 7]; Figure 4), respectively. The less common types of specific HDP were chronic hypertension (0.9%; 95% CI = [0.4, 1.8]; Figure 5) and eclampsia (1.5%; 95% CI = [1.1, 2]; Figure 6). Although there was substantial heterogeneity (Table 2), no publication bias was found for overall and type-specific HDP.

Meta-analysis of prevalence of overall hypertensive disorder of pregnancy.

Meta-analysis of prevalence of preeclampsia.

Meta-analysis of prevalence of gestational hypertension.

Meta-analysis of prevalence of chronic hypertension.

Meta-analysis of prevalence of eclampsia.
Summary statistics of the prevalence of hypertensive disorders of pregnancy in Sub-Saharan Africa.

I2: heterogeneity; HDP: hypertensive disorders of pregnancy.
Subgroup analysis
Subgroup analysis of HDP by design and region revealed substantial heterogeneity across the studies in terms of HDP prevalence (I2 > 83%, P < 0.0001). There was a tendency for study-specific prevalence to vary by study design and region, with the cross-sectional and western SSA studies reporting significantly higher prevalence (P < 0.0001).
Subgroup analysis of HDP prevalence by SSA region showed a significantly higher pooled prevalence in west (2%; 95% CI = [1.3, 2.9] for eclampsia) and central (6.7%; 95% CI = [3.1, 13.8] for preeclampsia) SSA. The subgroup analysis by study design also revealed high pooled prevalence in cross-sectional (3.1%, 95% CI = [2.9, 3.3] for chronic hypertension; 4.7%, 95% CI = [3.5, 6.1] for preeclampsia; and 1.6%, 95% CI = [1.2, 2.3] for eclampsia) and cohort (5.7%, 95% CI = [2.8, 11.2] for gestational hypertension) study designs. The lowest prevalence estimates were observed in eastern (0.5%, 95% CI = [0.1, 2.3] for chronic hypertension; 1.5%, 95% CI = [0.6, 3.8] for gestational hypertension; and 3.6%, 95% CI = [2.5, 5.3] for preeclampsia) and southern (1%, 95% CI = [0.5, 1.7] for eclampsia) SSA (Table 3).
Subgroup analysis of prevalence of hypertensive disorders of pregnancy by study design and regions in Sub-Saharan Africa.

CI: confidence interval; CH: chronic hypertension; SSA: Sub-Saharan Africa; GH: gestational hypertension.
The studies in the analysis included a mix of cross-sectional, prospective, or retrospective cohort and longitudinal studies; prospective and longitudinal studies reported on the prevalence of various HDP outcomes. The analyses were accomplished by consecutively omitting one study at a time to endorse the results. Sensitivity analysis was completed using diagnostic criteria, sample size, and width of CI, although change in heterogeneity was insignificant.
The meta-regression indicates that the number of publications on HDP is increasing which shows that hypertensive disorders are currently receiving attention (Figure 7). This is aligned with the current shift of attention to non-communicable diseases such as hypertension and cardiovascular disease specifically in the LMICs.
Meta-regression of studies on hypertensive disorders of pregnancy by year of publication in SSA.
Pregnancy outcomes of HDP
The meta-analysis shows that maternal mortality was significantly associated with HDP, OR = 17 (95% CI = [9.6, 28.8]) with homogeneity among the studies’ findings, I2 = 0.000, P = <0.000152,56,65,109–111 (Figure 8).
Forest plot displaying maternal mortality associated with hypertensive disorders of pregnancy in SSA.
The meta-analysis also showed pregnant women with hypertensive disorders were more likely to have cesarean section compared to normotensive pregnant women, OR = 3.1 (95% CI = [1.7, 5.6]). However, there was high heterogeneity among the studies, I2 = 86.45%, P = <0.000144,109,110,112 (Figure 9).

Forest plot displaying cesarean section among women with hypertensive disorders of pregnancy in SSA.
Perinatal mortality was significantly associated with HDP, OR = 8.2 (95% CI = [2.8, 24]), although the meta-analysis revealed large heterogeneity, I2 = 96.9%, P = <0.000144,65,82,109,112 (Figure 10).
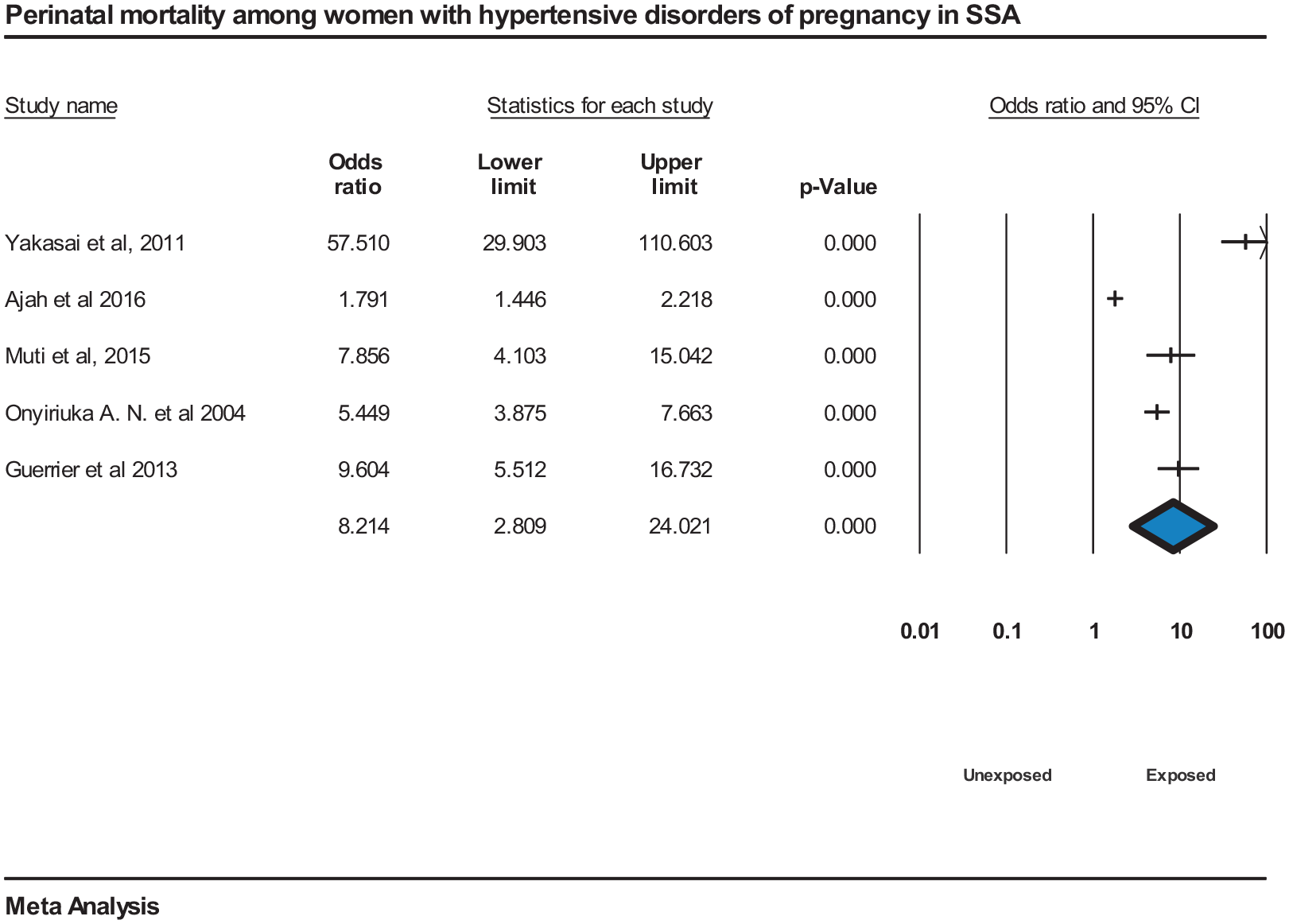
Forest plot displaying perinatal mortality among women with hypertensive disorders of pregnancy in SSA.
The pooled risk of having a low birth weight newborn was high among women who have HDP compared to normotensive pregnant women, OR = 3.2 (95% CI = [2, 5]). However, the meta-analysis revealed high heterogeneity among the studies, I2 = 57.7%, P = 0.00019,109,111 (Figure 11).

Forest plot displaying low birth weight newborn among women with hypertensive disorders of pregnancy in SSA.
HDP have significant pooled association with preterm delivery, OR = 7.8 (95% CI = [2.5, 25.3]), though the meta-analysis of studies had high heterogeneity, I2 = 84.34%, P = 0.001.52,113,114
Publication bias
There was no evidence of publication bias across studies reporting on the prevalence of HDP, chronic hypertension, gestational hypertension, and preeclampsia with the Egger’s test for bias giving a P value of 0.27, 0.10, 0.33, and 0.11, respectively. However, there was some indication of publication bias across studies reporting on eclampsia prevalence, with the Egger’s test for bias giving a P value of 0.037 (Table 2).
Duval and Tweedie’s trim and fill analysis using the random effect model analysis was performed for overall HDP, chronic hypertension, gestational hypertension, preeclampsia, and eclampsia. The adjusted values were zero to the right or left of the mean for overall HDP, gestational hypertension, and preeclampsia, and 2 to the left of the mean and 4 to the right of the mean for chronic hypertension and eclampsia, respectively, although insignificant.
Discussion
This meta-analysis confirms that HDP are associated with adverse pregnancy outcomes. Maternal and fetal complications increase with HDP; however, appropriate maternal and perinatal care can prevent adverse outcomes such as eclampsia, maternal and perinatal death.
The overall prevalence of HDP was 8% in SSA which is in line with global estimates (5.2%–8.2%), 13 slightly lower than a review from Africa (10%), 12 and higher than the pooled prevalence of HDP in Ethiopia (6.1%). 115 This may be due to sample size differences, inclusion criteria, and vast geographical differences. The finding is also higher than the global secondary analysis of the WHO’s multicountry survey prevalence of 2.7%. 11 The difference might be due to variability in maternal risk factors, socio-demographic factors, and the difference in prenatal care service utilization. Most studies were facility-based from the record review, which may result in inflated numbers. Due to poor health-seeking behavior, women typically present late and with advanced disease states in SSA that contributed to high maternal and perinatal morbidity and mortality.7,12,116 Furthermore, there may be delayed and lack of intervention due to poor infrastructure. As a result, most studies had a relatively high prevalence of eclampsia that affected overall pooled analysis.
The pooled prevalence of preeclampsia was 4.1% in SSA, and this finding is in line with the prevalence of preeclampsia in Africa (5.3%), 12 the United States (3%–5%),117,118 and global estimate (1.8%–4.4%). 13 The pooled prevalence of eclampsia was 1.5% according to this review, which is similar to a review performed in Africa (1.47%) 12 and global estimates (0.2%–9.2%), 13 but slightly higher than a survey performed in China (0.9%) and WHO multicountry survey prevalence of 0.3%. 11 The difference may be due to racial differences since this study focused on Sub-Saharan African countries.12,119–121 Furthermore, the variation may be attributed to differences in ethnic background, age distribution, socioeconomic status, parity, and study methodology. The pregnant women in SSA may have presented immediately with convulsions and right away diagnosed with eclampsia and no diagnosis ever of high blood pressure or anything. Estimates also varied substantially according to the SSA region, with a significantly higher prevalence of HDP among women in central and western SSA compared to other parts of SSA.
There was high heterogeneity between studies which showed an insignificant decrease when subgroup analysis was performed. However, the meta-analysis did not identify any other underlying causes of heterogeneity, suggesting that either populations with HDP are varied or the determination of HDP and outcomes may not be consistent. Meanwhile, it might be due to differences in geographical locations, diagnostic and measurement methods of disorders, socioeconomic status, and sample size. Hence, it also highlights the necessity to standardize HDP definition in SSA. 12
The meta-analysis has shown that maternal mortality has a significant association with HDP. Mothers with hypertensive disorders were more exposed to maternal mortality and morbidities as compared to those who were not affected. 51 Moreover, according to the studies in 29 countries from Africa, Asia, Latin America, and the Middle East, the risk of death was nearly four times higher for women with preeclampsia than non-preeclamptic women, and for those with eclampsia, the risk increased exponentially. 11
Women with HDP are more likely to have a cesarean section compared to normotensive pregnant women and significant pooled association indicates increased perinatal mortality. Similarly, the studies have shown the risk of fetal and neonatal deaths, as well as preterm birth and admission to a Neonatal Intensive Care Unit were increased in both preeclampsia and eclampsia. 11
The pooled risk of preterm delivery and low birth weight newborn was high among women with HDP compared to normotensive pregnant women. Similarly, the studies have shown the more significant the severity of hypertension, the increased risk of complications associated with the pregnancy, and the greater the possibility of pregnancy termination.122,123 HDP are associated with prematurity (which may be iatrogenic) and low birth weight even when corrected for gestation, 124 which is in line with the analysis of this study.
The pooled ORs of HDP and cesarean section, perinatal mortality, low birth weight, and preterm delivery have shown high heterogeneity. The geographic differences, ethnicity, socioeconomic status, adjustment for confounding, sampling error (within and between), and design aspects may contribute.
These findings have important policy implications for the treatment of HDP and pregnancy outcomes in SSA. The strong influence of HDP on maternal mortality, cesarean section, perinatal mortality, low birth weight, and preterm birth suggests that safe motherhood programs need to explore applicable methods of increasing maternal service utilization among women of reproductive age, pregnant mothers, and mothers diagnosed with HDP in SSA. The review has revealed that preeclampsia and eclampsia prevalence is high. Therefore, attention should be given to improving women’s health-seeking behavior, preeclampsia and eclampsia management protocol adherence. This calls for a rigorous evaluation of the effectiveness of existing antenatal and intranatal care programs in which prevention and management of HDP will be undertaken in SSA to identify gaps in policy and program implementation. Targeted interventions to strengthen the infrastructure of antenatal and intranatal care both for women and newborns should be considered.
Duval and Tweedie’s trim and fill analysis using the random effect analysis showed adjusted values of 2 to the left and 4 to the right of the mean for chronic hypertension and eclampsia, respectively, although non-significant. Publication bias may be due to difficulty in accessing gray literature in SSA and less publication of non-significant results. In the analysis, checking study quality, sensitivity analysis, and acknowledging potential sources of bias were completed.
“Strengths and weaknesses” of study
Studies were carefully selected according to a rigorous search strategy to enable unbiased inclusion of retrospective or prospective studied cohorts and cross-sectional studies. These studies were included if they calculated prevalence/proportion or mentioned pregnancy outcomes.
Despite the selection of relevant and appropriately performed studies, there was a range of reported incidences of HDP. There was difficulty in selecting studies of (any type of) HDP and compiling the relevant data, particularly because HDP include various types of disorders and individual studies did not always assess every type. As a result, the overall prevalence of HDP may be liable to bias. There may also be bias due to differences in the selection of women studied, difficulties in measuring HDP, and true differences within the population of women. In addition, the authors failed to define the control group in the studies.
Most papers did not report relevant baseline demographics defining the studied population and this was not considered in the meta-analysis, which limited the assessment of confounders. Coexisting factors including maternal age and ethnicity, recognized to be associated with both HDP and adverse pregnancy outcome, may contribute to confounding, but their relative effects are unknown. Few studies in the meta-analysis reported control data, so a direct comparison of outcomes between women with HDP and normotensive women was not possible. We found substantial heterogeneity which may be partly explained by characteristics of the studies shown by subgroup analysis. The included studies were facility-based that may have a slightly elevated proportion of HDP compared to population-based study; hence, the findings may not represent true prevalence in the community. Also, a significant proportion of studies that included data with HDP and pregnancy outcomes were retrospective studies.
Conclusion
The overall pooled prevalence of HDP was high compared to those reported from other regions. The meta-analysis indicates that HDP are associated with maternal mortality and cesarean section as well as adverse pregnancy outcomes such as preterm delivery, low birth weight, and perinatal mortality.
The meta-analysis supports the importance of increased antenatal surveillance for women with HDP to enable early identification of complications. Women should receive counseling to optimize their health during pregnancy and to inform them of the increased maternal and fetal risks associated with their hypertension. Strategies to predict those at greatest risk of HDP, determine optimal drug treatments, and reduce adverse pregnancy outcomes are needed.
Supplemental Material
sj-pdf-1-whe-10.1177_1745506520973105 – Supplemental material for Prevalence of hypertensive disorders of pregnancy and pregnancy outcomes in Sub-Saharan Africa: A systematic review and meta-analysis
Supplemental material, sj-pdf-1-whe-10.1177_1745506520973105 for Prevalence of hypertensive disorders of pregnancy and pregnancy outcomes in Sub-Saharan Africa: A systematic review and meta-analysis by Kasiye Shiferaw Gemechu, Nega Assefa and Bizatu Mengistie in Women’s Health
Footnotes
Acknowledgements
We would like to acknowledge all the authors of the studies included in this review. We also thank Abdulbasit Musa for unreserved support, and Ogbudu Emmanuel for language edition. Finally, we appreciate Tara Wilfong and Rosanna Glazik for their constructive comments and language edition.
Author contributions
All authors involved in the design, selection of articles, data extraction, statistical analysis, and manuscript writing. All authors read and approved the final draft of the manuscript.
Availability of data and materials
All data pertaining to this study are contained and presented in this document.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.