
Abstract
Background:
Male involvement in family planning includes not only using contraceptives but also encouraging and supporting their partners’ contraception needs and choices, encouraging peers to use family planning, and influencing policy to make male-related programs more conducive. In Ethiopia, the prevalence and associated factors of male involvement in family planning were highly inconsistent across studies. As a result, the goal of this study was to use a systematic review and meta-analysis to estimate the pooled prevalence of male involvement in family planning and its associated factors in Ethiopia.
Methods:
Electronic literature search using PubMed, Google Scholar, EMBASE, HINAR, Scopus, and Web of Sciences were performed without time restriction to identify the primary studies. Data were extracted using a pretested standardized data extraction format and analyzed using STATA 14 statistical software. A random-effect model was used to estimate the pooled prevalence of male involvement.
Results:
A total of 17 studies were included to give the pooled prevalence of male involvement in family planning in Ethiopia, which was 39.66% (95% confidence interval = 29.86, 49.45). Educational status (adjusted odds ratio = 1.99, 95% confidence interval = 1.26, 3.14), discussion of family planning with wife (adjusted odds ratio = 4.15, 95% confidence interval = 2.21, 7.80), knowledge (adjusted odds ratio = 1.83, 95% confidence interval = 1.26, 2.64), positive attitude about family planning (adjusted odds ratio = 2.57, 95% confidence interval = 1.70, 3.90), and approval of contraceptive use (adjusted odds ratio = 2.57, 95% confidence interval = 1.70, 3.90) were found to be significantly associated with involvement of men in family planning service.
Conclusion:
The overall prevalence of male involvement in family planning in Ethiopia was significantly low. Male involvement in family planning should be made available, accessible, and advocated for by government and non-governmental organizations, service providers, program planners, and stakeholders. In addition, to increase the role of men in the use of family planning services, a conducive environment for education, behavioral change, and open discussion about reproductive health issues is required.
Introduction
Men are often the primary decision-makers on family size and their partner’s use of family planning (FP) methods, even though contraceptive methods and services are frequently geared toward women. 1 Furthermore, spousal disagreement can act as a deterrent because women may be hesitant to bring up the subject of FP. 2
Men have historically been devalued in receiving and disseminating information about sexuality, reproductive health (RH), and birth spacing. Many FP programmers have neglected or precluded them in some way because FP is seen as a woman’s affair. Women were not seen as decision-makers, but rather as implementers of what men had agreed, without questioning the men’s choices. 3
Men’s involvement in RH has grown in popularity since the 1994 International Conference on Population and Development (ICPD). Evidence suggests that increased spousal interaction can lead to contraceptive uptake when men are involved.4,5 Male participation in FP has become a big topic among RH program designers, policymakers, and population researchers recently. 6
In developing countries, increasing the availability of FP services and improving their use could prevent up to 42% of maternal deaths. 7 Maternal and child health (MCH) centers provided the majority of FP services. The majority of studies and public awareness campaigns focused on women, assuming that women are the ones who bear children. This emphasis on women has reinforced the perception that FP is primarily a woman’s responsibility, with the man playing only a minor role. 8
Male involvement in RH service utilization encompasses how men accept and express support for their partners’ needs, choices, and rights, including the use of contraception and their own reproductive and sexual behavior to promote human rights observance and the need to enforce equity. 9
In Ethiopia, a number of primary studies were conducted in order to estimate male participation in FP.10–26 According to the reports, at the national level, there is a significant variation in the level of FP involvement among males, ranging from 8.4% 13 to 68.1%. 12 The cause of these disparities in male involvement in FP among Ethiopian men has yet to be determined. As a result, estimating the pooled prevalence of male involvement and associated factors is critical in order to identify existing gaps and make suggestions for strategies that increase male participation while reducing the burden on women from contraceptives, unmet needs, and unintended pregnancies. Ethiopia’s population policy prioritizes expanding FP services through clinical and community-based interventions in order to achieve a contraceptive prevalence rate (CPR) of 65% by 2015. It also entails encouraging men to engage in a variety of beneficial RH and social behaviors in order to ensure the well-being of women and children. 27 Despite this, there have been a few attempts to engage men in reproductive issues. As a result, the findings of this study will be used as a benchmark for policymakers and program planners when it comes to incorporating males into FP programs and strategies.
Methods
Protocol registration
The purpose of this study was to estimate the pooled prevalence rate of male involvement in FP utilization in Ethiopia using a systematic review and meta-analysis. It was submitted to the prospective international registry of systematic reviews (PROSPERO no. CRD42021260084). It was done in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) checklist guidelines. 28
Eligibility criteria
Inclusion criteria
The review included married men whose wives were of reproductive age and lived in Ethiopia. Married men from a variety of socioeconomic backgrounds, ethnic groups, and dialects were also included. All published and unpublished observational (cross-sectional) studies that evaluated male involvement in FP and factors affecting their involvement up to 15 June 2021 were included.
Exclusion criteria
The review excluded articles written in languages other than English, qualitative papers, case studies, and secondary works (e.g. review articles, commentaries, editorials, and unpublished conference abstracts).
Searching strategy and data source
The primary studies were identified by searching PubMed, Google Scholar, EMBASE, HINAR, Scopus, and Web of Sciences without regard for time constraints. Gray literature was also searched in online repositories at universities and research institutes. Initially, the full titles (male involvement in FP and associated factors among married men in Ethiopia) were examined, and then the following terms and phrases (“Male” OR “male partner” AND “involvement” OR “participation” AND “family planning” OR “family planning utilization” AND “associated factors” OR “predictors” OR “determinants” AND “married men” AND “Ethiopia”) were searched (Additional file 1).
Identification and study selection
All identified studies were imported into the Endnote X7 reference manager software, and duplicated articles were removed. After reviewing the titles and abstracts, studies were screened. Articles were screened and evaluated independently by two authors (L.A.T. and B.G.K.). The full text of the study was evaluated based on its objectives, methodology, participants/population, and key findings (male involvement in FP and associated factors). Disagreements were resolved through discussion and consensus-based on predetermined criteria, or by the last two investigators (A.D.A. and G.A.T.).
Quality assessment
The Newcastle–Ottawa Scale quality assessment tool adapted for cross-sectional study quality assessments was used to assess the quality of each included original cross-sectional study. 29
The tool has the three major components; the main component is rated from one to five stars and focuses on the methodological quality of each primary study. The tool’s second component concentrated on the comparability of the primary studies included in this systematic review and meta-analysis. The final component, which was based on three stars, assessed the quality of primary articles in statistical analysis and outcome point of view. Using these pointers, three authors independently weighted the qualities of each original study. The analysis included primary studies with a medium score (satisfying 50% of quality evaluation criteria) and high quality (7 out of 10). The three investigators’ differences were managed using the results of their quality evaluations (Additional file 2).
Data extraction
The data were extracted independently by two authors (L.A.T. and B.G.K.) using a pretested standardized data extraction format. The primary author, year of publication, study setting, sample size, study design, response rate, the prevalence of male involvement in FP, and specific factors associated with FP involvement are all included in the format. The variables in this study were chosen because they were found to be a significant factor in two or more studies. When the investigators could not agree on how to abstract data, they reached a consensus, and the final two investigators took over (A.D.A. and G.A.T.).
The outcome of interest
The primary outcome of this meta-analysis was male involvement in FP service utilization. The second objective of the review was to determine the factors affecting involvement in FP among married men in Ethiopia.
Publication bias and heterogeneity
A qualitative visual inspection of the funnel plot graph reveals the presence of publication bias. We also used Egger’s correlation tests with a 5% significance level to quantitatively assess the presence of publication bias.30,31 In addition, study regions were divided into subgroups to reduce random variations in the point estimates from the primary study. To identify the potential source of heterogeneity, a sensitivity analysis was carried out. The random-effect model with inverse-variance (I2) statistics and corresponding p-values was used to assess heterogeneity across studies.
Statistical analysis
The extracted data were first entered into Microsoft Excel before being exported to STATA version 14 for analysis. Based on eligibility criteria, the associated factors of male involvement in FP were investigated. We looked at least two studies that shared a measure of effect and a 95% confidence interval (CI) for at least one associated factor of male involvement. To compare the studies, a random-effects model based on the DerSimonian–Laird method was used. Texts, tables, and forest plots were used to present the findings, which included effect measures and a 95% CI.
Result
Description of studies
A total of 687 records were identified using electronic search. From these identified studies, 319 were excluded after reviewing their titles due to duplication, and the remaining 368 studies were further screened for inclusion. Out of 368 studies; 297 studies, were excluded due to irrelevance, and 54 were removed due to inappropriate use of statistical analysis, irrelevant target population, and inconsistent study reports. Finally, 17 articles fulfilled the inclusion criteria and were included in this systematic review and meta-analysis (Figure 1).

Flow chart describing the selection of studies for the systematic review and meta-analysis of the prevalence of male involvement in family planning and associated factors among married men in Ethiopia, 2021.
Characteristics of the included studies
All of the 17 studies included in this review were cross-sectional in nature and reported in English. A total of 9117 married men took part in the systematic review and meta-analysis. The sample size for the primary articles ranged from 28610 to 80411 in Oromia regional state. The highest prevalence of male involvement in FP was observed in Debre Tabor Town Northwest Ethiopia (68.1%), 12 and the lowest was from Debre Marko’s Town (8.4%). 13 Regarding geographical distribution of the studies, five studies were conducted in Amhara regional state,12–16 six from the Southern Nation, Nationalities, and Peoples’ Region (SNNPR),17–21 three conducted in Oromia,10,11,22 one from Benishangul-Gumuz, 23 one from Tigray, 24 and one in Afar 25 (Table 1). Concerning the quality score of the primary studies, eight studies had a quality score of eight, six studies had a quality score of seven, and the remaining three had a quality score of nine. Hence, all of them had a good and above quality score (Additional file 2).
Summary of the 17 observational studies included in the meta-analysis assessing involvement of males in family planning in Ethiopia, 2021.

AF: associated factors; CI: confidence interval; C/S: cross-sectional; MIFP: male involvement in family planning; SNNPR: Southern Nation, Nationalities, and Peoples’ Region.
Prevalence of male involvement in FP in Ethiopia
The pooled prevalence of male involvement in FP among married men in Ethiopia was 39.66% (95% CI = 29.86, 49.45) (Figure 2). A random-effect model was used to estimate the pooled prevalence of male involvement in FP as a result of extreme heterogeneity across the included primary studies (I2 = 99.8%, p < 0.001).

Forest plot of the pooled prevalence male involvement on family planning in Ethiopia, 2021.
Publication bias
Publication bias was observed among the included studies as evidenced by the asymmetric shape of the funnel plot (Figure 3) and Egger’s regression test (p < 0.001). To correct the observed publication bias, trim and fill analyses were conducted, but the trim and fill analyses were not filled (data unchanged) (Figure 4).

Funnel plot to test the publication bias of included studies on male involvement in family planning in Ethiopia, 2021.

Trim and fill analysis for adjusting publication bias of the included studies on male involvement in family planning in Ethiopia.
Sensitivity analysis
To identify the potential source of heterogeneity observed in the pooled prevalence of male involvement, the authors conducted a leave-one-out sensitivity analysis. The result of the sensitivity analysis found that the finding did not rely on a particular study. The pooled prevalence of male involvement was varied and ranged from 37.87% (28.34, 47.41) to 41.61% (32.32, 50.90) after the deletion of four studies (Table 2).
Sensitivity analysis of the prevalence of male involvement in family planning among married men in Ethiopia, 2021.

CI: confidence interval.
Subgroup analysis
Subgroup analysis by region was calculated to compare the involvement of males in FP service utilization across regions of the country. Accordingly, the highest pooled prevalence of male involvement in FP was observed in the Oromia region 44.66% (95% CI = 36.04, 53.28), followed by the Amhara region 37.79% (95% CI = 14.65, 60.93), whereas the lowest prevalence of male involvement was observed in SNNPR 32.56% (95% CI = 16.81, 48.30) (Table 3).
Subgroup analysis of male involvement in family planning among married men in Ethiopia, 2021.

CI: confidence interval.
Factors affecting the involvement of males in FP
In the current systematic review and meta-analysis, men’s educational status, discussion of FP options with their wives, knowledge of FP, a positive attitude toward FP, and approved FP service utilization were all found to be significantly associated with male involvement in FP service utilization.
In this review, three primary articles14,19,23 found that men who had received formal education were nearly two times (adjusted odds ratio (AOR) = 1.99, 95% CI = 1.26, 3.14) more likely than men who had not received formal education to use FP services. There was very little heterogeneity between the studies (I2 = 23.1%, p = 0.273). As a result, the pooled odds ratio was estimated using a random-effect model (Figure 5).

Association between education and male involvements of family planning.
Seven primary articles12,17,19–21,23,26 noticed married men who have discussed with wife regarding FP issues were four times (AOR = 4.15, 95% CI = 2.21, 7.80) higher the odds of their involvement in FP than their counterparts. The heterogeneity test showed higher heterogeneity across the studies; as a result, we used the random-effects model to estimate the pooled odds ratio (Figure 6).

Association between discussion on FP with wives and male involvements of family planning.
Knowledge of men about FP is also another important determinant of male involvement in FP as highlighted by four primary studies.12,17,23,25 Married men knowledgeable about FP were nearly two times (AOR = 1.83, 95% CI = 1.26, 2.64) increased the odds of involving in FP service utilization than their counterparts. The heterogeneity test showed (I2 = 66.7%, p = 0.029). Hence, the pooled odds ratio was estimated using random-effect model analysis (Figure 7).

Association between knowledge and male involvements of family planning.
Similarly, having a positive attitude toward FP was also a key factor for male participation in FP service, which was mentioned by three studies.17,18,23 Men with a positive attitude toward FP were 2.6 times (AOR = 2.57, 95% CI = 1.70, 3.90) more likely to be involved in the service than those who had a negative attitude toward FP service. Since heterogeneity between articles was I2 = 31.7% and p = 0.231, random-effect model was the preferred model for analysis (Figure 8).
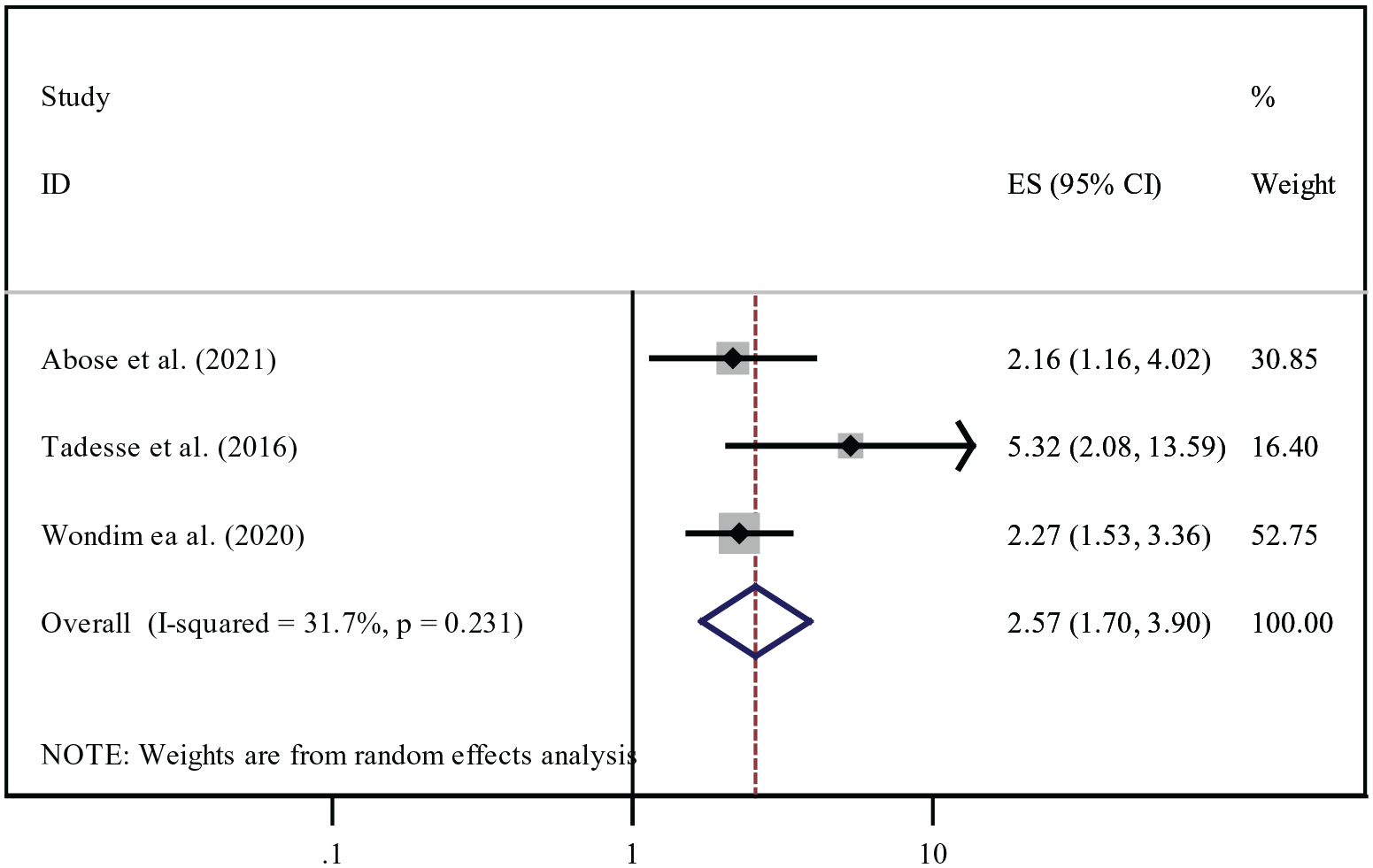
Association between attitude and male involvements of family planning.
Finally, three studies13,19,21 reported that approval of men in contraceptive use was highly associated with involvement in the FP service. Men who approved FP services utilization were 9.56 times (AOR = 9.56, 95% CI = 3.74, 24.48) more likely involved in FP services utilization than men who did not approve. Random-effect model analysis was conducted to estimate the pooled odds ratio because of the higher heterogeneity effect (Figure 9).
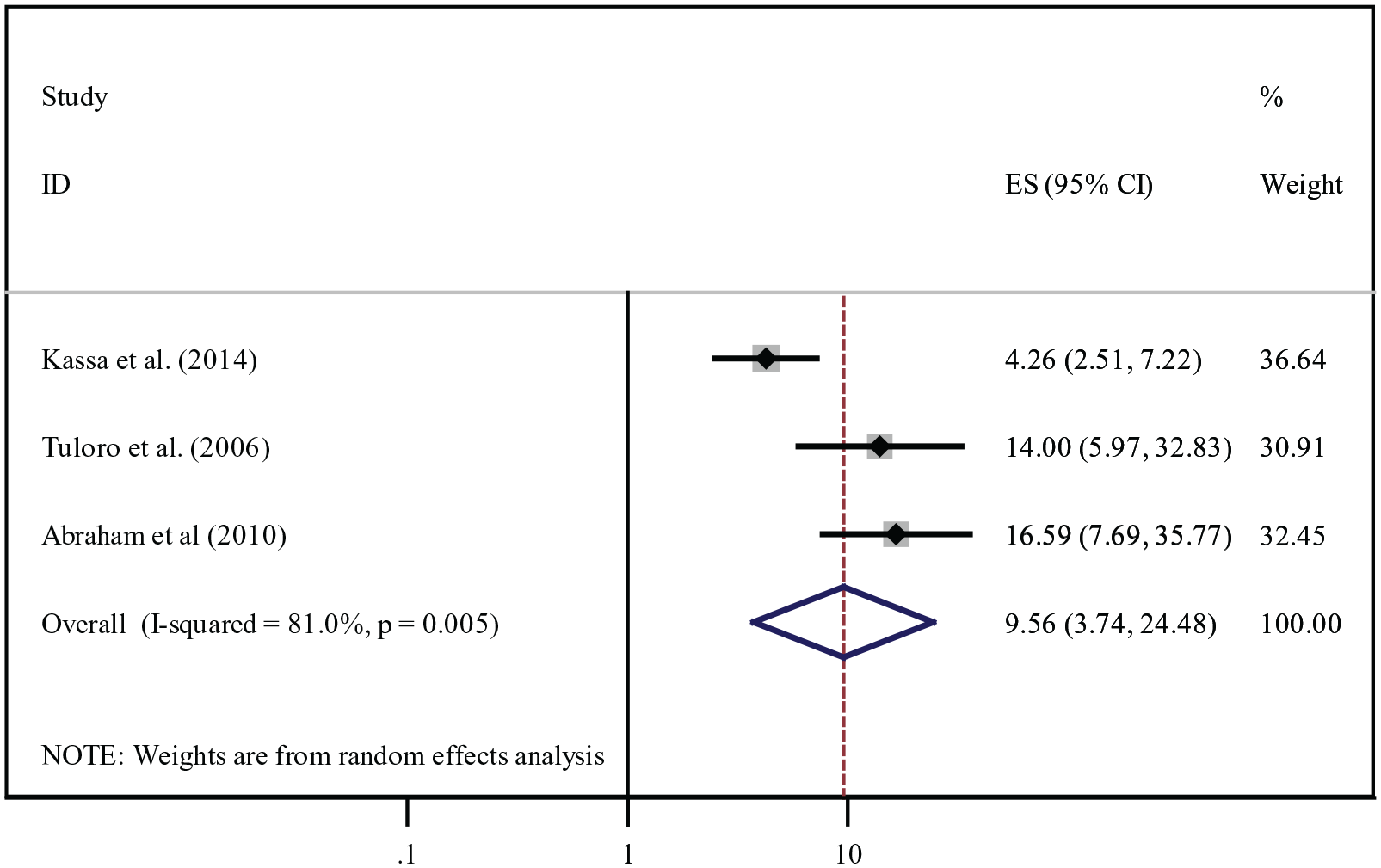
Association between approval and male involvements of family planning.
Discussion
Males’ role in FP is getting more attention these days, as population planners recognize the importance of men’s influence over reproductive decisions around the world. 32 This systematic review and meta-analysis present findings from documented primary studies and experience in a different part of Ethiopia to assess the current state of knowledge regarding this issue. The review’s current goal is to improve men’s knowledge and attitudes about FP, with the ultimate aim of encouraging behavior change and active participation in the issue.
According to this review, the national pooled prevalence of male involvement in FP was 39.7%. This finding was consistent with a study conducted in Turkey, 33 Ghana (34.4%), and (38.9%),34,35 and Uganda (40%). 36 However, the level of male involvement in FP was lower than a study conducted in Bangladesh (63.2%), 37 Vietnam (63.7%), 38 Kenya (52%), 39 Nigeria (89%), 40 and India (71.2%). 41
This disparity could be due to low socioeconomic status, differences in health infrastructure, and media reports of a lack of male involvement promotion. This could also be due to a lack of shared responsibility, low educational attainment, a negative attitude toward male participation in FP services, and a misunderstanding that FP is solely a woman’s business. Male participation in FP is once again given insufficient attention by program planners and policymakers. Men’s low participation was also due to the lack of various contraceptive options available to them. To increase male participation in FP services, more involvement of healthcare providers to motivate governmental concerns, media coverage to raise awareness, and individual motivation may be required.
The subgroup analysis of this systematic review and meta-analysis revealed regional differences in male involvement in FP. The Oromia region had the highest pooled prevalence of male involvement in FP (44.7%), while the SNNPR had the lowest prevalence, which was 32.56%. This disparity could be due to a time difference, a difference in study settings, or a socio-cultural difference in the community.
Based on the current review, educational status of men was a significant positive predictor of male involvement in FP. When the educational status of males increases, the active involvement of males in FP improves, which is inclined with previous studies done in Bangladesh, 37 sub-Saharan Africa, 42 Nigeria, 40 Kenya, 39 Ghana, 43 and Cameroon. 44
This could be because educated men have a better understanding of FP and its importance, which encourages them to engage in active FP use. Furthermore, men’s educational attainment has a positive impact on a couple’s RH decisions and overall fertility preferences. Moreover, uneducated men frequently hold misconceptions about FP methods, particularly regarding side effects. These misunderstandings are frequently the cause of low male participation. As a result, obtaining at least a primary education is a critical intervention for improving male involvement in FP.
Parental discussion on the issue of RH, including FP, had a positive association with men’s involvement which is supported by studies done in Bangladesh, 37 India, 45 and Nigeria. 40 The possible explanation might be that spousal discussion regarding reproduction and FP is viewed as successful to the extent that it directly increases the use of contraception and favorable attitudes toward contraception among couples. Furthermore, through open discussion, couples communicate with one another about RH-related issues such as the types of FP methods they will choose, problems encountered with RH and sexual life, and the best decision from which they will seek appropriate RH services. On the contrary, lack of discussion may reflect a lack of personal interest, hostility to the subject, or a customary reticence in talking about sex-related matters. Thus, implementing strategies to improve spousal communication between couples on the issue of reproduction is an important weapon to tackle; one of the major barriers to the unmet need for FP was women’s perceptions of husbands’ opposition by scaling up men’s participation.
In this systematic review and meta-analysis, men’s level of knowledge about FP positively correlates with their involvement. Men who had sound knowledge about contraceptives were nearly two times more likely to scale up their involvement in FP than their counterparts. Findings from Bangladesh, 37 Myanmar, 46 New Guinea, 47 Nigeria, 48 Ghana,34,49 Kenya, 39 and Cameroon 44 also concluded that improved knowledge of different contraceptive methods was a positive predictor of male involvement. This could be because men who have adequate knowledge of contraceptive methods are willing to participate in the selection of a suitable method for use with their wives. Furthermore, men with sufficient knowledge of various FP methods, particularly male contraceptive options, may be directly involved in FP use and encourage their partners to do so, reducing maternal mortality because knowledge of FP is a prerequisite for male involvement in FP use. As a result, there is a need to improve men’s knowledge through education and media training.
Similarly, men who had a positive attitude toward FP service were nearly three times more likely to participate in FP service utilization. Findings from sub-Saharan Africa 50 and Nigeria40,48 provided consistent outcomes to those reported in this study. This implies that men’s positive attitude toward contraceptives approves either to use contraceptives on their own or support their wives to use contraceptives. Furthermore, men who have a positive attitude toward FP may like the service and might be interested in participating in their partners’ FP service. Whereas those who have a negative attitude toward FP may even refuse and violet their partner not only to involve but also to stop the FP method used by their partner. Hence, this review highlights the need to convert men’s negative attitudes into positive attitudes and then into positive behaviors through intensive RH education.
As mentioned elsewhere, men’s approval for FP was strongly associated with men’s involvement in FP.42,48,51,52 This may be due to the accessibility of information and shared responsibility; female partners were taking responsibility for FP. Besides, men approving FP service utilization increases women’s confidence in the decision-making process regarding various reproductive issues, including FP.
Despite its significant importance, this systematic review and meta-analysis have their own limitations. All of the primary articles enrolled in this meta-analysis were cross-sectional; as a result, increased risk of biases, affected by heterogeneity and the outcome variable, might be affected by other confounding variables. Besides this, some of the studies enrolled in this study had a small sample size, which may affect the actual prevalence of male involvement at the country level. Furthermore, all regions in Ethiopia were not represented in this systematic review and meta-analysis due to a limited number of studies in the country (only six regional states were represented in this study). As a result, the finding of this systematic review and meta-analysis may not exactly estimate the national pooled prevalence of male involvement in FP service.
Conclusion
In a conclusion, the overall national pooled prevalence of male involvement in FP in Ethiopia was significantly low. Educational status, open discussion on the issue of FP with their spouses, knowledge, attitude, and approval of FP were among the significant predictors of male partner involvement in FP service utilization. Both governmental and non-governmental organizations, service providers, program planners, and different stakeholders should ensure availability, accessibility, and sustained advocacy for male involvement in FP services utilization. Besides, creating a conducive environment for education, behavioral change, and open discussion concerning RH issues, including FP. FP programs should also incorporate males in the uptake of FP services.
Supplemental Material
sj-docx-1-whe-10.1177_17455057221099083 – Supplemental material for Prevalence and determinants of the involvement of married men in family planning services in Ethiopia: A systematic review and meta-analysis
Supplemental material, sj-docx-1-whe-10.1177_17455057221099083 for Prevalence and determinants of the involvement of married men in family planning services in Ethiopia: A systematic review and meta-analysis by Bekalu Getnet Kassa, Lebeza Alemu Tenaw, Alemu Degu Ayele and Gebrehiwot Ayalew Tiruneh in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057221099083 – Supplemental material for Prevalence and determinants of the involvement of married men in family planning services in Ethiopia: A systematic review and meta-analysis
Supplemental material, sj-docx-2-whe-10.1177_17455057221099083 for Prevalence and determinants of the involvement of married men in family planning services in Ethiopia: A systematic review and meta-analysis by Bekalu Getnet Kassa, Lebeza Alemu Tenaw, Alemu Degu Ayele and Gebrehiwot Ayalew Tiruneh in Women’s Health
Footnotes
Acknowledgements
The authors acknowledge the sources of all primary studies.
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The data set used in this review is available upon a reasonable request to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.