
Abstract
Background:
Adolescent girls are more likely to develop anemia as a result of physical and physiological changes that place a greater strain on their nutritional needs. Primary studies, on the other hand, may not be sufficient to provide a complete picture of anemia in adolescent girls and its major risk factors.
Objective:
The study aimed to describe the pooled prevalence of adolescent girls’ anemia and the factors that contribute.
Methods:
We conducted a systematic review of observational studies using the databases CINAHL (EBSCO), PubMed, Science Direct, Cochrane Library, and Google Scholar. The Newcastle-Ottawa Scale was used to assess the quality of the articles, and studies of fair to good quality were included. We pooled anemia prevalence among adolescents and odds ratio estimates for risk factors. Subgroup analysis employing sample size and study setup was computed to determine the source of heterogeneity, and the I2 test was used to identify the existence or absence of substantial heterogeneity during subgroup analysis. The pooled prevalence of adolescent girls’ anemia was calculated using a random-effects meta-analysis model.
Results:
The overall pooled prevalence of anemia among adolescent girls in Ethiopia was 23.03% (95% confidence interval: 17.07, 28.98). Low dietary diversity (odds ratio: 1.56; 95% confidence interval: 1.05, 2.32), illiterate mothers (odds ratio: 1.45; 95% confidence interval: 1.13, 1.86), household size greater than five (odds ratio: 1.65; 95% confidence interval: 1.14, 2.38), food-insecure households (odds ratio: 1.48; 95% confidence interval: 1.21, 1.82), and menstrual blood flow more than 5 days (odds ratio: 6.21; 95% confidence interval: 1.67, 23.12) were the identified factors associated with anemia among adolescent girls.
Conclusion:
The pooled prevalence of anemia among adolescent girls in Ethiopia was moderately high. Therefore, to combat the burden of anemia among adolescent girls offering nutritional education is crucial. Iron supplementation is also recommended for adolescent females who have a menstrual cycle that lasts longer than 5 days.
Introduction
Anemia is a condition in which the body does not have a sufficient number of red blood cells and/or hemoglobin. In women, a hemoglobin level less than 12.0 g/100 mL is considered to be indicative of anemia. It is one of the main global public health problems in both developed and developing countries.1,2 Among the type of anemia, iron deficiency anemia is the most common at the start of adolescence and is caused by increased nutrition requirements due to the rapid growth rate among adolescent girls and is exacerbated at the time of menstruation for them. 3 Globally, about 1.2 billion population comprises adolescents, 90% of whom live in low- or middle-income countries (LMICs). 4 In Ethiopia, about 48% of the population constitutes adolescents, of which nearly 25% are adolescent girls. 5
The World Health Organization (WHO) defined adolescence as the age group between 10 and 19 years, with the second most rapid growth rate next to infants. 6 It is a period of rapid growth, and 45% of skeletal growth, 15%–25% of the adult height, and up to 37% of total bone mass are achieved during this period.7,8 This rapid growth increases iron requirements for hemoglobin in the blood and myoglobin in muscle. They are a vulnerable group to anemia because of increased iron requirements to support their rapid growth and mental development and replenished loss due to menstruation.9,10 Adolescent girls are at high risk of anemia due to the physical and physiological changes that put them in a higher demand on their nutritional requirements.
The factors associated with anemia are inadequate dietary iron intake or poor absorption, growth period increased the need for iron during menstruation, intestinal worms’ infestation, and some socio-economic factors. Other important causes of anemia are infection and other nutritional deficiencies like folate and vitamin 12, vitamins A and C, genetic conditions (include sickle cell anemia, thalassemia—an inherited blood disorder—and chronic inflammation), and severe malaria and may be associated with secondary bacterial infection.11,12 In Ethiopia, studies indicate that family economic status, type of family adolescents live with, residence, family size, adolescent’s age, maternal literacy level, household dietary diversity score (DDS), menses status, duration of menstruation, and intestinal parasitic infection were the factors associated with adolescent anemia.13–25
Globally, anemia increased among women of non-pregnant reproductive age groups from 464 million in 2000 to 578 million in 2016. In LMICs, the overall prevalence of anemia among adolescent girls was higher than 35%. 26 This condition existed in Southwest Asian countries ranging from 30% to 58.6%; 27 similarly, in Sub-Saharan Africa, about half of adolescent girls were anemic. 26 Ethiopia also shares the high burden of anemia in young women, which ranges from 24% to 38%, with an average rate of 29%. 22
The outcome of anemia can cause cognitive impairment in animals and humans, with brain mitochondrial damage as a basis related to lose attention span, intelligence, sensory perception function, emotion, and behavior.28,29 Furthermore, more adolescent girls’ anemia will contribute to high maternal mortality, increased incidence of low birth weight, perinatal mortality, and fetal loss and considered one of the consequences of the cycle of malnutrition. It may also include detrimental impacts on economic and social development. 30 Currently, study findings indicated that adolescents were the second window of opportunity to impede the intergenerational cycle of malnutrition and become recognized that they are the most nutritionally vulnerable groups prone to be anemic. However, in most developing countries, nutrition intervention mainly focuses on under-five children and pregnant women, and adolescent girls considered a nutritionally non-vulnerable age group.
Cognitive to the situation, the government of Ethiopia comprised adolescent girls’ nutrition separately on the national food and nutrition policy, although, still, the national level of anemia among adolescent girls remained unknown. Even the Ethiopian Demographic Health Survey (EDHS) did not report the level of anemia among adolescents in particular, while children and mothers are reported. Despite this and to the best knowledge of the reviewers, there is no single national pooled figure about the level of anemia among adolescent girls and also there is inconsistency shown between the evidence on the factors associated with it. Therefore, this systematic review and meta-analysis will generate concrete results in which the evidence may urge policymakers and program managers to design appropriate interventions to control and minimize the negative consequence of anemia among adolescent girls.
Methods
Literature search approach and study design
For its rigor, this study was guided by Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 31 (S1_File). The articles for this study were identified through a comprehensive and reproducible electronic search of reputable databases (PubMed, Google Scholar, Science Direct, CINHAL (EBSCO), and Cochrane library) and the hand search of reference lists of previous prevalence studies to retrieve more related articles. The researchers also used the “related articles” option of PubMed and checked the reference lists of the original and review articles to detect more relevant publications. The search was independently performed by two groups of authors using the following key terms and Boolean operators: “(Adolescent* OR Adolescent[Mesh] OR Preadolescent*) AND (Anemia[Mesh] OR Anaemia OR Haemoglobin OR “Hematologic parameter*” OR “Hematologic profile*” OR “Micronutrient deficiency*” OR “Nutritional anemia” OR “Iron deficiency anemia”) AND (Ethiopia OR Ethiopian OR “Regions of Ethiopia”)” (S2_File). Before searching the databases, the appropriateness of searching words was verified for retrieving the relevant articles. The literature search was limited to the English language and human study category. The literature search for published articles up to February 2022 was considered to be included in this systematic review and meta-analysis. The articles were searched, organized, and extracted from November 2021 to February 15/2022. Also, the End-Note X7 reference manager has been used to manage the literature retrievals since the inception of the study. Unfortunately, the study was not registered on PROSPERO.
Study selection
Inclusion criteria
The contents of each of the identified publications were independently and thoroughly assessed by two groups of authors. The following studies were considered for inclusion in the study if they met the following criteria. The retrievals were evaluated for inclusion in the final review based on their titles, abstracts, and full-text papers.
Original studies reporting the prevalence and predictors of anemia among adolescent girls in Ethiopia were included. Only studies that were written in English were considered. Studies that met the eligibility criteria were included regardless of whether or not they had been published (published, unpublished, and gray literature).
Exclusion criteria
Following carefully examining the abstracts and full texts of the research, two groups of reviewers separately and anonymously selected the studies. The articles with methodological flaws were excluded. Any discrepancies that arose throughout the review process were resolved through consensus, and if disagreements persisted after discussion, a third party was seeking to resolve the issue. The PRISMA flow diagram was used to guide the procedures of identifying, screening, and including or rejecting records (Figure 1).

PRISMA flow diagram for the selection of eligible studies for systematic review and meta-analysis on anemia among adolescent girls in Ethiopia, 2022.
Data extraction and quality assessment
Using a pilot-tested and prepared data abstraction tool, two independent reviewers abstracted the relevant data. The following information was taken from the paper: first author, study area, study design, publication year, sample size, response rate, mean hemoglobin level, and prevalence of anemia in children. Any disagreements that arose throughout the data extraction process were handled through discussion and the involvement of the third group authors (D.W. and F.B.).
To assess the studies’ quality, we used the Newcastle-Ottawa 32 quality assessment tool scale adapted for cross-sectional studies. This standardized technique includes three primary indications for article methodological characteristics, comparability, and statistical analytics. The studies’ quality was assessed using the following indicators: those with medium (50% of quality assessment criteria met) or high (6 out of 10 scales) quality were included in the study. The assessment results were calculated using the average of the two authors’ scores.
Outcomes of interest
The prevalence of anemia among adolescent girls was the study’s most important finding. Anemia in adolescents is defined as a hemoglobin value of less than 11 g/dL in children aged 5–11 years, less than 12 g/dL in children aged 12–14 years, less than 13 g/dL in men aged 15 years, and above and below 12 g/dL in non-pregnant women aged 15 years and above, according to WHO 2011. 33 The research included in this study used WHO criteria to operationalize and characterize anemia, with some correcting for altitude. The prevalence was calculated by multiplying the number of anemic adolescent girls by the total number of adolescents included in the study (sample size).
The associated factors of anemia among the study individuals were the study’s second outcome. The odds ratio was used to measure the relationship between anemia and the variables. The odds ratio was derived using the original studies’ two-by-two table reports. The included studies measured household food security using the household food insecurity access scale (HFIAS) developed by Food and Nutrition Technical Assistance (FANTA) Project through the Academy for Educational Development 34 and the dietary diversity score (DDS) was assessed by the studies as consuming nine food groups over 24 h, which are starch (cereals and white roots), vegetables, fruits, fish, tubers, meat (including organ meat), milk, egg, and legumes. Each food group had been counted only once resulting in a possible score of 0–9. Food groups are categorized into low dietary diversity if ⩽3 food groups were consumed.
Heterogeneity and publication bias
Publication bias and heterogeneity were checked using Egger’s and Begg’s tests. A p-value of less than 0.05 was considered to declare the statistical significance of publication bias and heterogeneity. The heterogeneity of studies was also assessed using I2 test statistics. The I2 test statistics of 25%, 50%, and 75% were considered as low, moderate, and considerable heterogeneity, respectively. For the test results that exhibited heterogeneity, the random-effects model was used as a method of analysis.
Data analysis/synthesis of results
The authors used STATA 14 version software to analyze the results after extracting pertinent data from the studies using Microsoft Excel 2010 format. A table and a forest plot were used to summarize and present the original studies. Using the binomial distribution formula, the authors calculated the standard error of prevalence of anemia for each original study. We used the I2 test and Cochrane Q statistics to look for potential heterogeneity in the reported prevalence of the studies. 35 Because the test data revealed significant heterogeneity 36 among the studies (I2 = 96.33%, p < 0.001), the DerSimonian and Laird’s pooled impact was estimated using a random-effects model. We also performed a univariate meta-regression analysis using the study’s publication year and sample size to identify potential sources of variance; however, all of them were statistically insignificant (p > 0.05). Sterne and Egger’s 37 weighted correlation and Begg’s regression intercept tests were used to objectively analyze potential publication bias at the 5% significant level. Sensitivity analysis was also conducted to identify the effect of small studies on the overall result. In addition, subgroup analysis based on research regions, study settings, and publication year was carried out to minimize random variations between the point estimates of the original studies. The log odds ratio was used to determine predictors of adolescent girls’ anemia.
Results
Search results
Through manual and electronic searches, we were able to find a total of 305 records from the start. To identify more related articles, an electronic search was conducted using databases such as MEDLINE/PubMed, Google Scholar, Science Direct, EMBASE, Cochrane Library, and reference lists from prior studies. Ten of the records were eliminated from the retrievals due to duplication. After the authors evaluated the titles and abstracts of the records, 118 records were eliminated from the remaining 295 retrievals since they were not relevant for this evaluation in terms of the study’s outcome. Then, according to the study population, study area, and study inclusion time, 148 publications were eliminated. Then, based on the pre-set eligibility criteria, 29 complete texts were evaluated and scored for eligibility. Finally, this systematic review and meta-analysis comprised 10 articles that were deemed relevant (Figure 1).
Description of original studies
In this systematic review and meta-analysis, the descriptive summary of the characteristics of 10 studies was included.14,16,18–22,25,38,39 All of the studies are cross-sectional (community-based and school-based) by design. The studies were conducted in different regions of Ethiopia with a sample size that ranges from 257 in Huruta district, Oromia region to 570 in Addis Ababa 2019. The eligible studies have been carried out since 2016. In the present systematic review and meta-analysis, a total of 5386 adolescent girls were enrolled to estimate the pooled prevalence of anemia (Table 1).
Characteristics of 10 studies reporting the prevalence of anemia among adolescent girls in Ethiopia included in the current systematic review and meta-analysis, 2022.
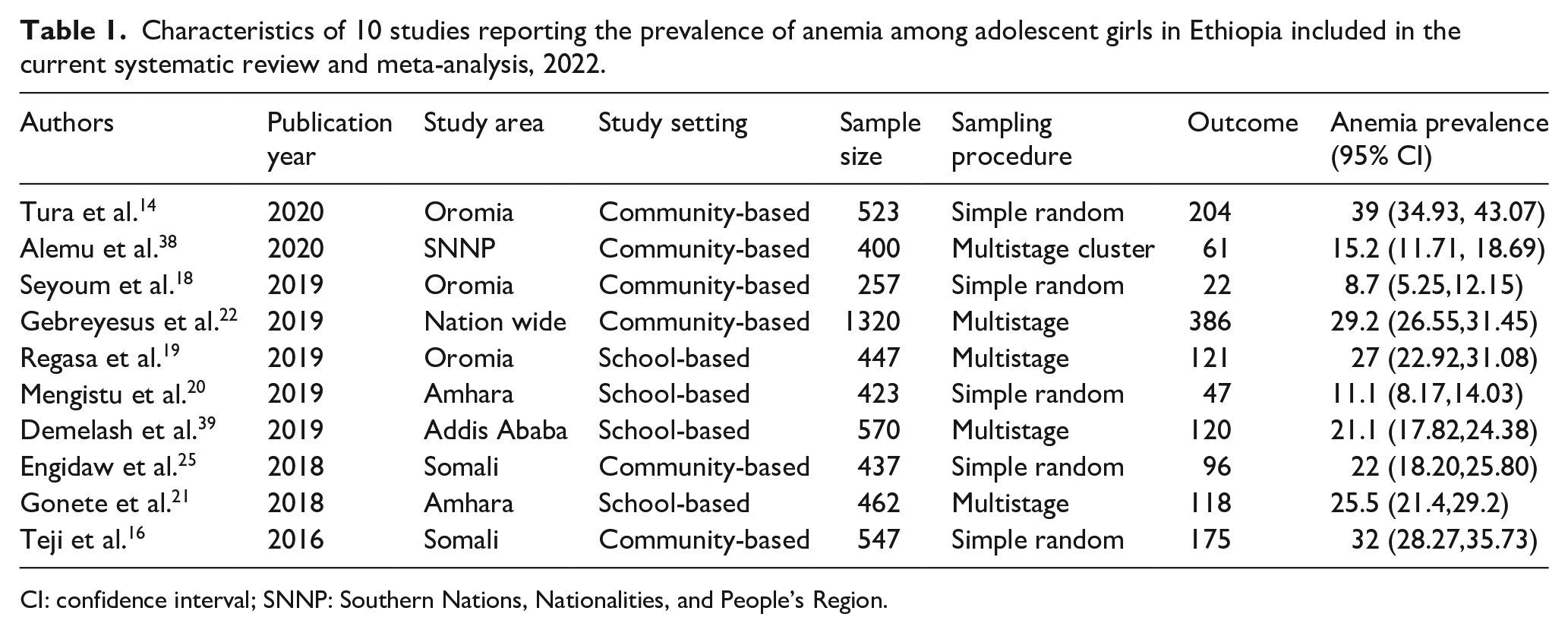
CI: confidence interval; SNNP: Southern Nations, Nationalities, and People’s Region.
The 10 studies have been done in most regions of Ethiopia: one of the studies was conducted in Addis Ababa; two in the Amhara region, three in the Oromia region, Amhara, two in the Somali region, one from the Southern Nations, Nationalities, and People’s Region (SNNPR), and one study conducted in three districts of three regions (Oromia, Amhara, and SNNPR). The highest prevalence of anemia (39%) was observed in the Oromia region (Ambo town) in 2020. On the other hand, the lowest prevalence (8.7%) of anemia was reported in Oromia Region in 2019. Furthermore, the primary studies included in this analysis had response rates ranging from 91% to 100%, and almost all of them had a strong response rate (Table 1).
Regarding the publication status of the studies, all of the studies were published studies. Also, one of the studies is conducted in three districts of three regions. However, the rest of the studies included in the current meta-analysis were retrieved by exhaustive and reproducible search from reputable databases such as PubMed. The authors meticulously appraised all the studies before review and analysis, and the included articles were confirmed fit for their quality, that is, quality scores ranging from 5 to 8 out of 10 marks.
Meta-analysis and meta-regression
To provide a visual summary of the data in this meta-analysis, a forest plot was utilized to estimate the pooled effect size and the effect of each study with their corresponding confidence interval (CI). The overall pooled prevalence of anemia among adolescent girls in Ethiopia was 23.03% (95% CI: 17.07, 28.98), as per the forest plot of 10 included research. Detected by I2 statistic (I2 = 96.65, p < 0.001), we observed considerable heterogeneity across the included studies. As a result, we employed the DerSimonian and Laird random-effects model to estimate the overall pooled prevalence of anemia among adolescent girls since the model gives a more conservative effect size (Figure 2). Taking publication year and sample size of the studies as potential factors associated with the prevalence variation, we performed a univariate meta-regression analysis to determine the likely sources for the variation. However, none of them is statistically significant for the variation (Table 2). In addition, Egger’s and Begg’s tests revealed that there is no statistically significant publication bias, p > 0.13 and p > 0.08, respectively. The test results showed that there is no significant publication bias (p > 0.05). The funnel plot also supports subjectively the absence of publication bias (Figure 3).
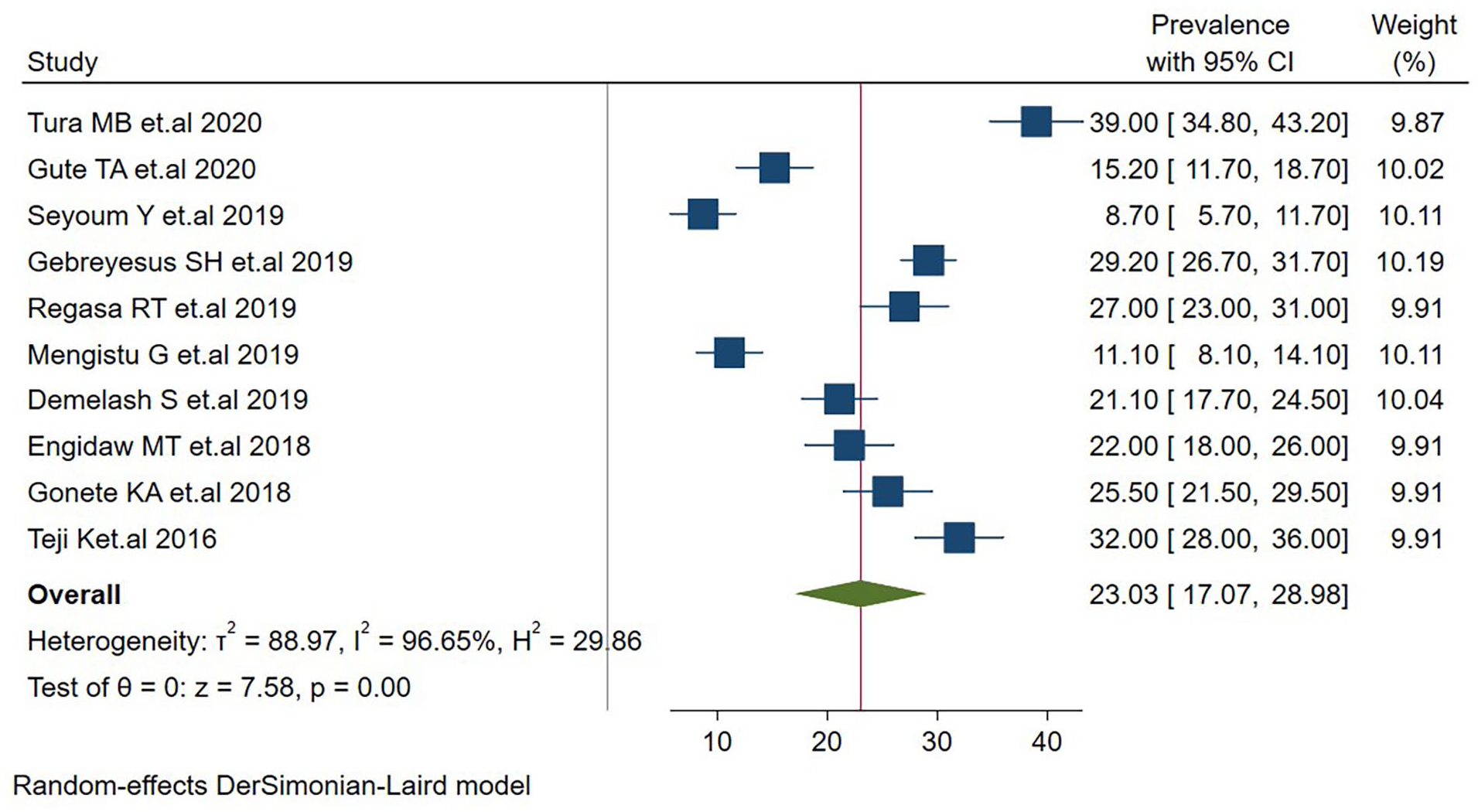
Forest plot depicting pooled prevalence of anemia among adolescent girls in Ethiopia, 2022.
Univariate meta-regression of factors related to the heterogeneity of anemia among adolescent girls in Ethiopia, 2022.


Funnel plot showing publication bias of anemia studies among adolescent girls in Ethiopia, 2022.
Subgroup analysis
We conducted subgroup analyses to investigate the likely sources of heterogeneity based on the publication year, study area, and study setting where the studies were done. Although it is not significant, the result showed that the highest prevalence of anemia among adolescent girls was observed in the Somali region with a prevalence of 27% (95% CI: 17.20, 36.80) followed by Oromia region studies, 24.85 (95% CI: 06.72, 42.99). But the prevalence of anemia in the subjects was the least in Amhara 18.24 (95% CI: 04.13, 32.35) (Figure 4). Regarding the study settings, the prevalence of adolescent girl’s anemia was relatively similar in community and school-based studies, 24.31% (95% CI: 15.38, 33.23) and 21.10% (95% CI: 13.60, 28.59), respectively (Figure 5). Also, anemia in adolescent girls was found to be higher in the studies conducted before the year 2019, 21.57% (95% CI: 13.80, 29.34) than in the studies conducted in 2019 and after (Figure 6).

Subgroup pooled prevalence estimate of anemia by study area among adolescent girls in Ethiopia, 2022.

Subgroup pooled prevalence estimate of anemia by publication year among adolescent girls in Ethiopia, 2022.

Subgroup pooled prevalence estimate of anemia by study setting among adolescent girls in Ethiopia, 2022.
Sensitivity analysis
The authors also performed a sensitivity analysis for each study, and none of the studies showed a significant difference (Table 3).
Sensitivity analysis for estimates on anemia among adolescent girls in Ethiopia, 2022.
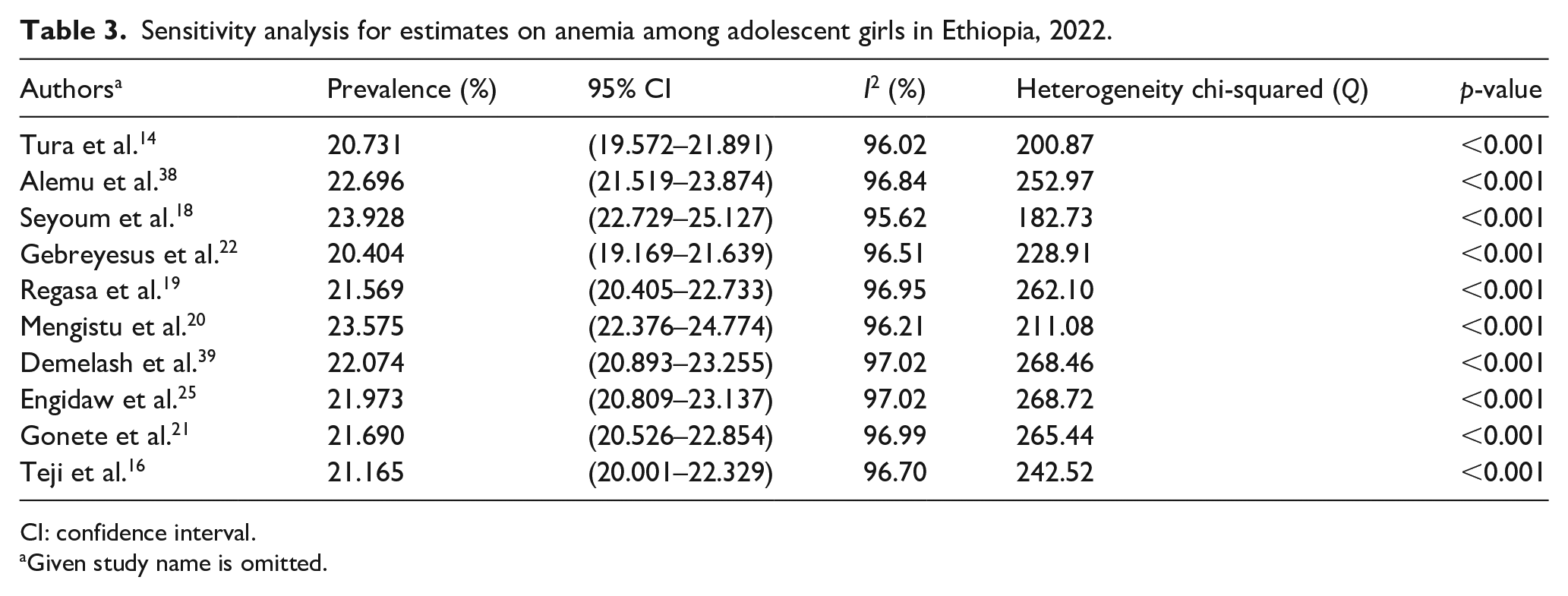
CI: confidence interval.
Given study name is omitted.
Predictors of anemia among adolescent girls
The authors did comprehensively review and meta-analyze the predictors of anemia among the study subjects using nine meta-analyzable studies14,16,19–22,25,38,39 from the relevant articles included in the current study. Age, household size, DDS, mother’s educational status, menses status (have/have not started menstruation), duration of menses, and household food security status were found to be worth reviewing and meta-analyzable. Except for age and menses status, all the predictors revealed a statistically significant association with anemia among adolescent girls in Ethiopia.
The pooled estimate of the studies showed that adolescent girls with low dietary diversity were 1.56 times more likely to be anemic than their counterparts, odds ratio of 1.56 (95% CI: 1.16, 3.31) (Figure 7). Those adolescent girls whose mothers are illiterate (not educated) were 1.45 times more likely to be anemic as compared to those whose mothers are literate, odds ratio of 1.45 (95% CI: 1.13, 1.86) (Figure 8). In addition, those adolescent girls whose household size was greater than five were 1.65 times more likely to be anemic as compared to those whose household members were less than five, odds ratio of 1.65 (95% CI: 1.14, 2.38) (Figure 9). Adolescent girls who live in food-insecure households were 1.48 times more likely to be anemic than food secured households 1.48 (95% CI: 1.21, 1.82) (Figure 10). Adolescent girls with menstrual blood flow of more than 5-day duration were 6.21 (95% CI: 1.67, 23.12) times more likely to be anemic than adolescent girls having less than 5 days of menstrual bleeding (Figure 11).

Forest plot showing the association between dietary diversity score and anemia among adolescent girls in Ethiopia, 2022.

Forest plot showing the association between maternal illiteracy and anemia among adolescent girls in Ethiopia, 2022.

Forest plot showing the association between household size and anemia among adolescent girls in Ethiopia, 2022.

Forest plot showing the association between household food insecurity and anemia among adolescent girls in Ethiopia, 2022.

Forest plot showing the association between menstrual flow duration and anemia among adolescent girls in Ethiopia, 2022.
Discussion
In Ethiopia, the combined prevalence of anemia among adolescent girls was 23.03% (95% CI: 17.07, 28.98). Anemia among adolescent girls was found to be lower in this study than in studies conducted in Sudan, 40 India,41,42 and Nepal.43,44 This result, however, was higher than many other studies undertaken in Turkey (8.3%), 45 Kavar Urban Area, Southern Iran (5.8%), 46 and China (7.4%). 47 The differences may be a consequence of variations in study participants, socio-demographic characteristics, sample size, study period, and time.
The prevalence of adolescent girl’s anemia differ substantially across Ethiopian regions, according to subgroup analyses, while the differences were not significant based on study settings, publication year, or study area. The Somali region had the highest anemia prevalence (27%) among adolescent girls, while anemia was less widespread in the Amhara region (18.24%). The diversity in anemia prevalence among Ethiopian areas could be related in part to differences in economic, socio-demographic, and nutritional differences, as well as the amount of food security. The discrepancy could potentially be explained by the difference in study numbers included in each group (region). Different cultural practices that predispose girls to be anemic, such as female genital mutilation, may be other reasons.
The prevalence of anemia in adolescent females and their families differed according to some predator characteristics, with statistically significant differences for some parameters but not for others. We discovered that the severity of anemia is unaffected by adolescent girls’ age or menstrual history. The dietary diversity status of adolescent females, on the other hand, was a statistically significant predictor of anemia in adolescent girls. In comparison with their counterparts, girls who did not eat a diverse diet were more likely to be anemic. This is supported by research conducted in Nigeria 48 and West Uganda. 49 Diversification of diets clearly improves the micronutrient adequacy of the diet. As a result, an undiversified diet is a proxy indicator of inadequate micronutrient consumption, raising the risk of anemia and other micronutrient deficiencies in adolescents. 50 In another perspective, the disparity could be due to seasonality.
Adolescent girls from food-insecure families were more likely to be anemic than girls from food-secure families. The finding is similar to the study conducted in Bangladesh. 51 Food insecurity can lead to anemia due to insufficient consumption of micronutrients, 52 and food-insecure households tend to consume fewer micronutrients as a result of under- or over-consumption of energy-dense foods with fewer micronutrients, which facilitate iron bioavailability. 53
Furthermore, the findings of four research combined revealed that adolescent females from families with more than five members were 1.65 times more likely to be anemic than those from families with fewer than five members. Bonga town, southwest Ethiopia, 15 Tang ail region of Bangladesh, 54 and Khordha Rural District of Odisha in India, 41 all agree with this conclusion. This could be because the big size of the family is linked to poor care for each family member and a lack of family money in those research locations, making it difficult to access a range of foods high in iron and other micronutrients.
Adolescent girls with illiterate mothers, on the other hand, were 1.81 times more likely to be anemic than girls with literate mothers. This finding matches that of a research conducted in India. 41 The explanation for this could be explained by the fact that when parents’ educational status improves, so does their economic status and nutritional diversity. This leads to improved feeding practices and better adolescent girl health care.55,56 It could be because a well-educated mother is more likely to provide sufficient nutrition to her family, as mothers prepare or manage the majority of a family’s meals in Ethiopia.
Finally, adolescent girls who had more than 5 days of menstruation were 6.21 times more likely to be anemic than girls who had less than 5 days of menstruation. Similar findings were observed in Bangladesh’s Tang ail region, 54 India’s Guntur, Andhra Pradesh, 57 Odisha’s Khordha rural district, 41 and Western Kenya. 58 This could be caused by blood loss during menstruation.59,60
Age and adolescent menses status were not shown to be significantly associated to anemia in adolescent girls in this systematic review and meta-analysis. This might be because anemia is more common in girls with excessively long menstrual duration than it is in girls with regular menstrual periods. In relation to age, the adolescent girl’s growth spurt happens during the early stages of adolescence, before the iron reserve started to deplete.
Strength and limitations of the study
The review investigated at all of the literature and attempted to include all of the factors linked to adolescent anemia. As a limitation of this review, all of the studies included were from four regions of Ethiopia, which may not accurately reflect the true prevalence of anemia among adolescent females. Furthermore, because all of the studies included in this review were cross-sectional in design, they may not be reflective of the seasonal variation in anemia status among adolescent girls, and the snapshot character of the design makes it difficult to establish a causal temporal association. In addition to the foregoing, this review only included items written in the English language.
Conclusion
In this review, the pooled prevalence of anemia among adolescent girls in Ethiopia was moderately high. Household size, maternal educational status, household food security, DDS, and menstrual duration were identified as statistically significant factors of anemia among adolescent girls in Ethiopia. These barriers of the second window of opportunity should be mitigated to ensure the adolescent growth spurt.
Iron supplementation is particularly suggested for adolescent females who have a menstrual cycle that lasts longer than 5 days to avoid anemia. To combat the prevalence of anemia, adolescent females should be offered health education to enhance health, particularly on dietary diversity. Nutritional education via the media is also crucial.
Supplemental Material
sj-docx-2-whe-10.1177_17455057221129398 – Supplemental material for Menstrual abnormality, maternal illiteracy, and household factors as main predictors of anemia among adolescent girls in Ethiopia: Systematic review and meta-analysis
Supplemental material, sj-docx-2-whe-10.1177_17455057221129398 for Menstrual abnormality, maternal illiteracy, and household factors as main predictors of anemia among adolescent girls in Ethiopia: Systematic review and meta-analysis by Fitsum Endale, Demelash Woldeyohannes, Fanuel Belayneh, Aiggan Tamene, Aklilu Habte, Addisalem Gizachew, Dawit Sulamo, Yohannes Kebede, Janet Yohannes, Tadesse Mekonen and Denebo Akiso in Women’s Health
Supplemental Material
sj-docx-3-whe-10.1177_17455057221129398 – Supplemental material for Menstrual abnormality, maternal illiteracy, and household factors as main predictors of anemia among adolescent girls in Ethiopia: Systematic review and meta-analysis
Supplemental material, sj-docx-3-whe-10.1177_17455057221129398 for Menstrual abnormality, maternal illiteracy, and household factors as main predictors of anemia among adolescent girls in Ethiopia: Systematic review and meta-analysis by Fitsum Endale, Demelash Woldeyohannes, Fanuel Belayneh, Aiggan Tamene, Aklilu Habte, Addisalem Gizachew, Dawit Sulamo, Yohannes Kebede, Janet Yohannes, Tadesse Mekonen and Denebo Akiso in Women’s Health
Supplemental Material
sj-xls-1-whe-10.1177_17455057221129398 – Supplemental material for Menstrual abnormality, maternal illiteracy, and household factors as main predictors of anemia among adolescent girls in Ethiopia: Systematic review and meta-analysis
Supplemental material, sj-xls-1-whe-10.1177_17455057221129398 for Menstrual abnormality, maternal illiteracy, and household factors as main predictors of anemia among adolescent girls in Ethiopia: Systematic review and meta-analysis by Fitsum Endale, Demelash Woldeyohannes, Fanuel Belayneh, Aiggan Tamene, Aklilu Habte, Addisalem Gizachew, Dawit Sulamo, Yohannes Kebede, Janet Yohannes, Tadesse Mekonen and Denebo Akiso in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.