
Abstract
Objective
Non-steroidal anti-inflammatory drugs are used as first-line treatment of primary dysmenorrhea, but there has been no optimal clinical choice among non-steroidal anti-inflammatory drugs yet. The present study was to assess the relative benefits of different common non-steroidal anti-inflammatory drugs for primary dysmenorrhea patients with a network meta-analysis.
Methods
Randomized controlled trials were screened by our criteria and included in the network meta-analysis. Pain relief was considered as primary outcomes and adverse effect was supplied as a safety outcome, while additional rescue, assessment score, and pain intensity difference were secondary outcomes. All the indexes were evaluated with odds ratio or standardized mean difference. Surface under cumulative ranking curve result was used to calculate the ranking of each treatment.
Results
Totally, 72 randomized controlled trials of 5723 patients and 13 drugs were included in our study after screening. As for pain relief, all drugs except nimesulide, rofecoxib, and waldecoxib were superior to aspirin (odds ratio with 95% credible intervals, diclofenac: 0.28 (0.08, 0.86), flurbiprofen: 0.10 (0.03, 0.29), ibuprofen: 0.32 (0.14, 0.73), indomethacin: 0.21 (0.07, 0.58), ketoprofen: 0.25 (0.10, 0.64), mefenamic acid: 0.28 (0.09, 0.87), naproxen: 0.31 (0.15, 0.64), piroxicam: 0.15 (0.03, 0.59), and tiaprofenic acid: 0.17 (0.04, 0.63)). Aspirin also required additional rescue when compared with the majority of other drugs (flurbiprofen: 3.46 (1.15, 11.25), ibuprofen: 6.30 (2.08, 20.09), mefenamic acid: 7.32 (1.51, 37.71), naproxen: 2.66 (1.17, 6.55), and tiaprofenic acid: 9.58 (1.43, 94.63)). As for assessment of the whole treatment, ketoprofen, naproxen, rofecoxib, and ibuprofen got higher score significantly than placebo. In addition, ibuprofen performed better than placebo in pain intensity difference. Considering the safety, tiaprofenic acid and mefenamic acid were noticeable in low risk, and indomethacin revealed higher risk than any other drugs. According to the results of network analysis and surface under cumulative ranking curve, flurbiprofen was considered to be the best one among all the treatments in efficacy, and aspirin was worse than most of others. On the other hand, tiaprofenic acid and mefenamic acid were indicated as the safest drugs.
Conclusion
Considering the efficacy and safety, we recommended flurbiprofen and tiaprofenic acid as the optimal treatments for primary dysmenorrhea.
Keywords
Introduction
Dysmenorrhea is commonly divided into two types: primary dysmenorrhea (PD) and secondary dysmenorrhea. PD is defined as the hypogastric pain originated from uterine without pathology during menstrual period which often occurs with the menarche or after the establishment of the ovulatory cycles of reproductive women and usually lasts two or three days during each period. 1 About 43%–91% adolescent females (under 20 years) are reported with PD and show a decreasing tendency as the age grows older. 2 Women experiencing severe PD will be debilitated to accomplish daily works, even absent from school or job. According to the previous studies, PD is often considered to be the result of abnormal prostaglandin release which leads to strong contracts of uterus and reduced oxygen supply to the uterus muscles. 3 Besides, unhealthy lifestyle (such as smoking, intemperance, and stressfulness) and family history may also have some negative influence on the symptoms of PD. 4
There are several treatments for PD like non-steroidal anti-inflammatory drugs (NSAIDs), oral contraceptive drugs, physical therapy interventions, Chinese traditional herbology, and so on. 5 Among them, NSAIDs are the first-line treatment. 6 There are many types of NSAIDs which are widely used as analgesics and anti-inflammatory agent through inhibiting cyclooxygenase (COX) enzymes including COX-1 and COX-2. The pain relieve ability of NSAIDs is mainly attributed to COX-2 enzymes inhibition—an important pathway related to hormone release and the process of inflammation, while their adverse effects (such as indigestion, headaches, and lethargy, which are considered to be the most concerning adverse effects in PD patients) are thought to be involved with the COX-1 enzymes inhibition.7,8 Recently, selective COX-2 inhibitors have been established to mitigate the adverse effects in gastrointestinal tract and extend the drug effects with lower dose. 9 However, this kind of drug has been discovered to be related to increase the risk of heart complications if taken regularly and thus should be used more prudently. 10 Therefore, the requirement to evaluate efficacy and safety of NSAIDs is imminent for patients with PD.
To date, a large number of randomized controlled trials (RCTs) assessing the efficacy and safety of NSAIDs have been conducted,11,12 and several published meta-analysis studies also compared the mainly used NSAIDs in the PD treatment. 13 However, the traditional meta-analysis only evaluates the direct comparison of pair-wised drugs, and there also exists conflict between different studies. Therefore, the purpose of this network meta-analysis is to indicate the relative efficacy and safety among most of the NSAIDs through not only direct but also indirect comparisons. We expect to draw a conclusion about the optimal treatment of PD by analyzing all published RCTs data of 13 individual NSAIDs.
Materials and methods
Literature search and selection criteria
We searched through China National Knowledge Internet, MEDLINE, and Embase to obtain the relevant RCTs comparing the efficacy and safety of NSAIDs for patients with PD using the key words “primary dysmenorrhea,” “randomized controlled trial,” “non-steroidal anti-inflammatory agents,” “aspirin,” “diclofenac,” “flurbiprofen,” “ibuprofen,” “indomethacin,” “ketoprofen,” “mefenamic acid,” “nimesulide,” “piroxicam,” “rofecoxib,” “tiaprofenic acid,” and “valdecoxib” in searching process (Supplemental Material). As for ketorolac and celecoxib, they were not been included in this network meta-analysis due to their serious adverse effects and main function which are often in the treatment in arthritis.
One RCT would be included in this network meta-analysis if it fulfilled each of the following criteria: (1) trials evaluating the efficacy or safety of NSAIDs in patients with PD, (2) trials that were designed as single-/double-/triple-blind, (3) trials covering at least one of the outcomes of interest, and (4) trials that using the same or close evaluation index (the way to describe the pain intensity difference and other outcomes). Two investigators independently reviewed abstracts and studies to evaluate the trial eligibility, and all conflicts were solved through discussion. There was no language restriction.
Outcome measures and data extraction
The primary efficacy outcome was pain relief (the proportion of patients who received effective or at least moderate pain relief), and the incidence of total treatment-related adverse effects like insomnia and gastrointestinal disease was added as a complementally safety outcome. As for secondary outcomes, we also assessed the requirements for additional rescue and pain intensity difference from baseline to end point. Using rescue medication or other medical assistance beyond the trials during specified time periods would be regarded as additional rescue. Pain intensity difference was defined as change scores of pain intensity rated by patients from baseline to end point. Assessment of the whole treatment from patients in each trail was also included in the secondary outcome; a higher score represents a better global assessment of patients. 11 However, since all these outcomes contained more than one score scale, we standardized each continuous data during analysis.
After excluding the studies that failed to fulfill the criteria, two independent reviewers screened each study and extracted relevant data concerning of the outcomes of this network meta-analysis. The main information was extracted including basic study background, enrollment numbers, detailed interventions, and outcome measures.
Statistical analysis
We used a Bayesian framework with STATA software (13.0) and R software (V3.3.1) for this network meta-analysis. One advantage of using the Bayesian framework was its ability to produce ranking probabilities which could be used to evaluate medications with respect to each end point. The forest plots showed the result of the meta-analysis included in this research. Furthermore, odds ratio (OR) and standardized mean difference were calculated for dichotomous outcomes and continuous outcomes, respectively, with 95% credible intervals (CrIs) between the two treatments on each outcome. Moreover, the surface under the cumulative ranking curve (SUCRA) was computed based on the outcomes above to estimate the performance of different interventions, and higher SUCRA represented better efficacy and safety. The inconsistency of each outcome between direct and indirect evidence was evaluated by node-splitting results and the heat plots.
Results
Study selection and characteristics of included trials
A total of 1476 potentially relevant publications were identified by literature research. Then, 316 publications were removed as duplicates and 1039 publications were excluded due to the weak relevance to the subject. As a result, we retrieved 121 publications with full length into systematic review and included 70 studies with 72 RCTs of 5723 patients into our network meta-analysis due to the selection criteria as shown earlier.11,12,14–81 The flowchart of the whole process is shown in Figure 1. Among the 70 studies, 18 trials were three-arm studies, 48 trials were conducted between one intervention and placebo, and 6 trials were between two different interventions. All trials included 13 drugs as follows: aspirin, diclofenac, flurbiprofen, ibuprofen, indomethacin, ketoprofen, mefenamic acid, mefenamic, nimesulide, piroxicam, rofecoxib, tiaprofenic acid, and valdecoxib. The network structure is shown in Figure 1 and Figure S1, the circle area represented the enrollment of each treatment, and lines width showed the number of compared trials. Main characteristics of the included publications and trials are presented in Table 1.

Flowchart and network structure for pain relief. The network plots show direct comparison of different drugs, with node size corresponding to the sample size. The number of included studies for specific direct comparison decides the thickness of solid lines.
Main characteristics of included studies.
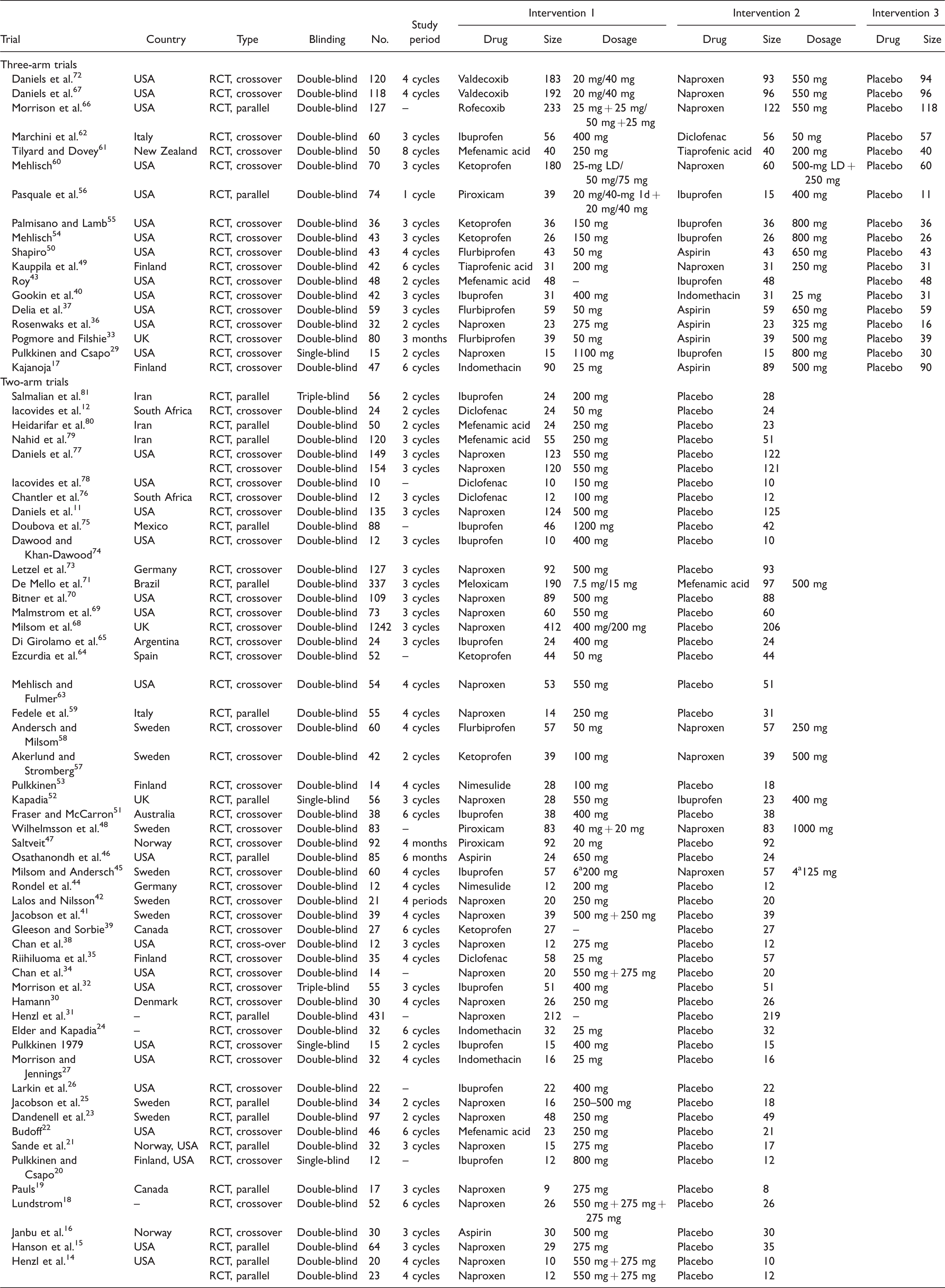
Note: RCT: randomized controlled trials.
aThe article does not mention the type of dysmenorrhea. 1d: Day 1.
Overall outcomes
All the data of this network meta-analysis results for five outcomes are presented in Tables 2 to 4 and the forest plots in Figure 2 and Figures S2 to S5. For the primary outcomes shown in Table 2, the comparison between each pair of drugs was evaluated. As for pain relief, all drugs except aspirin were superior to placebo. When aspirin was compared with other drugs, the results showed that it was worse than most of the drugs such as diclofenac (OR = 0.28, 95% CrI = 0.08–0.86), indomethacin (OR = 0.21, 95% CrIs = 0.07–0.58), and flurbiprofen (OR = 0.10, 95% CrI = 0.03–0.29), and so on. On the other hand, considering the safety, tiaprofenic acid and mefenamic acid were noticeable in low incidence of adverse effects, and indomethacin revealed higher adverse effects than any other drugs.
Network meta-analysis results for pain relief (lower left) and adverse effects (upper right).

Note: The column treatments are compared against row treatments.
Network meta-analysis results for additional rescue (lower left) and assessment (upper right).
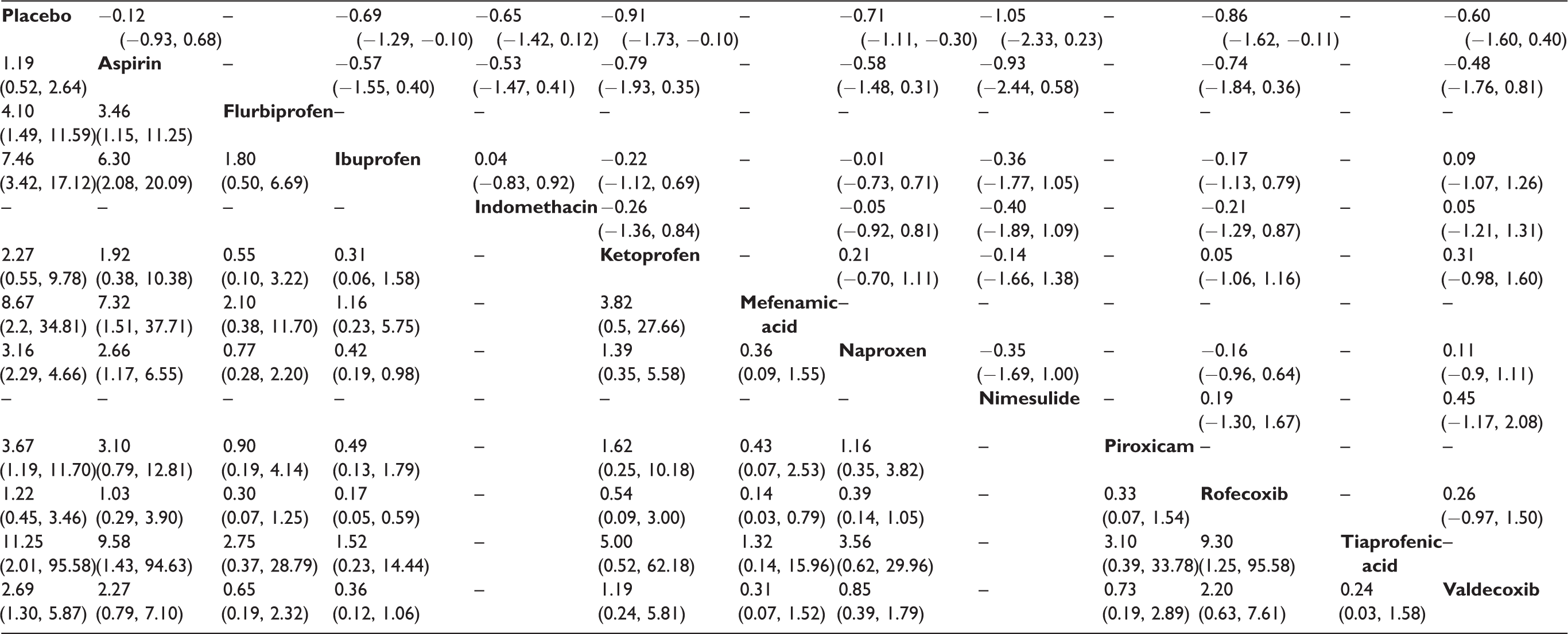
Note: The column treatments are compared against row treatments.
Network meta-analysis results for secondary pain intensity difference.

Note: The column treatments are compared against row treatments.

Forest plots for pain relief using ORs and 95% CrIs. OR: odds ratios; Crls: credible intervals.
The secondary outcomes of this network meta-analysis are listed in Tables 3 and 4. According to the outcomes, most of the drugs needed less additional rescue after assigned interventions compared with placebo. Nevertheless, aspirin still required additional rescue when compared with the majority of other drugs. As for assessment of the whole treatment, ketoprofen, naproxen, rofecoxib, and ibuprofen got higher score significantly than placebo. In addition, ibuprofen performed better than placebo in pain intensity difference.
Ranking conclusion
The results of SUCRA under five outcomes are shown in Table 5. According to the standing list of the primary outcomes, flurbiprofen (SUCRA: 0.904) ranked first in pain relief, successively followed by piroxicam (SUCRA: 0.787), tiaprofenic acid (SUCRA: 0.751), and indomethacin (SUCRA: 0.678). Besides, aspirin was indicated to be the worst among all of the NSAIDs in pain relief. In terms of adverse effects, the lower SUCRA suggested the higher incidence of adverse effects. Tiaprofenic acid (SUCRA: 0.872) performed best with mefenamic acid (SUCRA: 0.824) and ketoprofen (SUCRA: 0.781) followed. Combining these two primary outcomes, flurbiprofen was the most efficacious treatment in our result, and tiaprofenic acid was also a good treatment when took efficacy and safety into consideration. The ranking in secondary outcomes also revealed the excellent performance of these drugs. In addition, aspirin was considered to be the worst intervention because it ranked last among all the interventions except for placebo in most outcomes.
Surface under the cumulative ranking curve (SUCRA) results of six outcomes.

Note: The warm color represents a high SUCRA value, which also suggests a relatively high ranking.
Inconsistency test
Node-splitting analysis of five outcomes for all the drugs is shown in Tables 6 and 7. A value of P less than 0.05 indicated that there was a significant inconsistency. As the results of the analysis show that there was no significant difference in the outcome of pain relief, additional rescue, pain intensity difference, and assessment. As for the outcome of adverse effects, inconsistency between flurbiprofen and aspirin (P = 0.012), as well as naproxen and flurbiprofen (P = 0.036), was found. The net heat plot results of consistency test are also shown in Figure 3 and Figures S6 to S9, which revealed the same result.
Node-splitting results of the network meta-analysis for three dichotomous outcomes.

Note: Three dichotomous end points include pain relief, adverse effects, and additional rescue. Direct, indirect, or network odds ratios (ORs) and 95% credible intervals (CrIs) indicate the relative efficacy or safety. Bold values means P-value is smaller than 0.05, which indicated that there was significant inconsistency.
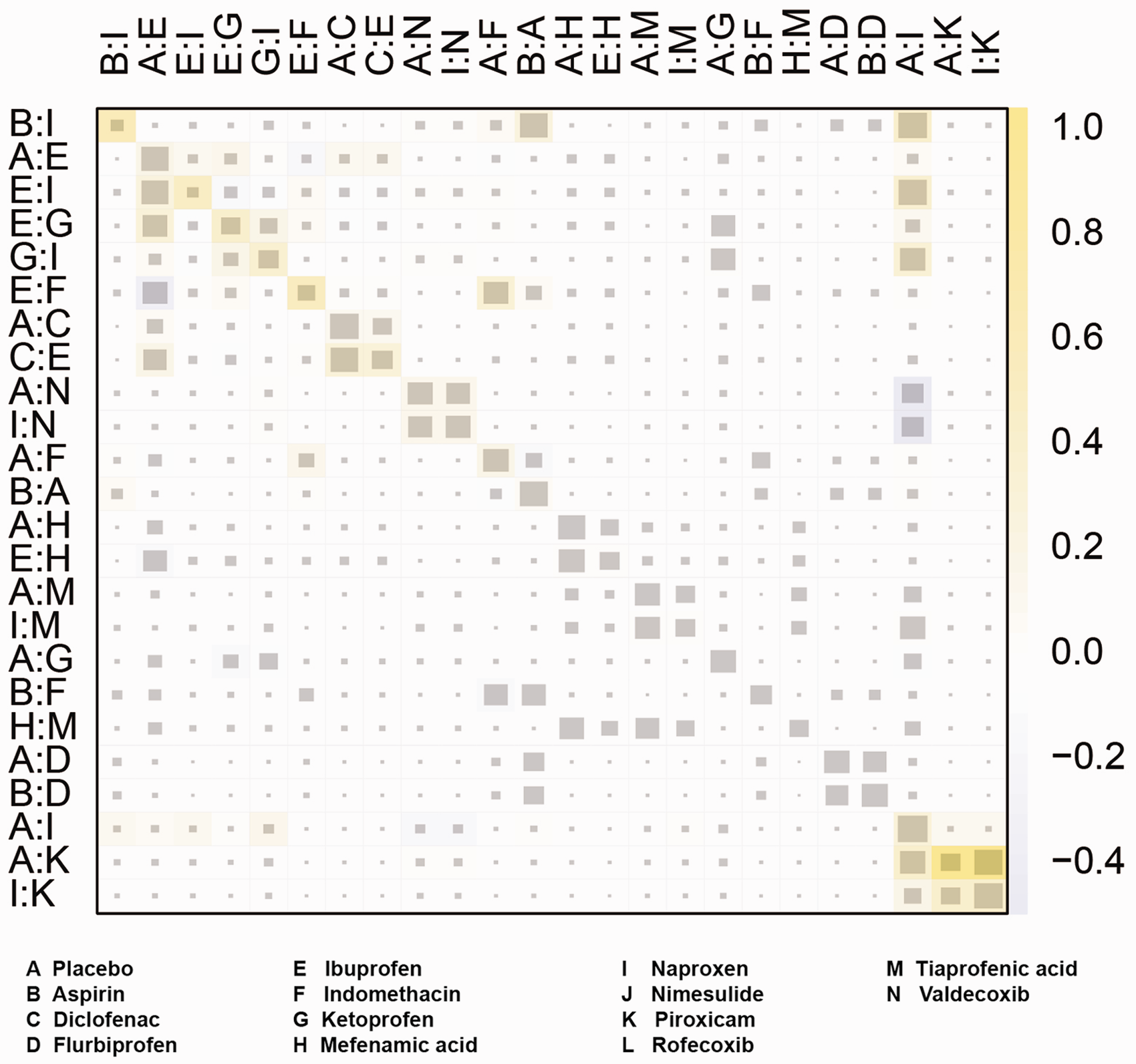
Heat plots for pain relief. The size of the gray squares indicates the contribution of the direct evidence (shown in the column) to the network evidence (shown in the row). The colors are associated with the change in inconsistency between direct and indirect evidence. Blue colors indicate an increase in inconsistency, and warm colors indicate a decrease in inconsistency.
Node-splitting results of the network meta-analysis for two continuous outcomes.
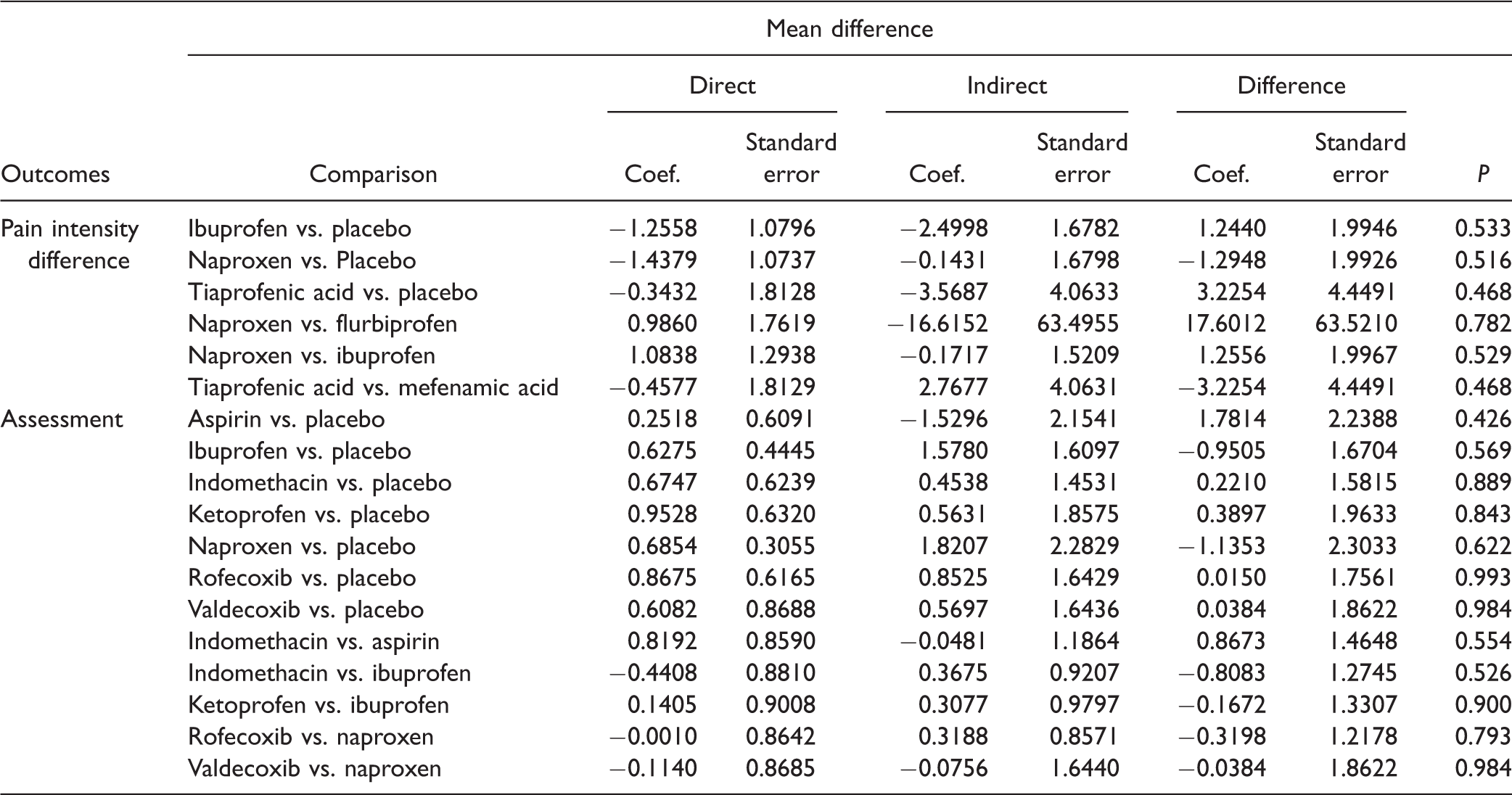
Note: Three continuous outcomes include pain intensity difference and assessment. Direct, indirect, or network results of standardized mean difference and standard error indicate the relative efficacy or safety.
Discussion
PD is a high-frequency female disease which will disturb the quality of normal lives of women. 82 NSAIDs are considered to be the first-line treatment for patients with PD; they are certain to be effective in relieving pain, but there is still no conclusion about the optimal choice in clinic. 13 Therefore, the objective of this network meta-analysis is to draw a conclusion about the optimal treatment within several types of NSAIDs through direct and indirect statistical analysis. Although only a small amount of studies in our database performed in the recent years, the results of our research were still meaningful since NSAIDs system has been developed a long time ago and maintained its crucial role in relieving PD in the last 30 years.
The results of our network meta-analysis suggested that all the drugs except aspirin were significantly more efficacious than placebo. However, there is no significant difference between each pair of NSAIDs concerning pain relief through direct evidence, which is consistent with the research by Marjoribanks et al. 3 In their research, they pointed out that NSAIDs were effective in relieving dysmenorrhea, whereas the sample size was too small to conduct a suitable meta-analysis for the comparison between two NSAIDs. Complementary to their results, the SUCRA ranking in our research provided the information of more efficacious treatments: flurbiprofen, piroxicam, and tiaprofenic acid. Naproxen was an analgesic that has been applied widely in many disease and showed significant relief of pain in PD in early time. 38 However, with the development of NSAIDs drugs, several other drugs have been illustrated as similar efficacy to naproxen.11,73 In our result, naproxen was not significant efficacious compared to other NSAIDs drugs and showed an average efficacy in ranking.
As for the safety outcome, tiaprofenic acid and mefenamic acid were indicated as the safest NSAIDs drugs, while indomethacin was the worst one which was more likely to cause mild gastrointestinal discomfort. Naproxen, different from the research by Marjoribanks et al., was not reported with higher incidence of gastrointestinal side effects according to our network meta-analysis. Importantly, it is generally believed that selective COX-2 inhibitors, for example, rofecoxib and valdecoxib, are related with higher risk of serious cardiovascular disease with long-term usage. 9 Accordingly, our research demonstrated that the inferior performance of both rofecoxib and valdecoxib which were already announced withdrawal from the U.S. market in 2004 and 2005, respectively. Furthermore, it should be noted that flurbiprofen and tiaprofenic acid revealed good efficacy and were recommended to be the suitable choices for the patients with severe adverse effects. The safety ranking of flurbiprofen was not ideal in our results; however, the inconsistency of direct and indirect evidence was significant between flurbiprofen and naproxen as well as flurbiprofen and aspirin. Besides, there was only one trial having direct comparison of each pair. Thus, the relevant safety of flurbiprofen lacked enough credibility, and more researches are needed in the future.
Although the result of our network meta-analysis was relatively comprehensive, there were still several limitations which may affect the strength of each result. Firstly, even though the trials included in the research were various, the population employed was small scale (many trials included less than 100 people), and the reliability of the data was lightly weakened, especially in recommended NSAIDs like tiaprofenic acid (assessed in only 71 patients). Moreover, the availability and cost of these drugs have not been taken into consideration when they are regarded as recommended therapies. Secondly, we only evaluated the difference of efficacy and safety among NSAIDs but overlooked the dosage and frequency factor related to one drug. Also, we did not provide the optimal intake way of one single drug. Furthermore, previous studies have mentioned that the symptoms of PD were similar to the adverse effects of drug treatments which may also reduce the credibility of the results. 63 Thirdly, some included studies are pharmaceutically funded and may have risks of bias, though it can be adjusted with network meta-analysis method in some degree.
In conclusion, according to our network meta-analysis, we advocate flurbiprofen and tiaprofenic acid as the recommended NSAIDs therapies for patients with PD. Naproxen, as a well-established drug, did not show superior in efficacy or safety in our result. More efforts need to be made to further explore the characteristic of NSAIDs for PD patients.
Supplemental Material
Supplemental material for Comparison of the efficacy and safety of non-steroidal anti-inflammatory drugs for patients with primary dysmenorrhea: A network meta-analysis
Supplemental material for Comparison of the efficacy and safety of non-steroidal anti-inflammatory drugs for patients with primary dysmenorrhea: A network meta-analysis by Xuan Feng and Xiaoyun Wang in Molecular Pain
Footnotes
Author Contributions
XF contributed to research conception and design, data analysis, interpretation, and drafting of the manuscript. XW contributed to data analysis, interpretation, and statistical analysis. XW and XF are involved in critical revision of the manuscript, approval of final manuscript, and taking public responsibility for appropriate portions of the content.
Supplemental Material
Supplementary material is available for this article online.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Lingnan traditional Chinese medicine gynecology treatment of menstruation and clinical study (No. 2013B032500013) and State Administration of Traditional Chinese Medicine (16MLZY02), 2016 National Famous Traditional Chinese Medicine Expert Inheritance Studio Construction Project-Wang Xiaoyun Chinese Medicine Office.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.