
Abstract
Therapies treating psoriasis can be categorized into five classes according to their mechanism: anti-metabolites (AM), anti-interleukin-12/23 agents (anti-IL12/23), anti-interleukin-17 agents (anti-IL17), anti-T-cell agent (ANT), and anti-tumor necrosis factor-α agent (anti-TNF-α). This network meta-analysis (NMA) aimed to give a quantitative and systemic evaluation of safety and efficacy for the five kinds of therapies mentioned above. Odds ratios and mean differences were calculated to evaluate binary and continuous outcomes, respectively. Forest plots were conducted to show the performance of pair-wise comparison of above therapies in each outcome, and surface under the cumulative ranking curves was given to evaluate the relative ranking of above therapies in each outcome. Node splitting was conducted to evaluate the consistency between direct and indirect evidence. Direct comparisons from 65 studies (32,352 patients) were included in this NMA. Our results showed an excellent efficacy of anti-IL12/23 and anti-IL17. However, these two therapies and anti-TNF-α were revealed to have a high possibility to cause adverse effects (AEs) such as infections. Additionally, node splitting showed that no inconsistency appeared between the direct and indirect comparisons. Anti-IL12/23 was the most recommended therapy according to this NMA. Anti-IL17 had similar efficacy to anti-IL12/23 but should be applied with caution since it has poor performance in safety outcomes.
Introduction
Psoriasis, characterized by quick and excessive growth of the skin’s epidermal layer, 1 is a common, chronic, and systemic disease, affecting 1–3% of the world population. It is widely considered as a genetic disease and could be affected by some environmental factors. 2 Up to now, various therapies are available for psoriasis, including phototherapy, topical treatment, systemic therapies, and biologic drugs. 3
The biologic drugs can be classified into five classes based on their mechanism: anti-metabolites (AM), anti-tumor necrosis factor-α agent (anti-TNF-α), anti-T-cell agent (ANT), anti-interleukin-12/23 agents (anti-IL12/23), and anti-interleukin-17 agents (anti-IL17). It is reported that methotrexate, an AM, has been applied as a valid systemic treatment for psoriasis patients over 48 years. 4 However, it is relevant to hepatotoxicity and myelosuppression. 5 Besides, the TNF is widely regarded as an important cytokine involved in the pathophysiology of psoriasis. Therefore, monoclonal antibodies, such as adalimumab and infliximab, which antagonized TNF, were applied in the treatment of psoriasis.6,7
Relevant studies showed that psoriasis was possibly an autoimmune disease where the activation of skin-directed T-cells performed an important role. 8 Alefacept, a recombinant protein, has the ability to block T-cell’s proliferation and activation by combining with CD2 on the surface of T-cells. Alefacept can also induce selective CD45RO+ T-cell apoptosis by interacting with the immunoglobulin receptors FcγRIII on the accessory cells. 9 Other drugs, such as efalizumab and itolizumab, are humanized monoclonal antibodies which could directly deal with the pathogenic T-cells by binding to CD11a or CD6 and inhibit T-cell functions, such as activation, trafficking, and migration.10–12
Meanwhile, it has been discovered that TNF is produced by the immune pathways stimulated by two interleukins, interleukin-12 (IL-12) and interleukin-23 (IL-23). 13 This discovery indicates that both IL12 and IL23 play a pivotal role in the psoriasis development. In addition, IL-17A and IL-17RA were also found related to the disease severity because of the elevated levels of IL-17A in the diseased skin and blood of patients with psoriasis. 14 Etanercept, a human fusion TNF soluble receptor, is used to prevent the TNF-mediated inflammatory response and applied for the therapy of psoriatic arthritis and chronic plaque. 15
To make an effective and safe decision in treatment of psoriasis, it is necessary to conduct reliable evidences of comparison among these drugs. A number of traditional meta-analysis studies had been done to make comparison between two therapies, which indicated that all the therapies are more effective than placebo (PBO). But they cannot compare several therapies simultaneously. Therefore, the network meta-analysis (NMA) is required to synthesize all valuable evidences from randomized control trials (RCTs), combining both direct and indirect evidences, to convincingly draw the conclusions about competitive efficacy and safety information.
Woolacott et al. made the comparisons among three biological therapies, efalizumab, infliximab, and etanercept, and two nonbiological therapies. 16 Adalimumab was taken into consideration in the work of Bansback et al. 17 After then, with the development of biological treatment, more NMA were conducted, such as the works of Reich et al. 18 and Lin et al., 19 who added the ustekinumab, which antagonizes IL-12/23p40. Besides, Nast et al. 20 assessed the efficacy and safety of treatments of systemic long-term treatments. Recently, Gomez-Garcia et al. 21 used the new 2015 PRISMA statement for the NMA and evaluated the comparative short-term efficacy and tolerance of the agents. Jabbar-Lopez et al. established the relative efficacy and tolerability of six monoclonal antibodies. None of them compared the biotics from the level of large classes.
The primary objective of our study was to give an extension to the existing NMAs to evaluate the efficacy and safety of different treatment agents. More agents were taken in account to provide more reliable conclusion. Moreover, the ranking possibility in specific efficacy and safety were also presented to help making optimal decision in clinical drug using. Besides, no NMA similar to this study, with sufficient samples and consideration of all therapies, had been done yet.
Materials and methods
Search strategy
To get the relevant studies, the following three electronic databases were taken into our retrieval: Chinese National Knowledge Infrastructure, PubMed, and Embase. Regardless of the limitation of language, key terms “psoriasis,” “antimetabolites,” “macrolides,” “antibodies, monoclonal,” “etanercept” as well as their acronyms were searched in this work. Besides, the reference lists were examined to identify the potentially available studies.
Inclusion and exclusion criteria
All included trials must satisfy the following criteria: (i) the studies must be RCTs; (ii) the patients involved in the studies must be diagnosed as psoriasis; and (iii) relevant outcomes should be contained. Besides, duplicate RCTs or the studies with isolated comparison were excluded.
Outcome measure and data extraction
Data extraction was conducted by two reviewers independently, and following characteristics of each study were extracted from the original documents: (i) the basic information, including the first author, country, published year, and blinding; (ii) the patients characteristics, including ages, gender ratio, and disease duration; (iii) efficacy outcomes, including the Psoriasis Area and Severity Index (PASI), Dermatology Life Quality Index (DLQI), and Physician’s Global Assessment (PGA); (iv) safety outcomes, including the incidence of all AEs, infection, nasopharyngitis, headache, and upper respiratory tract infection (URTI).
Statistical analysis
Odds ratio (OR) with corresponding 95% credible interval (CrI) were used to evaluate the binary outcomes. Mean difference with corresponding 95% CrI were applied to assess the continuous outcomes. Meanwhile, forest plots were drawn to visually present the relative efficacy and safety of different comparisons for each outcome. Consistency between direct and indirect comparison was analyzed by the node-splitting method. p<0.05 indicated a significant inconsistency for a specific comparison. Moreover, surface under the cumulative ranking curves (SUCRAs) were calculated to present the ranking probability of each treatment to find the relatively optimal treatment to improve the efficacy and decrease the incidence of adverse events. Software R (version 3.2.3) and STATA (version 13.0) were used to implement the NMA.
Results
Included studies
In the retrieval, 1562 records were identified at the beginning, and 17 records were added manually. Among them, 573 duplicates were removed, and 989 records were left. After 242 records excluded during screening, 432 records were full-text assessed. Finally, 75 studies and 25,108 patients were included in our NMA.4–6,9–14,22–87 The flow chart was shown in Figure 1. The details of specific treatment, the characteristics of patients, and outcomes of each trail were provided in Table 1. The study sample sizes ranged from 33 to 1831. The follow-up period ranged from six weeks to 120 weeks. Among 58 trails, five trails failed to provide age range of the patients,27,29,49,59,62,70 while six trails failed to provide gender ratios of the patients.14,27,49,59,70,86 The mean disease duration was 17.5 years (range 5.6–22.8). Besides, disease severity was assessed containing all the trails with a baseline PASI score of 19.9 (range 5.5–33.1) and a body surface area (BSA) of 28.8% (range 5.1–49.8). Jadad score of included RCTs was shown in Table S1. Meanwhile, the network diagram was shown in Figure 2. The area of dots represents the number of patients in the therapy, and the width of lines stands for the number of references including the comparison.

PRISMA flow chart.
Baseline population characteristics of included studies.

HPA: history of psoriatic arthritis (%); BSA: biologic systemic agents; PASI: psoriasis area and severity index; AM: anti-metabolites; anti-TNF-α: anti-tumor necrosis factor-α agents; ANT: anti-T-cell agents; anti-IL12/23: anti-interleukin-12/23 agents; anti-IL17: anti-interleukin-17agents; PBO: placebo; MTX: methotrexate.
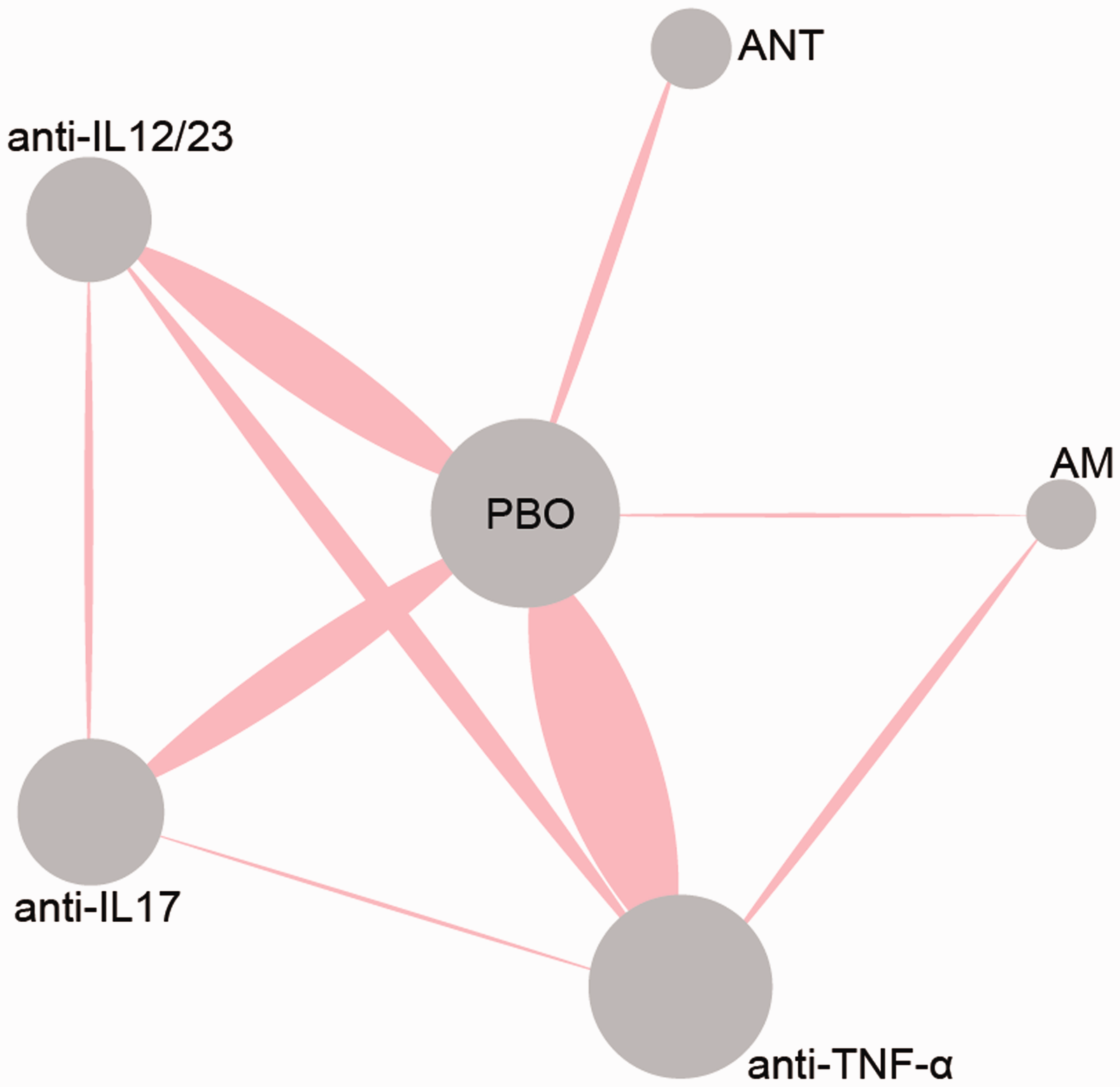
Network diagram of all included studies. Each node represents a medicine type; the diameters of circles represent the number of people involved, and the widths of lines between two nodes represent the number of study involved in the head-to-head comparison.
NMA results for PASI reduction
Table 2 showed the network comparison of different treatments for PASI reduction. In terms of PASI 75, it shows that anti-IL12/23 and anti-IL17 are significantly superior compared with PBO (OR=43.0, 95% CrI: 27.9–66.7; OR=62.2, 95% CrI: 36.6–104.6, respectively). (OR=5.9, 95% CrI: 2.5–13.7) and ANT (OR=2.44, 95% CrI: 1.3–4.8).
Network comparison of different treatments for PASI reduction in psoriasis patients.

Bold: data with statistically significant difference, which is highlighted in the upper region of each outcome. PASI 50: ≥50% reduction in psoriasis area and severity index; PASI 75: ≥75% reduction in psoriasis area and severity index; PASI 90: ≥90% reduction in psoriasis area and severity index; AM: anti-metabolites; anti-TNF-α: anti-tumor necrosis factor-α agents; ANT: anti-T-cell agents; anti-IL12/23: anti-interleukin-12/23 agents; anti-IL17: anti-interleukin-17 agents; PBO: placebo.
According to PASI 75, all the therapies had significantly higher ORs compared with PBO. Furthermore, anti-IL12/23, anti-IL17, and anti-TNF-α were estimated to be more effective than AM (OR=13.6, 95% CrI: 5.2–35.2; OR=19.5, 95% CrI: 7.0–53.0; OR=5.9, 95% CrI: 2.5–13.7, respectively) and ANT considering PASI 75 (OR=5.6, 95% CrI: 2.7–11.6; OR=8.0, 95% CrI: 3.6–17.5; OR=2.44, 95% CrI: 1.3–4.8, respectively).
For the comparison of treatments under PASI 90 reduction, all treatments were statistically more effective than PBO. Moreover, anti-IL17 was significantly better than other treatments. Meanwhile, it was revealed that anti-IL12/23 had significantly higher ORs than AM (OR=11.0, 95% CrI: 3.3–35.5) and anti-TNF-α (OR=2.39, 95% CrI: 1.19–4.62). Besides, anti-TNF-α had a better performance than AM (OR=2.2, 95% CrI: 1.2–3.9). The visualized result was also provided in Figure 3.

Forest plots for different treatment effects in psoriasis area and severity index reduction in psoriasis patients.
NMA result for DLQI and PGA
Table 3 showed the network comparison of different treatments for DLQI and PGA. In view of DQLI, only two drugs, anti-IL12/23 and anti-TNF-α were superior compared with PBO (OR=13.8, CrI: 4.6–23.3; OR=9.6, CrI: 1.2–18.1, respectively). Considering PGA, all drugs were superior compared with PBO, and anti-IL12/23, anti-IL17, and anti-TNF-α had better PGA compared with AM (OR=6.62, 95% CrI: 1.68–25.79; OR=21.54, 95% CrI: 4.57–101.49; OR=4.06, 95% CrI: 1.20–13.60, respectively) and ANT (OR=11.94, 95% CrI: 4.48–31.82; OR=38.36, 95% CrI: 11.47–134.29; OR=7.32, 95% CrI: 2.8–18.73, respectively). In addition, anti-IL17 was estimated to be superior to anti-TNF-α (OR=5.31, 95% CrI: 1.93–14.88). The forest plots were presented in Figure 4.
Network comparison of different treatments for Dermatology Life Quality Index and Physician’s Global Assessment in psoriasis patients.

Bold: data with statically significant difference, which is highlighted in the upper region of each outcome. AM: anti-metabolites; anti-TNF-α: anti-tumor necrosis factor-α agents; ANT: anti-T-cell agents; anti-IL12/23: anti-interleukin-12/23 agents; anti-IL17: anti-interleukin-17 agents; PBO: placebo.

Forest plots for different treatment effects of Dermatology Life Quality Index and Physician’s Global Assessment in psoriasis patients.
NMA result for AEs
Table 4 showed the network comparison of different treatments for adverse events. According to all adverse events (AAE), only anti-IL17 showed a significant result that it had more AAE than PBO (OR=0.68, 95% CrI: 0.48–0.97). In view of incidence of infection, anti-IL12/23, anti-IL17, and anti-TNF-α showed more infection cases than PBO (OR=1.28, 95% CrI: 1.11–1.48; OR=1.32, 95% CrI: 1.05–1.68; OR=1.28, 95% CrI: 1.12–1.48, respectively). Besides, anti-TNF-α was associated with statistically significant increased odds of nasopharyngitis compared with PBO (OR=0.64, 95% CrI: 0.42–0.94). In view of headache, few of them demonstrated a significant difference. ANT, anti-IL17, and anti-TNF-α was assessed to be worse compared with PBO (OR=1.54, 95% CrI: 1.14–2.10; OR=1.77, 95% CrI: 1.12–2.83; OR=1.40, 95% CrI: 1.06–1.88, respectively). As for URTI, only AM was associated with statistically stronger URTI compared with PBO and all the other inventions. Meanwhile, the network comparisons for incidence of withdrawal due to the AE showed that compared with patients using PBO, patients using IL12/23 or TNF-α had statistically higher possibility to keep on (OR=0.64, 95% CrI: 0.42–0.98; OR=0.64, 95% CrI: 0.46–0.92, respectively). In addition, AM was associated with higher withdrawal probability than other inventions. The forest plots of the random-effects model were shown in Figure 5.
Network comparison of different treatments for adverse events in psoriasis patients.

Bold: data with statically significant difference; in the upper regions, columns are compared with rows, while lower regions are opposite. AM: anti-metabolites; anti-TNF-α: anti-tumor necrosis factor-α agents; ANT: anti-T-cell agents; anti-IL12/23: anti-interleukin-12/23 agents; anti-IL17: anti-interleukin-17 agents; PBO: placebo.
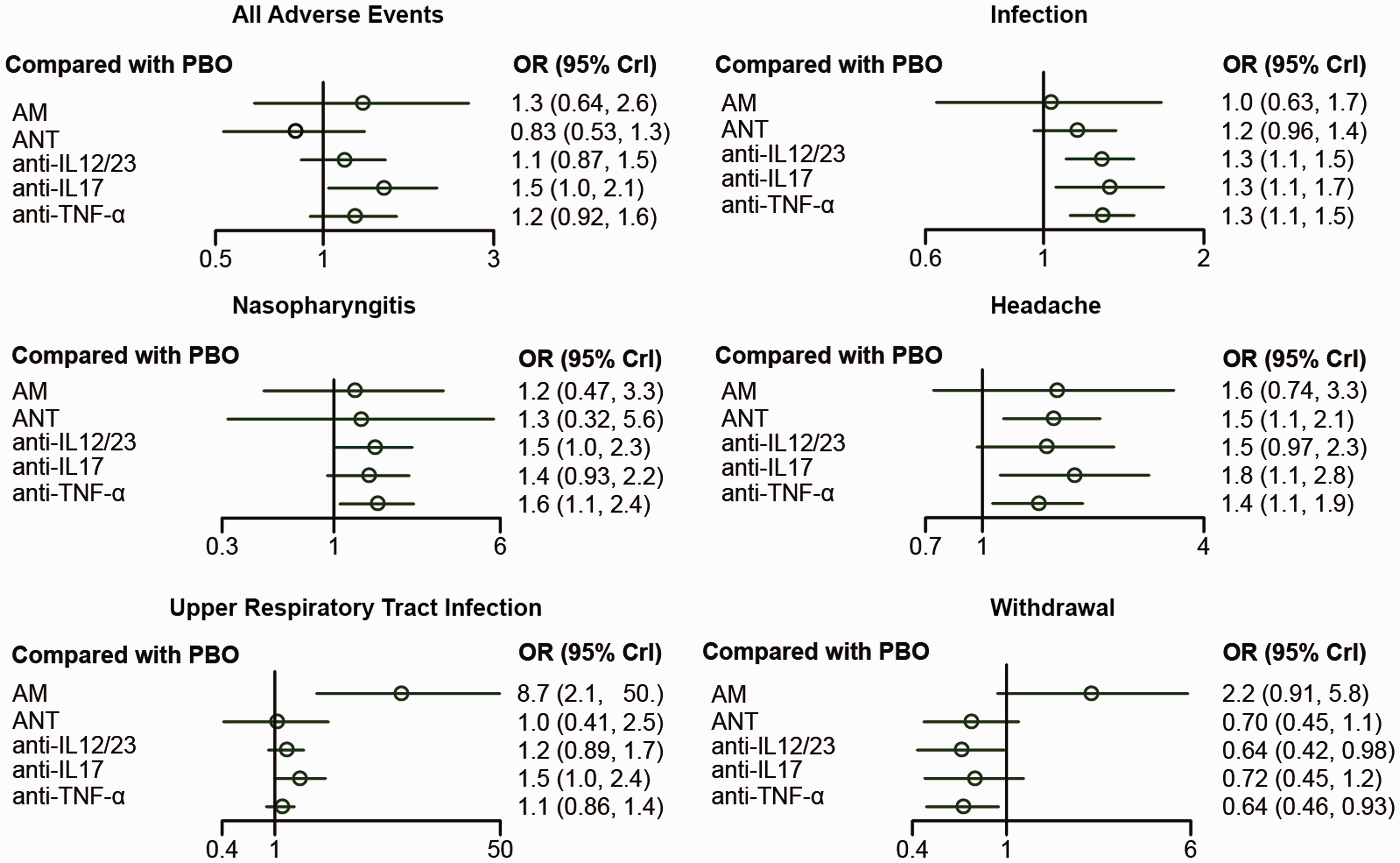
Forest plots for different treatment effects of adverse events in psoriasis patients.
Ranking of treatments
The SUCRA values for different treatments for all outcomes was calculated in order to determine the best method for curing psoriasis, and the calculated numbers were listed in Table 5. The result showed that anti-IL12/23 had better efficacy in ≥50% reduction in PASI (0.997) and led to better Dermatology Life Quality (0.842), but for better efficacy in PASI, it is indicated that anti-IL17 had the most possibility to rank the first among all six drugs (PASI 75: 0.980, PASI 90: 0.995, PGA: 0.998). Meanwhile, anti-TNF-α had good performance in PASI 50, 75, and 90. However, AM and ANT showed less efficacy. As for ranking of incidence of AE, it showed that none of the interventions were better than PBO except for ANT in AAE outcome. And anti-IL17 showed worse effect in both AAE and infection (AAE: 0.281, infection: 0.352).
Surface under the cumulative ranking curve (SUCRA) values for different treatments for all outcomes in psoriasis patients.

PASI 50: ≥50% reduction in psoriasis area and severity index; PASI 75: ≥75% reduction in psoriasis area and severity index; PASI 90: ≥90% reduction in psoriasis area and severity index; DLQI: Dermatology Life Quality Index; PGA: Physician’s Global Assessment – minimal or cleared; AAE: all adverse events; URTI: upper respiratory tract infection; AM: anti-metabolites; anti-TNF-α: anti-tumor necrosis factor-α agents; ANT: anti-T-cell agents; anti-IL12/23: anti-interleukin-12/23 agents; anti-IL17: anti-interleukin-17 agents; PBO: placebo.
Inconsistency analysis
The direct and indirect evidences for each comparison under all outcomes, as well as network results, were presented in Table 6. p<0.05 suggested a significant inconsistency between direct and indirect evidence. Overall, no inconsistency was found for each comparison under all outcomes (all p>0.05), which indicated reliable results of the current NMA.
Comparison of direct and indirect evidences of treatments for psoriasis.

URTI: upper respiratory tract infection; PASI 75: ≥75% reduction in psoriasis area and severity index; PGA: Physician’s Global Assessment – minimal or cleared; AAE: all adverse events; AM: anti-metabolites; anti-TNF-α: anti-tumor necrosis factor-α agents; ANT: anti-T-cell agents; anti-IL12/23: anti-interleukin-12/23 agents; anti-IL17: anti-interleukin-17 agents; PBO: placebo.
Discussion
Undoubtedly, as the NMA results revealed, all included therapies showed significant efficacy when compared with PBO in terms of all the efficacy outcomes except for DLQI, which in general corresponded to the results of previous RCTs. Meanwhile, the efficacy and safety of these therapies were certainly different from each other.
First of all, as was shown in the NMA results, anti-IL12/23 was proved to be the most ideal therapy among the included therapies. Its excellent efficacy as well as mild AEs was revealed. Additionally, its extraordinary efficacy and safety were also proved by previous RCTs, which corresponded with the results of previous RCT studies.25,29 Ustekinumab, an antibody agent binding to the shared p40 subunit of IL 12/23, was the most widely researched agent among the therapies mentioned above. It bound to the interleukins specifically and prevented their binding with respective receptors, thus blocked the downstream signaling cascades. 25 Meanwhile, briakinumab, another research focus with analogous structure and function with ustekinumab, also showed an excellent performance clinically. Tildrakizumab and guselkumab are also experimental monoclonal antibodies (Statement on a Nonproprietary Name Adopted by the USAN Council—Tildrakizumab; Statement on A Nonproprietary Name Adopted by the USAN Council—Guselkumab) designed to block IL-23. However, such agents still required more research to promote its clinical appliance.
Second, anti-IL17 showed a satisfactory efficacy performance in this NMA. It was revealed that this therapy had a similar efficacy with anti-IL12/23. These anti-IL17 monoclonal antibody agents including ixekizumab, brodalumab, and secukinumab selectively bind to the IL 17 and neutralize the bioactivity of this cytokine. 22 Though its efficacy was excellent, the safety of this therapy was not very good.
Third, ANT showed a weaker efficacy; however, its total AE ranked the first among the relevant therapy, and as a result, it can be regarded as a milder treatment in the clinical appliance.
Fourth, anti-TNF-α showed weaker efficacy than anti-IL-17 or anti-IL12/23 accompanied with a stronger AE; as a result, it was not recommended in this NMA research. As revealed in the introduction part, interleukins stimulate T-cells to produce TNF causing psoriasis. These biological agents work on the stimulation interleukins, the producer T-cells, and the final production TNF, respectively. The selectivity of these therapies gave them totally different mechanism and excellent efficacy. However, infection, the major AE of the above-mentioned biological agents according to the NMA results and previous studies,88,89 was still a severe problem to be solved. Additionally, a number of relevant biological agents were still at the stage of laboratory research, requiring more clinical studies and appliances.
Finally, AM did not work well in both efficacy and AE outcomes, which made is the least satisfactory therapy.
In this NMA research, there also existed some limitations. First of all, most of included studies reported the latest biological agents comparing with PBO or traditional therapy AM. However, direct RCT studies between these different treatments were still required for the unchallengeable authority of clinical experimental data. Besides, this NMA did not evaluate the treatment of mild psoriasis and topical therapies indicated for patients whose affected area is less than 10% of the BSA.90,91 The majority of this research and relevant works focused on severe psoriasis, and little attention was paid to the topical therapies like vitamin D and emollient. Finally, in this NMA, we divided the drugs treating psoriasis into five classes and regarded each whole class as a therapy; the efficacy and safety performance of interclass drug was not revealed in this NMA.
In conclusion, the efficacy and safety of some therapies of psoriasis were evaluated comprehensively and quantitatively in this NMA; monoclonal antibody agents of IL 12/23 and IL 17 were two recommended agents according to the results, while anti-IL17 should be used in caution since it has severe side effects.
Supplemental Material
Table S1 -Supplemental material for Quantitative evaluation to efficacy and safety of therapies for psoriasis: A network meta-analysis
Supplemental material, Table S1 for Quantitative evaluation to efficacy and safety of therapies for psoriasis: A network meta-analysis by Jingjing Lv, Dongmei Zhou, Yan Wang, Jingxia Zhao, Zhaoxia Chen, Jinchao Zhang, Tingting Di, Jing Hu, Bo Li, Ping Li and Feng Huang in Molecular Pain
Footnotes
Author Contributions
Research conception and design: DZ, YW, and JZ. Data analysis and interpretation: ZC, JZ, and BL. Statistical analysis: TD and JH. Drafting of the manuscript: PL. Critical revision of the manuscript: JL. All authors approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Beijing Financial Research Institute Project: Clinical and Biological Studies of Eczema and Psoriasis (No.PXM2017_026273_000001).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.