
Abstract
Objectives
The aim of this network meta-analysis is to assess the effectiveness of therapeutic strategies for patients with radiculopathy, including physical, medical, surgical, and other therapies.
Methods
We electronically searched electronic databases including PubMed and Embase for randomized controlled trials. The response rate and visual analog scale of pain change were considered as primary outcomes. The outcomes were measured by odds ratio (OR) value and corresponding 95% credible intervals (CrIs) or standardized mean difference (MD) with 95% CrIs. Besides, surface under cumulative ranking curve (SUCRA) were performed to rank efficacy and safety of treatments on each end points.
Results
A total of 16 eligible studies with 1071 subjects were included in this analysis. Our results showed that corticosteroid was significantly more effective than control regarding the response rate (OR = 3.86, 95% CrI: 1.16, 12.55). Surgery had a better performance in pain change compared with control (MD = −1.92, 95% CrI: −3.58, −0.15). According to the SUCRA results, corticosteroid, collar, and physiotherapy ranked the highest concerning response rate (SUCRA = 0.656, 0.652, and 0.610, respectively). Surgery, traction, and corticosteroid were superior to others in pain change (SUCRA = 0.866, 0.748, and 0.589, respectively).
Conclusion
According to the network meta-analysis result, we recommended surgery as the optimal treatment for radiculopathy patients; traction and corticosteroids were also recommended for their beneficial interventions.
Introduction
Radiculopathy is a set of neuropathic conditions caused by compressed nerves in the spine at or near the level of the nerve root. 1 The location of radiculopathy occurrence depends on which nerve root is affected. 2 Common symptoms of radiculopathy include radicular pain, numbness, tingling, and weakness in the muscles. 3 Cervical and lumbar radiculopathy can be induced by factors such as disc herniation, bone spurs, trauma, osteoarthritis, inflammation, and tumor or diabetes in some rare cases.4,5 Important risk factors associated with the incidence of radiculopathy include aging, race and hereditary factors, poor posture, and spinal abnormalities. 6 Some studies have also shown that occupation is related to radiculopathy, for example, one study states that people involved in heavy labor, sports, or military service are more likely to develop radiculopathy than those who live a sedentary lifestyle. 7 The prevalence of lumbar radiculopathy was 3% to 5% 8 while cervical radiculopathy showed an incidence of 83.2 per 100,000 persons annually. 9
Lumbar and cervical radiculopathy can be diagnosed through physical examination, imaging, and electrodiagnostics.10,11 Most patients with radiculopathy respond well to non-surgical, conservative treatment such as medication (corticosteroids, non-steroidal anti-inflammatory, tricyclic antidepressants, analgesics, and muscle relaxants), physical therapy, chiropractic treatment, spinal manipulation, traction, and corticosteroid injections. 10 The injection of corticosteroids into various structures in and around the spine is a common procedure used to reduce inflammation and lower back pain; 12 75% to 90% of patients’ symptoms are improved after non-operative care. However, for patients with persistent pain or severe functional deficit, surgical options are necessary and more beneficial when the pathology has been clearly identified. 13 In clinical practice, several procedures are usually adopted by surgeons, such as anterior and posterior decompression, anterior cervical discectomy, laminectomy, and minotomy. 14
Despite various kinds of non-surgical and surgical therapies were widely used for patients with radiculopathy, the relative efficacy of each treatment option was still unclear. One of the main causes was the deficiency of multiple-arm comparisons in clinical trials. Although a few meta-analyses have been published, the results from different studies for the same comparators have demonstrated controversial and contradictory results. Therefore, there was no recognized conclusion that has been obtained with respect to efficacy of these treatments. Moreover, currently published studies mainly focus on pairwise comparisons. Thus, it was more difficult for clinical practitioners to comprehensively integrate all of the evidence regarding all therapies and make the ideal choice. Our group conducted the first network meta-analysis (NMA) that synthesized the data from eligible randomized controlled trials (RCTs) in order to overcome the abovementioned shortages. We intended to illustrate the effectiveness of different strategies in radiculopathy treatment and provide more comprehensive and authentic evidence for the selection of treatments.
Methods
Search strategy and literature selection criteria
Two independent reviewers conducted the literature selection by searching electronic databases (PubMed and Embase). They restricted the search standard to articles published in English. The key search term was “radiculopathy,” and other subordinate entry terms (such as “cervical radiculopathy” and “lumbosacral radicular syndrome”) as well as different treatment strategies (corticosteroid, collar, physiotherapy, traction, surgery, serotonin, non-steroidal anti-inflammatory drugs, chemonucleolysis, and pulsed radiofrequency) were also included in the search query. All search terms were searched with Boolean operators AND or OR. Conference proceedings, bibliographies of the identified articles, and registries of clinical trials were not considered during searching progress.
The inclusion criteria of RCTs were (1) RCTs evaluating the efficacy of two or more different treatment therapies for radiculopathy patients, (2) RCTs with post-therapy response rates or changes in pain score as the outcome measurements, and (3) patients diagnosed with radiculopathy. (1) Studies that do not have relevant outcomes and (2) conferences or unpublished studies were excluded. The eligibility of papers retrieved was checked by two experienced reviewers independently. Any disagreements between the two reviewers would reach unanimity through consultation. If certain disagreements still remained, a third reviewer would be asked to intervene.
Data extraction
The characteristics and data were extracted from all 16 included studies. The following contents were considered in data extraction: (1) baseline characteristics of each study, including author, published year, blind condition, and study size; (2) basic patient information, including age and gender; (3) interventions in study and control groups; and (4) outcome data including the binary variable response rate and continuous variable pain score change.
Statistical analysis
Meta-analysis has been utilized to pool data from clinical trials and calculate estimates of drug efficacy. 15 Yet medical professionals may face more than one option when making decisions and pairwise comparisons might not be enough to figure out which treatment is more effective. Hence, NMA would be a wise choice when related regimens have not been compared directly. By combining direct and indirect evidence in clinical trials, NMA could execute evidence synthesis. 16
Two outcomes, response rate and pain score change, were considered to be equally vital in the systematic data analysis. Response rate was evaluated using odds ratio (OR) with 95% confidence intervals (CIs) in direct pairwise comparisons, which were generated using random-effects model. Further standardization of pain scores was conducted before data processing to explain variations in the evaluation scales accepted by individual studies. After standardization, a standard mean difference was computed on the comparisons. Data analyses were processed using STATA 13.0 and R 3.2.3 software; 95% credible intervals of outcomes were calculated in NMA. Pairwise comparisons from NMA were further presented visually using forest plots. The consistency between direct and indirect comparisons was evaluated using node-splitting results and heat plots (blue color represents higher inconsistency). In this case, p value < 0.05 was considered as a significant inconsistency. Furthermore, surface under cumulative ranking curve (SUCRA) was used to represent and evaluate the relative rank of each treatment under different outcomes.
Results
Selection and baseline information of included studies and network structure
The PRISMA flow diagram in Figure 1 illustrates the literature selection process. Two independent reviewers identified a total of 1703 eligible studies, which were selected for further screening. Of these, 161 studies were selected for abstract or full-text assessment, which ensured that irrelevant and insufficient articles were discarded. Finally, 16 studies were selected for data extraction and statistical analysis.17–32

PRISMA flow diagram.
Basic information from the 16 included studies was organized and displayed in Table 1. The studies were published between 1966 and 2014. The outcome of response rate was included in 8 of these studies, and the outcome of pain score was included in 12 of these studies. Therapies in all studies included corticosteroid, collar, physiotherapy, traction, surgery, serotonin, non-steroidal anti-inflammatory drugs, chemonucleolysis, pulsed radiofrequency, and control. All the treatments and their direct comparisons formed the networks as shown in Figure 2. Each node represented a different treatment, and the size of node corresponded to the number of patients studied with respect to the treatment represented. The lines between two nodes indicated the existence of direct evidence. Jadad scale for the 16 included studies is shown in Table S1.
Basic characteristics of included studies.
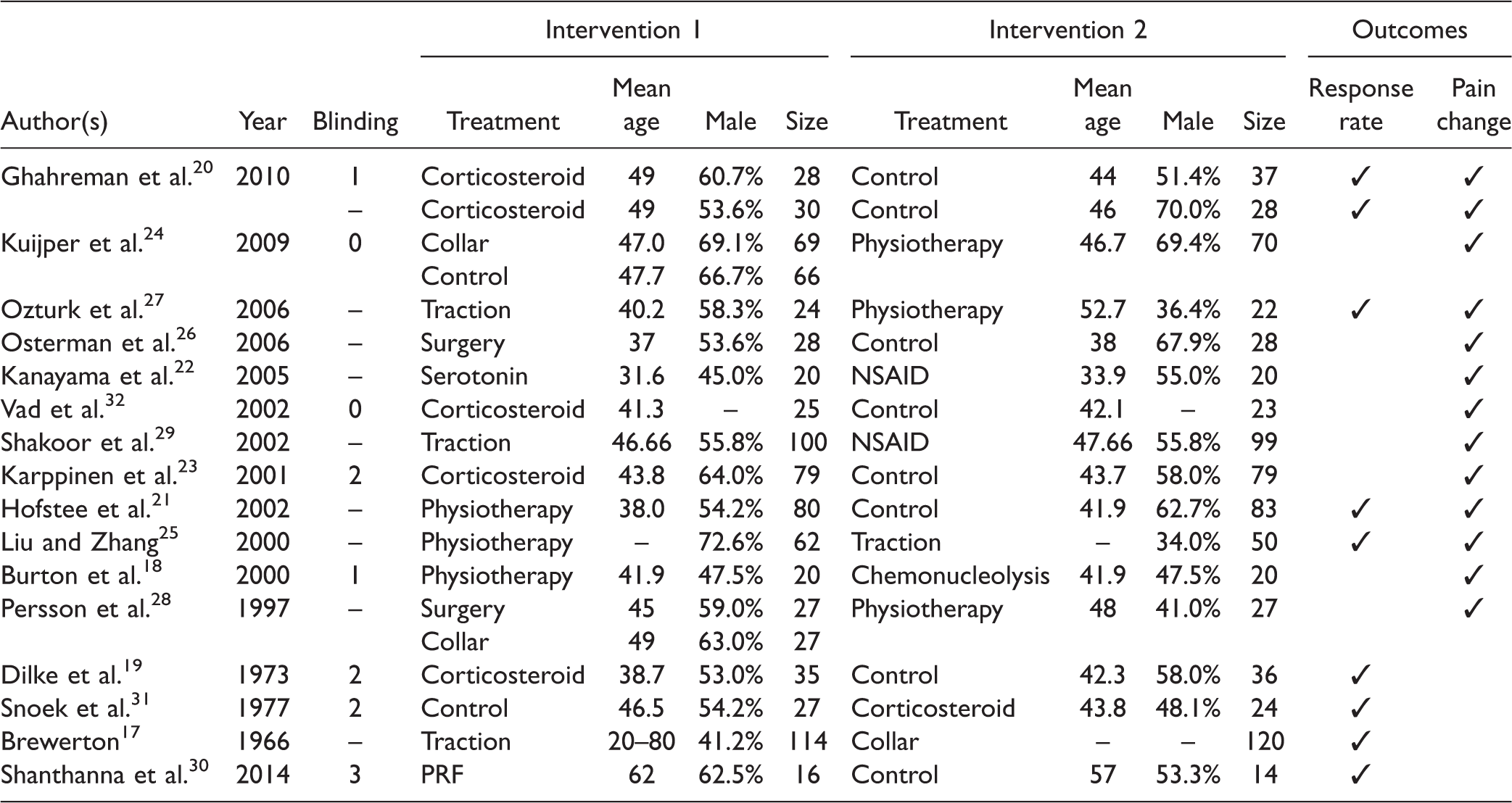
NSAID: non-steroidal anti-inflammatory drugs; PRF: pulsed radiofrequency.

Network of response rate and pain change. Lines represent direct comparisons between two interventions. The thicker the line is, the greater the number of existing direct comparisons between the two interventions. Numbers above dots show the total number of patients for each intervention.
Response rate and pain score change from NMA results
The network results in Table 2 showed that corticosteroid treatment had a significantly better response rate than control (OR = 3.86, 95% CrI: 1.16, 12.55). In addition, surgery displayed higher efficacy in pain change compared with control (MD = −1.92, 95% CrI: −3.58, −0.15). The results can be further proved by the forest plots as displayed in Figure 3.
Network meta-analysis results of response rate and pain change.

NSAID: non-steroidal anti-inflammatory drugs; PRF: pulsed radiofrequency.
Odds ratio (OR) or mean difference (MD) with 95% credible intervals (CrIs) were used to measure the relative efficacy. The network meta-analysis results are in the form of OR and 95% CrIs for response rate and MD and 95% CrIs for pain change. Boldfaced numbers indicate significant results (p < 0.05).

Forest plot of response rate and pain change. Odds ratio (OR) and 95% credible intervals (CrIs) for response rate and mean difference (MD) and 95% CrIs for pain change.
Ranking probability from SUCRA
SUCRA was evaluated in Table 3 for the purpose of rationally ranking the treatments with respect to each outcome. Concerning response rate, corticosteroid, collar, and physiotherapy held the top three rankings (SUCRA = 0.656, 0.652, and 0.610, respectively). Surgery, traction, and corticosteroid were superior to the others in pain change (SUCRA = 0.866, 0.748, and 0.589, respectively). Surgery has been recommended as the optimal treatment due to its high effectiveness in pain change. This is because that response rate and pain change were the most important primary outcomes of this study, and only 6 out of 10 treatments were available for response rate efficacy ranking, making this outcome lack comprehensiveness. Traction and corticosteroid can also be considered beneficial interventions regarding the two outcomes.
Surface under cumulative ranking curve of response rate and pain change.

NSAID: non-steroidal anti-inflammatory drugs; PRF: pulsed radiofrequency.
Consistency of direct and indirect comparisons for pain change
Node-splitting method (Table 4) and heat plot (Figure 4) were utilized to assess the inconsistency between direct and indirect comparisons. Based on the direct evidence results shown in Table 4, no significant outcomes were detected concerning pain change. It can also be seen that no inconsistency existed between direct and indirect evidence according to node-splitting results. No high levels of inconsistency were observed in the heat plot for pain change (node splitting and heat plot were only available for pain change). Funnel plot showed no significant publication bias (Figure S1).
Node-splitting results of pain change.

Mean difference with 95% credible intervals and p values were used to determine the difference between direct and indirect evidence.

Heat plot of pain change. The area of the gray squares displays the contribution of the direct estimate in design (shown in the column) to the network estimate in design (shown in the row). The colors are associated with the change in inconsistency between direct and indirect evidence (shown in the row) after detaching the effect (shown in the column). Cold colors indicate an increase in inconsistency, and warm colors indicate a decrease in inconsistency (the stronger the color is, the stronger the change is).
Discussion
We conducted the first NMA of the different treatment strategies for radiculopathy in order to better understand the relative efficacies of the available treatment options. A total of 16 RCTs were selected according to the standard literature selection criteria and included in this NMA. The response rate or pain score change data were extracted from each study and synthesized. Surgery along with traction and corticosteroids is highly recommended as the first-class treatments for radiculopathy based on the relative effects and SUCRA values. Surgery, in particular, has been highly recommended for being the highest rank treatment in pain score change. As for inconsistencies between indirect and direct evidence, no obvious inconsistencies were detected. Thus, it confirmed the acceptable quality of evidence included in this NMA.
Furthermore, our results showed consistency with other recent published systematic reviews, which strengthened the reliability of this NMA. In a prospective study, cervical radiculopathy patients who underwent surgical procedure exhibited a significant improvement in pain as compared to patients without surgery in the first year after diagnosis. 33 Another systematic review, which focused on the effectiveness of treatments for the lumbosacral radicular syndrome, demonstrated that surgery was more efficacious for patients with lumbosacral radicular syndrome regarding overall improvement after a one-year follow-up, compared to physiotherapy. 34 Corticosteroid injections showed early and moderate but unsustained improvements versus placebo in certain outcomes.35–37 Corticosteroids demonstrated effectiveness in reducing pain in a substantial proportion of patients with lumbar radicular pain. 38 The first report regarding the clinical use of steroid injection was published in 1953; 39 since then, it has been increasingly utilized on the strong pathophysiologic basis that its local anti-inflammatory function can inhibit inflammation by eliminating the secretion of cytokines, thereby reducing pain. 36 Therefore, corticosteroid injections were considered as an efficient and safe choice. Complications resulting from corticosteroid injection are rare. However, the method involving injection into the patients’ foramen is still worthy of optimization with regard to the detection of arterial injuries. 37
Although our study showed consistencies with other recently published analyses, contradictory results can also be observed according to other associated MAs. In an MA carried out by Nikolaidis et al., 14 it was concluded that the trials included in the analysis did not provide reliable evidence of surgery effectiveness on cervical spondylotic radiculopathy or myelopathy. They also stated that low-quality evidence was used to demonstrate that surgery might provide pain relief faster than physiotherapy or hard collar immobilization in patients with cervical radiculopathy, but little or no difference was shown in the long term. With respect to traction, one MA pointed out that traction was no more effective than placebo and collar. However, it should be noted that the study admitted that the evidence was of very low quality. 40 This inconsistency with our findings may be due to risks of bias and patient background variations. As the first NMA study to evaluate the efficacy of different treatments for radiculopathy, the conclusion of our study is clear and is supported by reproducible eligibility criteria. However, admittedly, a few limitations still exist. First, the optimal treatments for three kinds of radiculopathy might be different while in our study we put all the relevant studies together due to the lack of correlated researches. Second, when it came to SUCRA rankings of response rate, only 6 out of the 10 treatment groups could be assessed, making the evaluation process lack comprehensiveness. Furthermore, the different administrative approaches and doses of specific treatments were not considered as variables in this analysis. The different approaches in steroid injection, surgery, traction, or different combination and dosage of drugs in medication therapies would also have impacts on efficacy rankings. For instance, among steroid injection, facet injection has been suggested to be more effective and safer than transforaminal injection. 41 The combination of bupivacaine and betamethasone has also been shown to achieve better response rates than using bupivacaine alone. 42 Autotraction seems to perform better with regard to traction pain relief compared to conventional passive traction methods. 43
Besides, several limitations still exist in our NMA although we conducted it as meticulously as possible. First, the sample sizes of included studies were not very satisfying, which is also due to the essential characteristics of NMA. Second, a lack of sufficient data caused the absence of some variables in our analysis, such as administrative methods and dosages of drugs aforementioned. More RCTs with appropriate sample sizes should be conducted in future studies in order to better understand and compare efficacies of the regimens of radiculopathy. Third, various types of treatments used in control groups such as needle placement, physical therapy, and “wait and see” might weaken the credibility of the comparisons among different trials.
In summary, according to this NMA, surgery is recommended as the optimal treatment while traction and corticosteroid can also be considered good interventions. However, the choice of treatment should be based on the clinical situation. Moreover, related RCTs with long-term follow-up data and other outcome measurements such as side effects were needed to further analyze all the treatments.
Footnotes
Author Contributions
Research conception and design: DS; Data collection and screening: XZ and ZZ; Drafting of the manuscript: XZ, JW, and JL; Critical revision of the manuscript: YS and DS; Approval of final manuscript: All authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.