
Abstract
Dysmenorrhea (period pain) affects over 40% of women and is a leading cause of missed school and workdays. However, the molecular mechanisms underlying this pain are not fully understood. We conducted a systematic review (Prospero registration: CRD42024535081) to identify and evaluate the biomolecules in menstrual effluent that may contribute to dysmenorrhea and assess how non-hormonal medications (e.g. NSAIDs) impact these biomarkers. Fifteen studies involving two hundred twenty-three participants met the inclusion criteria. We used the Newcastle-Ottawa Scale (for observational studies) and the Cochrane RoB2 tool (for randomized controlled trials) to evaluate the risk of bias and the quality of studies. Eight studies consistently reported elevated prostaglandin levels in the menstrual effluent of women with dysmenorrhea, though sample sizes were generally small, and methodological issues were noted. Seven studies demonstrated that NSAIDs reduce prostaglandin concentrations; however, these trials utilized multiple-day dosing protocols instead of single-dose regimens, leaving questions about acute treatment effects. Two studies highlighted alternative molecular targets, such as 12-HETE and platelet-activating factor (PAF), that may also play key roles in menstrual pain. Overall, elevated prostaglandins are a recurring finding, but the limited scope and design of existing studies indicate a need for larger, methodologically rigorous investigations. Nevertheless, the few studies that identified molecules other than prostaglandins suggest there are viable druggable targets for clinical trials to reduce menstrual pain.

Keywords
Introduction
Dysmenorrhea or painful menstruation is the leading cause of school or work absenteeism, diminished physical activity, and reduced quality of life in reproductive-age women.1–3 Primary dysmenorrhea is defined as having no identifiable pelvic pathology, although it is resistant to conventional treatment in 15%–20% of women.4,5 The specific molecules released during menstruation that trigger uterine pain remain imprecisely known despite the ready availability of menstrual effluent for scientific investigation.
Historically, early researchers identified a so-called “menotoxin” in menstrual effluent that elicited phytotoxicity and neural excitability, 6 which was later revealed to be prostaglandin. 7 This discovery led to decades of research aimed at understanding how elevated prostaglandin levels cause increased myometrial contractility, resulting in menstrual pain. 7 Subsequent reviews have reinforced prostaglandins as key mediators of dysmenorrhea, yet many women do not achieve adequate pain relief with nonsteroidal anti-inflammatory drugs (NSAIDs), which primarily target prostaglandin synthesis.4,8 This discrepancy highlights the potential role of other biomolecules in dysmenorrhea pathophysiology. Indeed, recent studies have demonstrated that additional molecules (e.g. platelet activating factor, epoxy eicosanoids) can be present in even higher concentrations among women with dysmenorrhea, suggesting that prostaglandins alone may not fully account for the pain experienced.9–11 Therefore, re-evaluating the evidence concerning both prostaglandins and other potential molecules is essential for more fully elucidating the root causes of dysmenorrhea.
Since then, many researchers have attributed dysmenorrhea’s cause almost entirely to increased myometrial activity due to elevated prostaglandin levels. Given that many women experience incomplete pain relief or no pain relief with drugs that target prostaglandin synthesis (NSAIDs), it is essential to reanalyze the prior evidence of altered prostaglandin levels or other candidate molecules to fully identify the root causes of menstrual pain. We identified a few studies that examined molecules other than prostaglandins to be present in even higher concentrations of menstrual effluent among women with dysmenorrhea.9,11 This led us to consider that other important molecules may be responsible for menstrual pain.
Therefore, we conducted a systematic review to address two main research questions: 1. Among reproductive-age women, how do the molecular profiles in menstrual effluent differ between those with dysmenorrhea and those without? (Primary outcome: presence and/or concentration of specific biomolecules) 2. Among women with dysmenorrhea, how do prostaglandin levels in menstrual effluent compare between those treated with NSAIDs and those treated with placebo, non-NSAIDs, or no treatment? By investigating these questions, we aim to clarify whether altered prostaglandin levels alone drive dysmenorrhea or whether other molecular factors also play critical roles, thereby helping to identify more effective targets for therapeutic intervention.
Methods
Eligibility criteria, information sources, search strategy
We conducted this review following the Cochrane Handbook, PRISMA guidelines and prospectively registered our protocol, available at PROSPERO (york.ac.uk; CRD42024535081).
To identify relevant literature on molecular biomarkers in menstrual effluent linked to menstrual pain, we searched PubMed, EMBASE, and Web of Science, and using the keywords “menstrual” in conjunction with either “pain” or “dysmenorrhea” and terms related to menstrual fluid collection methods (“menstrual fluid,” “effluent,” “tampon,” “pad,” or “cup”) since inception through March 2024. The specific query “menstrual” and (“pain” or “dysmenorrhea”) and (“menstrual fluid” or “effluent” or “tampon” or “pad” or “cup”) identified 575 published citations. Studies were required to meet the following criteria to be eligible for subsequent data abstraction and analysis: (1) observational studies (case-control, cross-sectional) or (2) randomized control trials or cohort studies that consider menstrual pain or dysmenorrhea status as a relevant variable. Additionally, we reviewed the references cited in these papers to uncover any potentially overlooked studies or reviews.
Study selection
In our selection process, we excluded studies that: (1) focused away from eicosanoid-targeted therapies, such as those on the effects of hormonal contraceptives or herbal treatments for primary dysmenorrhea due to the ambiguity surrounding their specific impacts, (2) focused on secondary dysmenorrhea (endometriosis, fibroids) because of alternative mechanisms for pain in these conditions, (3) were published in languages other than English, and (4) were conference abstracts, which were reviewed but not included in the full qualitative review.
Data extraction
A coding manual was developed to extract information from each study. Variables such as publication information (author and publication year), study population (general or clinical), the study design (cross-sectional, case-control, randomized controlled trial, or cohort study) and sample size, method of menstrual pain severity assessment, how menstrual blood was collected (tampon, pad, or cup), method of effluent extraction, biomarker concentration, and analytical techniques. We also included the standard deviation of reported biomarker concentrations to provide a metric of the confidence in each measurement.
Quality and risk assessment
Two reviewers (GA, MS) independently assessed the quality of each study using the Newcastle-Ottawa Scale for observational studies 12 and the Cochrane RoB2 for randomized controlled trials. 13 A third reviewer (KH) was used to help judge discrepancies between the two independent reviewers.
The NOS scale awards a maximum of nine stars to each study: 4 stars for the adequate selection of cases and controls, 2 stars for comparability of cases and controls based on study design and analysis, and 3 stars for the proper ascertainment of the exposure in both the case and control groups. According to the guidelines, high-quality studies score a maximum of 9 stars and medium-quality studies score 7–8 stars. The Cochrane RoB2 assesses five critical criteria: random sequence generation, allocation concealment, blinding, incomplete data, and selective reporting. The quality of each trial was categorized as low/unclear/high risk of bias. Trials that met all criteria were categorized into low risk of bias, while trials with ≥2 high-risk scores were categorized as high risk of bias.
Data synthesis
A total of 575 studies were identified from the database search (Figure 1). We excluded 194 duplicates and 367 for a combination of reasons (e.g. Wrong publication type- conference abstract only, articles that lacked biomarkers, didn’t study dysmenorrhea, etc.). Additionally, an additional relevant article was found from reading introductions pertinent to the goals of this systematic review. Two reviewers independently examined the collected data to verify data accuracy. Cohen’s D was calculated for all identifiable molecules within the effluent that provided mean values with variance. In one of the studies, when variance was missing for one of the parameters, we assumed comparable variance in the second parameter. Although we computed Cohen’s d to help with interpretation, given the wide variety of analytical methods, creating a meta-analysis for a pooled analysis was not meaningful. The full data set, including papers identified and reasons for exclusion, are available on open science framework (DOI: 10.17605/OSF.IO/GJT8R).

PRISMA diagram for study selection.
Results
Study selection
After removing studies that did not discuss molecular biomarkers for menstrual pain, 15 studies were included in the review (Figure 1).
Study characteristics
Eleven studies were published between 1978 and 1995; the remaining three studies were published between 1995 and 2023. One published report captured outside of the search appeared to be a replicate publication of the same finding. 14 Half of the studies included were clinical trials (parallel, randomized clinical trials, and cross-over designs) undertaken to ascertain NSAIDs’ efficacy (prophylactic or therapeutic) in relieving dysmenorrhea pain. Studies investigating cross-sectional differences (Table 1) and effects of NSAIDs on biomarkers (Table 2) had small sample sizes (n ≤ 16/group). All of these studies characterized effluent pooled over multiple days. The drug studies all measured the effect of NSAIDs for multiple days over effluent pooled from multiple days (Table 2).
Studies with group differences in effluent content included in this review.

Summary of clinical studies that assessed the efficacy of NSAIDs in relieving menstrual pain.

The quality of the studies included in this review, as indicated by the NOS score, ranged from 1 to 8, and thus are categorized as either medium quality or poorer quality. The major limitations affecting quality are sample selection and size, comparability, and outcome assessment (Table 3).
Quality assessment of case-control studies included in this review on the Newcastle-Ottawa scale.

A study can be awarded a maximum of one * for each numbered item within the Selection and Outcome categories to indicate better quality assessment.
A maximum of ** can be given for Comparability to indicate better quality assessment.
The controlled randomized studies examining drug effects for risk of bias were evaluated using the Cochrane RoB2 tool. One study was excluded because it only contained one participant. 16 Most studies were deemed to have a low level of bias (Table 4).
Risk of bias assessment of each of the studies included in this review by Cochrane RoB2 tool.

Synthesis of results
Although an early study using separation methods and myometrial strip assays suggested that women with dysmenorrhea (n = 7 cases, unreported number of control subjects) had elevated levels of menstrual fluid prostaglandin, 15 quantitation was not performed until 1978. The subsequent seven published studies confirmed that participants with menstrual pain had higher concentrations of PGF2α (Cohen’s d = 0.5–2.3) and PGE2 (Cohen’s d = 0.9–3.7) in their menstrual effluent compared to pain-free controls (Table 5).9,11,14,16–21,23,25,27 Among these studies, the most comprehensive profiling of effluent was performed by Bieglmayer 9 in 12 participants that reported various intensities of menstrual pain associated with elevated concentrations of several eicosanoids, including thromboxanes, leukotrienes, and hydroxyeicosatetraenoic acids (HETEs). 12-HETE, a product of 12-lipoxygenase (LOX) activity, was the most abundant eicosanoid (synthesis rate > 1 µg/h) even in control participants. Nigam et al. 11 (n = 7 dysmenorrhea, n = 5 pain-free controls) reported that leukotriene (LT)C4/D4 and platelet-activation factor (PAF) were elevated in the menstrual effluent of women with menstrual pain. In sum, although several studies have measured prostaglandins in menstrual effluent, only a few have included other molecules, such as alternative eicosanoids that might contribute to menstrual pain.
Menstrual eicosanoids and their concentration in the studies included in this review.
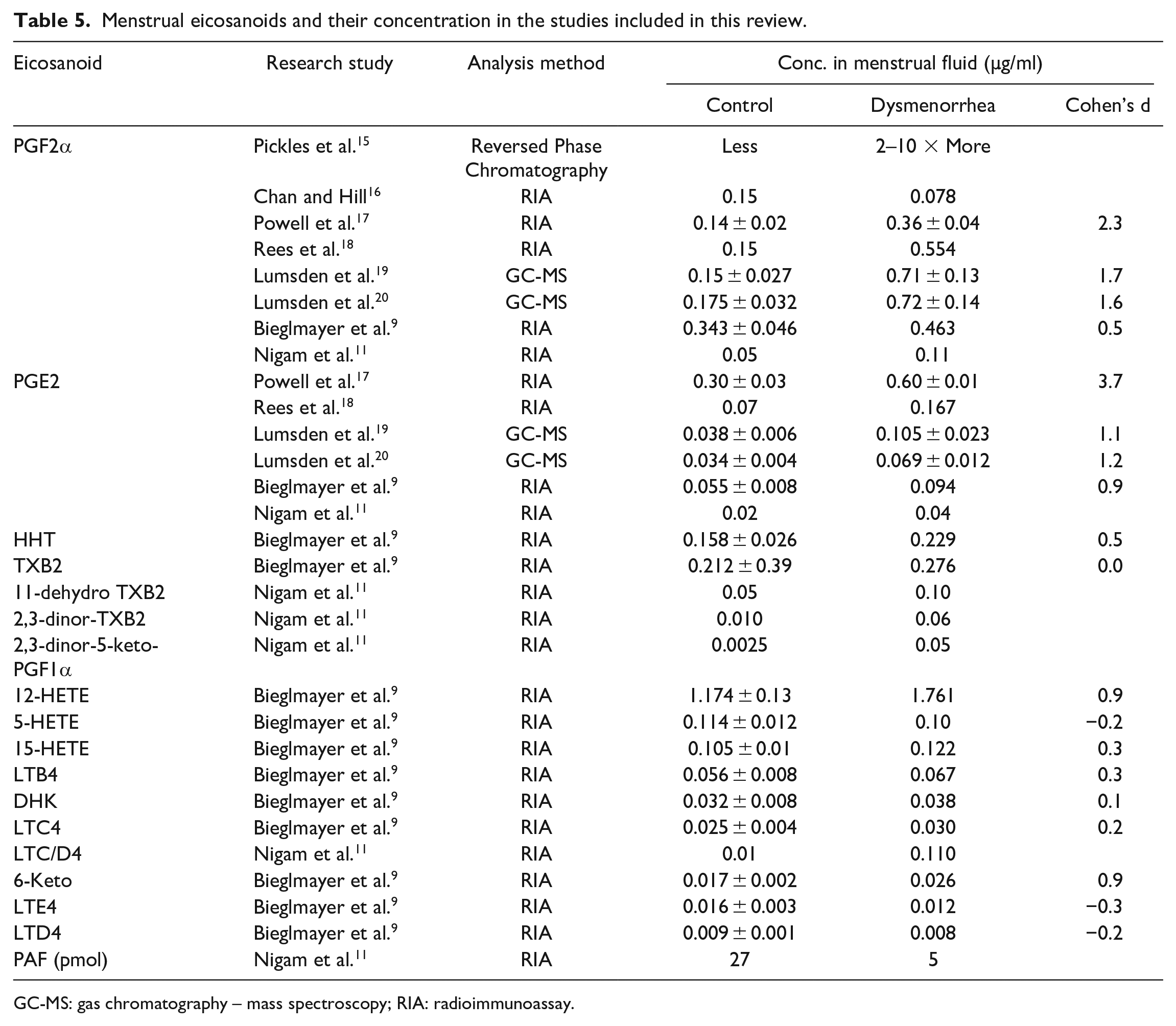
GC-MS: gas chromatography – mass spectroscopy; RIA: radioimmunoassay.
Effects of acetaminophen or NSAIDs on eicosanoid content in menstrual effluent
An overview of research designs in clinical trials employed to assess the efficacy of NSAIDs in relieving menstrual pain is summarized in Table 2. A quantitative synthesis of change in eicosanoid concentrations before and after NSAID treatment is presented in Table 6. We noted seven studies of NSAID use examining their impact on eicosanoid concentrations, all of which focused on PGF2α and a few that included additional eicosanoids. All the study designs involved repeated use of NSAIDs over multiple days (Table 2) and utilized effluent samples captured over this entire time period. These studies typically measured total PGF2α without accounting for potential differences in effluent volume. One study also included an acetaminophen arm. 26 Every study reported a significant decrease in prostaglandin concentrations (Cohen’s d 3.0–8.5) after NSAID or acetaminophen treatment.
Summary of the effect of NSAIDs on eicosanoid concentrations in menstrual effluent.

Discussion
This systematic review identifies that prior studies have linked excess prostaglandin to menstrual pain but that those studies have numerous methodological limitations and minimally address alternative inflammatory pathways for dysmenorrhea. Studies evaluating prostaglandin levels generally looked at effluent over multiple days, making it impossible to establish whether acute elevations of prostaglandin cause menstrual pain. Furthermore, the included studies involved relatively small sample sizes and did not examine the magnitude of the relationship between prostaglandin concentration and pain severity. This omission represents an important limitation, as understanding the strength of such a correlation, the percentage of explained variance, would help clarify the extent to which elevated levels of specific molecules contribute to menstrual pain. Likewise, these studies do not address whether acute treatment with NSAIDs rapidly reduces effluent levels of prostaglandin, despite the fact that NSAIDs can acutely reduce menstrual pain. Notably, the few studies that explored other biomarkers for menstrual pain identified other candidates, such as 12-HETE and PAF. Together, these papers suggest that prostaglandins and other inflammatory molecules contribute to menstrual pain and could be targeted to treat it (Figure 2).

Proposed biochemical pathway of NSAID-responsive and NSAID-resistant menstrual pain.
Comparison of effluent dysmenorrhea biomarkers to other studies of systemic circulation or endometriosis
Parallel to these effluent studies, others have reported differences in systemic serum concentration of eicosanoids. Participants with dysmenorrhea were reported to have plasma concentrations of PGF2α 1.68–2.74-fold higher than those of pain-free controls.28–31 However, it is essential to note that the concentration of eicosanoids is 1–2 orders of magnitude higher in menstrual effluent than in circulating blood, suggesting that prostaglandin is more likely to play a causal role in the uterine cavity. Notably, the highest concentration of biomarkers reported in effluent, particularly among women with dysmenorrhea, is 12-HETE. 9 12-HETE has been shown to potentiate TRPV receptors, 32 and TRPV receptors have been implicated in menstrual pain and endometriosis.33,34 Intriguingly, prior studies have not looked at prostaglandin concentrations among effluent in women with secondary dysmenorrhea such as endometriosis, adenomyosis, or even fibroids. Thus, given the centrality of prostaglandin to its hypothesized role in menstrual pain, it is surprising that there has not been more work to confirm its role in these related conditions.
One other such alternative molecule, PAF, was identified to be a higher levels in menstrual effluent in dysmenorrhea participants, 11 we have previously shown to affect uterine contractility, perfusion and pain in a mouse model. 35 Given there are PAF receptors antagonists have been used safely in studies such as rupatadine 36 BN52021, 37 and Lexipafant, 38 future clinical trials should investigate these drugs on menstrual pain. Also, considering a role for HETE-12 and other related molecules, a combination therapy targeting COX-2, LOX, and cytochrome-P450 pathways may be more effective than COX-2 inhibition alone. Thus, future clinical trials for dysmenorrhea should consider using Zileuton (a 5-LOX inhibitor) and GSK2256294A (a soluble epoxide hydrolase). 39
Nevertheless, most of the sample sizes included in this review were small, and it was assumed that the samples had normal distributions of biomarkers. Prior studies did not report the actual distribution, yet they noted considerable variability. For example, Chan et al. 21 noted that 28% of women who reported severe pelvic discomfort had menstrual effluent prostaglandin concentrations within or below the range of non-dysmenorrheic women. Notably, articles mostly focused on eicosanoids and neglected other proteins and mRNA transcripts in effluent. Future studies of menstrual pain desperately need larger sample sizes with unbiased analytical, statistical, and molecular methods to better identify mechanisms that contribute to menstrual pain.
Strengths and limitations
A key strength of this review is that it provides a comprehensive starting list of all known targets for investigating the mechanisms underlying menstrual pain. Because several studies have also looked at the effect of NSAIDs, it also quantifies their impact on prostaglandin synthesis. Limitations of this review include its exclusion of articles written in languages other than English and articles that look at biomarkers in things outside of the menstrual effluent (i.e. the systemic circulation). However, our exclusive focus on menstrual effluent will be useful for other scientists wishing to discover important targets within the menstrual effluent but may not have easy access to this older literature.
Conclusions
Despite decades of research, the etiology of primary dysmenorrhea is not precisely understood. This review found that while prior studies support a role for PGF2α, other molecules such as PAF and 12-HETE have been reported at higher concentrations in the effluent of participants with menstrual pain, and they may thus play a causal role. Analyzing the impact of drugs such as PAF receptor antagonists 40 or drugs that impact 12-HETE by inhibiting lipoxygenase activity 41 seems like an obvious future study. Ideally, studies should also include participants known to have minimal pain reduction after NSAID use. Because all prior studies looked at the effects of over 6–10 doses of NSAIDs on effluent, the acute effects of NSAIDs remain unknown. However, many women take NSAIDs acutely (often just a single dose) for menstrual pain and experience variable levels of relief. Therefore, it is valuable to establish whether NSAIDs effects on pain can be mediated by temporarily reducing local prostaglandin levels.
Given these findings, future dysmenorrhea studies should explore preclinical and clinical trials that follow levels of multiple molecular contributors to pain, which may yield better phenotyping of primary dysmenorrhea. Because individual response to analgesics may vary and multiple molecules may be involved, it may also be prudent for clinicians dealing with refractory dysmenorrhea to investigate combination anti-inflammatory therapies.
Footnotes
Acknowledgements
The authors thank Dr. G.F. Gebhart for help with advice and editorial assistance. During the preparation of this work the KMH used Grammarly to proofread the manuscript. After using this tool/service, the author reviewed and edited the content as needed and takes full responsibility for the content of the publication.
Abbreviations
COX: cyclooxygenase; NSAIDs: non-steroid anti-inflammatory drugs; PGF2α: prostaglandin F2 α alpha; PGE2: prostaglandin E2; HHT: hydroxyheptadecatrienoic acid; TXB2: thromboxane B2; 11-dehydroTXB2: 11-dehydro thromboxane; 2,3-dinor-TXB2: 2,3-dinor thromboxane B2; 2,3-dinor 5-keto PGF1α: 2,3-dinor-6-keto prostaglandin F1alpha; 12-HETE: 12-hydroxyeicosatetraenoic acid; 5-HETE: 5-hydroxyeicosatetraenoic acid; 15-HETE: 15-hydroxyeicosatetranoic acid; LTB4: leukotriene B4; DHK: 13,14-dihydro 15-keto-prostaglandin F2 alpha; LTC4: leukotriene C4; LTC/D4: leukotriene C/D4; 6-Keto: 6-keto-prostaglandin F1 alpha; LTE4: leukotriene E4; LTD4: leukotriene D4; PAF: platelet activating factor.
Author contributions
Conceptualization: KMH, MS, GA, CNK, MSO, FFT. Data curation: MS, GA, CNK, MSO. Methodology: KMH, GA, CNK. Funding: KMH, FFT. Interpretation: KMH, CNK, MSO, FFT. Writing – original draft: GA, CNK. Review and editing: KMH, MS, GA, CNK, MSO, FFT.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Tu reports stock options from Maipl Therapeutics and royalties from Wolters Kluwer. The remaining authors report no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Eunice Kennedy Shriver National Institute of Child Health and Human Development HD098193 to KMH and R01HD096332 to Dr. Tu.