
Abstract
The COVID-19 pandemic has disrupted the lives of people with intellectual disabilities in many ways, impacting their health and wellbeing. Early in the pandemic, the research team delivered a six-week virtual group-based program to help Canadian adults with intellectual disabilities cope and better manage their mental health. The study's objective was to explore ongoing concerns among individuals with intellectual disabilities following their participation in this education and support program. Thematic analysis was used to analyze participant feedback provided eight weeks after course completion. Twenty-four participants were interviewed in January 2021 and May 2021 across two cycles of the course. Three themes emerged: 1) employment and financial challenges; 2) navigating changes and ongoing restrictions; and 3) vaccine anticipation and experience. These findings suggest that despite benefiting from the program, participants continued to experience pandemic-related challenges in 2021, emphasising the need to continually engage people with intellectual disabilities.
Introduction
The COVID-19 pandemic has had a significant impact on people’s daily lives, affecting many of the programs and services they enjoyed and relied on. Early on in the pandemic, many activities and services were cancelled or moved online, including education (Gallagher- Mackay et al., 2021), health care (Canadian Institute for Health Information, 2022), work (Cotofan et al., 2021), and social events (Long et al., 2022). While the disruptions due to the pandemic were wide-reaching, the extent of their impact varied among individuals.
The disruptions and challenges associated with the COVID-19 pandemic have been particularly problematic for people with intellectual and developmental disabilities, impacting many aspects of their health and wellbeing. During the acute phase of the pandemic, the disruptions were extensive, including isolation from family and friends, loss of daily routines and activities, and increased stress and frustration (Schormans et al., 2021; Lake et al., 2022). Additionally, contracting COVID-19 put them at greater risk of complications and death (Lunsky et al., 2022a) as well as short and long-term health and mental health problems (Gleason et al., 2021), particularly during the period before vaccines became widely available.
In Canada, this group has experienced various inequities throughout the pandemic, including barriers to vaccine access (Rotenberg et al., 2021a), timely health care (Durbin et al., 2022), and basic financial support (Majnemer et al., 2021). A large proportion of Canadians with disabilities have long faced financial difficulties, living below the national poverty line for years (Wall, 2017) and being forced to rely on fragile caregiver support systems (Anderson et al., 2022; Pinto et al., 2022). Furthermore, the mental health implications of the pandemic have been serious, with an alarming number of people with intellectual and developmental disabilities reporting heightened anxiety, stress, depression, and isolation (Pettinicchio et al., 2021; Majnemer et al., 2021; Lunsky et al., 2022b).
In early 2020, at the height of the pandemic, most countries halted services for this group in the same sudden and extreme manner. However, the process of reinstating these services and supports varied. In Canada, incremental steps were taken to gradually re-open services and supports for this group throughout the summer and fall of 2020. However, due to subsequent COVID waves, a lockdown was later reimposed. Despite efforts by advocacy groups to highlight the increased vulnerability of people with intellectual and developmental disabilities, Canada’s vaccine prioritisation strategy was primarily age-based, leaving them unvaccinated until the spring of 2021.
Much of the research concerning the health and wellbeing of people with intellectual disabilities during the pandemic has focused on their early experiences. Researchers in the UK have followed participants throughout subsequent stages of the pandemic, and have shown that the needs of people with intellectual disabilities changed, with some issues improving and others remaining (Flynn et al., 2021; Hatton et al., 2023). Thus, to effectively address the challenges presented by the pandemic, it remains critical to conduct research involving people with lived experience and examine how their needs evolved across different jurisdictions as the pandemic progressed.
Intervention
As part of a larger initiative to develop a national virtual COVID education program for people with intellectual disabilities and those who support them, a six-week virtual group-based program was designed for adults with intellectual disabilities from across Canada. The program had two objectives: 1) to provide people with intellectual disabilities with the tools to help them cope during the pandemic, and 2) to provide a safe space for the community to talk about issues affecting their mental health and wellbeing. Over the six sessions, each 90 minutes long, participants learned about a variety of topics, taught jointly by other adults with intellectual disabilities and clinicians. Topics included healthcare communication, coping with stress and anxiety, and dealing with grief and loss. To evaluate the effectiveness of the program, participants completed questionnaires before and after taking the course to measure changes in their mental health. Overall, participants responded positively to the course and reported an increase in their self-efficacy to address their mental health needs (St. John et al., 2022). This intervention was delivered during a time of deteriorating pandemic circumstances. While mental health education and support were helpful, they could not fully address all of the challenges experienced at the time and therefore required additional inquiry.
This paper explores the pandemic-related experiences of adults with intellectual disabilities in 2021, eight weeks after completing the virtual group-based program. Our objective was to explore ongoing as well as emerging concerns among this group during the second year of the pandemic, following participation in a targeted education and support program designed to assist them in coping and managing their mental health and wellbeing.
Methods
This paper reports on a portion of the results from a broader study examining the impact of a six-week virtual mental health and wellbeing program. Participants were recruited from across Canada through various self-advocacy organisations for adults with intellectual disabilities (e.g., People First of Canada). To participate in the program, they needed to have access to the internet and a web camera. Participants were interviewed by a member of the research team prior to the course (pre), after course completion (post), and eight weeks later (follow-up). This paper examines participant qualitative responses from the follow-up data collection period. Additional details regarding course design, participant recruitment, and data collection are described elsewhere (St. John et al., 2022).
Participants
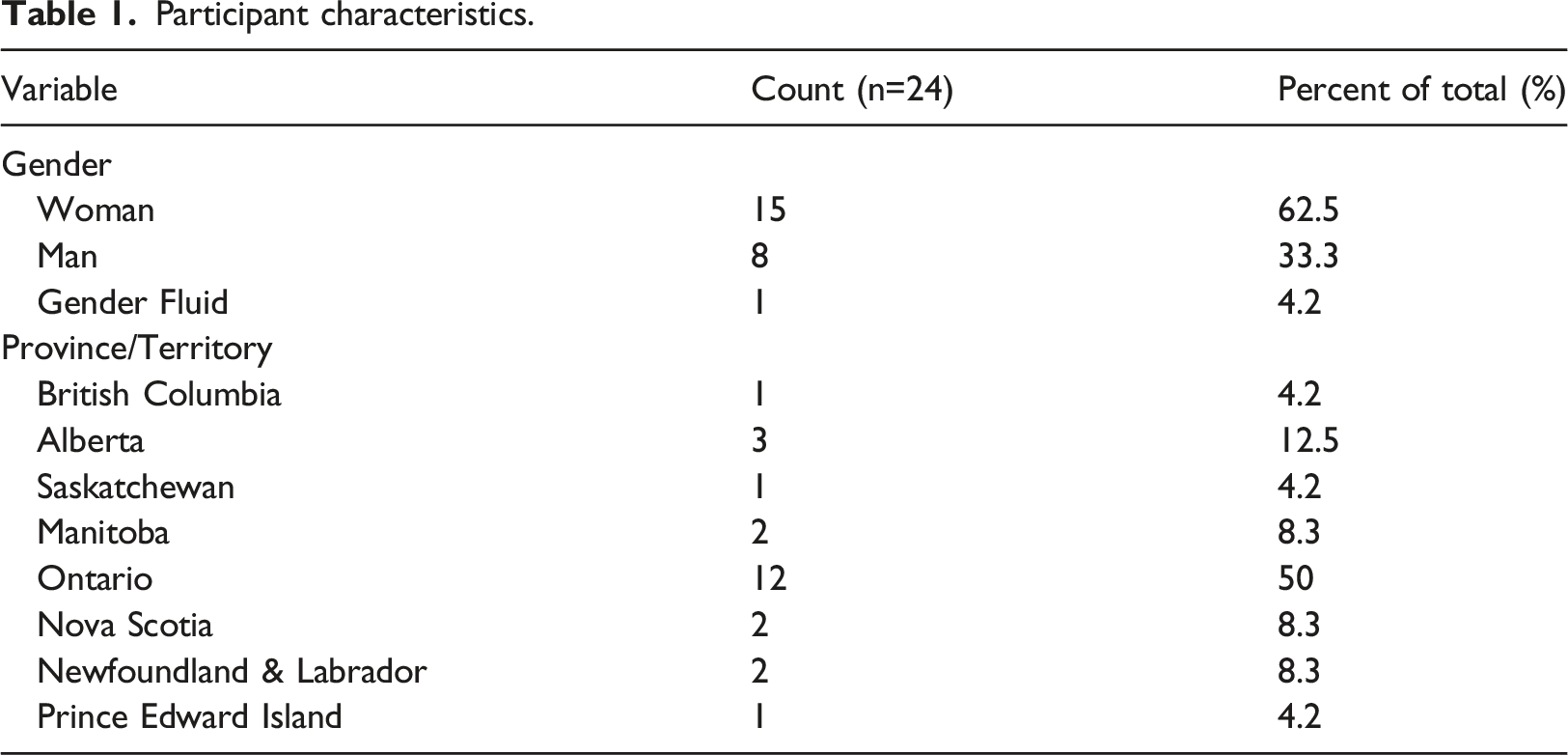
Participant characteristics.
Data collection process
An experienced qualitative researcher from the team completed virtual one-on-one interviews with course participants eight weeks following course completion. This interview was the final in a series of three interviews that consisted of a series of structured quantitative measures as well as a number of semi-structured open-ended questions to provide a more in-depth understanding of participants' experiences. These interviews coincided with the end of wave two (January 2021, cycle 1) and during wave three (May 2021, cycle 2) of the COVID-19 pandemic in Canada. Within this paper, we focus on the responses to two of the survey’s open-ended questions: “Please tell us about any issues or things that are difficult for you right now” and “Please tell us how COVID-19 restrictions where you live have affected you since you began the course”. The interviewer displayed the survey on a shared computer screen and read the questions aloud. Participants’ responses were transcribed verbatim into unrestricted text boxes with the participant looking on. The two survey questions served as prompts for discussion, with the interviewer asking follow-up questions for additional contextual details and clarification. This allowed for a more in-depth and nuanced exploration of participant experiences.
Data analysis
The analysis was conducted using a deductive and inductive approach to thematic analysis to summarise responses to the two questions of interest in this study. The deductive phase involved sorting the data into organisational categories based on the research questions, existing literature, and the expertise of the research team. In the subsequent inductive phase, we let codes emerge directly from the data, enabling us to develop themes beyond the initial categories.
Thematic analysis allowed us to explore common patterns across responses while also identifying nuances. What we considered codes were experiences or challenges during the time of the interviews. Despite us taking a more descriptive approach, we as researchers were not passive in summarising codes (Braun and Clarke, 2021). As such, we are telling our story of what participants have shared and acknowledge that we bring our own social, political, and ideological positioning into our approach.
The six-step analytic approach described by Braun and Clarke (2006) was followed. Author 1 and Author 2 independently familiarised themselves with the open-ended responses and met to discuss initial impressions. They then independently coded the data using NVivo 12 software (QSR International) and met to discuss the codes and develop initial themes. They met a final time after further reviewing the data to consolidate and define themes. Themes were developed by grouping similar codes. As the study questions focused on the impacts of the restrictions and challenges experienced during the data collection period, these ideas/topics were treated as organising categories/themes during the first round of coding. However, the specific themes emerged inductively from the data and were synthesised by Author 1 and Author 2 from what participants shared.
After completing the analysis, the team invited all participants from both cycles of the course to meet with them and hear about the results. Seven participants attended the virtual meeting and confirmed that the findings were consistent with their recollections.
Ethics approval
This research study was approved by the CAMH Research Ethics Board (REB#123-2020). All participants provided informed consent virtually via WebEx, a videoconferencing platform. An interviewer met with participants individually, during which the interviewer shared their screen, reviewed the consent form with participants, and obtained verbal consent prior to proceeding with the survey questions.
Results
Twenty-four participants from across Canada participated in follow-up interviews (Table 1), 12 participants from each cycle, out of 27 individuals who participated in the program evaluation. The average age of participants was 39.7 years (SD = 11.9), and half lived in Ontario (n=12), Canada’s most populous province. Most participants were women (n=15, 62.5%), eight participants were men (33.3%), and one participant identified as gender fluid (4.2%).
Themes
Three main themes were identified regarding the challenges experienced by participants after course completion: 1) navigating changes and ongoing restrictions; 2) employment and financial challenges; and 3) vaccine anticipation and experience. The interviews revealed many intersecting challenges that significantly impacted participants' mental health and wellbeing throughout the pandemic.
Theme 1: Navigating changes and ongoing restrictions
Participants identified four challenges related to the theme of navigating changes and ongoing restrictions: difficulties understanding evolving restrictions, the prolonged closure of in-person day programs, maintaining social connections in a virtual world, and attending virtual health appointments.
According to participants, communication from government and public health officials regarding COVID restrictions and their specific details were sometimes difficult to understand, particularly when there appeared to be no clear end in sight for some participants. The periodic recurrence of lockdowns also contributed to feelings of uncertainty and apprehension about permissible activities and required safety precautions. “They put more restrictions in December in [town] and said it would end in 2 weeks, but now they are not telling us when they will end. They have to do a better job of keeping us informed. There is so much information - what do you believe, what do you think? It is scary.” - Cycle 1 Participant 05 “It has been a long lockdown. I think we have a lockdown now. Isn't there a lockdown now?” - C2 P28
Furthermore, pandemic-related restrictions resulted in significant changes in regular programming and activities, with many transitioning to online delivery, pausing temporarily, or ceasing operations entirely. Participants shared that it was difficult to adjust to the abrupt changes to these structured activities, which they relied on to connect with other people with intellectual disabilities. “Everything has changed since COVID started. Even my activities have been cancelled. And everything is online, even my work.” - C1 P06 “Not being able to see friends or family has affected me. It doesn't make me feel happy. Not being able to go out…has been difficult. ... My routine has changed...there is no day program right now.” - C2 P16 “I don't like things being cancelled, camp meetings behind the church have been cancelled for 2 years. It is my favourite time of the year…makes me wonder if it will ever come back again.” - C2 P29
One participant pondered what the future post-COVID would look like and questioned whether pre-pandemic social norms would be a thing of the past, never to return. “How normal are we going to be with COVID-19? How long is it going to be until we feel comfortable? … When is it going to be that time that you will feel comfortable not wearing a mask? Even after getting a vaccine, will we feel comfortable? I have a feeling people will still wear a mask - I am not going to take that chance. So when am I going to feel comfortable? I keep thinking maybe a year from now, going back to normal, back to weddings, having a big party.” - C1 P11
Many participants found it difficult to adjust to online friendships without the ability to see friends in person, as well as navigating new norms around social gatherings. “The biggest thing since starting the course is not being able to see my friends.” - C1 P05 “I find staying home during lockdown is difficult. Not seeing the people that I want to see is difficult; the only way I see my parents is through WhatsApp; but not in person. And I talk to them on the telephone.” - C2 P16
Some were concerned about how they would adapt to social situations post-pandemic and acknowledged that it would take time to adjust. “The more I stay home, I feel like it will be harder to do things once they start up again. Your body may not be ready to do things when we are allowed to again. I am not doing anything - is my anxiety going to be worse? Will I be able to handle going out? I don’t know. I may need to get comfortable again slowly.” - C2 P20
Finally, participants discussed their frustrations with the changes to health care delivery necessitated by public health restrictions, which had shifted from in-person visits to virtual or phone appointments. While some participants indicated they were fine with virtual health care visits, others found the adjustment difficult. “Not being able to go out to appointments is difficult - I have to talk to my doctor over the phone. She is not seeing anyone in person.” - C2 P19 “Plus I have to do all my appointments online; it is not all bad.” - C2 P21
Theme 2: Employment and financial challenges
Participants identified two main challenges, either arising from COVID-related lockdowns or pre-existing conditions. The first challenge related to employment during the pandemic, given that many employers were either not hiring, eliminating positions, or reducing employees' work hours. For one participant, personal safety was also a consideration, opting not to return to their prior job and expressing fear of taking a new job due to COVID-related anxiety. “I can't find a decent job. ... But you can't even go try to apply because they are all closed.” - C1 P11 “The lockdown restrictions are difficult for me. I can only work 2 days instead of 3. They gave me a day off because of restrictions.” - C2 P29 “As for a job, I was working before COVID, and after, but then my boss asked me if I wanted to go back to my work, and I said no because I might get COVID. I worked at Tim Hortons. ... Mostly I am trying to find a new job soon, but I can’t really because of COVID.” - C2 P24
The second challenge reported by participants was the inadequacy of government-provided funding for their disability (i.e., Ontario Disability Support Program). This lack of adequate support made it difficult for them to meet their basic needs, which intensified as expenditures escalated during the pandemic. “Having enough money to pay for things is hard. I am on ODSP [Ontario Disability Support Program funding]... We don't get much money; it requires a lot of budgeting which is hard for me. Clothing, personal care, activities, etc. are all limited with the amount that we get.” - C2 P17 “A lot of my issues have nothing to do with COVID; for example disability money we get - they are threatening to take away the amount of money we get, the date we get paid. ... This makes COVID that much harder to deal with.” - C1 P07
The insufficient amount of government funding combined with unemployment left some course participants with limited finances for essential living expenditures such as food and transportation. “My phone died, we need new glasses and money has been tight. My wife’s are going to cost $400, but we only have $200. So we have to cut back on stuff this month… hopefully nothing else breaks. It will be tight with groceries.” - C1 P03
Others were able to find ways to save money, but they still acknowledged that it was harder to meet their needs now than it was before the pandemic. “I’ve been able to get Meals on Wheels. It is affordable, for $150 a month they bring me hot meals. I am finding ways to live independently. … I have Passport funding [a program in Ontario that gives funds to people with intellectual disabilities to purchase supports and services] for transportation so I can get to my appointments.” - C2 P20
Theme 3: Vaccine anticipation and experience
Participants identified three main challenges related to their experiences with the COVID-19 vaccine: their acceptance and/or hesitation in getting vaccinated; waiting for a vaccine appointment; and the actual experience of getting vaccinated. There was a notable difference in the vaccine experiences between the two program cycles as the COVID-19 vaccine was not widely available to cycle 1 participants when interviewed in January 2021. Participants in both cycles expressed generally positive feelings about the COVID-19 vaccines. Cycle 1 participants were hopeful and eagerly anticipating their turn to be vaccinated, while cycle 2 participants spoke about their experience of getting vaccinated and waiting for their second dose. Most participants across both cycles were fine with receiving the vaccine and did not express worries about the shot itself. “I want to get it because then I know I am protected. I can travel.” - C1 P01 “As long as vaccines make it easier for me to get out of the house, then I am fine with vaccines.” - C2 P21
However, some participants did express hesitation about receiving the vaccine, particularly concerns about potential side effects. “The vaccine is annoying because it is giving people side effects and people are still dying. They still don't know about the vaccine.” - C2 P19 “Maybe I am just a bit scared for the vaccine because I don’t know what is in there and whether I will have a reaction.” - C2 P22 “I do have concerns about side effects. I have not asked anybody about vaccines yet.” - C1 P09
Some participants shared that they looked to close friends or family for reassurance. “To me, I am not really worried about it because I have a friend who got it and he felt fine. He did research, and I know that if he is confident, then I am confident getting a vaccine.” - C1 P08
One participant was initially hesitant about receiving the vaccine, but after speaking with a trusted family member, they changed their mind and were more accepting. “At first I wasn’t sure about getting it because they were saying you might die. But my uncle is a pharmacist and he said that isn’t true, that is garbage. … I changed my mind and I will get the vaccine when I am able to get it. … My worker looked at me weird like I was crazy. I’m not sure what she thought.” - C1 P14
Because vaccines were not yet widely available during cycle 1 interviews, participants largely expressed uncertainty about when and where they would receive the COVID-19 vaccine. Some participants in cycle 2 were also unsure, albeit fewer than those in cycle 1. Part of their confusion centred around when the prioritisation of vaccine distribution would include them, leading some to become frustrated or find ways to become eligible. “I am waiting to get the vaccine to protect myself from getting COVID. I want to know where I can go to get the vaccine, I don’t know yet. My family doctor said I can’t get it yet. They said to go to Public Health, but I don’t know where they are.” - C1 P06 “I have not had my first vaccine shot. I am looking for human service jobs just so I can get the vaccine. You can’t tell I have a disability just by looking at my face. So you are not considered a vulnerable population. So I am being neglected by the system. The vaccine priority list does not include disabilities that you can not pick up by the way a person speaks or acts.” - C2 P18
During the cycle 2 interviews, conducted in May 2021, vaccines were readily available to the majority of Canadians, and many participants shared that they had received or were scheduled to receive their first dose. Participants talked about their experiences of booking and attending vaccine appointments. Many discussed having support from someone to make the process easier and less stressful. However, some participants did not have supports and experienced difficulties. “I had a lot of anxiety over getting the vaccine, but my roommate came with me to the clinic and she waited while I went in. I told them I was under the IDD category and they were good at explaining things to me. It was really fast. I had a lot of anxiety leading up to it but it was all in my head. I felt tired afterwards, but no other side effects.” - C2 P17 “I got my vaccine and I did not know where to go at first. I didn’t know it was in [city], the place where you get the vaccine. And then, I didn’t know how to fill out the forms for that. The process went well. I was nervous but then I calmed down.” - C2 P24 “I am getting vaccinated this Friday. My social worker made the appointment for me; she wanted to help me. She will bring me there and bring me home after. I am happy that I am going to get the vaccine, but just worried if I will have side effects or not. But I won’t be alone – my social worker will be there so I will be less stressed or worried.” - C2 P22
Discussion
This qualitative study described the experiences of people with intellectual disabilities during the second year of the pandemic, following participation in an educational program aimed at providing them with strategies to navigate COVID-19 and manage their mental health and wellbeing. Despite learning new information and acquiring coping skills, this group of adults continued to experience challenges related to ongoing restrictions, understanding complex and frequently changing public health information, dealing with financial and employment difficulties, and accessing the COVID-19 vaccine, all of which affected their mental health and wellbeing. Some of the concerns described in this study echo issues raised early on in the pandemic (Courtenay and Perera, 2020), and others were new, emphasising the importance of studying how experiences have changed for people with intellectual disabilities as the pandemic has continued and evolved.
Importantly, the study highlights the limitations of a brief, one-time educational mental health program in addressing all of the different types of challenges faced by adults with intellectual disabilities during and after the acute phase of the pandemic. While the program provided individuals with valuable mental health information, resources, and effective coping skills, which resulted in some positive changes related to mental health self-efficacy (St. John et al., 2022), it did not address ongoing systemic barriers that hinder their ability to interpret information, participate in meaningful activities with people important to them, afford basic living expenses, and address current or emerging health concerns. This emphasises the need to tailor supports based on both the individuals’ needs as well as the stage of the pandemic.
Pandemic restrictions brought about significant disruptions in the social lives of most participants in this Canadian study. For many, these restrictions had not yet eased in 2021, while others experienced a temporary easing in the summer and fall of 2020, only to be disrupted a second time. While several researchers have highlighted the impact of sudden losses at the start of the pandemic, it is also important to recognise the ongoing impact of chronic isolation, as well as the retraumatising nature of recurring disruptions for this vulnerable group. This included the continued closure of in-person day programs and recreational activities, with some shifting to virtual delivery. These programs were the main source of social connection for participants, and pandemic-related changes resulted in feelings of loneliness and longing for their return.
Whereas at the start of the pandemic, the shift to virtual communication was confusing and frustrating, by the second year, some individuals began to question whether pre-pandemic routines and social connections would ever return to normal. While some participants had adapted well to digitally-based communication methods by year two, others struggled to maintain meaningful connections and relationships. Research suggests that access to digital technologies, along with the necessary support for their use, can act as protective factors against the social isolation experienced during periods of lockdown (Caton et al., 2022; McCausland et al., 2021). However, these tools are not a panacea for addressing the social isolation and loneliness that participants continued to experience in the second year of the pandemic.
The constantly changing public health guidelines in Canada during the pandemic made it difficult for some individuals to keep up with new information. This highlights the importance of clear and accessible government communication (Basterfield, 2021; Meltzer, 2020; Taggart et al., 2022). Accessing COVID-related information continued to be problematic in the second year. Research shows that finding and using information in a digital age requires technological proficiency, which can be a challenge for some people with intellectual disabilities (Ramsten et al., 2020). While participants felt equipped to learn new information, the need to continuously process ever-changing information was confusing and increasingly frustrating for them. Thus, offering information in multiple formats (e.g. audiovisual, printed, Easy Read) and acknowledging the role that family and support staff play in delivering information are central to ensuring that adults with intellectual disabilities have access to accurate and trusted COVID-19 information (Chinn, 2022; Terras et al., 2021), including information about vaccines.
Participants discussed significant changes to how they participated in their health care appointments during the pandemic, with most happening over the phone or virtually. There were mixed experiences with this shift, with some indicating a preference for in-person visits while others stated that they managed well with virtual appointments. These results are similar to findings from recent studies (Selick et al., 2021; Selick et al., 2022).
Consistent with other studies conducted early in the pandemic (Amor et al., 2021; Nicholas et al., 2022), participants in our study flagged challenges around work and difficulty managing expenses given the insufficient financial support received from government disability programs. Several participants reported disruptions to paid employment during the pandemic, describing either a reduction in work hours, being laid off, or becoming unemployed, and then experiencing difficulty finding work as restrictions were lifted. Given their limited income, participants spoke about difficulties meeting their basic living expenses, a situation compounded by the new expenses brought about by the pandemic (e.g. technology hardware/software, grocery delivery, masks and hand sanitiser). These findings echo issues identified in studies earlier in the pandemic (Lake et al., 2021; Majnemer et al., 2021) as well as studies on finances and disability more generally (Friedman, 2022; Gignac et al., 2021). Notably, for some, this was also an issue prior to the pandemic, as existing government programs were insufficient for many participants who depended on the income from such programs. Some government programs allowed for pandemic-related costs to be covered by existing disability benefits, but they did not increase the allocated dollar amounts. The lack of financial support for this population is in stark contrast to the basic income benefits (Canada Emergency Response Benefit (CERB)) that the Canadian government distributed swiftly to people not receiving disability benefits who were unable to work during the pandemic. Our results suggest that our pandemic response must go beyond temporary or quick-fix interventions, and focus on the pre-existing social and economic inequalities faced by vulnerable populations such as those with intellectual disabilities. Accessible, sustainable, and long-term solutions are needed to address the mental health challenges resulting from the pandemic.
Participants in both program cycles expressed concerns about access to the COVID-19 vaccine, with experiences reflecting regional eligibility criteria at the time of their interviews. While cycle 1 participants were not eligible to be vaccinated at the time of their interviews, most cycle 2 participants had received or were scheduled to receive a vaccine. Nevertheless, many participants from both groups described the experience of learning about and accessing the vaccine as confusing and stressful, as described in other Canadian studies (Campanella et al., 2021; Sebring et al., 2022; Seth et al., 2023). Vaccine rollouts have been criticised for failing to prioritise people with disabilities, including people with intellectual and developmental disabilities (Rotenberg, Downer, and Cooper, 2021b; Shevzov- Zebrun and Caplan, 2022), given their increased risk for poorer outcomes, hospitalisations and death (Gleason et al., 2021; Lunsky et al., 2022a; Williamson et al., 2021).
In line with other studies (Hatton et al., 2021; Iadarola et al., 2022), participants were generally willing to get vaccinated. However, those without caregiver supports found it difficult to book appointments and attend vaccine clinics. There is a need to improve the vaccination process, from finding and booking vaccine appointments to making vaccine clinics more accessible for people with disabilities (Rotenberg et al., 2021a). A crucial step in promoting vaccination amongst this population is ensuring the availability of accessible information for people with intellectual disabilities as well as their caregivers and support staff, who are important facilitators of such information.
Limitations
Our study has some limitations. As participants reported on their experiences in response to open-ended questions asked in the survey, there might have been limitations in fully delving into their experiences (LaDonna et al., 2018). Additional concerns could have emerged if the team had asked about them explicitly. However, the qualitative information collected was robust and sufficient (LaDonna et al., 2021), yielding valuable insights into the research questions being investigated. An additional limitation is that the sample does not represent the experience of all people with intellectual disabilities as this group may have been more comfortable using technology, had experience using virtual meeting platforms, were more independent, could make more decisions for themselves, and may have been more motivated to learn how to support themselves during COVID-19 by participating in the course. This group does not represent people with more severe disabilities or those who were not provided the supports they needed to participate in the virtual course. However, our findings highlight that even for people who are given information and taught new coping skills, major concerns remain. The findings captured here are specific to experiences in Canada in early 2021. People from other jurisdictions, which rolled out vaccines differently, had smaller or larger waves at this time or had different public health restrictions, may report different experiences. Moreover, what was experienced then may not match what these same individuals are currently experiencing because concerns continue to evolve. We need to ask these individuals what has changed and what their concerns are now.
Conclusion
The findings from this study during the second year of the pandemic show the importance of evaluating how people with intellectual disabilities are faring at different stages of the pandemic and beyond. Even after benefiting from an intervention focused on building social connections and teaching key health information, people with intellectual disabilities who had some comfort with technology, awareness of health information, and the ability to self-advocate, continued to struggle in several ways. This study also provides key lessons on the importance of improving the accessibility of information about vaccines and other pandemic public health interventions.
Footnotes
Acknowledgement
The authors would like to thank the COVID-19 mental health course teaching team who helped to create and deliver this online program. They would also like to thank the participants for their time and contributions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Canadian Institutes of Health Research (Grant #MS2-1730090).