
Abstract
The current study examines how a virtual wellness intervention may improve health outcomes in adults with intellectual and developmental disabilities. Thirty-six adults with intellectual and developmental disabilities participated in the wellness intervention. Outcome measures related to satisfaction, mental health, wellbeing, health behaviours and overall health were completed at three time points (pre, post and follow-up). Participants reported high levels of satisfaction and had significant improvements in outcomes related to mental health and wellbeing. Changes in sleep, sedentary behaviour and overall health were not reported, though qualitative evidence suggests that some changes were implemented. The study provides evidence to support the use of virtual interventions to address health concerns in individuals with intellectual and developmental disabilities.
Introduction
Wellness refers to the integration of one’s physical, mental and social health (Stoewen, 2017). The concept of wellness is important for all individuals, but it is especially important for individuals who have complex and unique health needs such as individuals with intellectual and developmental disabilities (Taggart et al., 2018). Adults in this population experience a multitude of unique mental and physical health conditions that can greatly impact their health and wellbeing. Physically, they are more likely to develop Type 2 diabetes (Taggart et al., 2018), hypertension and cardiovascular disease (Sohler et al., 2009). Additionally, they are more likely to experience mental health conditions, such as anxiety and depression (Hsieh et al., 2020; Lunsky et al., 2006, 2022), as well as social isolation, loneliness and lack of social support (Emerson et al., 2021).
Unfortunately, interventional studies have often focused on single domains of wellness, disregarding the complex health challenges experienced by this population (Heller & Sorensen, 2013). Furthermore, there is limited evidence that unidimensional programs can affect long-term changes in health-related outcomes such as body composition or health behaviour (St John et al., 2020). Holistic programs, by contrast, generally go beyond individual components of wellbeing to include nutrition, exercise, education, and the integration of the circle of care, which have been associated with long-term behavioural changes (Guerra et al., 2019; Salse-Batán et al., 2022). Multi-dimensional programs are especially successful when they focus on social engagement while providing education and resources for participants (Heller & Sorensen, 2013; Stanish & Temple, 2012; Temple & Stanish, 2011).
One such program was a virtual multi-dimensional intervention intended to address mental health concerns in adults with intellectual disabilities because of the COVID-19 pandemic (St John et al., 2022). This web-based course included 27 adults with intellectual disabilities from across Canada. Results revealed high levels of engagement among participants, with the majority attending at least four out of the six sessions. Measurable increases in self-efficacy were reported but not wellbeing, although qualitative evidence on mental health improvements were provided (St. John et al., 2022).
This intervention was created during a time when interventions were rapidly shifting from in-person to online due to ongoing COVID-19 pandemic restrictions. As such, concerns arose that online modalities would not serve the needs of individuals with intellectual disabilities due to perceptions around digital literacy (Chadwick et al., 2022). For individuals with intellectual disabilities, poor digital literacy may mean they have trouble accessing online interventions independently, resulting in a lack of autonomy (Chadwick et al., 2022). However, research has shown that with proper design considerations, virtual interventions can be successfully implemented with this population (St. John et al., 2022). Additionally, virtual programs have the potential to reach a broader group of individuals, overcome transportation barriers, foster individual autonomy, and reduce social anxiety and isolation (Giummarra et al., 2022). Virtual technology offers numerous benefits when delivering interventions, including accessibility, convenience, and reach (Ebner & Gegenfurtner, 2019), however our overall understanding of its capabilities and utility for populations with intellectual and developmental disabilities remains limited (Tan et al., 2022).
While the study by St. John et al. (2022) highlighted the benefits of virtual mental health interventions for adults with intellectual disabilities during the pandemic, it also revealed ongoing and unmet physical health concerns, including reduced access to health care, access to vaccines, and an increase in sedentary behaviours. As such, there was an increased need to design interventions that approach health holistically, focusing on the mental, social and physical needs of individuals. Furthermore, while the previous study was focused exclusively on supporting the health of individuals with intellectual disabilities, it was postulated that a course of this nature could reach a broader population, including those with developmental disabilities without intellectual disabilities, such as Autistic adults.
As such, in the current study, our intention was to conceptually replicate the study by St. John and colleagues (2022), with expanded course content to address ongoing concerns related to physical health as well as mental health. Through conceptual replication, whereby the content and timing of the intervention have been modified (Hudson, 2023), we tested the utility of online courses beyond the height of the pandemic. Furthermore, we were also able to assess whether this type of course is appropriate for the broader intellectual and developmental disability population, including Autistic adults.
Methods
Design and participants
The current study followed the same procedures and sampling strategy as the original study by St. John et al. (2022). The study utilized a single arm, repeated measures within-subject study design. Data collection were completed through one-on-one interviews with a member of the research team (TV) and occurred in three phases: (1) pre course, (2) post course and, (3) eight week follow-up. The data collected were both quantitative (i.e. survey) and qualitative (i.e. open-text responses), to gain a more fulsome understanding of participant experiences. While the quantitative data allowed for direct comparison of change across the time points, the qualitative data captured the depth and complexity of the participants' experiences (Kroll et al., 2005).
Participants were recruited from across Canada through various provincial and national agencies. Interested participants would complete an online expression of interest form. Once completed, they would be contacted by a member of the research team (TV) to receive information about the course (i.e. start time) and schedule a time to complete their online consent form and one-on-one interview. The research team member who conducted the interviews was not involved in teaching the course. Furthermore, as a trained qualitative researcher, the interviewer employed strategies throughout to ensure that they remained impartial and objective so participants felt comfortable responding to questions as honestly as possible.
To be eligible for the study, participants had to: (1) be over the age of 18, (2) self-identify as having an intellectual and/or developmental disability (including autism), (3) have the capacity to provide informed consent, and (4) have internet access and/or support to access the internet. Unlike the original study, where program participants could elect to take part in the research evaluation (75% of participants opted to do so), in the current study, only individuals who consented to the research were accepted into the program to ensure a robust sample size for the evaluation.
Intervention description
The virtual course was delivered across two 6-week cycles, from May to June 2022 and from June to late July 2022. The course structure and topics remained the same across the two cycles, although minor modifications were made to ensure the materials remained relevant and appropriate for the time period.
Weekly course topics.

Similar to the previous course, two individuals with intellectual disabilities were members of the teaching team and co-led all six sessions. Each session lasted for 90 minutes and followed a consistent structure comprised of a number of components including an ice breaker; small or large group discussion; mindfulness activity led by a member of the team with an intellectual disability; didactic teaching co-led by clinician team members and team members with intellectual disabilities; and a physical activity break (new) led by a clinician team member with a background in adapted physical activity. After each session, an email summarizing the week’s learning and resources was sent to all participants.
Outcome measures
Participation and satisfaction
Participation was based on the number of sessions attended. The retention rate was determined by calculating the number of participants who attended at least four out of six sessions. To assess satisfaction, participants responded to ten items in the post-course survey using a three-point Likert scale (yes, somewhat, no).
Self-efficacy
Self-efficacy was measured using four questions related to mental health, health care, self-care and physical health (e.g. I am confident in how well I can prepare for health care and talk to my doctor during COVID), with participants providing a response along a 100-point visual analog scale (VAS) from 0 (not confident at all) to 100 (very confident). These questions and VAS were modified from a previous measure used by Thakur et al. (2021), with a new question about physical health added. This scale was previously found to have adequate internal consistency (St. John et al., 2022). For the current sample, the internal consistency was within acceptable ranges (Ω = 0.70).
Wellbeing
To assess wellbeing, the Warwick-Edinburgh Mental Wellbeing Scale - Intellectual Disability Version (Scior et al., 2023) was used. This modified version of the scale includes word and response options purposefully chosen for those with intellectual disability. Participants respond to 14 items using a four-point Likert scale (never, sometimes, often, always). This scale has been found to be a valid and reliable measure of wellbeing in individuals with intellectual disabilities (Scior et al., 2023).
Mental health and overall health (new)
To assess mental health, four questions were taken from the Coronavirus and People with Learning Disabilities Survey (COVID-LD; Flynn et al., 2021). Participants were asked to consider how often they had experienced loneliness, anxiety/worry, sadness/feeling down, anger/frustration in the last month. This was assessed on a four-point Likert scale (never, sometimes, often, always). Scores from this scale were summed and could range from four to 16. Though this scale has no defined cut-points, it can be assumed that a higher score indicates a greater degree of mental distress. Internal consistency for the current sample was within acceptable ranges with a McDonald’s omega of 0.73.
To assess overall health, participants were asked to rate their overall health on a four-point Likert scale (good, ok, not very good, don’t know; Flynn et al., 2021).
Sleep and sedentary behaviour (new)
Sleep and sedentary behaviour were measured using the Simple Physical Activity Questionnaire (Rosenbaum et al., 2020), a measure that was not used in the original study. This questionnaire was designed to measure physical activity and sedentary behaviour in individuals living with severe mental illness. The five-item questionnaire asks individuals about time spent sleeping, being sedentary, walking, engaging in physical activity and exercise, and completing leisure activities. While not previously validated for use with individuals with intellectual disabilities, the measure has been validated for individuals with mental disorders including depressive disorders, bipolar disorders, anxiety disorders and neurocognitive disorders (Rosenbaum et al., 2020). For this study, the focus was exclusively on sleep and sedentary time. A more comprehensive overview of findings from the Simple Physical Activity Questionnaire has been outlined by Koch et al. (Under Review).
To measure sedentary behaviour, participants were asked to subjectively rate their screen time using a ten-point Likert scale, “how much time do you spend using technology?”, where 1 was not much time and 10 was too much time.
Data analysis
Similar to the previous study, qualitative open-text comments were analysed using descriptive content analysis (Hsieh and Shannon, 2005). However, quantitative analysis was modified in order to better address the research objectives. Descriptive statistics were conducted using R Studio software (R Core Team, 2022) and Jamovi. Frequencies and percentages were calculated for all categorical variables while distribution measures mean, median, standard deviation and range were calculated for all continuous variables. To estimate whether time impacted change at the individual level, a series of mixed effects models were conducted for each variable of interest. For each model, time was a fixed effect while the participant was the random effect. To adjust for sample size, the Kenward-Roger method was used (Kenward & Roger, 1997). Finally, in cases where time did significantly impact the variable of interest, a post-hoc analysis was conducted to identify at which time point change occurred. In cases where single items were used to assess a construct (i.e. physical health), a Kruskal-Wallis test was conducted.
Results
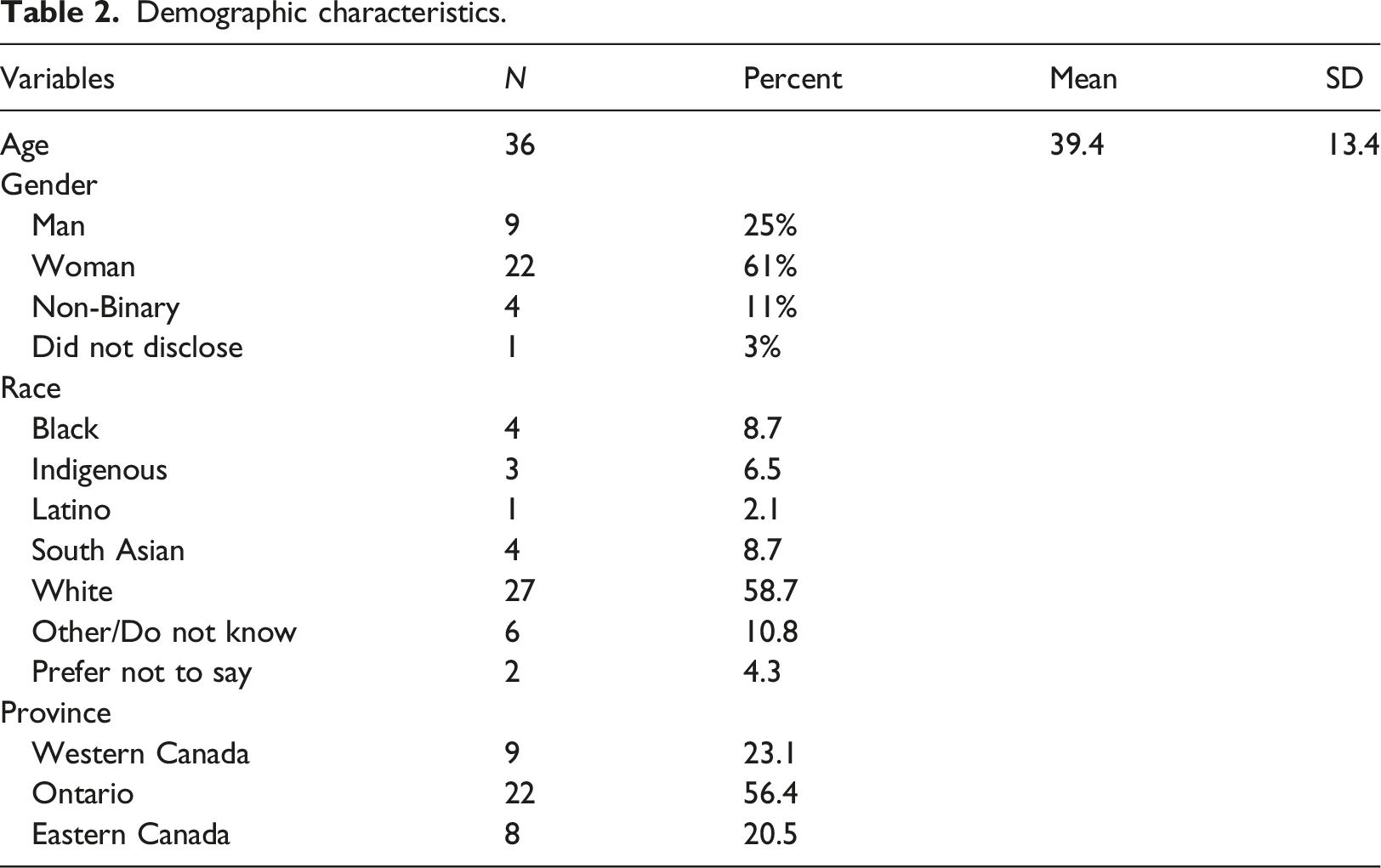
Demographic characteristics.
Participation
The median number of sessions attended was five out of six sessions, with no participants attending fewer than two sessions. Among the 36 participants, 29 attended at least four, 24 attended five and 12 attended all six sessions. Participants reported that sessions were easy to attend given the virtual nature of the course. Participant 104 stated, “Nothing made it [the course] hard to attend. It was on the computer, and it was in the comfort of my own home, so that made it easy to attend.” Furthermore, participants appreciated the weekly reminder emails from a member of the research team to support their attendance.
Work-related commitments were the most significant barrier to attendance. Participant 44 highlighted, “Work made it hard to attend… I had to work when the course was scheduled…” Several participants felt that an evening course, as opposed to a mid-afternoon course, would have made it easier to attend. Participant 5 stated, “Having the sessions later in the afternoon would have been helpful, I don’t get up until later [due to] sleep disturbances.…”. However, finding a time that suited all participants would have been challenging, given that the course was offered nationwide, spanning across six different time zones.
Satisfaction
Post-course satisfaction.
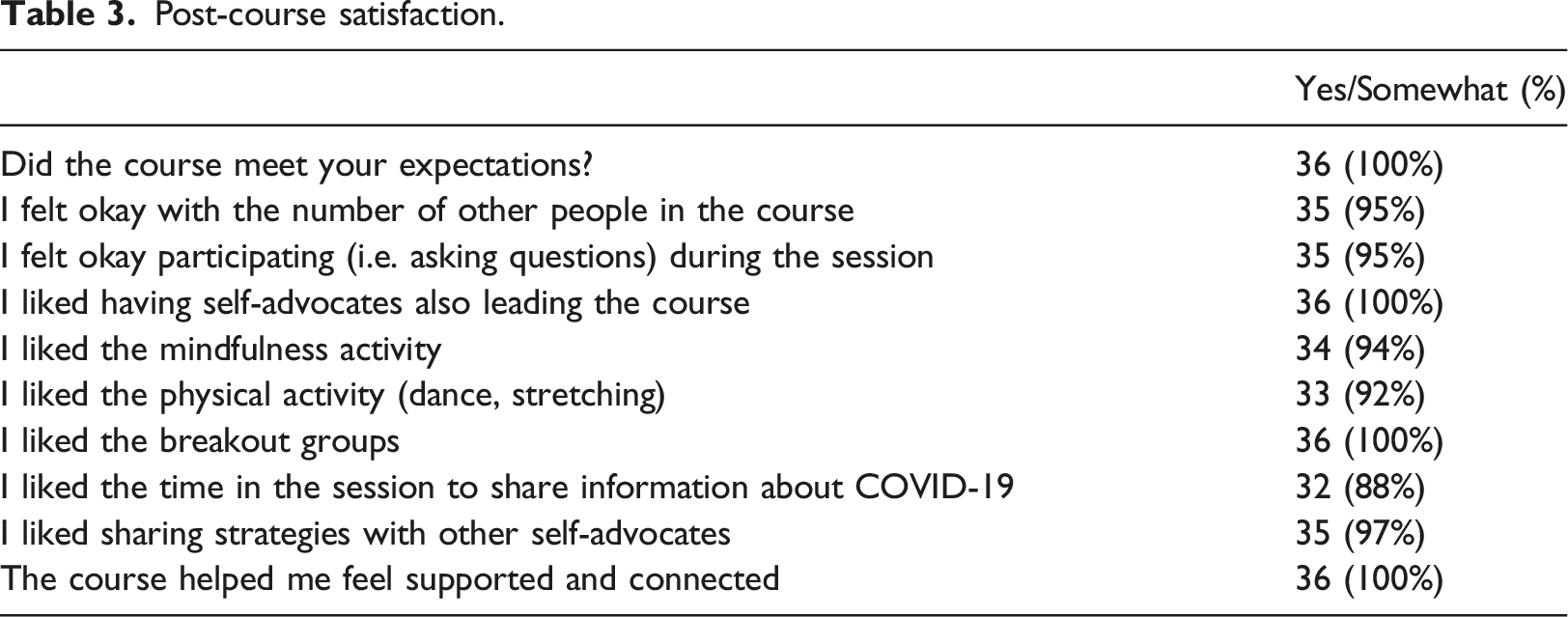
Finally, Participant 117 stated the importance of designing courses where participants have time to interact with one another and the teachers. “I expected the course to be a regimented program… I didn’t expect the free time to have breakout rooms and discuss other topics. The facilitators really cared.… Everybody was welcoming.”
Two activities that participants identified as being highlights of the course were the mindfulness activity (n = 34, 94% satisfied) and the physical activity breaks (n = 32, 92% satisfied). The mindfulness activity, led by a self-advocate and featuring positive affirmations, received overwhelming praise from many participants. For example, Participant 115 said, “[Self-advocate teacher] was amazing with the mindfulness. Holy Hannah. Being thankful for yourself, I am enough, you are worthy, you are loved…. The mindfulness was the best.”
The physical activity breaks were also well-received and enjoyed by participants. These breaks consisted of pre-recorded videos of line dances that could be performed in a seated or standing position. The dances, set to popular music, incorporated simple moves such as step claps or overhead reaches and were designed to be accessible to all participants, regardless of skill, activity level or disability status. Participant 111, who was legally blind stated, “The dance! The dance! I love [First Author]’s dance and the music.” Participant 117 said, “The dancing in the course was so fun. [First Author] had the best songs!”
Self-efficacy
Outcomes change across time.
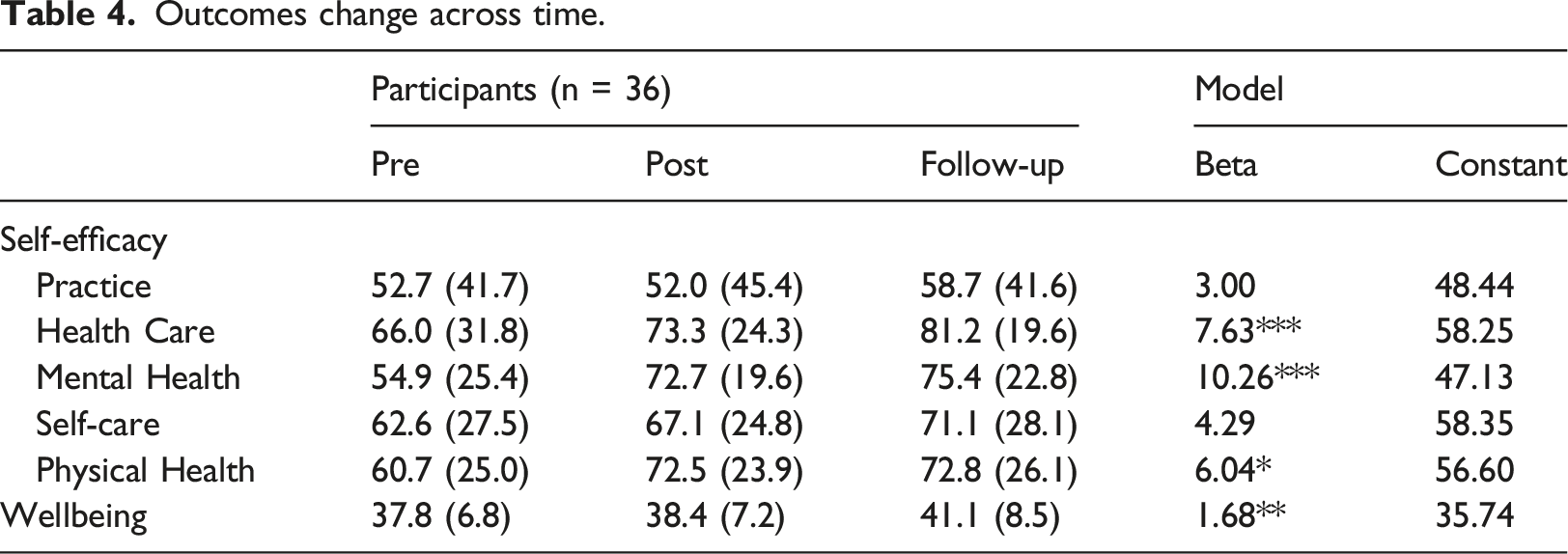
Health care self-efficacy, which had participants reflecting on their confidence in preparing and advocating for themselves during health care visits did change across time (β = 7.63, 95% CI [2.96, 12.29], p = 0.002). The change in scores was significant only from pre to follow-up (p = 0.006). Many participants echoed the value of learning to advocate for themselves, as stated by Participant 106, I was expecting to learn about how to advocate for myself in health care situations. The course did help me with that. Before the course, I was struggling a bit, and I find that with taking the course, it has helped me to learn about self-advocacy and how to advocate.
Mental health self-efficacy also improved significantly over time for participants (β = 10.26, 95% CI [5.71, 14.82], p < .001). Post hoc analysis indicated a significant change from pre to post (p = <.001), and from pre to follow-up (p = <.001). Participants noted that they felt better equipped to manage their mental and physical health after completing the course. Participant 101 stated, “I was able to ask some questions, which I liked a lot because I wanted to understand something, for example improving my mental health.”
Physical health self-efficacy significantly changed over time (β = 6.04, 95% CI [1.42, 10.67], p = 0.011). Post hoc analysis indicated significant differences from pre to post (p = 0.04) and from pre to follow-up (p = 0.03). Participants shared that the course provided them with resources to improve their physical health and related behaviours. Many cited that the dances encouraged them to integrate some purposeful movement into their days, “Dancing from my [wheelchair]. It only takes three minutes!” (Participant 115)
Finally, self-care self-efficacy was the only domain where time had no significant effect (β = 4.29, 95% CI [-0.47, 9.05] =, p = 0.077). Interestingly, one participant did mention that although they did not make any changes towards improving their self-care, they were made more aware of its importance, “There is a lot of stuff that we were taught that I was already doing to begin with. It reinforced that I have to do it more. Self-care is one example…. I don't take care of myself and put myself first. That is a big one for me.” (Participant 43)
Wellbeing
Time had an overall positive effect on wellbeing scores (β = 1.68, 95% CI [0.58, 2.78], p = 0.003. A significant increase was found from pre to follow-up (p = 0.01). Furthermore, while not significant, scores were trending in a positive direction from pre to post (p = 0.06) and from post to follow-up (p = 0.58). Many participants noted that they experienced positive changes in their lives since taking the course. Participant 117, who had been experiencing bouts of sadness stated, It has definitely changed my day-to-day life. I wake up feeling happier with more purpose. I have had a lot of grief over the last two years, and it was feeling monotonous. Someone close to me had died, and I found I was stuck…. I am just feeling much more hopeful than hopeless since the course. I feel like I have the capacity to open up my heart and make new friends.
Mental health and overall health
COVID-LD items related to mental health and overall health.
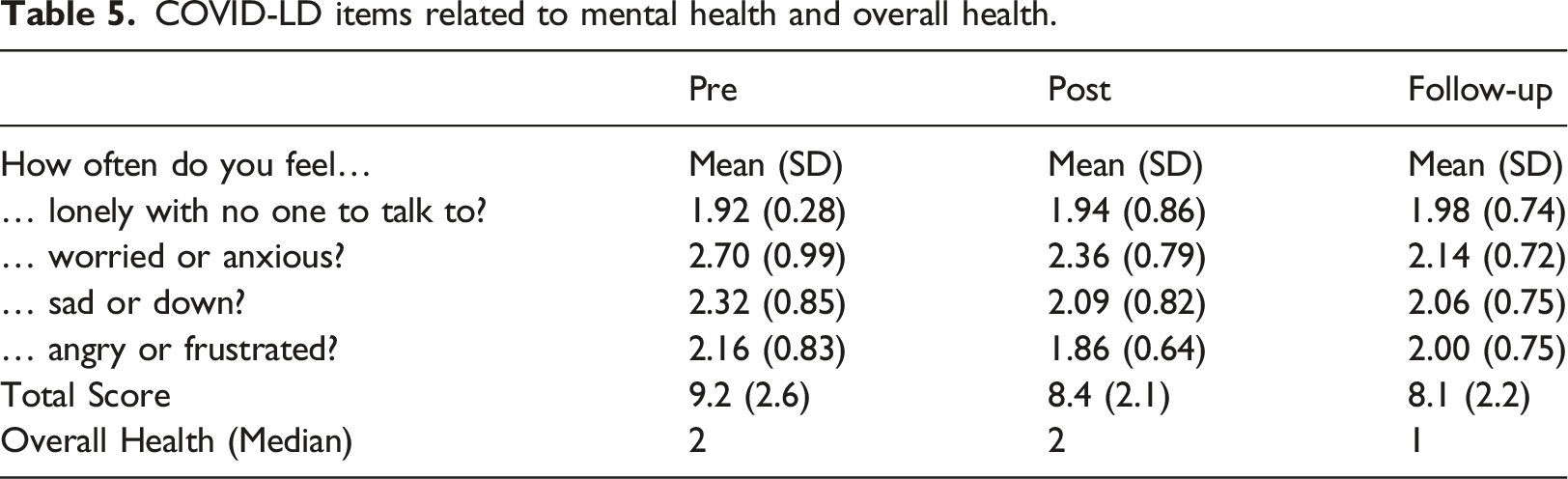
Participants shared that their anxiety and nervousness had diminished after taking the course, with one participant stating, “The course helped me to calm my nerves when feeling nervous” (Participant 45). Several participants mentioned that they were taking a positive step towards improving their mental health by integrating mindfulness exercises into their daily routines, “Day-to-day, I am better at being still, spending time focusing…. I tell Alexa to set a timer for five minutes and I breathe, focus my attention on something… I remind myself to be kinder to myself” (Participant 115).
While this version of the course had a broader focus on overall health rather than solely on mental health, it was noted that some participants felt a course specifically dedicated to mental health would be beneficial.
Sleep and sedentary behaviour
Sleep and sedentary behaviour change across time.
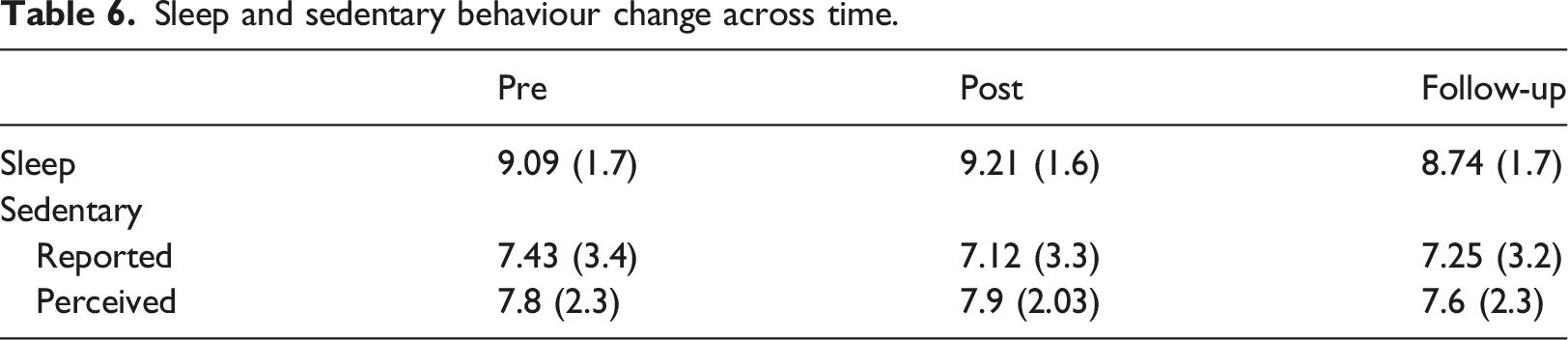
Sedentary time did not significantly change across the three time points (β = -0.10, 95% CI [-0.75, 0.55], p = 0.760) nor did participants' perception of their time spent using technology (β = -0.08, 95% CI [-0.43, 0.28], p = 0.664). Participant 116 noted that the course did not meet their expectations around suggestions for being active. However, Participant 47 did mention positive changes since taking the course, including spending less time on their technology and walking more often.
Discussion
The current study, a conceptual replication of a previous intervention (St. John et al., 2022), provides evidence that virtual courses are effective in addressing health concerns and wellness in individuals with intellectual and developmental disabilities. Results indicated that participants found the course extremely valuable, the lessons accessible, and the resources useful. Importantly, this study detected measurable improvements in mental health-related outcomes, something that was not observed in the prior iteration of the intervention.
Participation and retention for this course was strong, similar to the original program (St. John et al., 2022), with 80% of the sample attending at least four of six sessions. This study’s retention rate aligns with determined cut-offs for studies of this nature (Catherine et al., 2020). This finding is particularly interesting, given that the previous course ran during a period of pandemic restrictions, when participants might have had fewer reasons to miss sessions (i.e. work, social engagements). While there is little research on attendance rates in virtual courses for this population, pedagogical research has reported that in general, online courses tend to have lower attendance rates than in-person courses (Hollister et al., 2022), particularly amongst those with greater support and learning needs. However, in this heterogeneous population, most participants appreciated the online modality, as reflected in their satisfaction data. They noted that the online format made the course more accessible and easier to attend compared to an in-person course. Encouragingly, this preference was reported by many course participants, all of whom had diverse support, learning, and accessibility needs including those with visual impairments, hearing impairments or both. Simple modifications to course delivery, such as using closed captions, providing verbal descriptions of all visuals presented, and offering guidance to support staff, allowed participants with more complex needs to be fully included in the program. This finding helps to dispel concerns regarding the accessibility of online courses for those with greater support needs (Law, 2023), indicating that the effective use of accessibility features, such as those outlined, allows individuals to participate to the best of their abilities.
In the context of the current study, the online format was preferred by participants, despite previous literature highlighting that many clinical populations significantly prefer in-person interventions over virtual modalities (Mazurka et al., 2024). While in-person courses do have benefits for this population, they also present certain barriers such as travel concerns (Weissman et al., 2022), hypersensitivity to new environments (Black et al., 2022) and potential anxiety related to unfamiliar people (Spain et al., 2018). The virtual nature of the course was able to bypass these concerns, creating an inclusive and comfortable environment. Participants were able to use various accessibility features, participate with the assistance of a support worker or simply listen to the teaching when they felt drained or tired. High levels of both attendance and satisfaction illustrate that virtual interventions have value beyond the pandemic for individuals with intellectual and developmental disabilities.
Satisfaction rates were very high and one aspect that participants greatly enjoyed was the involvement of individuals with intellectual disabilities as course co-leaders. They played a crucial role in not only educating participants on the weekly topics, but also contributing to the course design and content, advising on accessibility accommodations (i.e. decisions around font size, images), and leading small group discussions as well as group activities (i.e. mindfulness). This approach is consistent with other studies highlighting the value in having individuals with intellectual and developmental disabilities take on leadership roles (Bazzano et al., 2009; Rodríguez Herrero et al., 2023; Stanish & Temple, 2012). For course participants, the integration of peer supporters and individuals with disabilities into the teaching process can make programs more engaging and enjoyable (Bazzano et al., 2009). In this study, the involvement of their peers as co-designers and leaders contributed to a more supportive and engaging learning environment.
Similar to the original course, this intervention showed improvements in self-efficacy. Average, mental, and physical health self-efficacy all showed measurable score increases from pre to post. As well, like the previous course, self-efficacy was not significantly different from post to follow-up indicating that these changes were maintained over time. While these findings suggest positive effects of the intervention, the changes could also be due to environmental and societal factors (i.e. fewer lockdowns, warmer weather) during the study period (Cutler, 2004). Though it has been argued that online and virtual courses are less effective than in-person options at imparting mental health improvements, for some clinical populations, it appears that online modalities may be effective for those with intellectual and developmental disabilities.
In the original study, participants' wellbeing scores did not significantly change (St. John et al., 2022). While qualitative evidence suggested that some participants exhibited factors associated with positive wellbeing (e.g. increased confidence and happiness), there was no significant change in Warwick-Edinburgh Mental Wellbeing Scale - Intellectual Disability scores and as such concerns were highlighted about the sensitivity of the measure and whether the previous study was adequately powered to detect change (St. John et al., 2022). In this study, mental wellbeing did show improvement for participants from pre to follow-up, with a trend observed from pre to post. It is important to note that the baseline wellbeing scores were on average 12.6 points higher than what was reported in the prior program, held during a period of pandemic restrictions. However, the quantitative improvements in wellbeing were bolstered by participant comments, where many highlighted that after taking the course, they felt more confident and optimistic about the future. It is not possible to know the extent to which the change in mental wellbeing can be attributed to the course itself versus external factors such as the lifting of pandemic restrictions. An important next step for this research would be to employ a randomized study design which would help to determine whether or not the change found is attributable to the intervention itself.
The structure and modality of interventions, whether digital or otherwise, can greatly impact outcomes. Giummarra and colleagues (2022) suggested that interventions designed to improve wellbeing in this population should be person-centered, focusing on improving self-efficacy and self-esteem. They also noted that courses aimed at providing participants with practical, adaptive, and social skills, were more likely to lead to positive change in wellbeing. The current course was able to address adaptive skill deficits in study participants, as a focus of the course was providing participants with tools and resources to become more actively engaged in their health and health care. Additionally, the inclusion of breakout rooms and small group discussions provided participants with opportunities to share their concerns, offer peer support, and build their autonomy (Entwistle et al., 2010). Such autonomy-building practices have been linked to improved wellbeing (Giummarra et al., 2022), making them an important feature of successful interventions for this population. However, it is important to note that while these resources were highlighted and discussed throughout the course, some participants may have been unable to apply these skills independently due to the nature of their disability. In some cases, when asked during follow-up interviews, participants had forgotten that the course discussed certain resources and tools. This highlights that for some participants further guidance is needed beyond the course intervention to support the development of these adaptive skills.
Observable changes related to mental health improved, and it is possible that this is due to some of the self-care skills participants developed throughout the course. Qualitative analysis revealed that participants had begun incorporating activities including mindfulness and physical activity, both of which can positively contribute to one's mental health. The mindfulness activity introduced in the course incorporated deep breathing and repetition of positive mantras, such as “You are loved” and “You are enough”. Participants were encouraged to encorporate these positive affirmations into their daily lives and to engage in positive self-talk, which may have helped participants manage negative thoughts while improving their self-concept (Finley et al., 2018). While participants did not report significant changes in their sleep and sedentary behaviour, several noted that they had incorporated more movement into their daily routines, including watching the in-course physical activity videos after the course was over. These short bursts of movement can be extremely beneficial, especially for someone leading a sedentary lifestyle (Hansen et al., 2001), though likely would not have been a large enough increase to be detected quantitatively.
Limitations
The study has some limitations that should be acknowledged. First, the study, which implemented a non-experimental design, did not use randomization. Without a control group, it is difficult to discern whether or not the intervention was responsible for the changes that were seen. However, in most cases, gains that were reported were maintained at follow-up. Secondly, the use of a subjective assessment of sleep and sedentary time may have resulted in some biases. While the use of this type of subjective assessment was the most feasible for a virtual study, future research may benefit from using an objective assessment such as an accelerometer or another form of wearable health device (Rosenberger et al., 2013). Finally, most of the participants in this study required minimal support in order to participate and as such limits the generalizability of the findings. More work needs to be done to understand how we might adapt a program such as this for individuals who have more complex needs and/or require a greater degree of support in order to participate effectively.
Conclusion
The COVID-19 pandemic has prompted researchers to explore different modalities for implementing interventions. This conceptual replication study provided an opportunity to explore the generalizability of a virtual wellness intervention for adults with intellectual and developmental disabilities. Findings highlight not only the value of wellness-based interventions for this population, but also the benefits of using virtual modalities. This study showed that virtual interventions that are interactive, engaging, and accessible, may be suitable for individuals with intellectual and developmental disabilities, especially when involving teachers with disabilities themselves. Importantly, the study dispels the previously held beliefs that virtual and online interventions are not suitable or feasible for supporting the health of populations with intellectual and developmental disabilities (Chadwick et al., 2022) and instead provides evidence that suggests virtual modalities may not only support the mental health of this population but also lead to improvements.
Virtual wellness courses provide an avenue for researchers to access and connect with participants, regardless of geographical distance, which is particularly advantageous for people who find travel difficult or who live in communities without clinical expertise. It is important to continue to offer opportunities like this, while also exploring how to tailor interventions to people who may not find them accessible, to ensure all individuals with intellectual and developmental disabilities can participate and benefit from these programs.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This study was funded by the Canadian Institute of Health Research (GRANT #EG2 179428).