
Abstract
The current study examined the impact that the COVID-19 pandemic and resulting restrictions have had on individuals with intellectual and developmental disability. Semi-structured focus groups were conducted to collect data from participants who attended day programming by local community agency. Results indicate that the COVID-19 pandemic and its safety restrictions impacted participants’ knowledge of the disease, programming and work, relationships, activities, and emotions in ways that were both similar to and different from other findings in other populations. Implications of these findings for research and practice are discussed.
The global pandemic caused by the novel coronavirus disease 2019, named COVID-19, has had far reaching and devastating impacts on the world (Charkraborty & Maity, 2020). Long-term impacts of the pandemic are just beginning to be realized such as increased poverty, global recession, social, and medical complications (Maital & Barzani, 2020; Sumner et al., 2020). Emerging research has found many factors which have influenced the impact the COVID-19 pandemic has on different populations, including such factors as age, chronic health conditions, ethnicity, and race (Gregory, et al., 2021; Jin et al., 2021). As people adjust to living in a world with COVID-19, it is imperative that researchers continue to explore how responses during the first phase of the COVID-19 pandemic impacted individuals. Examination of the initial and continuing COVID-19 responses for those individuals with intellectual and developmental disability who are an especially vulnerable population to the physical, mental, and social effects of the COVID-19 pandemic (Courtenay & Perera, 2020) is of extreme importance so that future responses can be improved.
As researchers continue to fill-in gaps regarding the impact the COVID-19 virus has on the physical health of individuals with intellectual and developmental disabilities, different statistical analysis, data, and outcomes are continuing to be examined and reported. Initial data from the United States of America and Scotland reported increased health risks and mortality rates for those with intellectual and developmental disabilities who contracted the COVID-19 virus (Gleason et al., 2021; Henderson et al., 2021; Turk et al, 2020). A longitudinal study out of the United Kingdom (Totsika et al., 2021) found that for young adults with intellectual and developmental disabilities, the impact of COVID-19 on health outcomes was not negative and was similar to same-aged typical peers. The researchers found that while older adults with intellectual and developmental disabilities faced poorer health outcomes due to COVID-19 than their typical peers, once researchers adjusted for pre-pandemic health and socio-economic status, health outcomes were like those in the typical population. However, research into long-term health impacts of contracting COVID-19 will continue to be examined for years to come.
Researchers have also examined the impacts that COVID-19 and resulting restrictions have had on the mental health of those with intellectual and developmental disability. Initial findings are troubling. Even though Amor et al. (2021) found that a large majority (greater than 80%) of individuals with intellectual and developmental disabilities in Spain had access to information about COVID-19, understood the information, and the reasons for the subsequent lockdown, still nearly 60% of those they questioned shared feeling fearful or more anxious since the beginning of the lockdown. Lake et al. (2021) found that in Canada adults with intellectual and developmental disability reported that the COVID-19 pandemic and resulting restrictions had negatively impacted their mental health wellbeing. They found that the pandemic and resulting restrictions worsened pre-existing mental illness (such as depression and anxiety) and negative emotional responses including frustration and anger. A thematic synthesis of 20 studies reported that those with intellectual disabilities had increased in difficult behaviors and mental problems including increased anxiety, loneliness, and stress (Parchomiuk, 2022).
Effects from COVID-19 restrictions also impacted global communities of those with intellectual and developmental disability regarding social services, like community programming disruptions, delayed eligibility, and loss of employment (Abbeduto, 2020). Individuals with intellectual and developmental disabilities in Spain reported that half (50%) encountered interruptions to their schooling, and over 70% faced interruptions to their work (Amor et al., 2021). While programming was restricted for some individuals with intellectual disabilities, Lake et al. (2021) found that Canadian adults with intellectual and developmental disability expressed a need for social connection with others including family, friends, peers, and the broader community. A study conducted in the Netherlands found that both residents of a care facility and their relatives reported that the regulations that were imposed by the facility, which limited social interaction and contact, caused emotional trauma, and was difficult to endure (Honingh et al., 2022).
Some research exploring the impacts of the COVID-19 pandemic and its restrictions yielded more positive outcomes. A study based in Ireland, found that adults with intellectual and developmental disability who lived in group homes reported increased rates of contact with families during COVID-19, which may have been due to increased technology use (McCausland et al., 2021). An international review found that the addition of digital solutions improved provision of services, loneliness, and impoverished daily lives (Chadwick et al., 2021). But as they discovered, digital exclusion, poverty, and literacy remain a significant issue for those with intellectual and developmental disabilities. McCausland et al. (2021) also identified the need to increase support and opportunities for individuals with intellectual and developmental disability to connect socially through technology, as they found uneven use of technology, potentially disadvantaging some individuals with intellectual and developmental disability from making social connections. While researchers suggest that virtual social contact may be feasible for those with varying levels of intellectual and developmental disorders, there is not much evidence to show if virtual contact can be used as an alternative to in-person contact (Bakkum et al., 2021).
Near the beginning of the pandemic, the American Association on Intellectual and Developmental Disabilities published a brief (Ervin & Hobson-Garcia, 2020) on the importance of keeping self-determination front and center when making decisions impacting the programming and restrictions for those with intellectual and developmental disabilities. Ervin and Hobson-Garcia (2020) stated that “Although the pandemic presents unique challenges, it cannot be used as a rationale to prevent people with IDD from exercising their rights to self- determination” (p. 456). The authors continue with advice and steps that government agencies and programming organizations could follow to help increase the ability for those within their care to continue expressing their rights to be self-determinate, while also protecting health and safety. However, as Ervin and Hobson-Garcia (2020) point out, there are many restrictions placed on organizations which provide care for those with IDD, and often solutions that balance health and safety and self-determination are not easy or clear-cut.
As researchers begin looking at how organizations responded to the initial lockdowns of COVID-19, it is important to determine how these responses impacted program participants so that future programming and responses can avoid similar pitfalls. Researchers have begun to do this; Friedman (2021) reported that their findings suggest quality of life was hindered by the COVID-19 pandemic for those with intellectual and developmental disabilities within the United States of America. COVID impacts greatly amplified the cracks in the current system for those with disabilities and speaks to the fact that many of the same self-determination issues are still occurring today, with those with intellectual and developmental disabilities bound by the decisions of their guardians or caretakers.
With previous assorted findings, it is imperative that research continue to examine how those with intellectual and developmental disability fared during the first phase of the COVID pandemic. The present study investigated the perceived impacts the COVID-19 pandemic and its resulting restrictions had on those with intellectual and developmental disability. The goal of examining these qualitative data was twofold; first, to better understand how those with intellectual and developmental disability perceived COVID-19 and its resulting restrictions on services, work, home, and social lives, and second, to help provide insight into an understudied population to help guide future responses to similar situations. Guiding research questions were: 1. What is the understanding of adults with intellectual and developmental disability have regarding COVID-19 and its restrictions? 2. What are the experiences and perceptions of adults with intellectual and developmental disability regarding the COVID-19 pandemic and its restrictions?
Methods
Participants & Setting
Participant Demographics
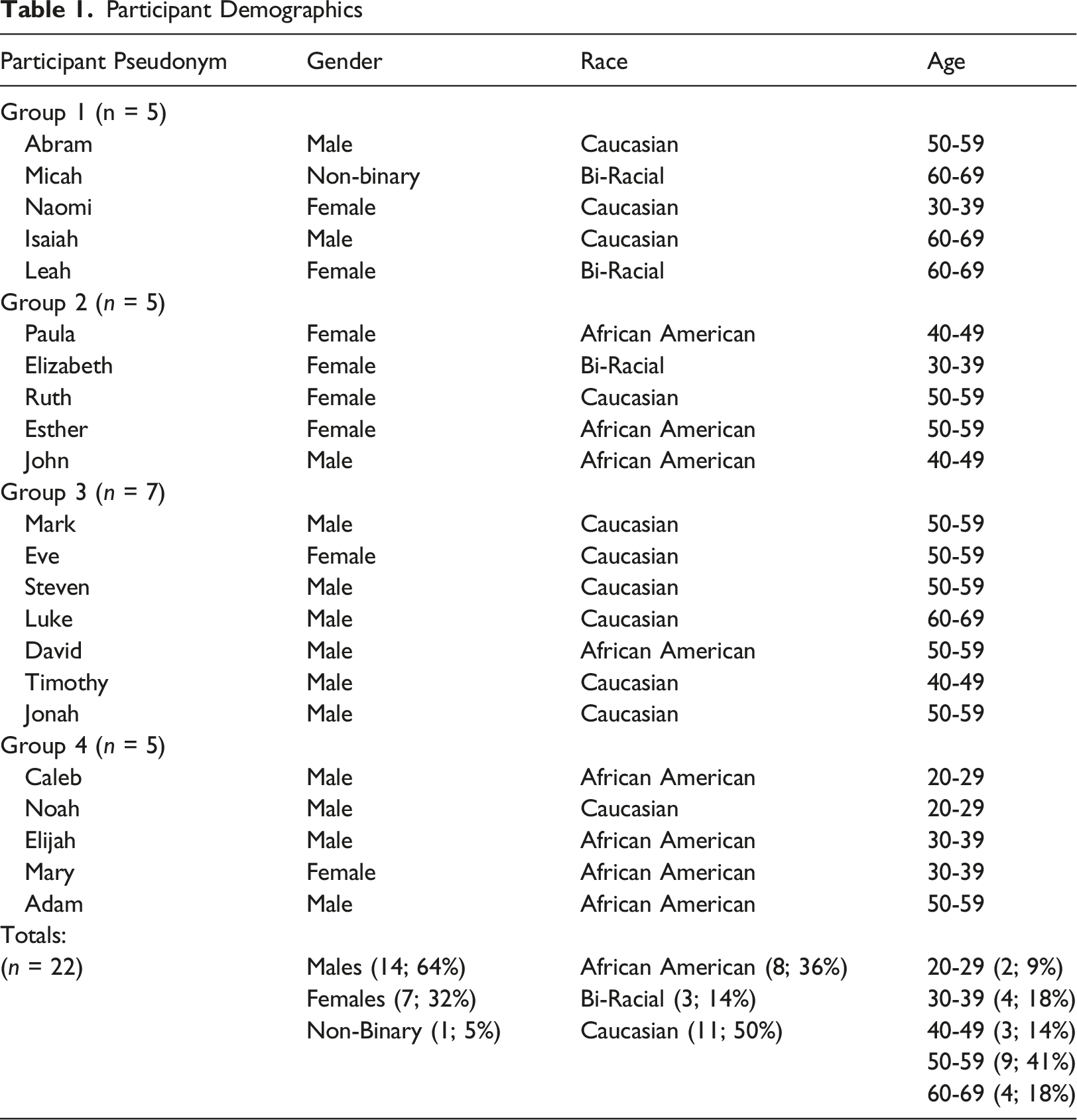
Participants attended two different types of programming at two different locations. The first location had one focus group, and the second location had three. Location one provided day services for clients who live in the community (that is, with family). Participants at location one attend programming daily where they have opportunities to participate in various activities (such as learning functional skills, exploring recreation and leisure activities, etc.). Location two provided programming in a sheltered workshop model. Most participants from location two live in agency-owned group housing or apartments. In addition to providing paid employment, participants at location two have the opportunity to receive additional training to be placed in community jobs (for example hardware stores, fast food restaurants) and have regular trips and outings to various community locations.
While the programming locations had been shut down for a short period (six weeks), programming had continued to run with new restrictions put into place. The state and local operations restrictions for the COVID-19 pandemic were minimally restrictive (e.g., mask requirements, physical distancing, partitions at workstations, signs displaying new rules), and most businesses were able to operate at 50% capacity starting as early as May 2020 (South Carolina Institute of Medicine & Public Health, 2022). At the time of data collection (December 2020), COVID-19 cases were on the rise in the local area, but additional restrictions from state or local officials had not been enacted.
In location one, due to COVID-19, many families chose to keep their family member with intellectual and developmental disability at home, instead of returning to programming. Some clients who had previously attended programming five days a week, had the option of attending less days. Additionally, clients who attended the location had their temperature taken three times each day, with scheduled hand-sanitizing times spread throughout the day. Programming itself had changed, with the location creating more “station-like” rooms, for groups of no more than two clients to participate in at any given time. All clients had to maintain a six feet social distance and wear a cloth face mask and a face shield. Location two had also implemented new procedures to help reduce the risk of COVID-19 infection to their clients with intellectual and developmental disability. Clients all had assigned worktables, that were placed at a minimum of six feet apart from others. While at the location, the client spent most of their time at their desk, including eating lunch there, with the intention of limiting contact with others. Clients at location two also had their temperature taken twice daily and had frequent hand-sanitizing breaks. They too were required to wear cloth face masks and shields. Additionally, locations were temporarily closed for quarantine and sanitizing if COVID-19 cases were identified in the clients.
Procedures
To investigate the impacts of the COVID-19 pandemic and restrictions on individuals with intellectual and developmental disability, this study includes data collected from semi-structured focus groups with participants from the program detailed above. We conducted focus groups across several days at two different sites within the same geographic region in the Southeastern United States. Participant groups were pulled from day programming activities in thirty-minute intervals. Participants completed informed consent forms and a brief demographic questionnaire prior to focus group participation. Each session generally had five to seven participants to allow each participant multiple opportunities to respond. We selected focus groups in order for allow for natural responses between the researchers and the participants as well as between participants; this format also allowed for follow-up questions to be asked as needed for clarification (Glesne, 2016). The focus group protocol was specifically designed with simple language, broad items, and specific follow-up prompts to give participants opportunities to respond with personal experiences and examples. In most cases, the primary researcher repeated responses back to participants to confirm and provide opportunities to member-check responses instead of asking participants to read completed transcripts of the discussion. This method was used to ensure member-checking was accessible for the population of the participants (Lincoln & Guba, 1985).
A detailed list of interview questions and follow-up prompts is available in Figure 1. All interviews were audio recorded using both a computer and a mobile recording device to capture all participant voices while maintaining social distance. Interview length averaged 32 minutes and 5 seconds (range 21:44 - 40:21). Study interviews were conducted by the first author, with the second author attending via Zoom when internet service allowed. Additionally, the interviewer and the participants wore face masks. Participants were not compensated for their participation in these focus groups. Combined, researchers had over 20 years of working with youth and adults with intellectual and developmental disability in public schools, post-secondary education programs, and adult workshop settings. The first author’s expertise in practice and research is special education and supporting youth and adults with intellectual and developmental disability, and the second author’s expertise in practice and research is general education and learning sciences. Semi-Focused Interview. Note. *Pseudonym used.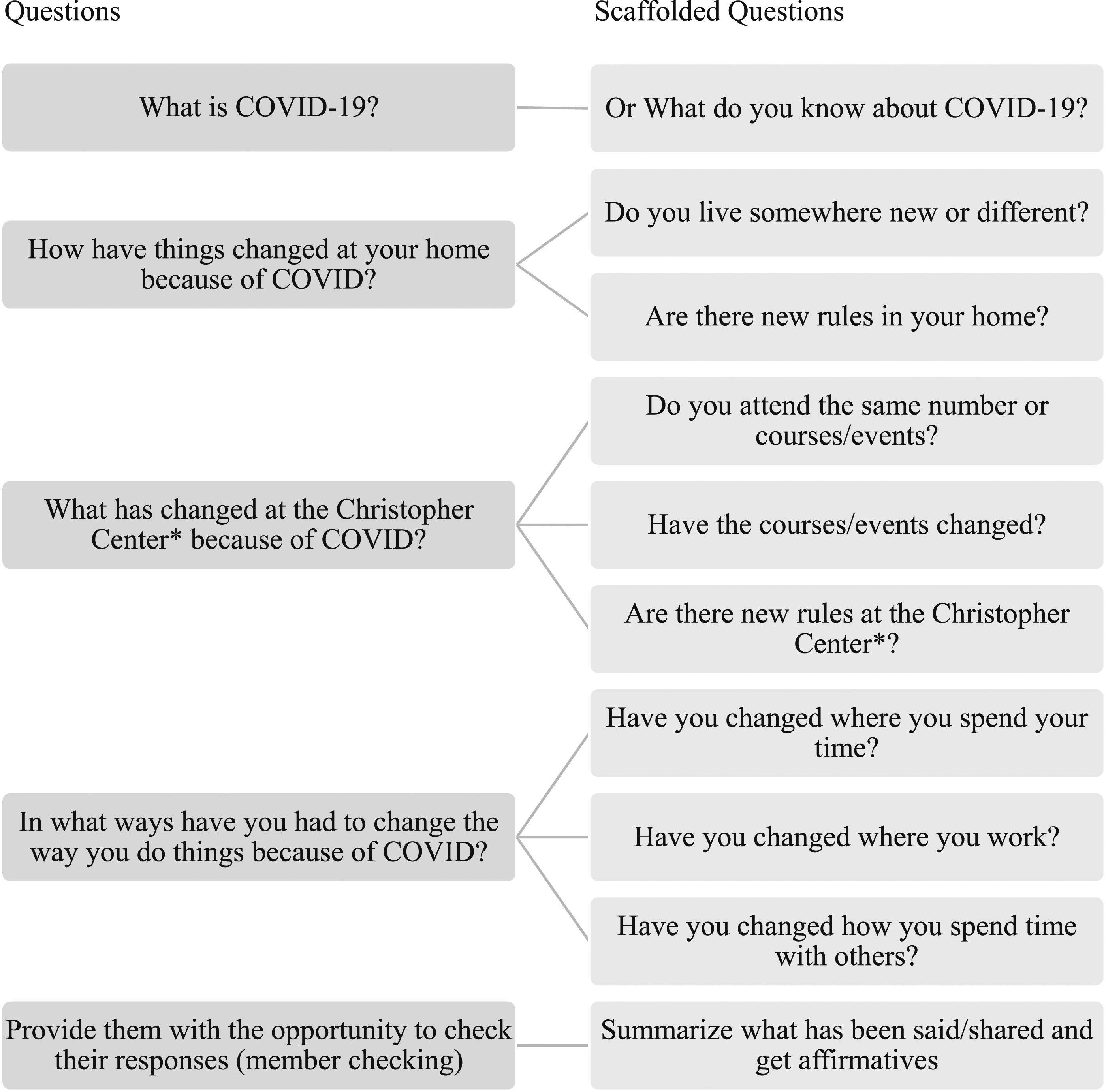
Analysis
Focus groups were recorded and transcribed by members of the research team. Transcripts were coded using Microsoft Word for analysis and were read multiple times by both researchers. Trends were discussed between both researchers before coding began. Data were coded using a grounded theory approach through emergent coding, which seeks to identify common themes and ideas across participant responses (Creswell, 2007; Saldaña, 2015). Notes and memos were kept to define codes, specify their properties, and identify gaps (Charmaz, 2006). Researchers developed official codes together by examining commonalities among participant responses and employed investigator triangulation by discussing and resolving all discrepancies (Morse, 2015). Triangulation across members of the research team suggests that the codes represent the data well in spite of a coder’s individual background or expertise (Patton, 2002). Following the coding process, codes were reviewed and sorted into broader themes, via pattern coding, based on the research questions and thematic similarities (Saldaña, 2015). The team reviewed the final codes and agreed that they accurately represented the participants' responses reflected in the transcripts.
Results
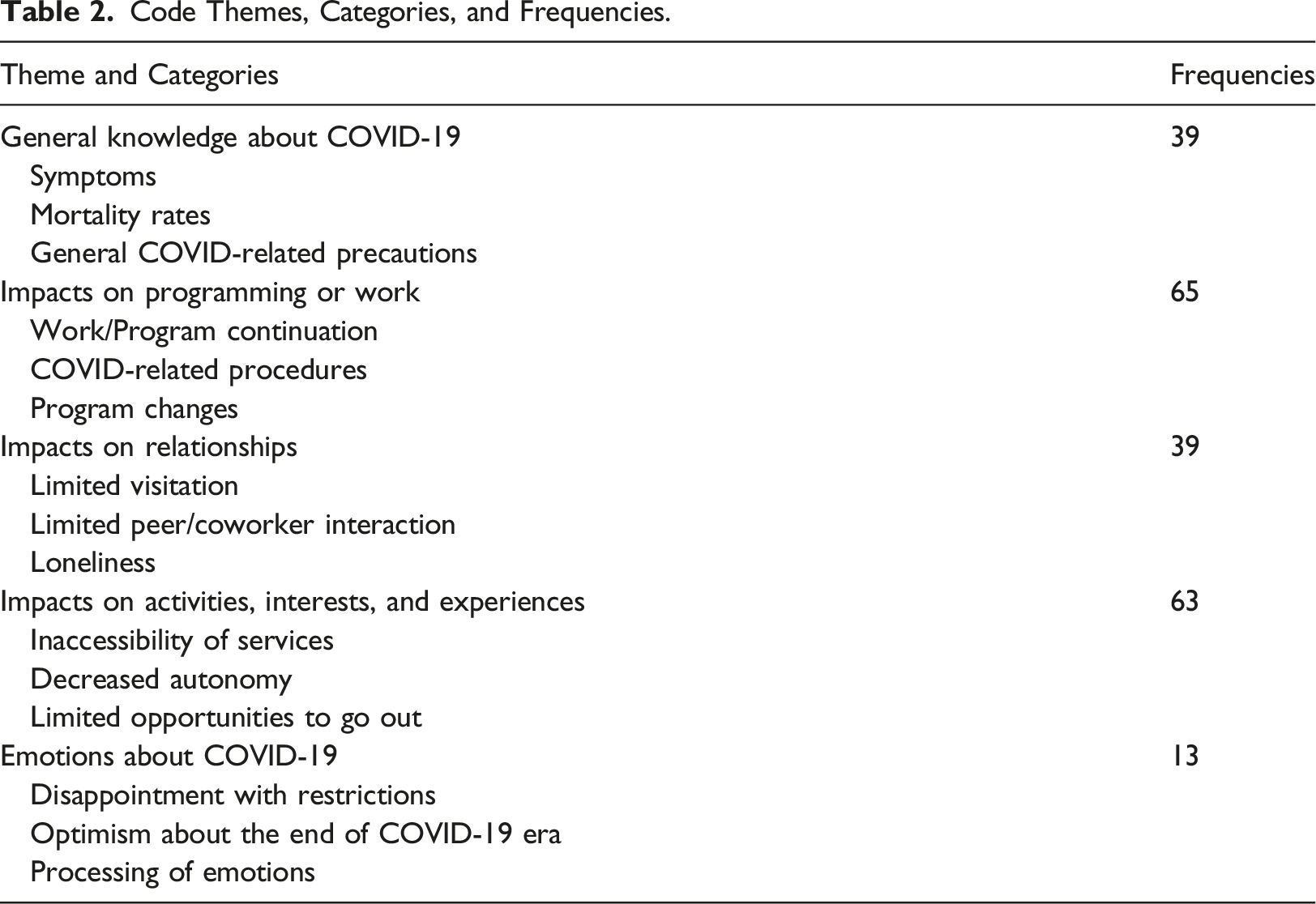
Code Themes, Categories, and Frequencies.
General Knowledge about COVID-19
A primary theme in the data represented participants’ general knowledge about COVID-19 sickness as well as precautions they had taken to prevent catching the disease. This theme included the categories of symptoms, mortality rates, and general COVID-related precautions. Participants stated that COVID-19 was “a virus or disease that’s going around,” (Abram) and that “If someone has it [COVID-19], you can get it from them” (Elizabeth). To illustrate the category of symptoms within this theme, participants described the most common symptoms a person may experience with COVID-19 by sharing statements such as “Sometimes your head might hurt, with it” (David), “They [people who have COVID] can’t talk. They can’t breathe” (Noah), “You get a fever” (Steven). Participants shared their concerns over the possibility of contracting COVID-19 “Someone might get really, really sick” (Timothy), “People on a ventilator machine, and they can’t talk or anything” (Adam), and “You don’t want to get it [be]cause you need to be healthy” (Naomi). Responses concerning the mortality rate associated with COVID-19 included statements about how many people had died from the disease and those recalling stories about specific people who had died like, “I know a couple that had a kid who died from COVID” (Jonah). Lastly, there were many statements about general protocols or precautions people should take to prevent a COVID-19 infection. These included statements like ““Okay, so as soon as you go outside [have to wear a mask]” (Micah), “You keep hand sanitizer with you,” “Wash your hands” (Mary), and “A [face] shield helps protect your face” (Jonah).
Impacts on Programming or Work
Participants also shared reflections about the impacts of COVID-related restrictions on their programming or work. These comments included those about how and when work resumed, new COVID-related procedures, and how programming offerings had changed. Statements about how and when work resumed focused primarily about how things were different when the sites were able to reopen. An example of this type of response includes a participant describing how lunchtime expectations had significantly changed in stating “We gotta get our food from the back room here and take it to the room in here. I just take it back to like my workstation and eat" (Ruth). Many discussed how previous outings at programming had been changed such as, “[We used to] go to outings, to the park. We are stuck in the building [now]” (Noah), and “We used to go to lunch at Bojangles, now we just eat here” (Isaiah). Participants also discussed new COVID-related procedures at their program and work sites by sharing statements like “You have to have your temperature taken" (Adam) and “You all have on a mask in a face shield” (Caleb) to describe new aspects of their daily routines. Lastly, participants described how the program offerings had changed as a result of COVID-19. They described how some of their previous programs had changed and how group activities were different. A participant shared “...social distancing, only two people to a room. So, that limits how close you can get to people” (Noah) when describing how the activity rotation had changed during COVID restrictions.
Impacts on Relationships
Participants also shared frequently about the impacts of COVID-19 restrictions on their relationships. Participant responses in this theme fell into three categories: limited visitation, limited interaction with coworkers and peers, and loneliness. Responses about limited visitation primarily concerned visitation restrictions for participants in residential programming. These participants shared about rules that prevented them from having non-residents (such as family members, significant others) inside their apartments. Responses like these often sounded like “Okay, so, before the whole COVID, I went on Fridays. Typically [to the] movies with my brother, but since COVID, I'm not able to do that anymore” (Isaiah), “I can’t have my boyfriend over at my apartment” (Paula), “[Family] can come and pick me up, but they can’t come into my apartment” (Eve), and “I see her [girlfriend] less now than what I used to” (Luke). Participants also shared examples of how COVID impacted their relationship with coworkers and peers by sharing statements like “[We] used to be one big family here, but now we are separated” (Timothy). A few participants also shared that they believed that due to COVID-19, some staff were no longer with the organization and as a result they felt “Bad and people that had been here aren’t any [more]. [We] miss them, so in a way we are also missing part of our family” (Timothy). Finally, participants shared statements about how the relationship strains from COVID restrictions resulted in loneliness. Some examples of these statements include: “You get lonely” (Ruth), “Okay, so it definitely messes with your social life” (Leah), and “[I] get sad or lonely with all the COVID, not being able to see people" (Esther).
Impacts on Activities, Interests, and Experiences
Participants’ responses often reflected the impact of COVID-19 restrictions on activities, interests, and experiences. The categories in this theme include being left out of COVID-era services, feelings of decreased autonomy, and limited opportunities to go out. Participants indicated that they were left out of some of the services that the general population had access to during COVID (such as meal delivery services, streaming services). Participants shared the new rule of only being allowed to shop at a specific grocery store, and two different dollar stores, “At home, you’re not allowed to go really anywhere. There’s a few places you can go” (Ruth), “[Staff] will go Christmas shopping for you” (Adam), and “They [family or staff] bring me stuff” (Adam). Responses like “Things are sort of normal, but you just aren't able to go out anymore. So instead of going out to dinner, they [staff] bring the food in or you're not able to like do your movie dates" (Isaiah) help to illustrate the ways that participants have had to work around COVID restrictions in spite of the inaccessibility of some burgeoning services. Participants also shared statements centered around a perceived loss of autonomy during COVID restrictions. Numerous participants shared comments about the vending machine being out of order like “But since this they've taken the drink machine away and you're only allowed to take your mask off to drink at breaks and lunch” (Abram), demonstrating a lack of autonomy both in the opportunity to make a drink selection and when they’re able to drink a beverage. Lastly, participants shared comments about restrictions on outings. Participants made statements like “We can. So, if your family comes to pick you up, and they say, ‘Hey let's go to the mall,’ you can [go]” (Elizabeth), “Christmas parade was cancelled” (Eve), “I can’t even go to Night to Shine” (Mark), and “No more going out to eat, you just you can go through the drive through and bring it home” (David). These statements demonstrated how new restrictions governed how and when participants could go out, and that participants with local family members had additional opportunities to go on outings.
Emotions About COVID-19
Our final theme concerns emotions about COVID-19. The categories for this theme include disappointment with the restrictions, optimism about the end of the COVID-era, and processing of emotions. Statements of disappointment with the restrictions generally included anger about not being able to do things that were routine before COVID. Examples include “[I feel] bad, I can't see my friends, angry” (Timothy), “[I] get angry all the time” (Paula), and “Because it's a real threat. Your mom [is] trying to protect you, but it still makes you sad that you're not able to spend Thanksgiving with them” (David). While participants generally seemed to demonstrate understanding that restrictions were in place to keep them safe, they did share strong feelings about how the pandemic impacted their lives. Statements of optimism about the end of COVID restrictions included comments like when Timothy shared “How I long for the day when we can look back and say ‘bye-bye COVID’.” These statements demonstrated participants’ understanding that COVID-related restrictions were finite, but that they were looking forward to a return to normalcy. Finally, statements demonstrating the processing of emotions were those that modeled the transition from negative emotions to more positive ones (for example anger to peace or optimism). These statements included examples like Jonah stating he was “Not real[ly] happy about these changes Not really, but now I understand,” demonstrating dissatisfaction with the current restrictions, but at peace with the current situation.
Discussion
Using qualitative methods, our study endeavored to discern the impact that the current pandemic and resulting restrictions have had on individuals with intellectual and developmental disability. We did this by attempting to examine participants’ subjective experiences and beliefs on the COVID-19 pandemic and resulting restrictions. Our study was guided by two research questions, both aimed at understanding our participants’ knowledge of COVID-19 and how the pandemic and resulting restrictions have impacted their lives. Answering these questions are critical, as we know that individuals with intellectual and developmental disability may experience more negative impacts (such as increased likelihood of death and mental health concerns [Reardon et al., 2015; Turk et al., 2020]) than the general population. Understanding the context and timeline surrounding the organizational and programmatic policies regarding COVID-19 help to position the study’s data within the larger international body of COVID-19 research. Programming provided by the organization began after the initial lockdown period in the summer of 2020. The organization utilized a soft re-opening process where a group of 7-10 clients were returned at a time per service. This process occurred over several months, and data for the current study was collected in December of 2020. While programming policies continue to be revised as COVID-19 cases rise and fall, the organization considers the response to COVID-19 to be a consistent response process. As of October 2022, the organization was at an approximate 70% return rate for all services.
The current research was designed and conducted using a grounded theory approach, which was exploratory in nature. Our purpose was to learn more on the impact the COVID-19 pandemic and resulting restrictions had on the study’s population, as there was not much published research when we began this project. After conducting the study however, we believe that our findings could be linked back to the self-determination theory as developed by Wehmeyer and colleagues (1996). Wehmeyer et al. (1996) posits the importance that autonomy plays in the development and demonstration of self-determination for individuals with intellectual and developmental disability. Findings from the current study support the critical element of autonomy and how it fosters self-determination and life satisfaction.
Our first question intended to examine the knowledge that adults with intellectual and developmental disability had regarding the COVID-19 pandemic and resulting restrictions. Findings indicated that participants had accurate and extensive knowledge regarding what COVID-19 is, how it’s spread, and what precautions they should take. Focus groups described how the COVID-19 virus spreads (e.g., through the air and person-to-person contact) and the various associated symptoms (such as cough, fever, headache, etc.). Participants shared safety protocols in place (that is face shields, hand sanitizer, six-foot distance from others), and how that would help to protect them from contracting the virus. This indicates participants are well informed and have been taught not only the proper precautions to take to keep themselves and others safe from the virus, but also the reasoning behind them. These findings are similar to those reported by Amor et al. (2021). As prior research has shown the devasting consequences that contracting COVID-19 can have on individuals with intellectual and developmental disability, who have the highest risk of death due to contracting the virus other than age (Gleason et al., 2021), it is encouraging to know that our participants are knowledgeable on proper safety precautions and were confident in the steps they could take to keep themselves and their peers from becoming ill.
While focus group participants had good knowledge of the COVID-19 virus, they still expressed feelings of frustration, sadness, and loneliness due to the subsequent isolation and restrictions. These findings are similar to previous research which found adults with intellectual and developmental disability reported feeling overwhelmed, stressed, and frustrated (Lake et al., 2021; Parchomiuk, 2022), even with proper information and understanding of COVID-19 illness and restrictions (Amor et al., 2021). Negative mental health consequences shared by those with intellectual and developmental disabilities are like those of the general population, where participants reported increased anxiety, depression, stress, and overall psychological distress (Serafini et al., 2020; Xiong et al., 2020). Interestingly, focus groups displayed knowledge regarding why the isolation and restrictions are necessary by sharing how COVID-19 is spread from person-to-person, and people can get very sick from the virus. Focus groups expressed that while they are sad and lonely due to the restrictions, they also understand the necessity of staying safe and healthy. Embracing these precautions in an effort to return to programming activities at the center may have also offered opportunities for participants to actively make decisions for themselves (i.e., choosing to wear a mask or face shield to prevent illness and return to activities). Additionally, participants may have viewed these precautions as autonomous decisions they could leverage to access some normalcy in uncertain times. We suspect that knowledge about COVID-19 and active decision making about precautions may be related, specifically in individuals who returned to programming shortly after the initial shutdowns were lifted.
Our second question was aimed at investigating the perceived impacts that various COVID-19 restrictions have on adults with intellectual and developmental disability on their home and program life. Those with intellectual and developmental disability need access to a wide variety of community services (such as libraries, public transportation, and public recreation) to participate fully in their community (Thompson & Nygren, 2020). However, focus group participants shared numerous examples of how COVID-19 and resulting restrictions have impacted both their home and program life. Participants opened up about feelings of anger, frustration, loneliness, and sadness when discussing how their lives have changed due to the restrictions from the pandemic. These findings are similar to other adults with intellectual and developmental disability who shared that the pandemic had significantly impacted their sense of connectedness to people (Honingh et al., 2022; Lake et al., 2021; Parchomiuk, 2022), as well as to the general population (Torales et al., 2020; Xiong et al., 2020). Many of the restrictions designed to keep the individuals safe from the virus have also significantly impacted interactions with partners, friends, and family, which can impact overall quality of life (Boehm & Carter, 2019; Friedman, 2021; Serafini et al., 2020). Focus groups were unanimous when sharing how visitors and outings have been severely limited. For example, previously participants could request shopping trips with staff on an as-needed basis (for example the mall, Walmart, etc.). Participants shared that new restrictions limit their shopping to three specific shopping locations (including Dollar General, a grocery store). Participants who live independently in program-operated apartment buildings or group homes were no longer allowed to have any visitors, including family. Participants were allowed to go to family members’ houses, but those with no family or nearby relatives were limited to their apartments. While our findings were similar across participant living situations (with family vs in a center-managed apartment), we suspect that participants living with their families had greater access to these opportunities because they were not beholden to the same COVID-19 policies and regulations as the center. The overall reduction in social outings and activities for everyone in high-risk groups in 2020 may speak to the similarities in responses across living situations. As a result, participants may not have realized how much their lives differed due to living with family or in program-provided housing.
Throughout the focus group interviews, participants each added pieces of information, that, when analyzed together, indicated frustration over loss of autonomy (such as choice-making). Participants in three focus groups who attended programming at the same location mentioned their anger and frustration over two specific changes that had been made to their daily work environment: (1) the removal of a drink and snack vending machine and (2) changes to lunch. A staff member shared that the vender did not restock the machines due to restrictions on vender personnel. As a result, many of the drinks and snacks expired. Participants also expressed that programming staff felt it would be safer if they were not touching the same buttons on the vending machines. As a result, the vending machines have been turned off. On the surface this may seem like a small change, however it appears to impact the participants autonomy. Before this change, individuals could bring in money and choose various drink and snack options. Now, that activity has been eliminated.
Additionally, participants all shared their frustration and anger over the change in the program’s lunch structure. Before COVID-19, participants all ate lunch in a large cafeteria where they received food that was made on-site and could choose to sit where they wanted (for example by friends). The programing lunch changes due to COVID-19 resulted in food being brought in from an off-site location, individuals getting their food from a smaller room, and then eating at their work desk. The work desk is six feet apart from other desks, and where participants spend most of their day. Participants were frustrated over having limited options for lunch, as well as being required to sit at the same place all day. While both the vending machine and lunch changes in and of themselves may seem insignificant, when we look at our participants ability to be self-determinant it is apparent that those with intellectual and developmental disabilities are still bound to others’ decisions.
Considering that those with intellectual and developmental disability traditionally have limited options to express autonomy, awareness of even more restrictions due to the pandemic is cause for concern (Ervin & Hobson-Garcia, 2020). Autonomy is the ability to make decisions based on personal preferences (Wehmeyer, 1999). Autonomy may be displayed in choosing what you want to eat for lunch or where you shop for your groceries. Individuals displaying autonomous behaviors act in ways that correspond with their own preferences, abilities, or interests, independently or free from excessive external pressure (Deci & Ryan, 1987; Wehmeyer, 1997). Behavioral autonomy can be placed into the following categories (Sigafoos et al., 1988): (a) self and family care activities, (b) self-management activities, (c) recreational activities, and (d) social or vocational activities. Autonomy is an important characteristic of self-determination (Wehmeyer, 1997; Wehmeyer et al., 1996; Wehmeyer, 1998). The current findings reveal that many of the activities that allow individuals the ability to be autonomous have been reduced due to pandemic restrictions, such as assigned seating at lunch, limited options for grocery shopping, and no visitors. Reduced opportunities for autonomous behaviors can lower individual’s self-determination skill levels, thus detrimentally impacting those individuals with intellectual and developmental disability.
Self-determination is essential for improved quality of life for individuals with disabilities. Research has shown that there is a direct correlation between self-determination skills and quality of life for individuals with intellectual and developmental disability (Wehmeyer & Palmer, 2003). That is, the higher the self-determination skills in an individual with intellectual and developmental disability, the higher their quality of life (Wehmeyer & Schwartz, 1998). Additionally, individuals with intellectual and developmental disability and high self-determination skills are significantly more likely to live independently, have financial independence, and maintain better jobs (Wehmeyer & Palmer, 2003). The loss of autonomy not only has the potential to negatively impact self-determination skills and quality of life for individuals with intellectual and developmental disability, but it may also increase mental health difficulties. Previous research has shown that traditional treatment options (such as cognitive behavior, telepsychiatry) for mental health concerns have been used with individuals with intellectual and developmental disability; but there is limited research showing the effectiveness of these methods (Koslowski et al., 2016). As a result, other ways of increasing mental health outcomes and well-being have been investigated by researchers. Time with family (Alonso-Sardón et al., 2019) and opportunities to express autonomy (Deci, 2004) both have been found to increase overall well-being for those with intellectual and developmental disability. However, as our and previous research findings have shown, if restrictions are in place limiting autonomy and connections with others, individuals with intellectual and developmental disability could potentially have a long road ahead to regain the independence they may have experienced prior to the pandemic.
Limitations
The following limitations should be considered when interpreting the findings of this study. First, our population was small with only four focus groups and 22 total participants. Of the participants from the first location, only families who were comfortable sending their loved ones to the center during the pandemic were in attendance. Participants from the second location were also limited, as the percentage of clients who returned to work varied in accordance with local area and or internal surges. Another potential limitation is that for this study we did not pursue data triangulation across different providers, or geographic locations with different restriction levels. Additionally, while participants attended two separate programs and facilities, both programs and facilities are run by the same central provider. As a result, findings from this study apply specifically to this population and provider. Another potential limitation is that while programming was shut-down for a short time (i.e., 6 weeks) during the initial response to the COVID-19 pandemic, programming was able to continue in some fashion during the majority of COVID-19 resulting shutdowns. As a result, the full effect of COVID-19 restrictions may have been subdued or lessened for the study’s participants compared to areas with longer shutdowns, more intense restrictions, or higher infection rates.
Implications for Practice
Results from this study add to the growing body of research available regarding individuals with intellectual and developmental disability and the impacts of the COVID-19 pandemic. Current study results should help inform current practice and encourage further research. Program coordinators and administrators have several tasks ahead as life continues to return to a more “normal”. Programs need to consider how COVID-19 restrictions impact mental health of their clients with intellectual and developmental disability, in addition to their physical health. Programs should organize and offer mental healthcare opportunities for people with intellectual and developmental disability (Cullen et al., 2020; Dodd et al., 2017; Serafini et al., 2020) to discuss mental health concerns (such as anxiety, fear, depression, anger) which have resulted from the current pandemic and restrictions. Increasing and supporting autonomy in individuals with intellectual and developmental disability is one way to help overall well-being and mental health. It is imperative that those who are involved in interactions and programming allow as much autonomy as possible for those with intellectual and developmental disability.
Also, while the various restrictions help to keep individuals with intellectual and developmental disability safe from the virus, they have also significantly impacted interactions with family. Previous research has indicated the importance of relationships in the overall quality of life of individuals with intellectual and developmental disability (Boehm & Carter, 2019). As a result, programming needs to carefully evaluate the benefits of isolation against the impact on quality of life as vaccinations and the decline of infection become more prominent and consider how they can facilitate healthy familial relationships in the wake of future service disruptions (e.g., natural disasters). Working with families of those with intellectual and developmental disability to establish evolving family visitation rules and policies is one way to approach this challenge illuminated by the COVID-1p pandemic (Bradley, 2020).
Additionally, once restrictions have abated, several program changes need to be executed. First, programming to re-establish and foster autonomy and independence following the COVID-19 pandemic needs to be developed and ready to implement. As Ervin and Hobson-Garcia (2020) state, restrictions from COVID-19 cannot be used to undo the progress that has been made in fostering and promoting self-determination of individuals with intellectual and developmental disability. While immediate challenges from the pandemic were inevitable (dining rooms of restaurants closed), there are alternative services available through online methods that can be used to foster and allow choice-making. Online banking, food delivery services (for example DoorDash, UberEats), and online shopping are just a few of the internet-based services that the restrictions have encouraged to become the new “normal”. As a result, programs need to look at developing and offering programming and education for their clients with intellectual and developmental disability to ensure that they have the skills and means needed to utilize these internet-based services.
Future Research
Future Research on impacts from the COVID-19 virus and resulting restrictions have had on individuals with intellectual and developmental disability should continue in several ways. Researchers should continue to explore the various impacts that COVID-19 restrictions may have on individuals with intellectual and developmental disability, specifically focused on identifying differences between those who remained in programming during the pandemic and those who did not. While we do not know the long-term effects that the current pandemic will have on the general population, it is imperative to continue to identify and examine the long-term effects of COVID-19 restrictions on independence and skills of people with intellectual and developmental disability. Future research should continue to examine the various supports and services available to individuals with intellectual and developmental disability, and how participants make use of available support staff and resources. Additional lines of research may emerge focusing on increasing opportunities to study autonomy in people with intellectual and developmental disability and how larger societal transitions (such as cashless economy, reliance on online shopping, etc.) may impact individuals with intellectual and developmental disability.
Conclusions
Participants shared concerns regarding the impacts of COVID-19 restrictions on their lives like those shared by the general population and by others with intellectual and developmental disability in previous research. Additionally, participants expressed a good working knowledge of how to prevent COVID-19; however, COVID-19 restrictions have impacted autonomy of participants in more and different ways than we expected. Mental health supports need to be provided to adults with intellectual and developmental disability, and programming and supports for individuals with intellectual and developmental disability need to continue to work on new and varied methods (such as online shopping) aimed at increasing autonomy for individuals with intellectual and developmental disability.
Footnotes
Acknowledgements
The authors wish to express our gratitude to the agency’s administration and staff for helping to organize the study and providing access to their clients. Additionally, a heartfelt thank you to the clients who participated in the discussions and shared their knowledge, thoughts, and feelings with us.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
Please contact the corresponding author for raw study data.