
Abstract
Objective
The clinical aspects of lung cancer patients are well-studied. However, healthcare charge patterns have yet to be explored through a large-scale representative population-based sample investigating differences by socioeconomic factors and comorbidities.
Aim
To identify how comorbidities associated with healthcare charges among lung cancer patients
Methods
We examined the characteristics of the patient sample and the association between comorbidity status (diabetes, hypertension, or both) and healthcare charge. Multivariate survey linear regression models were used to estimate the association. We also investigated sub-group association through various patient and socioeconomic factors.
Results
Of 212,745 lung cancer patients, 68.5% had diabetes and/or hypertension. Hospital charges were higher in the population with comorbidities. The results showed that lung cancer patients with comorbidities had 9.4%, 5.1%, and 12.0% (with diabetes, hypertension, and both, respectively) higher hospital charges than those without comorbidities. In sub-group analysis, Black patients also showed a similar trend across socioeconomic (i.e. household income and primary payer) and racial (i.e. White, Black, Hispanic, and Asian/Pacific Islander) factors.
Discussion
Black patients may be significantly financially burdened because of the prevalence of comorbidities and low-income status. More work is required to ensure healthcare equality and promote access to care for the uninsured, low-income, and minority populations because comorbidities common in these populations can create more significant financial barriers.
Introduction
In 2022, there were 130,180 lung and bronchus cancer deaths in the US and 236,740 new cases. 1 Although cases and deaths have been slowly declining, 1 lung cancer remains one of the most common cancers in the US and is responsible for the most cancer deaths in 2022. 2 Non-Hispanic Black patients have the second highest new cancer rates, surpassed only by non-Hispanic white patients, but have the highest cancer death rate. 3 Though treatment advancements have promoted decreased mortality rates, 4 most lung cancer cases have already metastasized, and their 5-year survival rate is 7%. 1 The overall 5-year survival rate is 22.9%, 1 and lung cancer screening remains underutilized. 5 Because of lung cancer's low survival rates, understanding underlying factors is crucial for adequate care.
The most common comorbidities associated with hospitalization include hypertension and diabetes. 6 Hospitalizations complicated by comorbidities can have longer lengths of stay, higher mortality rates, greater readmission, and higher total charge. 6 Hypertension is commonly uncontrolled and affects 37 million US adults. 7 It is most common in Black patients, but Black patients are less likely to have their blood pressure under control than white patients. 7 About 28.7 million people had diabetes in 2019, with the highest prevalence in minority populations than non-Hispanic Whites. 8 Non-Hispanic whites had a 7.4% prevalence of diabetes, half the amount of American Indians and Alaska Natives (14.5%) and 4–5% less than non-Hispanic Black patients (12.1%). 8 Some of the highest prevalence was in patients below the poverty level at 13.7% for men and 14.4% for women. 8
Because of how common comorbidities like diabetes and hypertension are and their effect on hospital outcomes, 6 it is relevant to explore how those comorbidities affect patients with lung cancer. Past literature found that more than half of their participants had lung cancer and one or more comorbidities associated with differential treatment selection and survival in the early stages. 9 Other research found that patients with comorbidities are more likely to undergo lung cancer screenings, possibly because of increased healthcare visits.9,10 However, these results are inconsistent with similar studies on veterans and patients with lung cancer and comorbidities, finding that screening was not associated with comorbidity.11,12 Still, patients who undergo lung biopsies and have COPD, a common lung cancer comorbidity, are at a higher risk for pneumothorax and complications than previously health patients.13,14 While research on the prevalence of comorbidities among patients with lung cancer has increased, more work is needed to apply this knowledge in practice through improved screening methods. 14
The importance of studying comorbidities and their effect on lung cancer survival rates is further highlighted in a study by Monirul Islam et al. which found that chronic diseases associated with older age are independently linked with changes in survival outcomes. 15 For example, diabetes with complications had one of the highest risks for poor survival in local lung cancer. 15 It was also more than double the risk from renal disease or myocardial infarction. 15 In addition, COPD and coronary artery disease were implicated in a greater risk of surgical complications, a standard treatment for stage 1 non-small cell lung cancer. 16 Other research found that patients with respiratory comorbidities are less likely to have surgical treatment and are more likely to have worse survival, while patients with cardio-related comorbidities had a higher risk of death from other causes. 17
Past literature has also demonstrated differences in healthcare charges based on differences in comorbidities. For example, patients diagnosed with depression before receiving a lung cancer diagnosis were more likely to use hospice care and be in hospice for longer than patients diagnosed with depression after their lung cancer diagnosis. 18 They were also less likely to be hospitalized, visit the ICU or emergency department, or die in-hospital than post-diagnosis depression patients. 18 Diabetes or pulmonary diseases are also associated with increased odds of death from radiation pneumonitis, a complication of radiation treatment for lung cancer. 19 Patients with comorbidities and lung cancer are more likely to die from those comorbidities rather than their lung cancer. 16
Comorbidities may play an essential role in lung cancer outcomes and could also demonstrate relevant health disparities. 20 For example, one study found a higher likelihood of diabetes and heart attack in men with lung cancer, while black patients (men and women) were more likely to have a history of stroke. 20 Research demonstrates differences between Black and White lung cancer patients regarding lung cancer treatment and mortality, with Black patients less likely to receive guideline treatment and more likely to die from lung cancer.21,22 While the disparity between races is multifaceted,21,22 it becomes relevant to determine how differences by comorbidity may also play a role since chronic diseases have historically impacted minorities more than white patients.23–25
This study explores if diabetes and hypertension, common comorbidities with racial disparities,6–8 are associated with differences in healthcare charges in patients with lung cancer. Comorbidities have been shown to affect lung cancer outcomes,15–17,19 and their disproportionate impact on minorities23–25 could contribute to differences in lung cancer treatment and death.21,22 By analyzing if comorbidities are associated with differences in healthcare charges and investigating those differences by patient factors like race, we hope to identify marginalized populations and areas with a greater need for research and resource allocation.
Methods
Data collection
The latest 2019–2020 United States National Inpatient Sample (NIS) data was used to obtain a population-based estimate for patients with lung cancer. As shown in Figure 1, we first identified the primary diagnosis of lung cancer (total n = 44,264) using the International Classification of Diseases, 10th Version (ICD-10) codes for lung cancer among all 2019–2020 NIS samples (N = 13,554,970). Then, after patients with missing variables were excluded, we obtained our patient sample (n = 42,549, National Estimates = 212,745), (Figure 1).
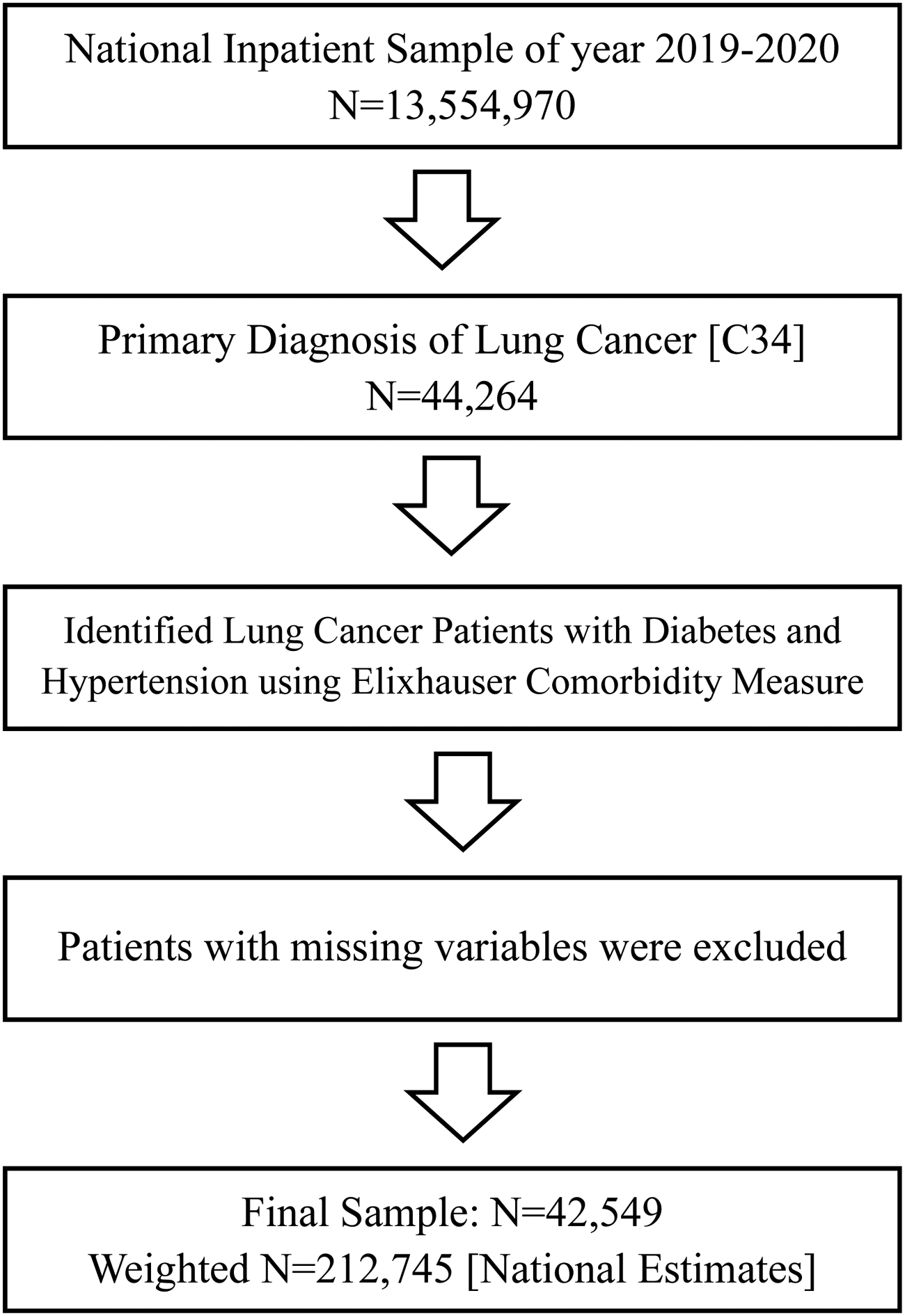
Flow chart of patient sample selection.
Variables
The primary outcome of this research was to investigate how comorbidity status is associated with hospital charges and any differences presented by critical socioeconomic factors. The variable pertaining to hospital charges was coded as “total charges” in the NIS data, serving as a metric for evaluating the financial expenditure borne by the hospital. We chose diabetes and hypertension as the comorbidities to be used because of their prevalence and high cause of mortality in the US. 26 We employed the comorbidity status directly from the NIS data sample; the dataset identified diabetes and hypertension comorbidity using the Elixhauser Comorbidity Measure from 2019. In addition, we adjusted for various patient and hospital confounders. Patient characteristics included age, race, annual median household income, primary payer (Medicare, Medicaid, self-pay, or private insurance), rurality, and whether the patient received surgery, radiation, or chemotherapy. Hospital characteristics include bed size, ownership, teaching status, and region.
Statistical analysis
Sampling weights were used for all statistical analyses to represent nationwide lung cancer patients, and due to the skewing of distribution for hospital charges, we conducted the natural log of those variables. First, we examined the characteristics of the final dataset. The patient characteristics were presented as weighted frequency (percentage) or means (SD). Then, we investigated the temporal trend of hospital charges by socioeconomic factors, race, primary payer, and sex. Next, we investigated how the comorbidities were associated with hospital charges using the multivariate survey linear regression analysis. Additionally, we ran the models with patient factor sub-groups to determine more specific comorbidity status associations. All analyses were conducted using SAS statistical software (version 9.4; SAS Institute Inc., Cary, NC, USA). All statistical tests were two-sided, and statistical significance was determined at a p-value <0.05.
Results
Patient characteristics
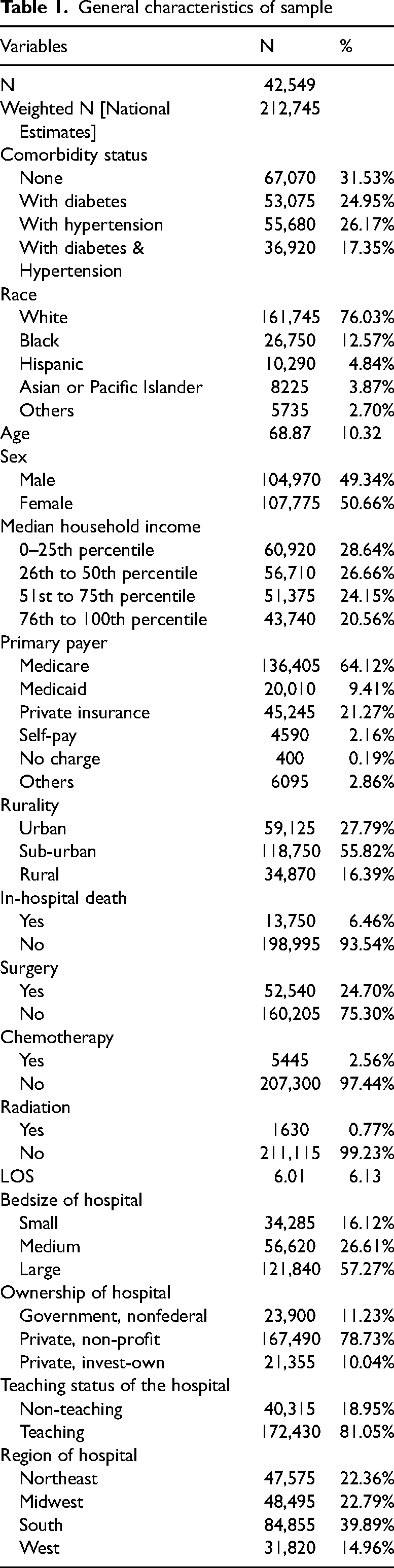
A total of 42,549 lung cancer patients were identified in the 2019–2020 NIS data (weighted n = 212,745, Table 1). Of them, 31.53% did not have either comorbidity, 17.35% had diabetes and hypertension, 26.17% had hypertension, and 24.95% had diabetes. More detailed characteristics of patient characteristics are presented in Table 1.
General characteristics of sample
Hospital charges by comorbidity status and social factors
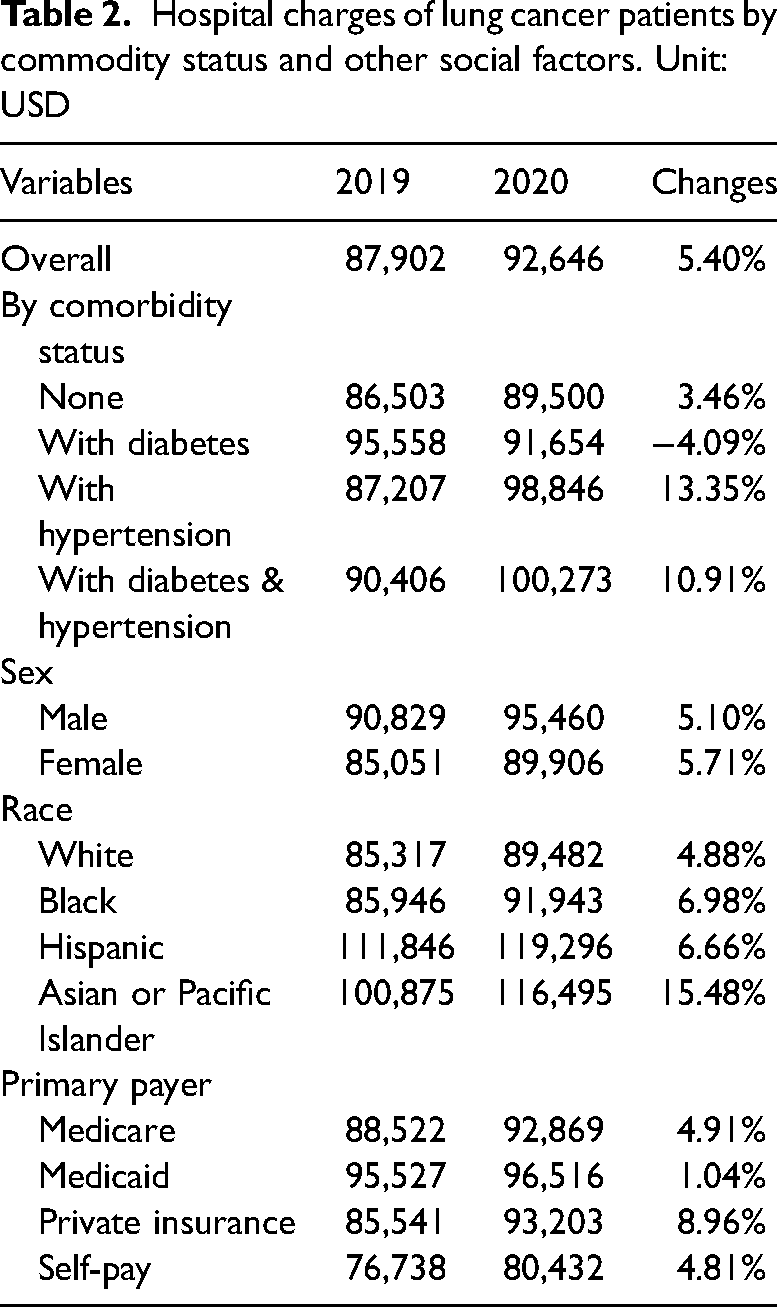
Table 2 shows the hospital charges among hospitalized patients with lung cancer between 2019 and 2020. Hospital charges somewhat increased during the study period. In addition, hospital charges were higher among patients with lung cancer who had comorbidities or were male, from minority populations, or who used Medicaid.
Hospital charges of lung cancer patients by commodity status and other social factors. Unit: USD
Association of comorbidity status with hospital charges
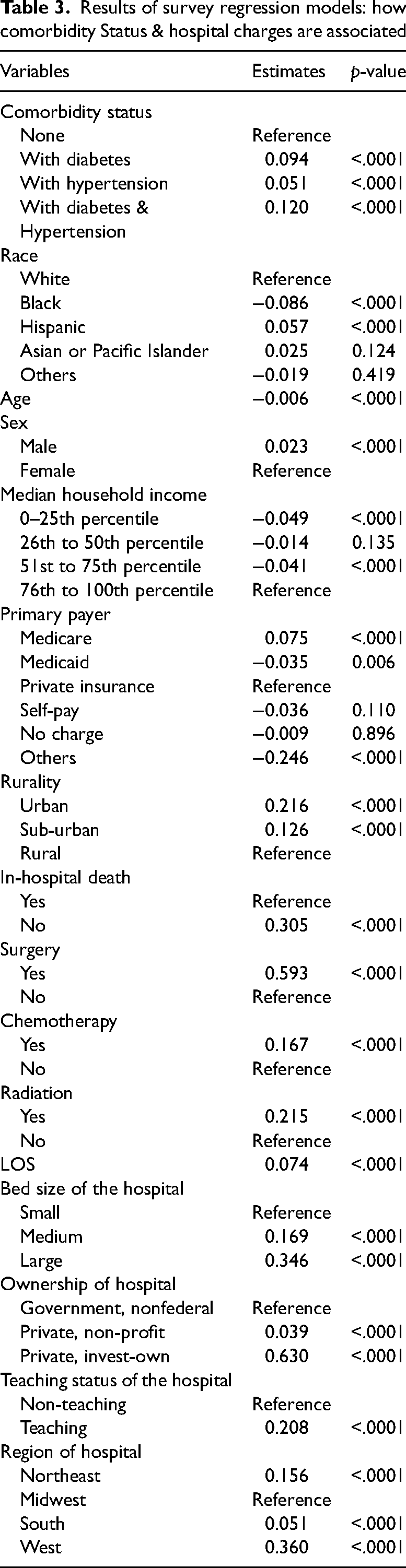
Table 3 demonstrates the associations of comorbidity status with hospital charges. We found a statistically significant difference in hospital charges by comorbidity status among hospitalized lung cancer patients. Results show that patients with lung cancer and comorbidities had 9.4% (diabetes), 5.1% (hypertension), and 12.0% (both) higher hospital charges than those without comorbidities. Factors like Hispanic ethnicity, male sex, higher income, Medicare, and urban residency were associated with higher hospital charges. Large, teaching, or privately owned hospitals and hospitals located in the Northeast and West were also associated with statistically significant higher hospital charges.
Results of survey regression models: how comorbidity Status & hospital charges are associated
Models with social factor sub-groups
Table 4 holds the results of the sub-group analysis. Again, patients with comorbidities were associated with higher hospital charges for most racial groups. Patients with both comorbidities had much higher hospital charges. This trend also holds in the sub-group models regardless of sex or primary payer.
Results of survey regression models: sub-groups analysis by social factors
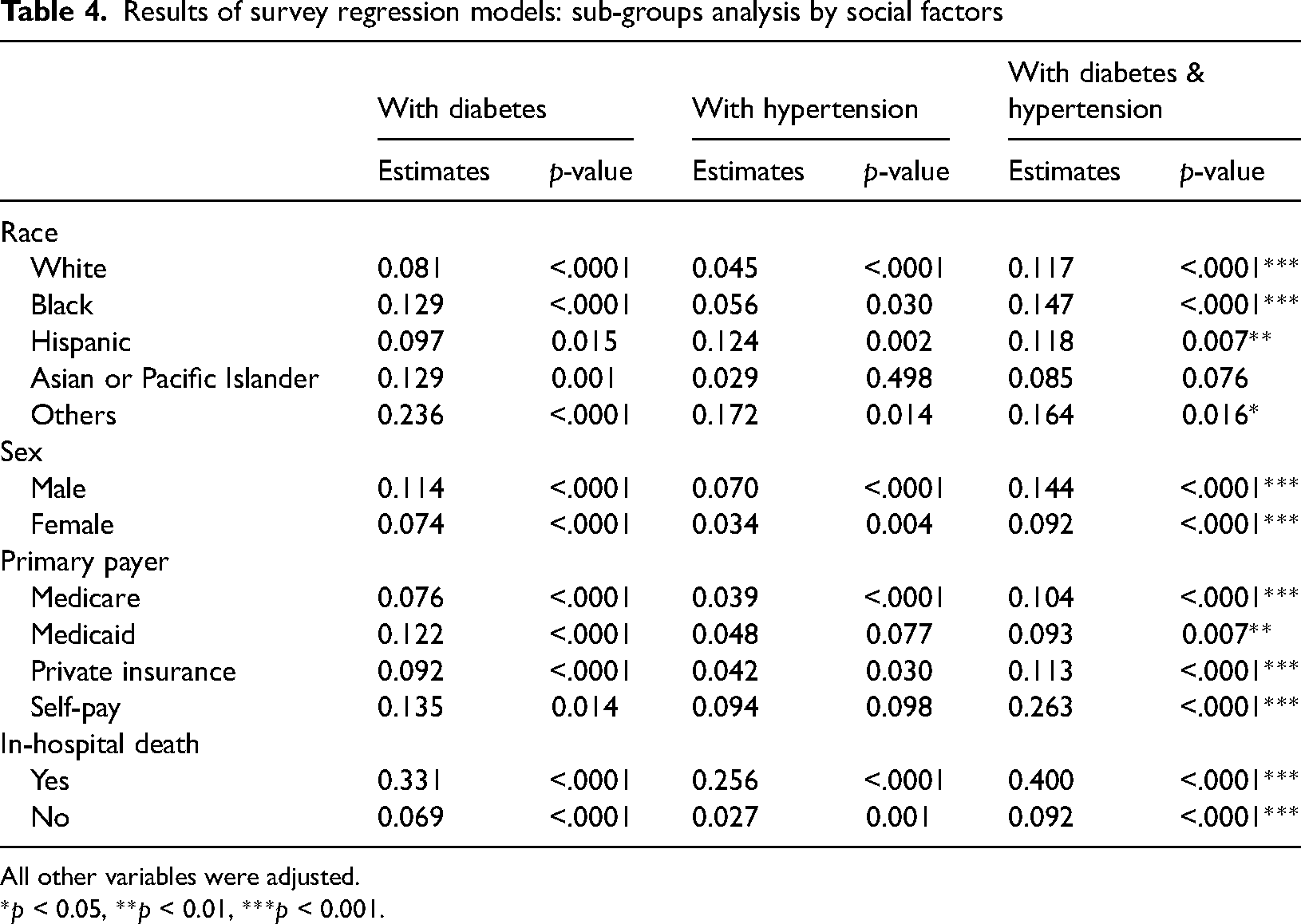
All other variables were adjusted.
*p < 0.05, **p < 0.01, ***p < 0.001.
Discussion
The study aimed to explore the association between diabetes and/or hypertension with racial disparities and healthcare charges among lung cancer patients. Furthermore, by analyzing sub-group, the present study identified the association between lung cancer patients’ individual factors (e.g. race, sex, primary payer, and in-hospital death) and differences in healthcare charges. Overall, the study's results demonstrated that comorbidities like diabetes and/or hypertension affected healthcare charges, and relevant healthcare disparities like race, sex, and primary payer were identified.
The survey regression models showed that comorbidity status is strongly associated with hospital charges for lung cancer patients. Specifically, patients with diabetes, hypertension, and both diabetes and hypertension had higher hospital charges than patients without comorbidities. The average hospital charge for patients with lung cancer increased from 2019 to 2020, but those charges were higher in patients with hypertension (13.35%) than those without comorbidities (3.46%). Previous literature demonstrated that comorbidities like diabetes and hypertension could complicate hospital stays, 6 and diabetes may negatively affect survival outcomes and lead to complications in patients with lung cancer. 15 It is understood that complications will lead to increased charges due to advanced care, but it is essential to recognize how the increased charge may marginalize specific populations more likely to have such comorbidities.
When accessing social factors, our findings for lung cancer patients with diabetes and/or hypertension coincide with the general prevalence of those comorbidities. Black and Asian or Pacific Islanders with diabetes were tied for the most increased charges for lung cancer patients with diabetes, and Black patients were also slightly more likely to be charged more if they had diabetes and hypertension compared to other races. Furthermore, Black patients are more likely to have uncontrolled hypertension and diabetes than White patients.7,8,27 Since Black patients are more likely to die from lung cancer, less likely to receive guideline treatment, and more likely to have uncontrolled hypertension and diabetes,21,22,27 the increased charges they face seem more unjust. Black households also have some of the lowest incomes in the US, 28 compounding their barriers to care. Minority patients also have some of the highest uninsurance rates compared to White patients, 28 further adding financial stress.
The type of insurance coverage was also found to be associated with hospital charges for lung cancer patients. Patients with Medicare had higher charges than those with private insurance, while those with Medicaid had lower charges than those with private insurance. Patients who self-pay also had higher expenses compared to those with private insurance. These findings suggest that insurance coverage is critical in determining the charge of healthcare for lung cancer patients. Other studies also indicate that overall charges for cancer treatment are higher for Medicare patients than for those with private insurance. 29 However, they found that uninsured patients had significantly lower charges and charges than those with private insurance, which contradicts to our findings. 29 Furthermore, patients who died in the hospital had higher charges than those who did not, while patients who received surgery, chemotherapy, and radiation had higher expenses than those who did not receive these treatments. Decreasing the costs of effective treatments for lung cancer patients with comorbidities as well as implementing more long-term recovery strategies could greatly decrease high healthcare charges facing lung cancer patients with comorbidities.
Another critical factor that was found to be associated with hospital charges was median household income. Compared to lung cancer patients with comorbidities in the 76th-100th percentile (earning over $82–86,000), patients who earned less in the 51st-75th percentile ($61–68,000) and 0–25th percentile ($1–49,999) were marginally but significantly charged less. In light of past research and our findings, the decreased charges associated with lower incomes may be due to reduced healthcare charges. Low-income patients have historically been unable to access care, especially compared to wealthy Americans. 30 Therefore, possible that more affluent patients are more likely to die in hospitals because they were there for care, while low-income patients are less likely to die in hospitals because they cannot afford care there.
This discrepancy is an opportunity for further research to characterize the barriers for low-income and uninsured patients. Our study found that low-income patients may be utilizing healthcare less, which indicates a barrier to care, but these findings don't necessarily correlate to uninsured patients. Out-of-pocket charges for outpatient chemotherapy tend to be higher for Medicare patients than those with private insurance and highest for uninsured patients. 31 Inpatient charges are also historically higher for uninsured patients than those with Medicare or private insurance. 31 Consequently, the higher charges reflected in our study may not be due to increased healthcare charges but to expensive out-of-pocket treatment, which can be a significant barrier. Considering the decreased charges found in low-income patients, our results reflect that low-income uninsured patients with lung cancer and comorbidities may utilize healthcare less but are charged more, and more concern can be needed to ensure equal access to treatment.
Limitations
Our study explored health disparities for patients with lung cancer and comorbidities like diabetes and hypertension to identify marginalized populations. However, there are some limitations to our results. First, we do not have information on disease severity, which could complicate cases and increase charges, limiting real-life interpretations. Second, the NIS dataset uses ICD-10 codes for lung cancer and the Elixhauser Comorbidity Measure from 2019 for diabetes and hypertension, which could restrict patient selection. Third, we do not have direct information on patient income by race to connect to hospital charges and can only generalize. Future research should focus on minority access to care and investigate if the patterns discussed here are mirrored in other cancer types.
Conclusion
The results of this study highlight the complex relationship between comorbidity status, social factors, and hospital charges for lung cancer patients. Black patients may be especially marginalized because of their historically lower income compared to white patients and the prevalence of uncontrolled comorbidities. Low-income and uninsured patients may access healthcare differently than their counterparts, and more significant reform is required to ensure healthcare equality. With the high mortality of lung cancer and prevalence of comorbidities in the US, it is crucial to understand how contributing factors can exacerbate financial conditions for patients and create an undue burden. Further research is needed to understand the underlying mechanisms contributing to these disparities and to develop strategies to reduce the charge of healthcare for lung cancer patients.
Footnotes
Acknowledgements
Not applicable.
Contributorship
JWC and SJK led the design and conception of the study, performed the data analysis, and wrote/reviewed the manuscript. JHP and MM contributed by writing a draft of the manuscript and reviewing and editing it. TP and MK provided the feedback for the manuscript. All authors read and approved the final manuscript.
Availability of data and material
All data generated or analyzed during this study are included in this published article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
We use secondary data, and all of the patient's data is encrypted and unable to be identified. This study was approved for a waiver by the Institutional Review Board at Soonchunhyang University (202203-SB-027).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the BK21 FOUR, (grant number 5199990914048).