
Abstract
Soluble cancer-related protein biomarker levels may be increased in subjects without findings at large bowel endoscopy performed due to symptoms associated with colorectal cancer. The present study focused on a possible association between increased biomarker levels in such subjects and subsequent development of malignant diseases. In a major study of 4,990 subjects undergoing large bowel endoscopy, 691 were without pathology and comorbidity. Plasma levels of TIMP-1, CEA, CA19-9, and YKL-40 were determined in samples collected just before endoscopy and compared with subsequent development of a malignant disease within a period of 7-8 years. The upper 90% limits of the reference levels of every single protein were used to differentiate between normal and increased levels. The levels were separated into three groups: 0, none of the biomarkers increased; 1, one biomarker increased; 2, two or more biomarkers increased. A total of 43 subjects developed a primary malignant disease in the observation period. Univariatly, increase of all four biomarkers was significantly associated with subsequent development of a malignant disease. A multivariate analysis showed that increased biomarker levels were associated with subsequent development of a malignant disease (P = 0.002). The cumulative risk of developing malignant disease within the first 5 years after endoscopy was group 0, 3.3%; group 1, 5.8%; group 2, 7.8%. It is concluded that increased levels of plasma TIMP-1, CEA, CA19-9, and serum YKL-40 at large bowel endoscopy without findings may be associated with an increased risk of developing a subsequent malignant disease.
Introduction
Screening leads to improved survival among patients with colorectal cancer (CRC).1–3 The statement is supported by the results of population screening for CRC showing more individuals being diagnosed with early-stage disease,4,5 which translates into improved survival compared to CRC patients not diagnosed by screening.6,7 In addition, screening may lead to reduction of CRC incidence 6 due to detection of patients with high-risk adenomas. Such patients are enrolled in programs with frequent follow-up colonoscopies, which reduce the number of patients, who develop CRC. 8
The compliance of screening procedures is far from sufficient, with ranges of 40%–60%. This leads to clinical sensitivities in ranges of 30%–45%, 3 meaning that >50% of those who may have a neoplastic large bowel lesion are not detected. Therefore, current research focuses on developing screening concepts that are accurate and acceptable by the screening population. Such concepts include blood-based procedures,3,9,10 and compliance rates > 90% for blood testing have been observed among subjects referred to large bowel endoscopy due to symptoms of CRC. 11 This supports recent results indicating that screenees may prefer blood-based compared with feces-based screening concepts. 12
Various challenges remain to be solved in the development of blood-based biomarkers for cancer screening. Hitherto, most results are based on plasma or serum proteins that also identify subjects with various benign diseases.3,13 Such results are classified as false positives and contribute to lowering the specificity of the tests. However, increased levels of cancer-related protein biomarkers are identified even among healthy subjects of the general population, and it has been argued that this phenomenon may identify subjects with increased risk of developing a malignant disease over the following years. 14 In a population-based study performed in 2004–2005, blood samples were collected before large bowel endoscopy of subjects referred due to symptoms of CRC or adherence to a hereditary nonpolyposis colorectal cancer (HNPCC) surveillance program. 11 Subsequently, the protein biomarkers plasma TIMP-1, CEA, CA19-9, and serum YKL-40 were determined.11,13–16 Some subjects without any malignant or benign large bowel findings had increased levels of some or all of the four protein biomarkers. Therefore, the aim of the present study was to evaluate a possible association between increased biomarker levels in subjects, without findings at large bowel endoscopy and subsequent development of malignant diseases.
Methods
This present study is based on a prospective, population-based study performed in 2004–2005, which included 4,509 subjects with various symptoms of CRC and 481 subjects adhering to a HNPCC surveillance program. The inclusion and exclusion criteria of the subjects have been presented previously. 11 Comorbidities were recorded for all subjects. Symptoms or adherence to HNPCC surveillance programs guided whether a subject was offered sigmoidoscopy or colonoscopy. Subjects without findings of colorectal pathology at sigmoidoscopy, but with persisting symptoms, were offered subsequent colonoscopy. Finally, subjects with persisting symptoms, without findings at sigmoidoscopy plus colonoscopy or colonoscopy alone, were offered additional examinations including ultrasound (US), computerized axial tomography scan (CAT), or magnetic resonance imaging (MRI).
The study was approved by the Regional Ethics Committee of Copenhagen and Frederiksberg no. H-KF-01-080/03 and The Danish Data Protection Agency no. 2003-41-3312, and the requirements of the Helsinki II declaration were fulfilled. Subjects gave their written, informed consent to participate in the research. Blood samples for serum, plasma, and buffy coats were collected from all subjects just before endoscopy and were handled and subsequently frozen at –80°C under electronic 24/7 surveillance, according to a validated standard operative procedure. The study was finalized on 31 December, 2005, and the audits were performed on-site and electronically via existing databases. TIMP-1, CEA, and CA19-9 were determined in ethylenediaminetetraacetic acid (EDTA) plasma using the Abbott ARCHITECT® i2000 automated immunoassay system. 11 Serum YKL-40 levels were determined by a commercial enzyme-linked immunosorbent assay (ELISA) platform, with a detection limit 10 ng/mL and intraassay coefficient of variation (CV) of 5% and interassay CV of <6%. 14
In total, 1,176 subjects had no pathology at the endoscopy, but 388 of these subjects had self-reported comorbidity or had concurrent diseases and/or were taking prescribed medication. Therefore, only 788 subjects were categorized as having no findings plus no comorbidity. However, the subsequent audit disclosed that 96 subjects were registered with previous or concurrent malignancy or a variety of diseases known to be associated with increased plasma biomarker levels. 11 Therefore, the final cohort of the present study only comprised 691 subjects, including 174 from the HNPCC surveillance programs. Using 31 December, 2012 as the cut-point, the subjects were identified in the databases, and the development of any malignant disease (except for basocellular and/or planocellular skin cancer) during the observation period of 7–8 years was recorded using the ICD10 codes. Some subjects had developed more than one malignant disease, but only the very first diagnosed disease was included in the study. In addition, we recorded the elapsed time (ET) within which a subject developed the malignant disease.
Statistics
Descriptive statistics were presented by the median, minimum, maximum, and quartiles for continuous data. The Spearman rank correlation was used as a measure of association, and tests for comparing marker levels between strata were done using the Wilcoxon rank sum test. Comparisons between strata with adjustment for age and gender were performed using a linear model with the biomarker levels log transformed. The latter results were presented by the relative differences (ratio) with 95% confidence intervals (CI).
The ET to development of a malignant disease and the association to the biomarker levels at the endoscopy were analyzed with death as a competing risk. 17 Each biomarker level has been defined as normal or elevated based on the 90th percentile of age and gender-adjusted reference intervals. The reference intervals for each biomarker were constructed by regressing the log of each biomarker on age and gender using a cohort of 400 subjects referred to colonoscopy who were without any findings, without comorbidity, and without medication. Univariate analyses of time to diagnosis of primary cancer have been done for each biomarker in addition to the association for subjects with no elevated (group 0), one elevated (group 1), or two or more (group 2) elevated biomarkers. All subsequent primary cancers recorded in the observation period were included, but the cumulative incidence rate was calculated within 5 years. P-values less than 5% were considered significant.
Results
The study cohort included 376 females and 316 males, and the median age at endoscopy was 47 (21–91) years for women and 45 (21–92) for men. In total, 43 of the 691 subjects developed a malignant disease within the observation period. The mean ET from endoscopy to diagnosis was 39 (1–99) months.
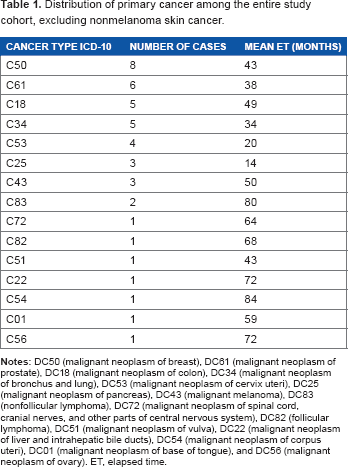
Distribution of primary cancer among the entire study cohort, excluding nonmelanoma skin cancer.
Distribution of subjects with normal and increased levels of the four specific biomarkers plasma TIMP-1, plasma CEA, plasma CA19-9, and serum YKL-40.

Categorizing the subjects with no elevated biomarker levels (group 0), 1 elevated level (group 1), or 2 or more elevated levels (group 2) showed that the cumulative risk of developing a primary malignant disease within 5 years after endoscopy was: group 0: 3.3% (2.0%–5.2%); group 1: 5.8% (2.9%–10.3%); group 2: 7.8% (2.5%–17.3%) (Fig. 1). Pairwise comparisons demonstrated a significant difference between those with no elevated markers and with one or two elevated markers, P = 0.024 and P = 0.0009, respectively. However, the difference between those with one or two elevated markers was not significant, P = 0.20.
Six patients had a nonbowel malignant disease diagnosed within the first 6 months after the primary endoscopy. An analysis excluding these patients showed that the combined biomarkers still were significantly associated with the subsequent risk of developing a primary malignant disease (P = 0.0021).
Discussion
The results of the present study showed that increased levels of one or more of four cancer-related soluble protein biomarkers at large bowel endoscopy without any findings + no comorbidity were associated with a minor, significant risk of subsequently developing a primary malignant disease.
The included subjects were referred to endoscopy due to symptoms or due to the fact that they were HNPCC family members. Therefore, all included subjects were at-risk subjects for colorectal neoplasia including malignancies, and the frequency of neoplastic findings is relatively high among at risk subjects.
11
However, most of the symptoms were caused by benign findings, for example, diverticula, and more than 50% of the subjects did not have any bowel pathology at all.
11
Some of the subjects were referred to endoscopy due to uncharacteristic symptoms that might be caused by a bowel lesion, and in most of these cases, the cause of the symptoms was never revealed.
The figure shows the cumulative incidence of any new cancer from the date of primary large bowel endoscopy. The strata are patients without elevated soluble biomarker levels (CEA, TIMP-1, CA19-9, and YKL-40) (black), patients with one elevated biomarker level (blue) and patients with at least two elevated biomarker levels (red).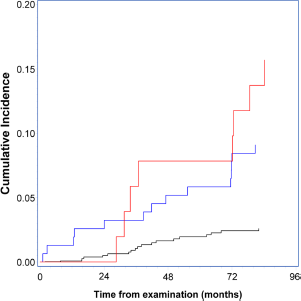
Studies with focus on developing blood-based CRC screening concepts have shown that soluble biomarkers may also be increased among subjects that have no bowel findings but various comorbidities; 11 even subjects without findings and without any comorbidity may have increased levels of soluble protein biomarkers. It has been considered that a rise in such biomarker levels may be the first indication of establishment and growth of neoplastic lesions. Although it could not be shown for CRC, 18 results on elevated levels of C-reactive protein appear to identify subjects at risk of developing a malignant disease.19,20 Combinations of certain elevated protein biomarkers may add to the risk profile, 14 as confirmed by the results of the present study.
Even though the study cohort was limited to 691 subjects, 43 developed primary malignancies, including five with CRC. Among these five subjects, two underwent sigmoidoscopy and developed right-sided colorectal cancer (CC). It is considered that the malignant lesions were not missed at that time because the diagnoses were established 37 and 84 months later, respectively. It cannot be documented, however, whether these two subjects had adenoma formation in the right colon at the time of sigmoidoscopy.
It is important to note that various primary malignancies that developed in the study period were indeed related to increased biomarker levels. Therefore, a couple of questions must be answered. First, are the results achieved by chance? The study population is limited and, in particular, the age distribution of the included subjects is far from similar to the distribution among subjects with symptoms of CRC, where the median age is 70 years. The number of HNPCC family members reduced the median age to 47 and 45 for women and men, respectively, where most age-related malignancies do not develop. Therefore, subsequent sufficiently sized studies with the correct age distribution may help to clarify that question. It should be considered, however, that the median age at diagnosis of primary malignant disease in this study was 56 years, with an interquartile range of only 50–65 years. This underlines that the developed malignancies were not associated with high age. Second, does elevated biomarker levels indicate subsequent examination if endoscopy shows no findings? If subsequent research confirms the association between increased biomarker levels in subjects without endoscopic findings and subsequent risk of developing malignant diseases, such subjects might be candidates for frequent examinations in order to detect primary malignant diseases, including extracolonic diseases at an early stage. The number of subjects with increased protein biomarker levels in the present study is relatively high, with 205 of the 691 subjects having increased levels of one or more biomarkers. Based on these numbers, specific follow-up to identify early malignant lesions cannot be recommended at present. It is important, however, to evaluate the present findings in subsequent sufficiently sized studies to verify the value of soluble biomarkers in prediction of the risk of subsequent malignancy. If confirmed clinically, such subjects might be candidates for frequent follow-up. It is concluded that increased levels of certain cancer-related soluble biomarkers at primary bowel endoscopy without findings and without comorbidity may be associated with risk of developing a subsequent primary malignant disease. However, the study size only allows for raising hypotheses, which should be tested in sufficiently sized studies of subjects at similar age distribution as CRC-risk subjects.
Author Contributions
Conceived and designed the experiments: TSK, TBP, LNJ, JO, HBR, KTN, SL, GD, BD, JSJ, IJC, NB, HJN. Analyzed data: TSK, TBP, IJC, GD, BD, JSJ, IJC, HJN. Wrote the first draft of the manuscript: TSK, HJN. Contributed to writing of the manuscript: TSK, TBP, IJC, HJN. Agree with manuscript results and conclusions: TSK, TBP, LNJ, JO, HBR, KTN, SL, GD, BD, JSJ, IJC, NB, HJN. Jointly developed the structure and arguments for the paper: TSK, TBP, LNJ, JO, HBR, KTN, SL, GD, BD, JSJ, IJC, NB, HJN. Made critical revisions and approved final version: TSK, TBP, LNJ, JO, HBR, KTN, SL, GD, BD, JSJ, IJC, NB, HJN. All authors reviewed and approved the final version.
Footnotes
Acknowledgments
The research nurses, secretaries and technicians at the participating hospital departments and laboratories are thanked for their skillful work.