
Abstract
Purpose:
The aim of this study was to evaluate the clinicopathological significance and prognostic role of programmed death-1 ligand 2 (PD-L2) expression in colorectal cancer according to intratumoral components.
Methods:
We used immunohistochemical analysis to investigate the impact of PD-L2 expression on clinicopathological characteristics and survival in 264 human colorectal cancer tissues. We also evaluated the correlation between PD-L2 expression and PD-L1 expression.
Results:
PD-L2 was expressed in 17.4% of the tumors (T-PD-L2) and in 19.3% of the immune cells (I-PD-L2) of the 264 CRC tissues. I-PD-L2 expression was significantly correlated with favorable tumor behaviors, including lower pathologic tumor stage, less lymph node metastasis, less distant metastasis, and lower pathologic tumor node metastasis stage. There was no significant correlation between I-PD-L2 expression and T-PD-L2 expression (P = 0.091). However, I-PD-L2 expression was correlated with PD-L1 expression in the immune cells (P < 0.001). There was also a significant correlation between high Immunoscore and I-PD-L2, but not T-PD-L2 (P < 0.001 and P = 0.190, respectively). The prognosis was better for patients who expressed I-PD-L2 than for patients who did not. In patients who expressed I-PD-L2, there was a significant difference in the survival rate between subgroups according to the presence or absence of T-PD-L2 expression.
Conclusions:
Our results suggest that I-PD-L2 expression is significantly correlated with favorable tumor behaviors and better survival rates. There is also a significant correlation between PD-L2 expression and PD-L1 expression in immune cells.
Introduction
Programmed death-1 ligand 2 (PD-L2) is a second ligand for programmed death 1 (PD-1). 1 PD-L1 is expressed in various immune and non-immune cells, including T and B cells, dendritic cells, and macrophages. Basically, PD-L2 is expressed in dendritic cells and macrophages within secondary and tertiary lymphoid organs. 2 However, PD-L2 can be induced by other immune and non-immune cells in various tissue microenvironments.1-6 PD-Ls, including PD-L2, are sometimes expressed in tumor cells of various malignant tumors. The tumor cells of malignant tumors can acquire the ability to evade the immune response via PD-L expression. 7 Interaction between PD-1 and PD-L2 may be involved in the inhibition of T cell proliferation and the downregulation of T cell responses. 1 In malignant tumors, the expression of PD-Ls can be important in predicting the response to PD-1 axis-targeted therapy. Because PD-L2 has not been studied as intensively as PD-L1, the clinicopathological significance of PD-L2 expression and its expression pattern in various intratumoral components have not been fully elucidated. If PD-L2 expression is correlated with PD-L1 expression, it may be possible to predict the roles of PD-L2 from previous reports. However, such a correlation has not yet been confirmed in colorectal cancer (CRC).3,8 The authors of a previous study reported that PD-L1 and PD-L2 were expressed in cultured fibroblasts from human non-small cell lung cancer, which are stromal components of the malignant tumors. 9 Therefore, an investigation of PD-L2 expression in tumors and their stomal components will be necessary.
The aim of the present study was to elucidate the clinicopathological significance and prognostic implications of PD-L2 expression in CRC according to intratumoral components, tumor cells, and immune cells. We investigated the correlation between PD-L2 expression and PD-L1 expression based on tumor cells and immune cells. We also evaluated the impact of tumor-infiltrating lymphocytes (TILs) on PD-L2 expression by determining the Immunoscore.
Materials and methods
Patients and tissue array methods
We examined the files of 264 patients who had undergone surgical resection for CRC at the Eulji University Medical Center, between 1 January 2001 and 31 December 2010. We reviewed medical charts, pathological records, and glass slides to assess the following clinicopathological characteristics: age; sex; tumor size; tumor location; tumor differentiation; vascular, lymphatic, and perineural invasion; depth of tumor; lymph node metastasis; metastatic lymph node ratio; distant metastasis; and pathologic tumor node metastasis (pTNM) stage. We evaluated these cases according to the 8th Edition of the American Joint Cancer Committee TNM classifications. 10 This protocol was reviewed and approved by the Institutional Review Board of Eulji University Hospital. We prepared five array blocks containing a total of 264 resected CRC tissue cores obtained from the patients. Briefly, we took tissue cores (2 mm in diameter) from individual paraffin-embedded CRC tissues (donor blocks) using a trephine, and arranged them in recipient paraffin blocks, as previously described. 11 The staining results of the various intratumoral areas in these tissue-array blocks were highly consistent. We chose a core from each case for analysis. An adequate case was defined as a tumor occupying more than 10% of the core area. Each block contained internal controls consisting of non-neoplastic colon tissue. Clinical outcomes were followed from the date of surgery to the date of death, resulting in a follow-up period ranging from 0 to 60 months.
Immunohistochemical staining and evaluation
We cut 4-μm-thick sections for immunohistochemical analysis from each tissue-array block, then deparaffinized and dehydrated them. For antigen retrieval, we treated the sections with 0.01 M citrate buffer (pH 6.0) for 5 min in a microwave oven, then treated them with 3% H2O2 to quench endogenous peroxidase. We treated the sections with normal serum from the host animal that produced the secondary antibody to block non-specific binding. We then incubated the sections with anti-PD-L1 antibody (clone SP263; Ventana Medical Systems, Inc., Tucson, Arizona, USA), anti-PD-L2 antibody (Cell Signaling Technology, Danvers, Massachusetts, USA), anti-CD3 (Leica Biosystems, Newcastle Upon Tyne, UK), and anti-CD8 (Leica Biosystems). We carried out immunohistochemical staining following a compact polymer method using a VENTANA BenchMark XT autostainer (Ventana Medical Systems, Inc.). We prepared the samples for examination by treating them with an OptiView universal 3,3′-diaminobenzidine kit (Ventana Medical Systems, Inc.). We used a negative control stain without a primary antibody to confirm the reaction specificity of each antibody. We lightly counterstained all the immunostained sections with Mayer’s hematoxylin. The immunohistochemical results for PD-L1 were evaluated by two independent researchers. According to the results of the immunohistochemical analysis, both PD-L1 and PD-L2 were present in the cell membrane. The positivity for PD-L1 and PD-L2 was defined as membranous expression of any intensity in ⩾10% of tumor or immune cells.
Determination of Immunoscore
We scanned all the immunohistochemically stained slides for CD3 and CD8 using a Pannoramic MIDI II slide scanner (3DHISTECH, Budapest, Hungary). We captured images from two regions—the core of the tumor and the invasive margin—using CaseViewer 2.0 software (3DHISTECH). CD3- and CD8-immunoreactive lymphocytes were identified from the captured images using NIH Image Analysis software (version 1.6.0; National Institutes of Health, Bethesda, Maryland, USA) after setting a consistent intensity threshold. The CD3- and CD8-immunoreactive lymphocytes were expressed as pixels in each region. In the present study, the cut-off was determined by the median value of pixels in each region. We classified the patients into two groups according to the cut-off: high (score 1) or low (score 0). Immunoscores are defined by the summation of the scores of two regions, and are divided into high (IS 3–4) and low (IS 0–2) scores. 12
Statistical analysis
We carried out statistical analyses using SPSS version 22.0 software (IBM Co., Chicago, Illinois, USA). The significance of the correlation between PD-L2 expression and the clinicopathological characteristics was determined using either the χ2 test or Fisher’s exact test (two-sided). The comparisons between PD-L2 expression and age, tumor size, or metastatic lymph node ratio were analyzed using the two-tailed Student’s t test. Survival curves were estimated using the Kaplan–Meier product-limit method, and differences between the survival curves were determined to be significant based on the log-rank test. In addition, for the multivariate analysis, a Cox-regression test was conducted. The results were considered statistically significant for P < 0.05.
Results
Correlation between PD-L2 expression and clinicopathological characteristics
We investigated PD-L2 expression in both tumor cells and immune cells. Representative images of PD-L2 expression in the tumor cells (T-PD-L2) and immune cells (I-PD-L2) in the CRC tissue are shown in Figure 1. PD-L2 was expressed in 17.4% of the tumors (T-PD-L2) and in 19.3% of the immune cells (I-PD-L2) of the 264 CRC tissues. I-PD-L2 expression was significantly correlated with smaller tumor size, tumor differentiation, lower pathologic tumor (pT) stage, and lower pTNM stage (Table 1). There were also significant correlations between I-PD-L2 expression and less lymph node metastasis and lower metastatic lymph node ratio (P = 0.008 and P = 0.032, respectively). However, there was no significant correlation between tumor (T)-PD-L2 expression and clinicopathological characteristics. Immune cells (I)-PD-L2 expression was not significantly correlated with T-PD-L2 expression (P = 0.091; Table 2).
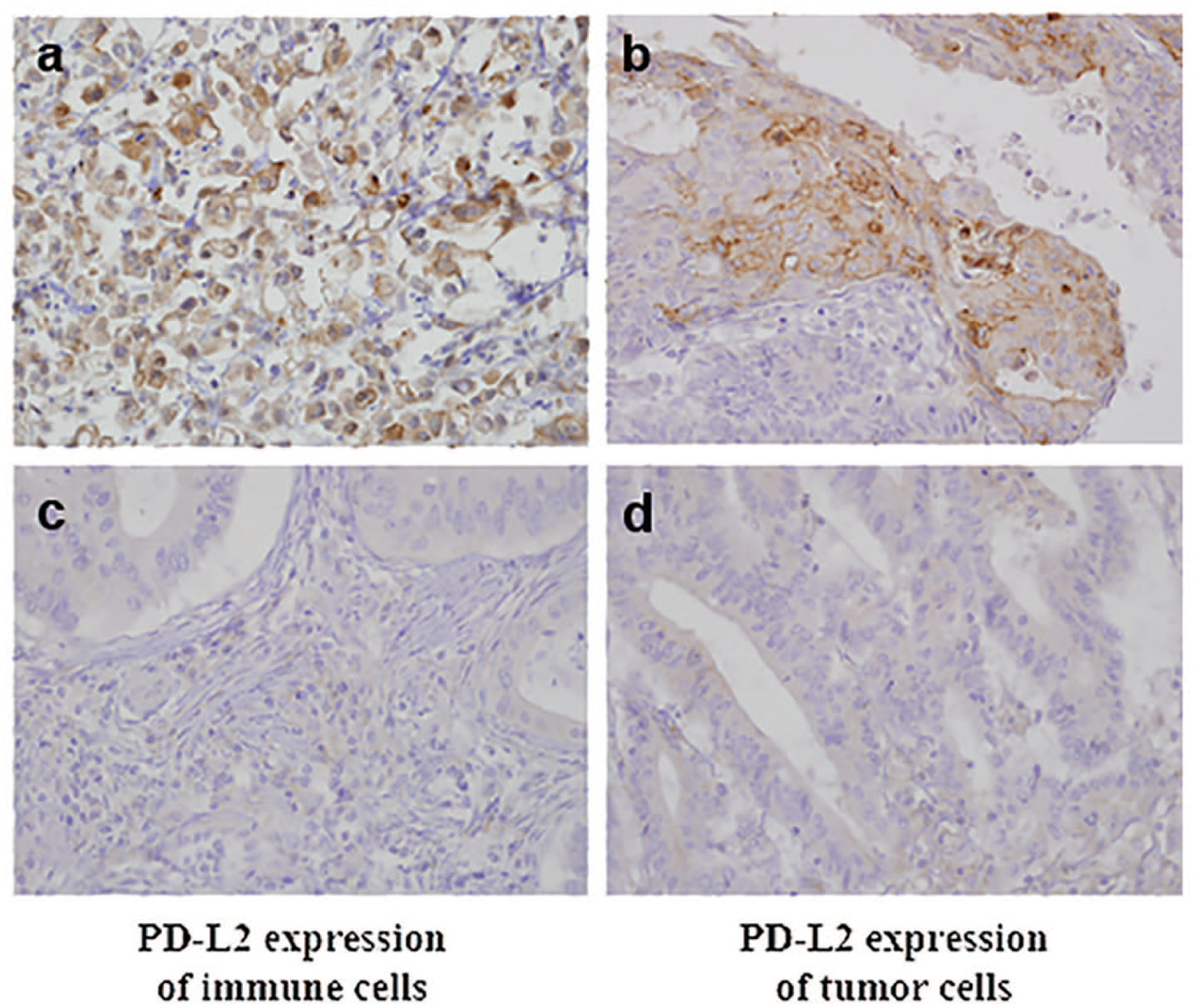
Representative images showing PD-L2 expressions of tumor (a) and (c), and immune cells (b) and (d) in colorectal cancer (×400).
The correlation between Immunoscore and clinicopathological parameters in colorectal cancers.
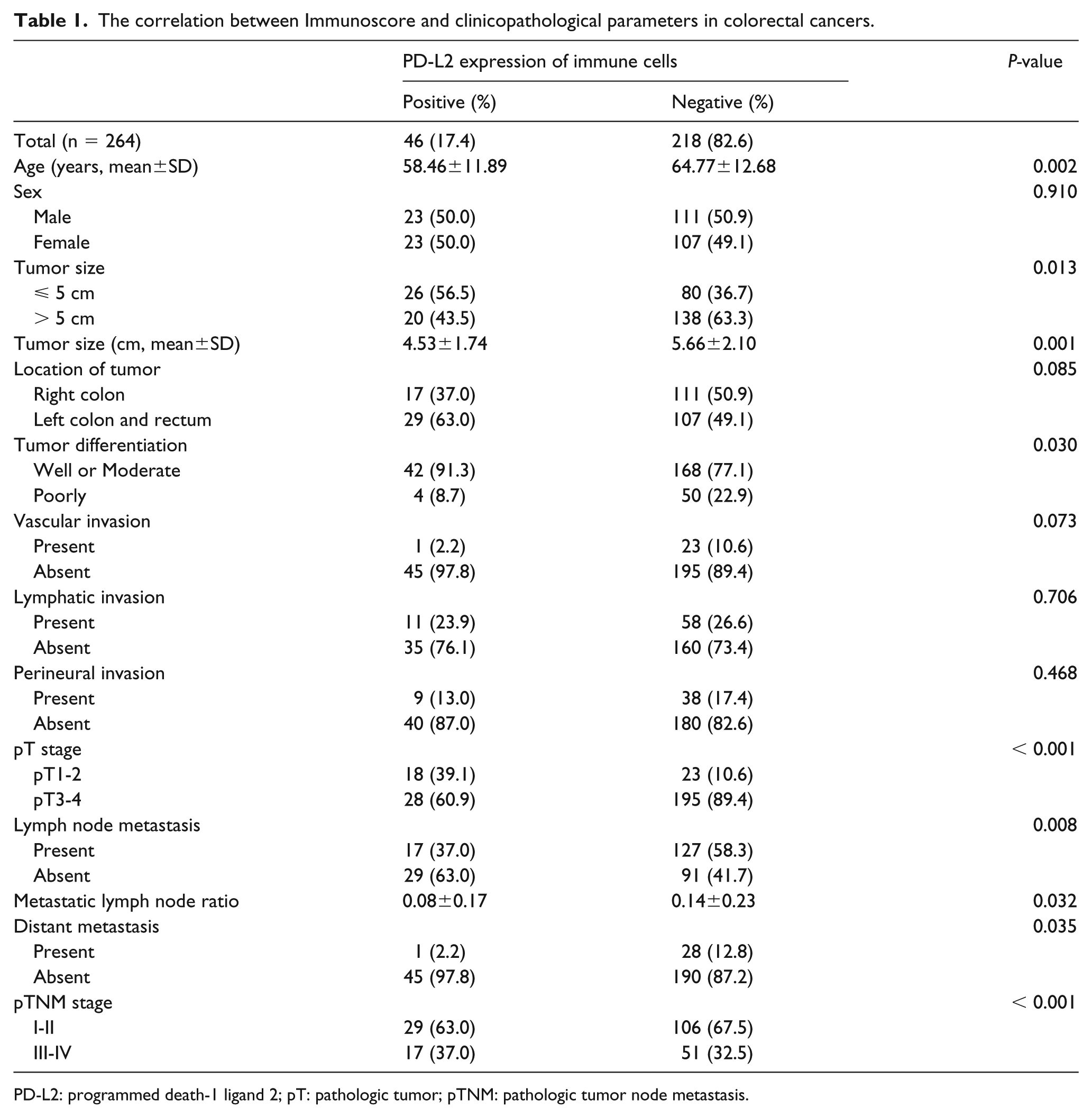
PD-L2: programmed death-1 ligand 2; pT: pathologic tumor; pTNM: pathologic tumor node metastasis.
The correlation between PD-L2 and PD-L1 expressions in colorectal cancers.
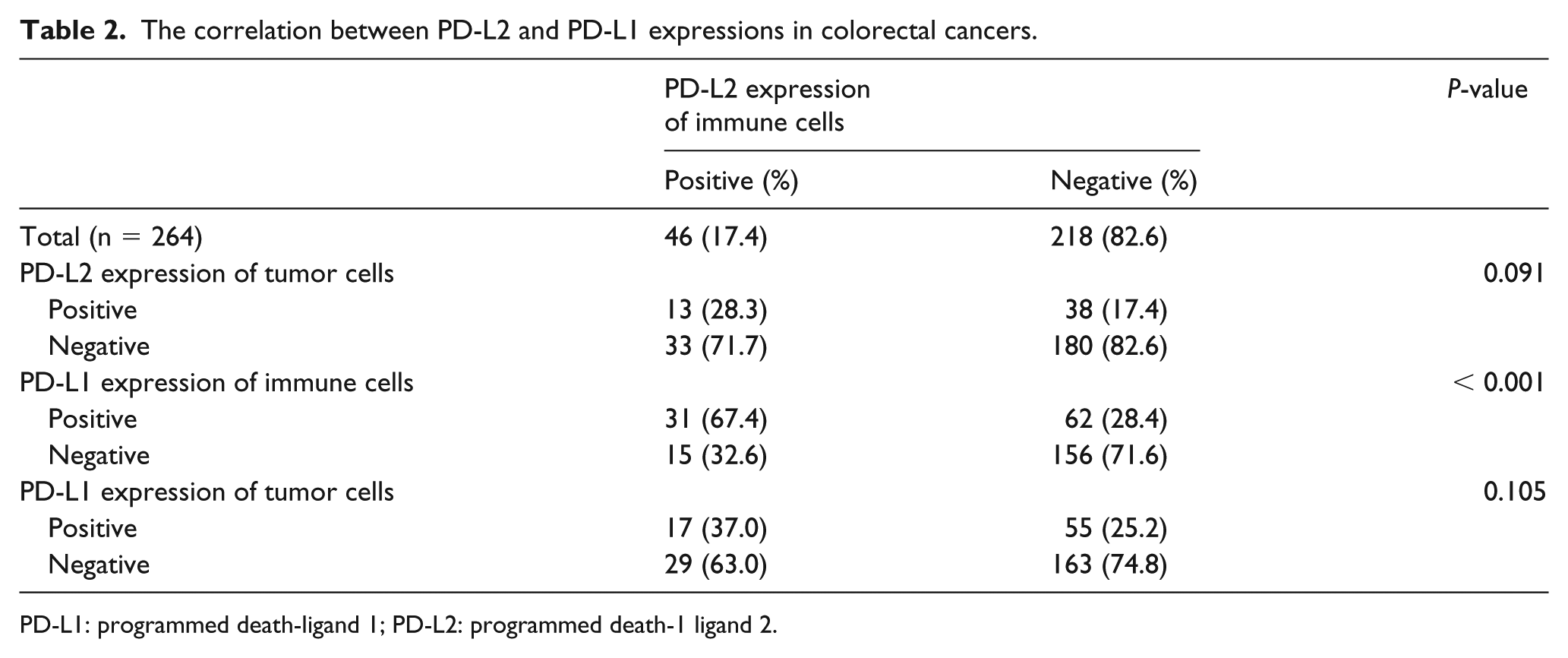
PD-L1: programmed death-ligand 1; PD-L2: programmed death-1 ligand 2.
Correlation between PD-L2 expression and PD-L1 expression and tumor-infiltrating lymphocytes
We investigated the correlations between PD-L2 expression and PD-L1 expression in the tumor cells and immune cells. I-PD-L2 expression was significantly correlated with PD-L1 expression in the immune cells (P < 0.001; Table 3). However, there was no significant correlation between I-PD-L2 expression and T-PD-L1 expression (P = 0.105). T-PD-L2 expression was not significantly correlated with PD-L1 expression in the tumor cells or the immune cells (P = 0.464 and P = 0.991, respectively). To evaluate the impact of TILs, we determined Immunoscores by immunohistochemical staining for CD3 and CD8. The CRC patients with high Immunoscores had higher rates of I-PD-L2 expression than those with low Immunoscores (P < 0.001). T-PD-L2 expression did not differ significantly between the high- and low-Immunoscore subgroups (P = 0.190).
The correlation between PD-L2 expression and tumor-infiltrating lymphocytes in colorectal cancers.
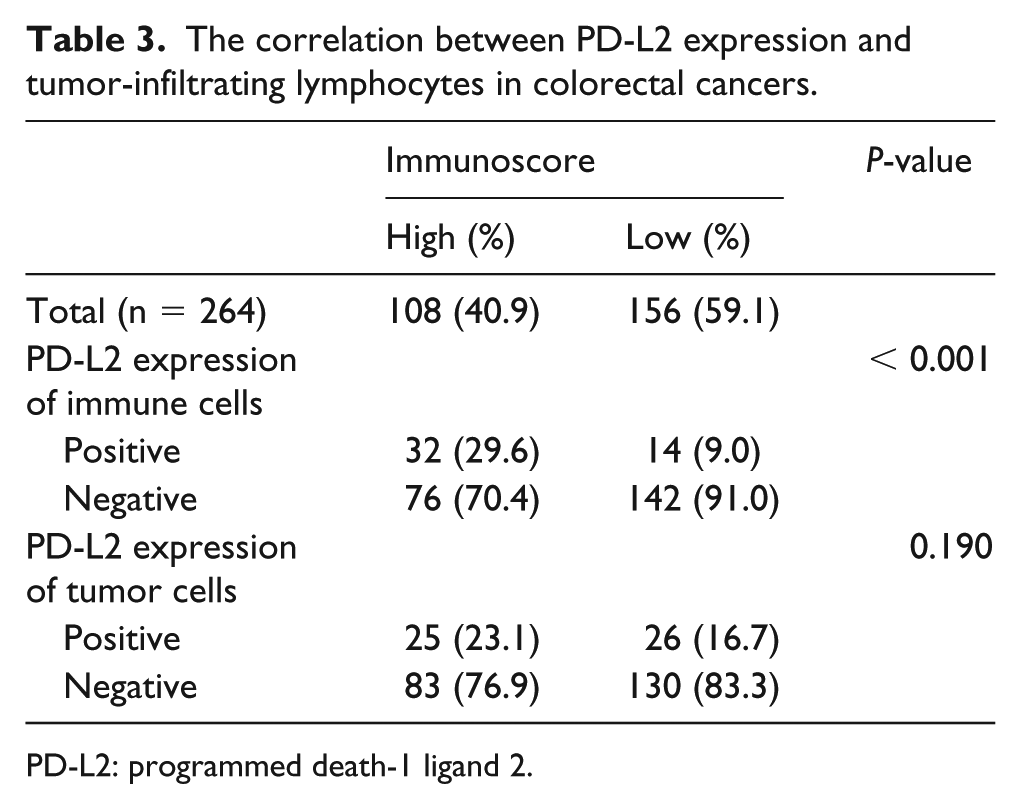
PD-L2: programmed death-1 ligand 2.
Correlation between PD-L2 expression and survival
CRC patients who expressed I-PD-L2 had better prognoses than CRC patients who did not (P < 0.001; Figure 2(a)). In addition, in the Cox-regression test, I-PD-L2 expression was an independent predictor of better prognosis in CRC patients (P = 0.001). There was a significant correlation between T-PD-L2 expression and better overall survival (P = 0.002). In addition, the prognostic roles of I-PD-L2 expression in tumor stage subgroups were analyzed. Tumor stage subgroups were divided into low (Stage I and II) and high (Stage III and IV) stages. In the present study, patients with I-PD-L2 expression had good prognosis in both low and high pTNM stages (P < 0.001 and P = 0.001, respectively; Figure 2(b) and (c)).
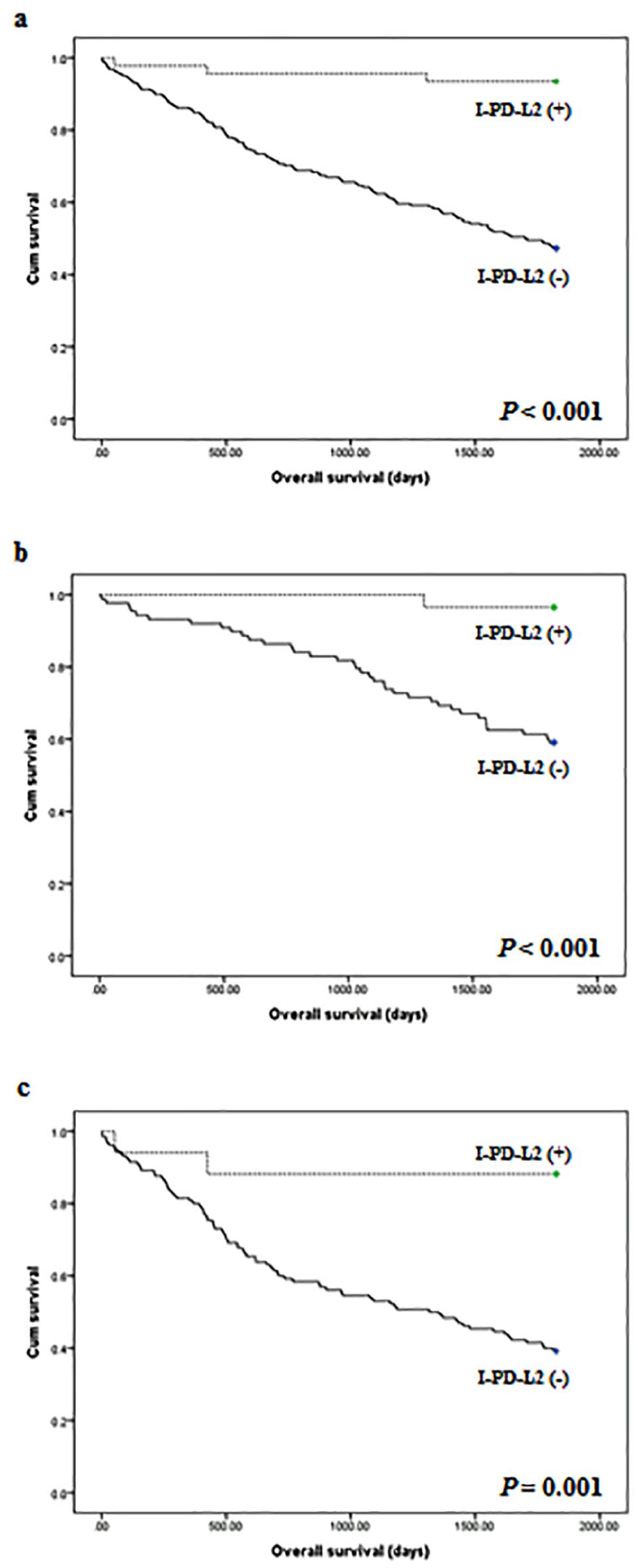
Kaplan–Meier curves for patient survival according to PD-L2 expression. (a) Survival according to PD-L2 expression of immune cells in overall cases. (b) Survival according to PD-L2 expression of immune cells in low tumor stages (I or II). (c) Survival according to PD-L2 expression of immune cells in low tumor stages (III or IV).
Discussion
PD-L2 is as a second ligand of PD-1.1,3 However, its expression patterns and prognostic implications are not fully understood in CRC. In the present study, we attempted to elucidate the clinicopathological significance and prognostic role of PD-L2. We also investigated the correlation between PD-L2 expression and PD-L1 expression by immunohistochemical analysis using human CRC tissues. We found that I-PD-L2 expression was significantly correlated with I-PD-L1 expression and better prognosis. We also discovered that subgrouping based on I-PD-L2 expression and T-PD-L2 expression could be useful for the differentiation of prognoses in CRC.
In the current study, we investigated PD-L2 expression separately in tumor cells and immune cells. As described above, the rates of I-PD-L2 expression and T-PD-L2 expression were 17.4% and 19.3%, respectively. In a previous study, PD-L2 expression was found in at least 40% of stromal cells in renal cell carcinoma, melanoma, gastric cancer, non-small cell lung cancer, triple-negative breast cancer, bladder cancer, and head and neck squamous cell carcinoma (HNSCC). 3 However, T-PD-L2 expression varied by up to 60% according to tumor type. 3 Masugi et al. 2 reported PD-L2 expression in stromal cells, including immune cells, in 78% of the CRC patients studied, which was not significantly correlated with any clinicopathological parameters, regardless of the number of positive cells. These reports had no detailed information on I-PD-L2 expression patterns in the stromal components.2,3 Previous studies reported that the expressed rates of PD-L2 were varied.2,3 Yearly et al. 3 reported that the rates of PD-L2 expression showed at least 40% of stromal cells, including immune cells. However, they were not investigated the PD-L2 expression in CRCs. 3 Also, Masugi et al. 2 reported that I-PD-L2 expression was expressed in 27% of CRCs. In these studies, evaluation criteria for PD-L2 expression used 0%, unlike our study.2,3 Because our study used 10% as evaluation criteria, the previous studies could be showed higher positive rates of PD-L2 expression compared to our results. Also, there was discrepancy for the clinicopathological significance of I-PD-L2 expressions between studies. To confirm the clinicopathological significance and prognostic implications of PD-L2 expression, it should be evaluated in immune cells. In the present study, I-PD-L2 was significantly correlated with smaller tumor size, tumor differentiation, lower pT stage, less lymph node metastasis, less distant metastasis, and lower pTNM stage. There was no significant correlation between T-PD-L2 expression and any of the clinicopathological characteristics.
PD-L1 expression is evaluated to predict the therapeutic effect of immunotherapy in daily practice. Moreover, PD-L2 expression is associated with the response to pembrolizumab therapy. 3 The objective response rates (ORRs) of the CRC patients with and without PD-L2 expression were 26.6% (95% confidence interval (CI) 18.0, 36.7%) and 9.6% (95% CI 3.2, 21.0%), respectively. 3 However, PD-L2 expression was assessed without distinguishing between tumor cells and immune cells. 3 A detailed investigation of the relationship between PD-L2 expression in intratumoral components and immunotherapeutic effect is required. In renal cell carcinoma, melanoma, gastric cancer, and triple-negative breast cancer, the rate of PD-L2 expression in stromal cells is lower than in tumor cells. 3 With regard to CRC, there is no detailed information on PD-L2 expression in each intratumoral component. However, in the present study, there was no significant correlation between I-PD-L2 expression and T-PD-L2 expression. Only 13 of the 264 CRC patients (4.9%) expressed both I-PD-L2 and T-PD-L2. Of the 46 CRC patients who expressed I-PD-L2, 28.3% expressed it in both tumor cells and immune cells.
The authors of a previous study reported that PD-L2 expression was significantly correlated with PD-L1 expression in various malignant tumors, including melanoma, non-small cell lung cancer, HNSCC, bladder cancer, and gastric cancer. 3 However, in that study the correlation was determined by gathering data on PD-L2 expression in stromal and tumor cells. In the present study, we divided PD-L2 expression into I-PD-L2 expression and T-PD-L2 expression. I-PD-L2 expression was significantly correlated with I-PD-L1 expression, but not with T-PD-L1 expression in the CRC patients. There was also no significant correlation between T-PD-L2 expression and T-PD-L1 expression. Interestingly, in a previous study on 172 pembrolizumab-treated HNSCC patients, the ORRs of patients expressing PD-L1 and PD-L2 were 23.0% (95% CI 16.0, 31.4%) and 26.6% (95% CI 18.0, 36.7%), respectively. Furthermore, in HNSCC patients with positive and negative PD-L2 expression, the ORRs were 26.6% (95% CI 18.0, 36.7%) and 9.6% (95% CI 3.2, 21.0%), respectively. In the pembrolizumab-treated HNSCC patients, PD-L2 expression was significantly associated with ORR, regardless of PD-L1 status. In our results, among 171 patients with negative PD-L1 expression of immune cells, PD-L2 expression of immune cells was identified in 8.8% (15 of 171). Thus, the evaluation for PD-L2 expression can be useful for predicting the immunotherapeutic effect in patients with negative PD-L1 expression.
The correlation between PD-L2 expression and survival is controversial. Ohigashi et al. 13 reported that PD-L2 expression was significantly correlated with poor prognosis in esophageal cancer. However, there was no significant correlation between T-PD-L2 expression and survival in pancreatic cancer, ovarian cancer, and hepatocellular carcinoma.14-16 The prognostic potential of PD-L2 is also controversial in lung squamous cell carcinoma patients who have not received PD-1/PD-Ls-targeted immunotherapy. 7 However, these studies did not investigate the prognostic implication of I-PD-L2 expression. Masugi et al. 2 reported that there was no significant correlation between T-PD-L2 expression and mortality in CRC patients. However, in that study, cases with no PD-L2 expression were included in the 0–20% subgroup, not in the negative subgroup. 2 In a previous meta-analysis, PD-L1 expression was significantly correlated with poor survival rates in certain malignant tumors. 17 Among four studies on CRC, Zhu et al. 18 reported that CRC patients that expressed PD-L1 had better survival rates. Lee et al. 19 recently reported similar results. In our study, PD-L2 expression was significantly correlated with better survival. Compared to PD-L1 expression, the prognostic implication of PD-L2 expression in CRC has received little attention. Various PD-L2 antibodies and evaluation criteria have been used in previous research as well as the present study. Further cumulative studies, including meta-analysis, are required. Although there was a significant correlation between T-PD-L2 expression and poor overall survival (P = 0.002), survival was significantly different in CRC patients that expressed I-PD-L2 but not T-PD-L2. According to our results, the prognostic implication of I-PD-L2 expression may be more important than that of T-PD-L2 expression in CRC patients. Therefore, subgrouping by I-PD-L2 expression and T-PD-L2 expression may be useful for prognostics in CRC patients. Among the CRC patients who expressed I-PD-L2, there was a significant difference in survival rates between those who did and those who did not express T-PD-L2. In our cohort, the CRC patients who did not express either I-PD-L2 or T-PD-L2 had the worst overall survival rates.
Lymphocytic infiltrations are frequently identified in the colorectum, and the prognostic implication of TILs in CRC is well understood.20-22 Although TILs are significantly correlated with PD-L1 expression, 19 the correlation between PD-L2 expression and TILs has not been fully elucidated in CRC. Masugi et al. 2 studied the correlation between PD-L2 expression and lymphocytic reaction in CRC. In that study, the researchers classified lymphocytic reactions as Crohn-like lymphoid reactions, peritumoral lymphocytic reactions, intratumoral periglandular reactions, and tumor-infiltrating lymphocyte reactions. Among those lymphocytic reactions, Crohn-like lymphoid reactions were significantly correlated with T-PD-L2 expression. However, as described above, the differentiation between PD-L2-negative and PD-L2-positive cases was indistinct. Furthermore, because detailed information on PD-L2 expression in the immune or stromal cells was not included, a comparison with our results is impossible. We evaluated the effect of TILs using Immunoscores, and the correlation between Immunoscores and PD-L2 expression. As a result, CRC patients with a high Immunoscore exhibited higher levels of I-PD-L2 expression—but not T-PD-L2 expression—than CRC patients with a low Immunoscore. Further evaluation of the impact of TILs on I-PD-L2 expression is required owing to the possibility of intratumoral heterogeneity and the variation in the ratios of TILs.
In conclusion, I-PD-L2 expression was significantly correlated with I-PD-L1 expression and better survival in CRC patients, regardless of tumor stages. There is also a significant correlation between the PD-L2 expression and PD-L1 expression of immune cells. Further studies for detailed evaluation criteria of PD-L2 expression is required before immunotherapeutic effects and prognosis can be predicted in daily practice.
Footnotes
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Medi-green Co,. Ltd (MG-2018-07) in 2018.