
Abstract
Purpose:
A nomogram is a reliable tool to generate individualized risk prediction by combining prognostic factors. We aimed to construct a nomogram for predicting the survival in patients with non-metastatic human epidermal growth factor receptor 2 (HER2) positive breast cancer in a prospective cohort.
Methods:
We analyzed 1304 consecutive patients who were diagnosed with non-metastatic HER2 positive breast cancer between January 2008 and December 2016 in our institution. Independent prognostic factors were identified to build a nomogram using the COX proportional hazard regression model. The prediction of the nomogram was evaluated by concordance index (C-index), calibration and subgroup analysis. External validation was performed in a cohort of 6379 patients from the Surveillance, Epidemiology, and End Results (SEER) database.
Results:
Through the COX proportional hazard regression model, five independent prognostic factors were identified. The nomogram predicting overall survival achieved a C-index of 0.78 in the training cohort and 0.74 in the SEER cohort. The calibration plot displayed favorable accordance between the nomogram prediction and the actual observation for 3-year overall survival in both cohorts. The quartiles of the nomogram score classified patients into subgroups with distinct overall survival.
Conclusion:
We developed and validated a novel nomogram for predicting overall survival in patients with non-metastatic HER2 positive breast cancer, which presented a favorable discrimination ability. This model may assist clinical decision making and patient–clinician communication in clinical practice.
Introduction
In China, breast cancer is the most commonly diagnosed cancer in women. 1 Human epidermal growth factor receptor 2 (HER2) protein overexpression or gene amplification is present in 15%–20% of breast cancers and is relevant to unfavorable survival.2,3 Trastuzumab has been proved to decrease the risk of recurrence and death in patients with HER2 positive breast cancer in several random control trials, and has since been the standard of care in this setting.4-6
It seems obvious that HER2 positive breast cancer is clinically heterogeneous, as the survival rate varies widely.7,8 As the National Comprehensive Cancer Network (NCCN) guidelines recommend 9 for patients with T1a-1b tumors that are node negative and HER2 positive, the administration of trastuzumab should balance the known toxicities of trastuzumab and its potential benefit. Thus, a reliable model to predict the outcome of patients with non-metastatic HER2 positive breast cancer is required. In addition to the conventional prognostic factors, other biomarkers such as estrogen receptor (ER) status might function to individualized risk prediction.
The nomogram is a statistical model that creates individualized risk prediction by incorporating prognostic factors. 10 Through a graphic presentation, it performs a risk quantification of a clinical event. For breast cancer, nomograms have been documented to predict pathological complete response after neoadjuvant therapy 11 or survival in metastatic breast cancer. 12 However, nomograms to predict survival in patients with non-metastatic HER2 positive breast cancer are sparse.
In this study, we intend to identify independent prognostic factors and build a prognostic nomogram for patients with non-metastatic HER2 positive breast cancer based on a single institution prospective cohort. A validation cohort from the Surveillance, Epidemiology, and End Results (SEER) database was used for externally validation. 13
Materials and methods
Patients
From January 2008, we began prospective data collection on clinicopathological characteristics, treatments, and outcomes of patients diagnosed with breast cancer in our institution. We recruited 1304 consecutive female patients who were diagnosed between January 2008 and December 2016 and met the following inclusion criteria: HER2 positive disease; had undergone mastectomy or breast-conserving surgery; no synchronous distant metastases or other malignancies; no neoadjuvant therapy; and no previous history of malignancies. Demographic, pathological, and treatment information was derived from the database. The HER2 status was determined by the testing results of immunohistochemistry or fluorescence in situ hybridization. 14 Modified lymph node ratio (mLNR) was calculated as (pLN + 0.5)/(tLN + 0.5). pLN represented the number of positive lymph nodes, and tLN was the number of examined lymph nodes. The study was approved by the Clinical Test and Biomedical Ethics Committee of our institution, and informed consent was gained from the enrolled patients.
The SEER cohort consisted of 6379 patients diagnosed with non-metastatic HER2 positive breast cancer who underwent surgery in 2010.
Follow-up
All patients in the training cohort were followed up to May 2017. Overall survival was counted as the interval between the surgery date and the last follow-up date or death. The frequency of follow-up was once every 4 months in the first 3 years after surgery; once every 6 to 12 months in the fourth and fifth years; and annually after 5 years. Follow-up was operated through office visit, telephone, or postal contact.
Construction, validation of the nomogram, and statistical analysis
Univariable and multivariable analysis in the Cox proportional hazards regression model was conducted to identify independent prognostic factors in the training cohort. Based on these identified prognostic factors, a nomogram predicting 3-year overall survival was built. The discrimination ability of the nomogram was assessed by concordance index (C-index) and subgroup analysis. According to the quartiles of the nomogram score from the training cohort, patients were sorted into four subgroups, and the Kaplan–Meier curve was used to examine the difference between the subgroups. Calibration was conducted by comparing the nomogram prediction and the actual observation. External validation was performed through a cohort from the SEER database.
A P value less than 0.05 in a two-tailed test was considered to be of statistical significance. All analyses were conducted using SPSS 22 (IBM, Armonk, NY, USA) and R version 3.4.1 (http://www.r-project.org).
Results
This training cohort consisted of 1304 patients with non-metastatic HER2 positive breast cancer—the clinicopathological characteristics of which are listed in Table 1. All patients received mastectomy or breast-conserving surgery; of these, 1269 (97.3%) patients received adjuvant chemotherapy and 360 (27.6%) patients received adjuvant trastuzumab. A total of 719 patients had positive hormone receptor tumors, 90.5% (n=651) of whom received adjuvant endocrine therapy. The median number of examined lymph nodes was 20 (range, 0–74). At a median follow-up of 40 months (range, 4–112 months), a total of 65 (5.0%) deaths occurred.
Characteristics of the training cohort and SEER cohort.
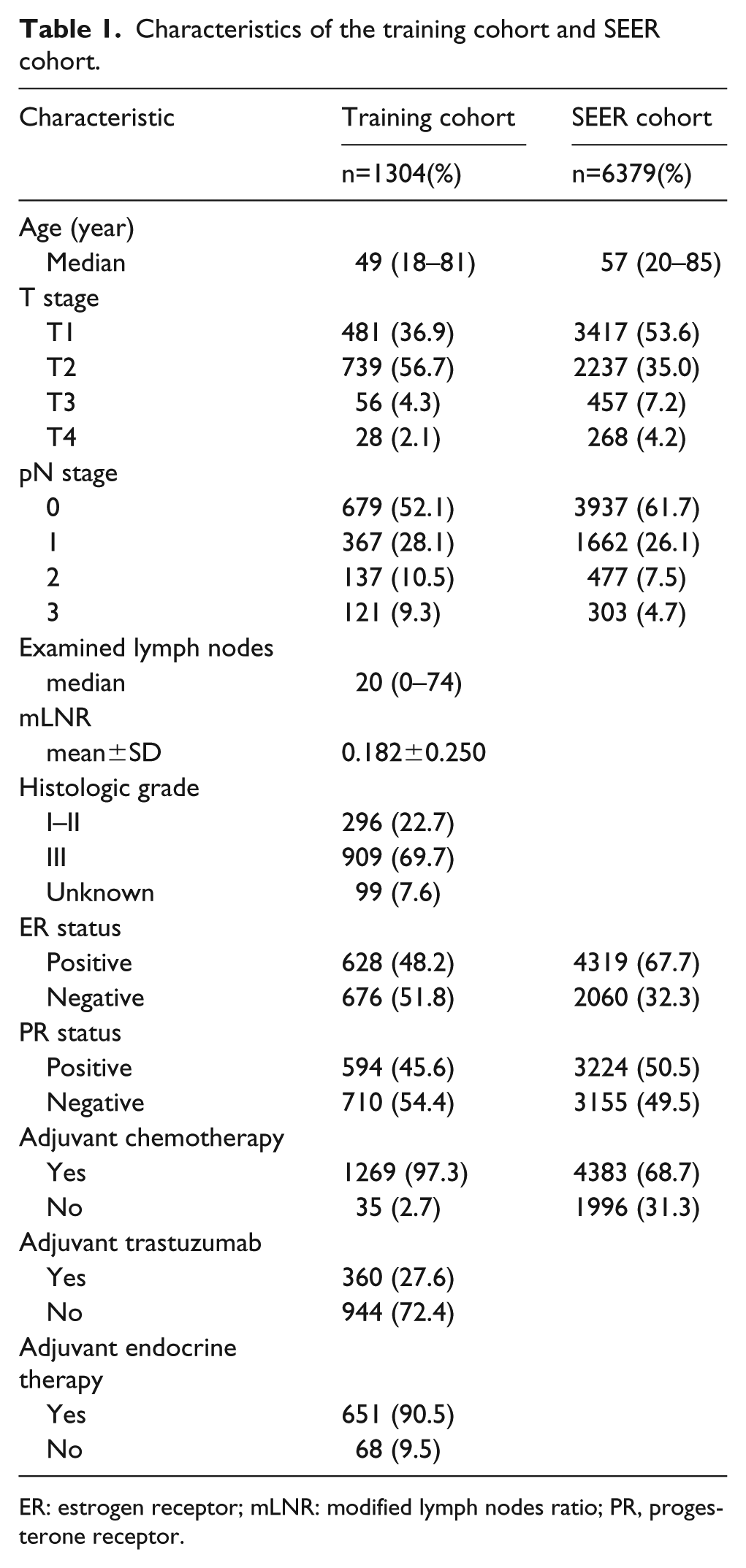
ER: estrogen receptor; mLNR: modified lymph nodes ratio; PR, progesterone receptor.
The SEER cohort was comprised of 6379 patients with non-metastatic HER2 positive disease, whose clinical characteristics are listed in Table 1. All patients received surgery, and 4383 (68.7%) received adjuvant chemotherapy; 897 (14.1%) deaths occurred.
After univariable analysis in the training cohort, the variables that achieved significance (P<0.05) were factored into multivariable analysis in the COX proportional hazard regression model. Finally, five factors (age, T stage, pathological N stage, ER status, and receipt of adjuvant trastuzumab) were found to be independent prognostic factors for overall survival (Table 2). A nomogram predicting 3-year overall survival was constructed by incorporating the above independent prognostic factors (Figure 1). Each variable was assigned a risk score according to its contribution in the multivariable analysis (Table S1). The probability of overall survival for a patient can be identified in the lowest scale after adding up these scores.
Univariable and multivariable Cox regression model for overall survival in the training cohort.
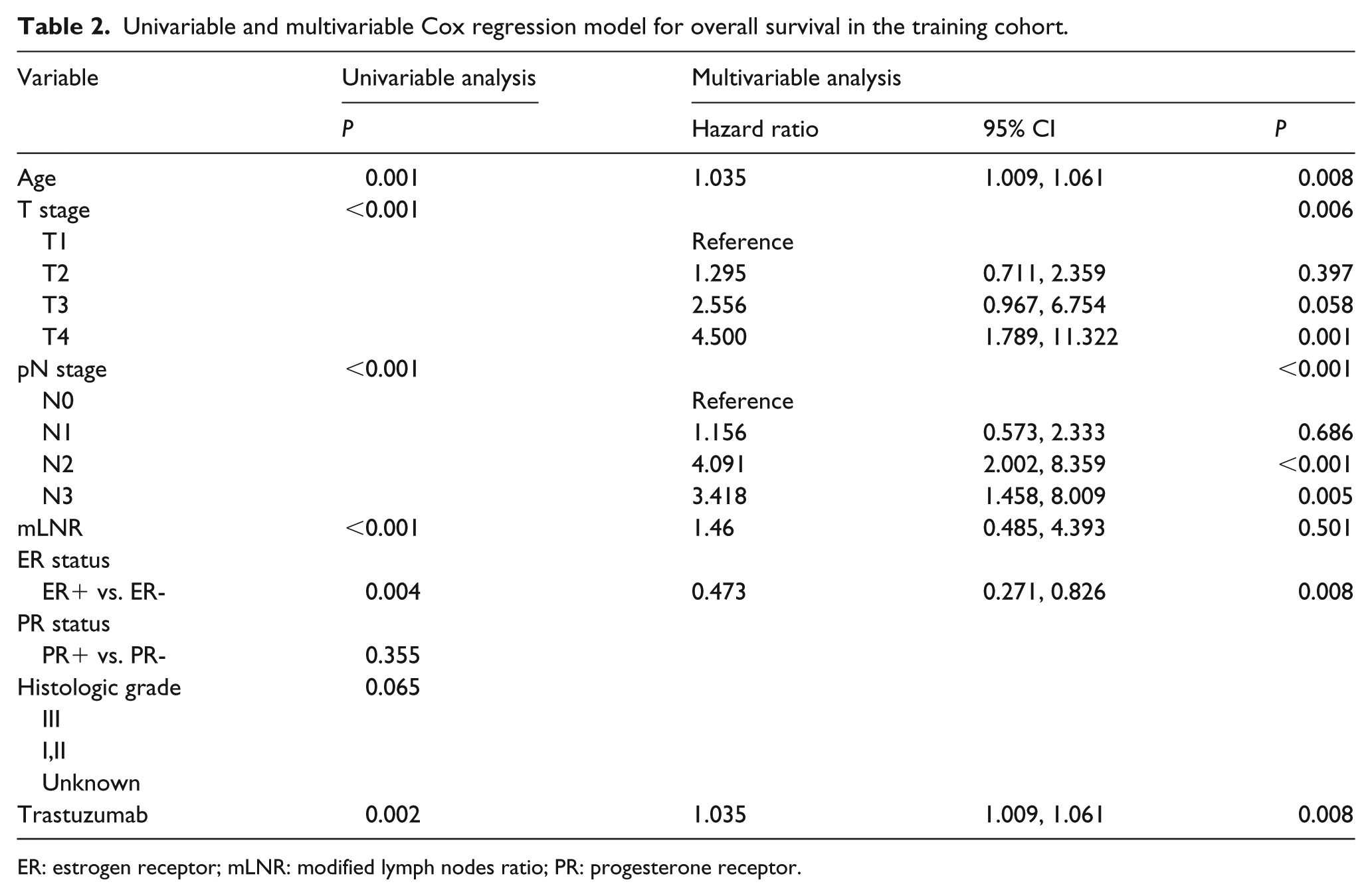
ER: estrogen receptor; mLNR: modified lymph nodes ratio; PR: progesterone receptor.
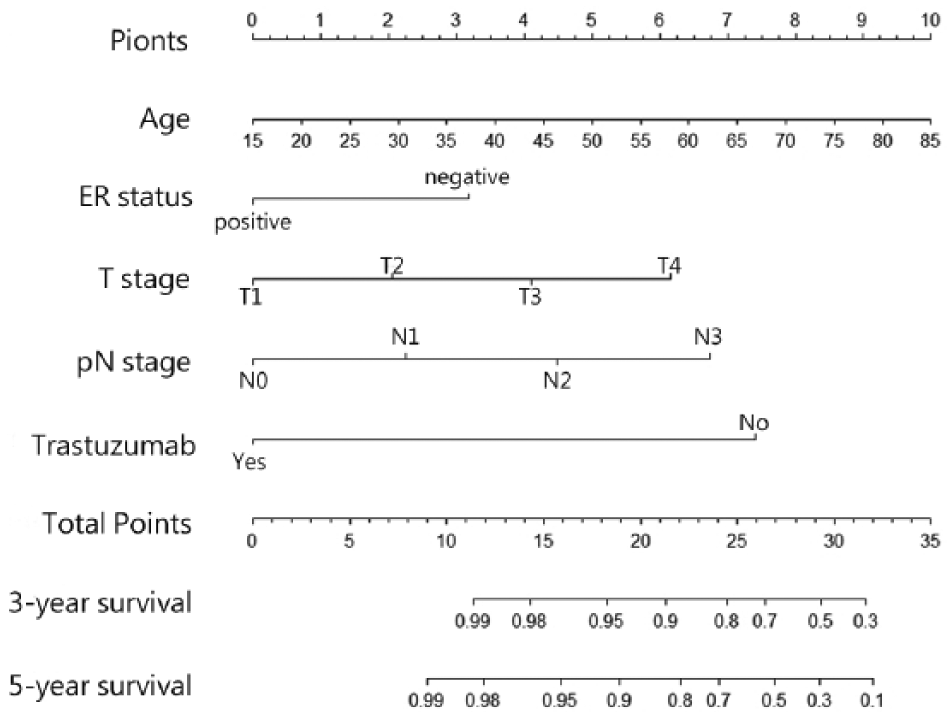
Nomogram predicting overall survival for patients with non-metastatic HER2 positive breast cancer.
The C-index of the nomogram for predicting 3-year overall survival were 0.78 (95% CI 0.72, 0.83) in training cohort and 0.74 (95% CI 0.72, 0.76) in SEER cohort.
The calibration plots for 3-year overall survival showed favorable accordance in both cohorts (Figure 2). Based on the quartiles of the nomogram score from the training cohort, patients in both cohorts were sorted into four subgroups: quartile 1 (score 0–10), quartile 2 (score 11–14), quartile 3 (score 15–16), and quartile 4 (score >17). As shown in Figure 3, the subgroups experienced distinct overall survival in the training cohort and the SEER cohort (P<0.001). In addition, subgroups of patients not receiving trastuzumab from the training cohort also exhibited distinct overall survival (P<0.001). The quartile 4 subgroup in patients receiving trastuzumab from the training cohort experienced significant worse overall survival than the other quartile 1–3 subgroups (P=0.01).
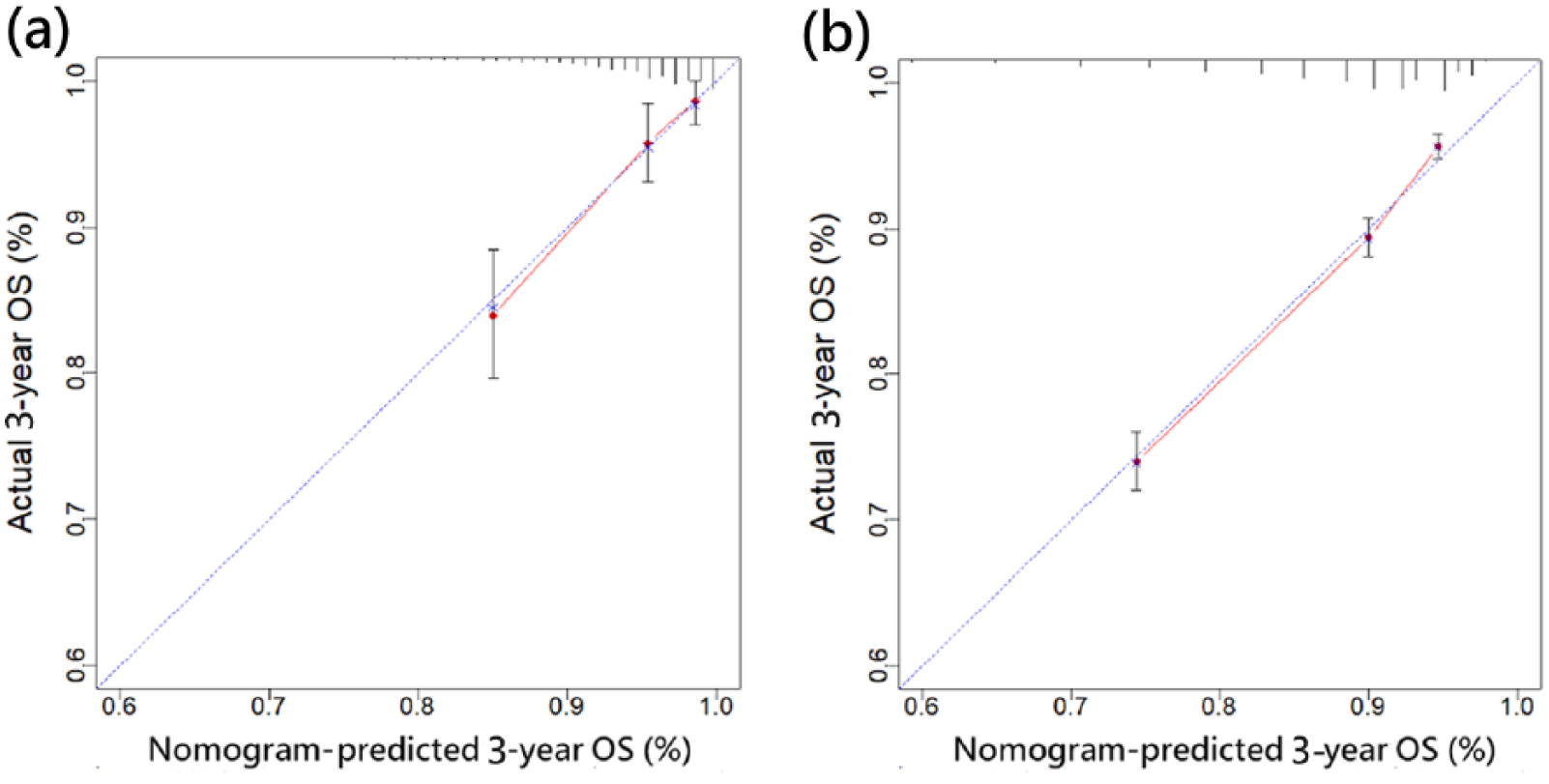
Calibration curves of the nomogram to predict 3-year overall survival in training cohort (a) and SEER cohort (b). Nomogram-predicted 3-year overall survival is plotted on the x-axis; actual observed 3-year overall survival is plotted on the y-axis. The dotted line served as the ideal reference line where the predicted survival matched the actual survival.
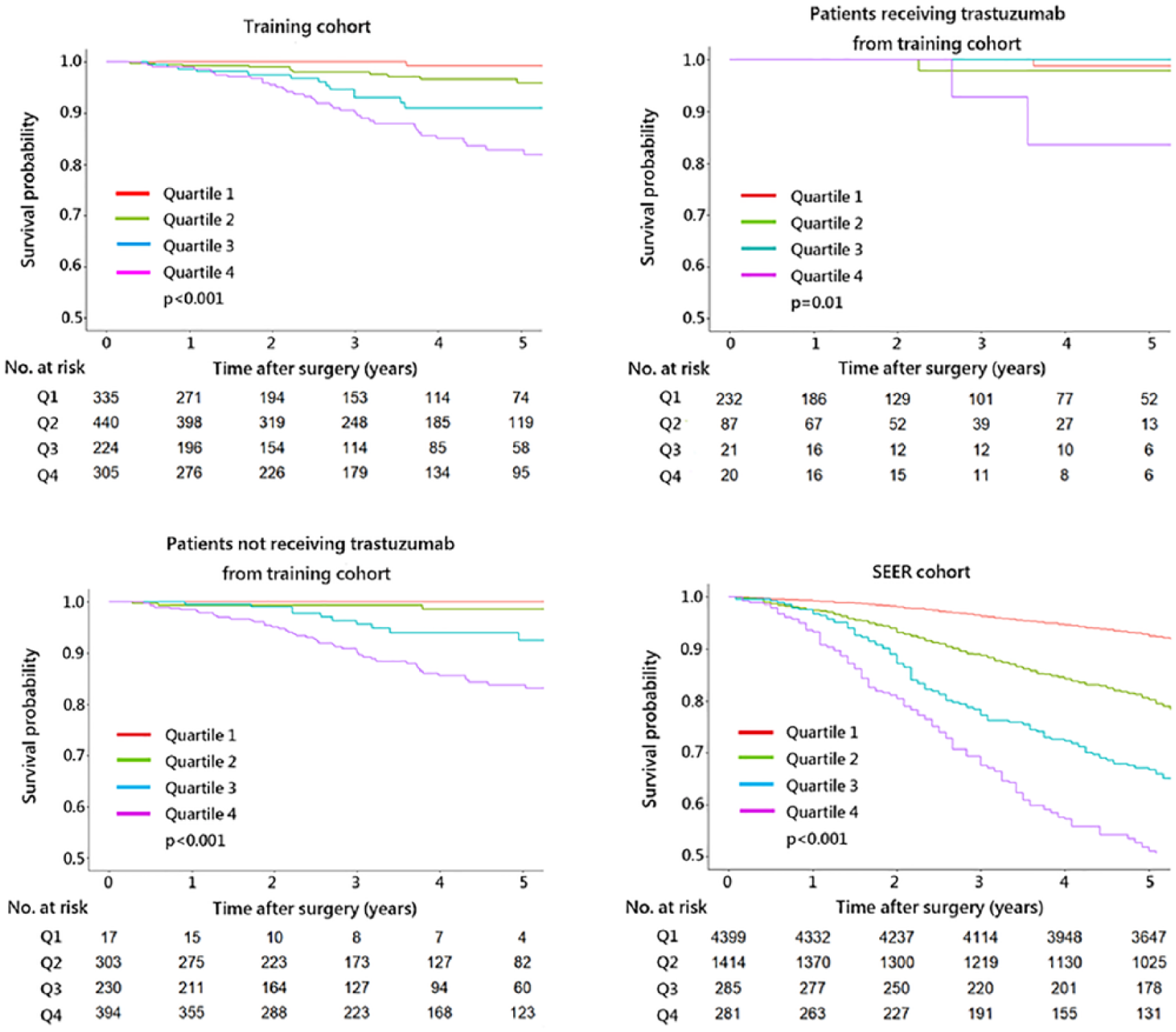
Kaplan–Meier curves of subgroups by quartiles of nomogram score in the training cohort and the SEER cohort.
Discussion
The administration of trastuzumab has rewritten the natural history of HER2 positive breast cancer, yet there is no prognostic model specific to the overall survival of non-metastatic HER2 positive breast cancer based on real-world evidence. In the present study, we built and validated a prognostic nomogram specific to non-metastatic HER2 positive breast cancer in a prospective cohort, which demonstrated a favorable predictive ability.
Outside the clinical trials, the effectiveness of trastuzumab has been confirmed in several real-world studies. Vici et al. 15 reported trastuzumab to be associated with improved 5-year overall survival of HER2 positive breast cancer patients in an observational cohort study. Seferina et al. 16 documented that trastuzumab was relevant to a 13.3% gain in 5-year overall survival. Consistent with previous knowledge, our study found that trastuzumab was an independent prognostic factor for overall survival in a multivariable analysis.
The use rate of trastuzumab in clinical practice was also examined by real-world studies. The real-world evidence from western populations reported a use rate of trastuzumab from 49% to 83%,15-19 but always with disparities between different races or socioeconomic status.19,20 In contrast, the use rate of trastuzumab in China was relatively low. Li et al. 21 reported that the use rates of trastuzumab in resource-abundant regions and resource-limited regions were 37% and 13%, respectively. The use rate of trastuzumab in our study (27%) was lower than that in resource-abundant regions (37%). Although the current health expenditure (CHE) per capita in China has been raised from $42.5 to $425.6 from 2000 to 2015, the out-of-pocket expenditure as percentage of CHE (32.4%) was higher than that of the US (11.1%) and the UK (14.8%). 22 This finding might suggest out-of-pocket expenditure to be a reason for the underuse of trastuzumab in China, apart from other common reasons, such as comorbidity and the long duration of treatment.
The presence of ER indicates the favorable survival of endocrine treatment. 23 Moreover, this predictive role of the ER status is maintained in the setting of HER2 positive breast cancer. Several random control trials have reported that positive ER status was significantly associated with increased overall survival, irrespective of other pathological characters or the receipt of trastuzumab.5,24 Similarly, in the present study, the ER status was found to be an independent prognostic factor for overall survival in a multivariable analysis. The benefit derived from trastuzumab did not mask the survival impact of the ER status.
External validation is a vital method to address overfitting and to examine the external applicability of the nomogram. We externally validated the nomogram using an independent cohort from the SEER database. The C-index of the nomogram achieved 0.78 (95% CI 0.72, 0.83) in the training cohort and 0.74 (95% CI 0.72, 0.76) in the SEER cohort, both of which were comparable to those of other nomograms for breast cancer.11,25 Moreover, four subgroups classified by the quartiles of the nomogram score displayed distinct overall survival in the Kaplan–Meier curves, suggesting a favorable discrimination ability and generalizability. The calibration plots for the probability of 3-year overall survival displayed a favorable agreement in both cohorts.
Although the large sample size of our study offered substantial statistical power, we acknowledge some limitations in the present study. Histological grade has been reported as a prognostic factor for relapse-free survival in HER2 positive breast cancer. 15 However, we could not sufficiently examine the overall survival effect of histological grades since the data of 99 (7.6%) patients were missing. Furthermore, the information of trastuzumab was unavailable in the SEER cohort, which may limit the power of external validation.
Conclusion
We built and validated a prognostic nomogram for patients with non-metastatic HER2 positive breast cancer. The nomogram presented a favorable discrimination ability. As a novel nomogram specific to non-metastatic breast cancer, our nomogram needs to be improved by further studies.
Supplemental Material
Table_S1 – Supplemental material for Prognostic nomogram for patients with non-metastatic HER2 positive breast cancer in a prospective cohort
Supplemental material, Table_S1 for Prognostic nomogram for patients with non-metastatic HER2 positive breast cancer in a prospective cohort by Chuanxu Luo, Xiaorong Zhong, Zhu Wang, Yu Wang, Yanping Wang, Ping He, Qian Peng and Hong Zheng in The International Journal of Biological Markers
Footnotes
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.