
Abstract
Background:
Chemotherapy plus targeted therapy is the established treatment for human epidermal growth factor receptor 2 (HER2)–overexpressing breast cancer (BC). Limited data regarding the safety and activity of the combination of eribulin and trastuzumab (E/T) in pretreated HER2-positive advanced BC (ABC) are available. The aim of this observational, retrospective, multicenter study was to examine the tolerability and the clinical activity of E/T in this setting.
Methods:
Patients treated with eribulin mesylate plus standard dose of trastuzumab were included. Data on overall response rate (ORR), progression-free survival (PFS), overall survival (OS), and safety were reported.
Results:
Between October 2012 and November 2015, 24 consecutive patients with HER2-positive ABC were included. All patients were heavily pretreated: the median number of prior chemotherapy regimens for ABC was 3 (range 2–9). The median number of cycles with E/T was 11.5 (range 2–26). The ORR was 41.7%. Median PFS was 5.4 months, median postprogression survival was 5.4 months, and median OS was 8 months. Neutropenia was the most common grade 3/4 clinical adverse event (16.7%).
Conclusions:
Tolerability and clinical activity of the E/T combination schedule are encouraging. The results of this study indicate that this combination might be considered for treatment of pretreated HER2 ABC.
Introduction
Breast cancer (BC) is the leading cause of cancer death in women. 1 Amplification or overexpression of the human epidermal growth factor receptor 2 (HER2) is observed in approximately 20% of women who develop BC and is an indicator of poor prognosis and more aggressive clinical phenotype.2–4 The discovery of therapies directed at HER2 has modified the natural history and the mortality from HER2 - positive BC; however, about 50% of patients with metastatic BC progress within 1 year. 5 The efforts to overcome trastuzumab resistance have led to the development of new drugs directed against the HER protein family, such as pertuzumab or the discovery of antibody–drug conjugate such as T-DM1.6,7
Chemotherapy plus targeted therapy is the established treatment for HER2-positive BC. Trastuzumab, an immunoglobulin G monoclonal antibody directed against HER2, is recommended within combination regimens for HER2-positive BC treatment. Trastuzumab in association with different conventional chemotherapy agents such as carboplatin, docetaxel, vinorelbine, paclitaxel, or capecitabine is effective in the management of advanced disease, but the debate about anti-HER2 combination beyond standard therapies is still open.8–10
Eribulin mesylate is a novel, completely synthetic, structurally simplified, nontaxane, microtubule dynamics inhibitor, macrocyclic ketone analogue of Halichondrin B (NSC 609395).11,12 Food and Drug Administration and European Medicines Agency approval of eribulin is based on results from 2 phase 3, international, multicenter, open-label, randomized clinical trials.13,14 These studies demonstrated improvements in overall survival (OS) in patients with advanced BC (ABC) receiving eribulin mesylate compared with those receiving a treatment of physician’s choice 13 or capecitabine. 14 Safety and tolerability profile was similar with the different regimens tested.
Limited data regarding the safety and activity of the combination of eribulin and trastuzumab (E/T) in pretreated HER2-positive ABC are available.15–17 The aim of our observational, retrospective, multicenter study was to evaluate the tolerability and the clinical activity of eribulin plus trastuzumab in this setting.
Methods
Patients
Between October 2012 and November 2015, 24 consecutive patients with HER2-positive ABC treated with eribulin mesylate (1.23 mg/m2 on days 1 and 8 of a 21-day cycle) plus standard dosing of trastuzumab (16 patients received 3-week schedule: 8 mg/kg load, 6 mg/kg every 3 weeks; 3 patients received weekly schedule: 4 mg/kg load, 2 mg/kg once a week) in 6 Italian Oncology Units were included in our retrospective analysis.
The status of estrogen receptor (ER) and progesterone receptor (PgR) was assessed by immunohistochemistry. HER2 status was assessed by either fluorescent in situ hybridization or a validated immunohistochemistry method. Patients with HER2-receptor overexpression or amplification were eligible for inclusion. ER and PgR status was defined positive if ⩾1% immunostained tumor cells were present.
Concomitant medication that did not interfere with the evaluation of eribulin could be administered, including antiemetics, antidiarrheal therapy, corticosteroids, and antihistamines. Cardiac function was monitored every 3 months. The efficacy of eribulin and trastuzumab was assessed every 2 or 3 cycles following administration according to the Response Evaluation Criteria in Solid Tumors (RECIST 1.1 version) guidelines.
Statistical analysis and end points
This is a retrospective study. Data on clinical features, tumor characteristics, and baseline data were collected using an anonymized database to enable the retrieval of files manually based on patient codes at the “Antonio Perrino” Hospital Oncology Department (Brindisi, Italy).
Numerical and categorical variables were explored with descriptive statistics (mean/median and intervals, frequencies, and cross-tabulation tables). Time-to-event end points were analyzed using the Kaplan-Meier method.
Overall response rate (ORR) was defined as the rate of complete response (CR) plus the rate of partial response (PR), while clinical benefit rate (CBR) was defined as CR and PR rates plus stable disease (SD) for at least 6 months.
Postprogression survival was defined as time from evidence of disease progression during treatment with eribulin mesylate to death for any reason. OS was defined as time from first administration of eribulin mesylate to death for any reason. All patients were evaluated for toxicity using the Common Terminology Criteria for Adverse Events (CTCAE) version 4.0.
All the data were analyzed using IBM SPSS Statistics 20.0.
Results
Efficacy
The median age of the 24 consecutive patients with HER2-positive ABC at the time of the E/T regimen administration was 57 years (range 32–74 years). All patients were heavily pretreated, with a median of 3 prior chemotherapy regimens for ABC (range 2–9). Eastern Cooperative Oncology Group Performance Status was 0–1 in 75%, and visceral metastases were present in most patients (Table 1). The HER2 assessment was performed mostly in primary tumors.
Baseline characteristics of the 24 patients diagnosed with advanced breast cancer (ABC) treated with eribulin mesylate and trastuzumab (E/T).
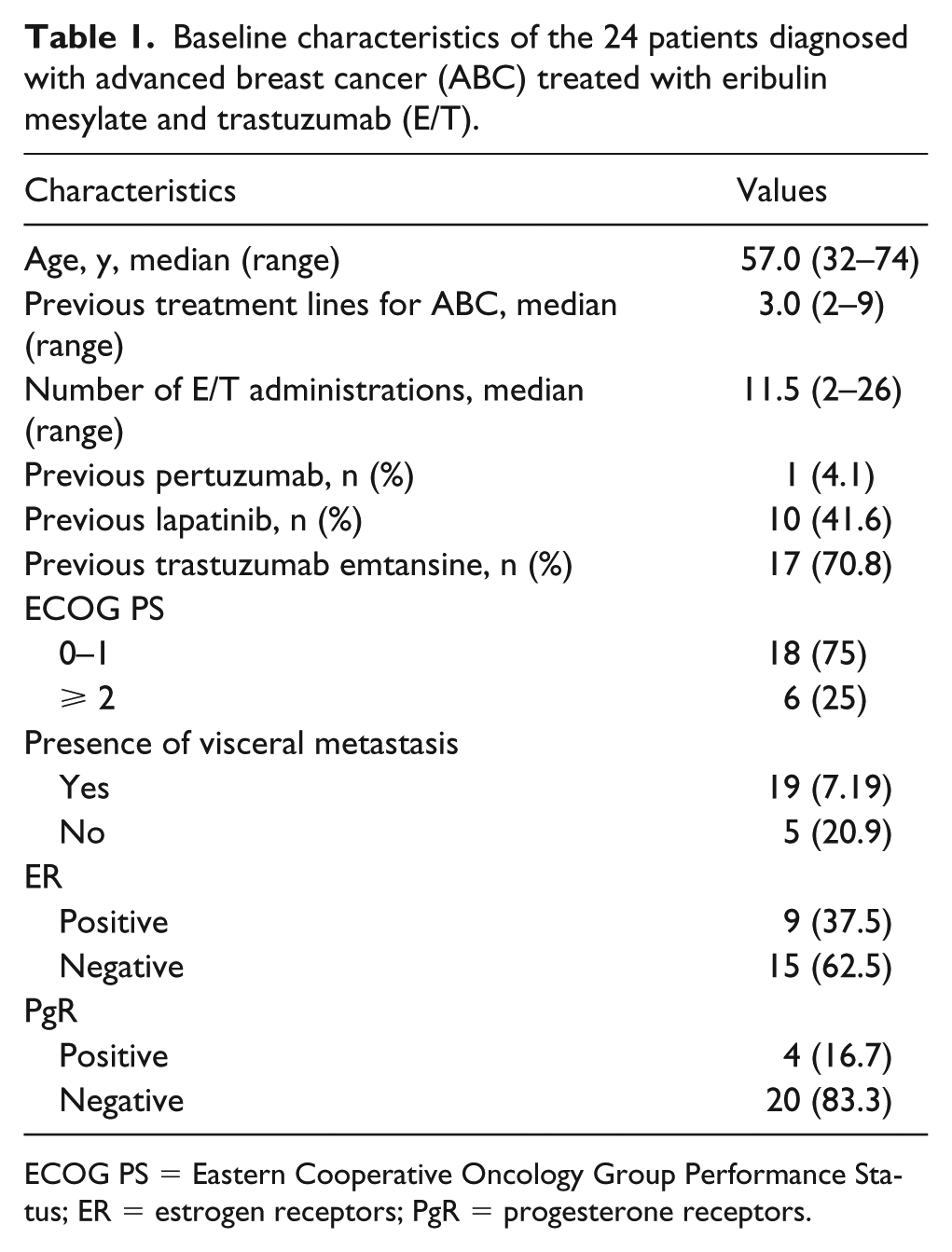
ECOG PS = Eastern Cooperative Oncology Group Performance Status; ER = estrogen receptors; PgR = progesterone receptors.
The median number of cycles with E/T was 11.5 (range 2–26). The ORR was 41.7% and CBR was 79.2%, with 1 CR, 9 PRs, 9 cases of SD, and 5 cases of progressive disease (PD). Median PFS was 5.4 months (range 1–10.5) and median OS was 8 months (range 1.3–14.8) (Figure 1, A and B).
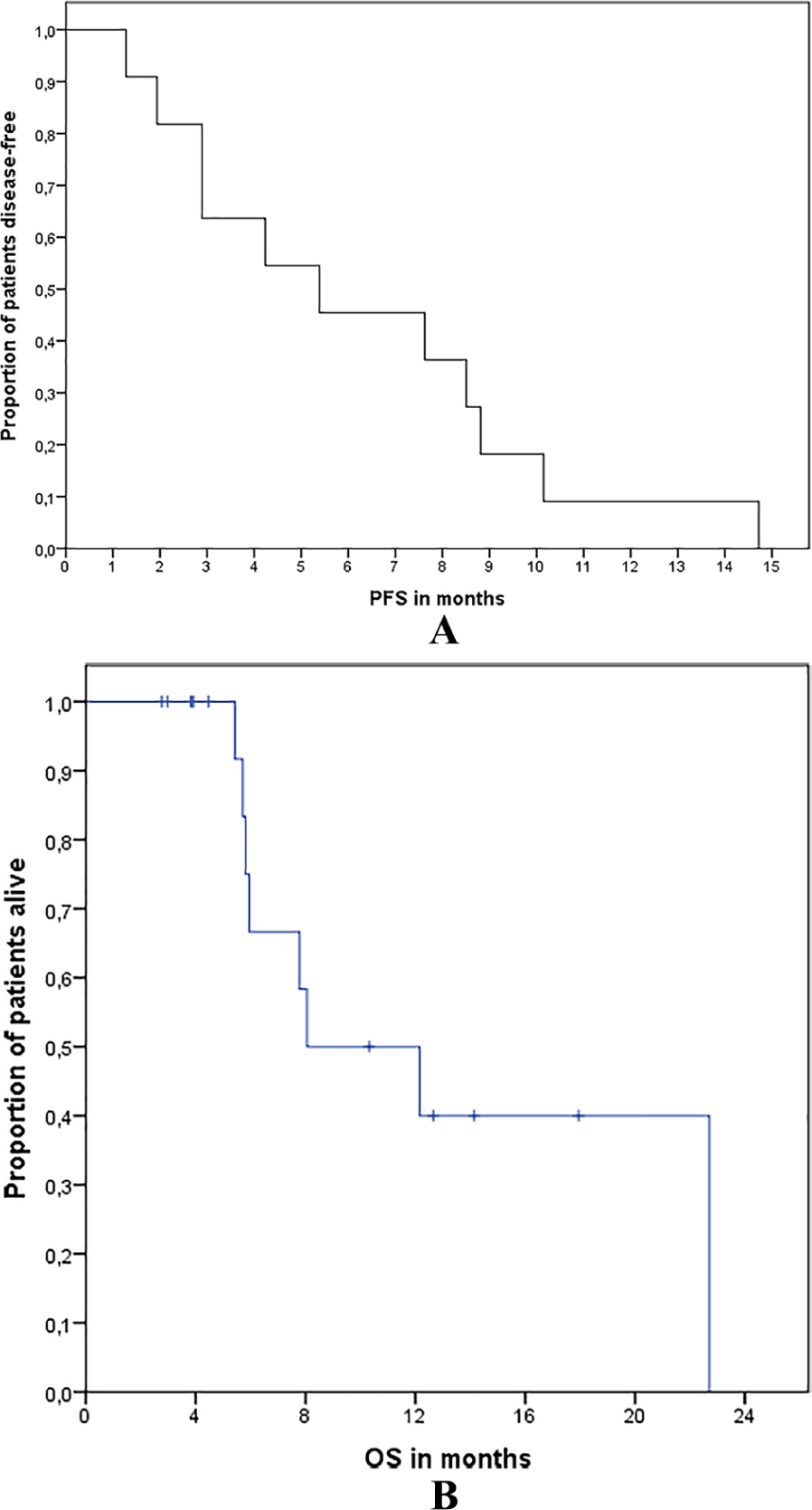
Kaplan-Meier analysis of time-to-event endpoints. (A) Progression-free survival (PFS). (B) Overall survival (OS).
Toxicities
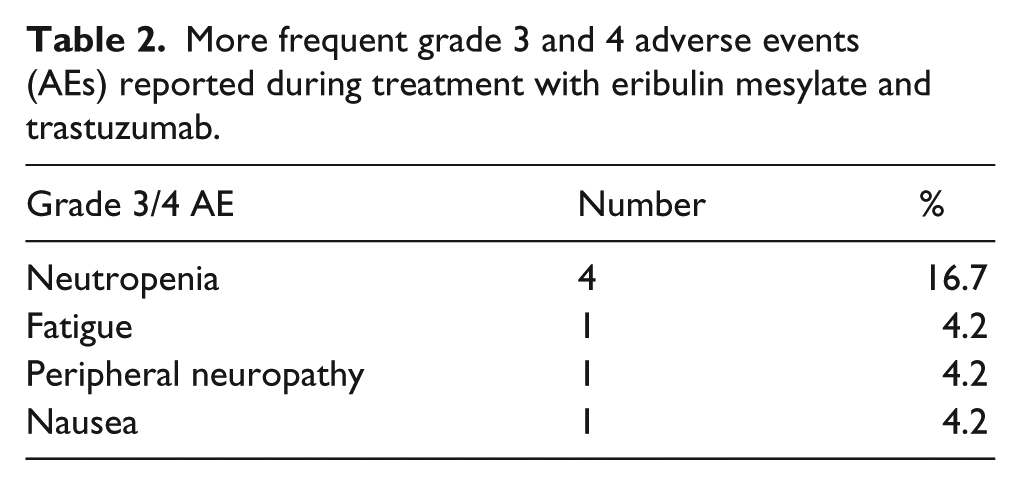
Overall, hematologic toxicity was reversible and manageable. Neutropenia was the most common grade 3/4 clinical adverse event (16.7%); no febrile neutropenia was observed. Patients also reported grade 3/4 fatigue (4.2%), peripheral neuropathy (4.2%), and nausea (4.2%) (Table 2). Grade 2 alopecia was observed in the majority of patients (62.5%). Cardiac toxicity was not observed. Dose reduction was necessary in 6 patients (25.0%); no patients interrupted the treatment prematurely. There were no treatment-related fatalities.
More frequent grade 3 and 4 adverse events (AEs) reported during treatment with eribulin mesylate and trastuzumab.
Discussion
The present retrospective analysis investigated the tolerability and activity of E/T combination therapy in pretreated HER2-positive ABC. The ORR was 41.7%, CBR 79.2%, and median PFS 5.4 months in this population of heavily pretreated ABC.
Eribulin is a new generation chemotherapy agent with a wide range of activity. 12
The pooled analysis of 2 phase 3 studies of eribulin in pretreated patients13,14 showed a longer OS in all subgroups. 18 Both the 305/EMBRACE study and 301 Study included HER2-positive or HER2-negative patients. In the pooled analysis, a nonsignificant advantage in terms of OS was achieved with eribulin monotherapy also in HER2-positive population (hazard ratio [HR] 0.82, 95% confidence interval [CI] 0.62–1.06; p=0.135; median OS 13.5 versus 12.2 months). However, single agents in the HER2-positive population are now less frequently administered with the mounting knowledge about the benefit of continuing HER2 blockade following disease progression.
In the EMBRACE trial, eribulin significantly prolonged OS in women with ABC after either adjuvant or metastatic anthracycline and taxane treatment (HR 0.85, 95% CI 0.77–0.95; p=0.003; median OS 15.2 versus 12.8 months). This OS benefit was observed in patients with BC negative for HER2, regardless of hormone receptor status, and triple-negative BC (TNBC) (HER2-negative BC: HR 0.82, 95% CI 0.72–0.93; p=0.002; median OS 15.2 versus 12.3 months; TNBC: HR 0.74, 95% CI 0.60–0.92; p=0.006; median OS 12.9 versus 8.2 months). Differences in treatment were not significant in women with HER2-positive ABC (HR 0.82, 95% CI 0.62–1.06; p=0.135; median OS 13.5 versus 12.2 months). The most common eribulin-related adverse events were fatigue, neutropenia, alopecia, peripheral neuropathy, nausea, and constipation. Peripheral neuropathy was the adverse event most frequently resulting in discontinuation of therapy, occurring in fewer than 5% of patients involved in the EMBRACE study.
The role of eribulin in advanced TNBC is now well-known, as opposed to HER2-positive ABC. 19
The standard of care for patients with HER2-positive BC with metastatic disease in first-line therapy is the combination of pertuzumab plus trastuzumab and taxane 6 and trastuzumab emtansine in the second-line, 7 followed by different combinations of trastuzumab plus single-agent chemotherapy and capecitabine plus lapatinib. 8
The chance of prolonged survival achieved with new agents has led to the need for further therapies for progressive HER2-positive patients. The introduction of vaccines, antibody drug conjugate, and bifunctional antibodies will probably make the trastuzumab/chemotherapy combination less exciting.20,21 However, the availability of further, low-toxic association of old cytotoxic and anti-HER2 agents could be useful to obtain disease control and maintain a good quality of life also in subsequent lines of treatment. Moreover, the earliest use of anti-HER2 strategies such as pertuzumab and trastuzumab emtansine in the (neo)adjuvant setting22,23 will raise the need for other combinations in advanced settings.
The role of eribulin in HER2-positive BC has been investigated. A multicenter, phase II, single-arm study evaluated 52 patients with recurrent or metastatic HER2-positive BC who received first-line eribulin with trastuzumab. 24 The ORR was 71.2% with a median time to first response of 1.3 months; duration of response and PFS were 11.1 and 11.6 months, respectively. Patients received a median of 10.0 cycles of eribulin and 11.0 cycles of trastuzumab. Most common grade 3/4 treatment-emergent adverse events were neutropenia in 20 (38.5%) patients, grade 3 peripheral neuropathy in 14 (26.9%) patients, fatigue in 4 (7.7%) patients, and febrile neutropenia in 4 (7.7%) patients. The authors concluded that combination E/T is an acceptable treatment option for recurrent or metastatic HER2-positive BC.
A recent study by Kiba et al. 15 evaluated the efficacy of E/T in the treatment of 5 patients with recurrent BC. The median number of prior treatment regimens was 5 (range 5–11). Overall, 1 patient achieved PR, 3 SD, and 1 PD; no CR was documented. The ORR was 20% and the CBR was 80%. Although 80% of patients reported grade 3/4 neutropenia, hematologic toxicity was reversible and manageable. The most common grade 3/4 nonhematologic toxicities were fatigue (20%), peripheral neuropathy (20%), and appetite loss (20%). No patients withdrew from treatment, and favorable compliance was achieved in the study.
Also in our series, toxicity was mild and manageable and driven by eribulin, as expected. No cardiac event was observed in this pretreated population.
Conclusion
Our retrospective study confirmed literature data and showed that tolerability and clinical activity of the E/T combination schedule are encouraging. The E/T combination holds potential to be a suitable treatment option in patients with recurrent BC.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, or publication of this article.